
Abstract
Transitioning to practice is challenging for baccalaureate nursing students. In baccalaureate nursing programs, the process typically begins in the junior year. A Successful transition depends on how well students apply their developing knowledge during clinical placements. A cross-sectional, multisite, qualitative study was conducted at four universities in Greater Beirut, Lebanon. In total, 35 junior baccalaureate students participated in audio-recorded focus group discussions. Thematic analysis was used to analyze the data. Three themes were sufficient to summarize the students experiences: “being unprepared,” “learning unexpected lessons,” and “taking responsibility.” Three subthemes, revising expectations, discovering divergence, and self-monitoring, were used to clarify the unexpected lessons students learned during clinical placements and how students responded. “Loving nursing and protecting yourself,” making the most of every day, and doubting future readiness were subthemes within the “taking responsibility” theme. Students troubled by nursing practices that diverged from their expectations monitored themselves to avoid falling into poor practices and kept track of the nursing procedures they performed. Only by taking responsibility for their learning, could students develop the competencies they will need as registered nurses. Faculty, clinical instructors, hospital administrators, nurse managers, and registered nurses need to do more to support students to take control of their learning.
Keywords
Introduction
Being a nurse can be defined as possessing the knowledge, skills, and attitudes necessary to provide safe and efficient nursing care (Gillespie & Peterson, 2009). Whether making the transition from junior nursing student to senior nursing student, or from nursing student to novice nurse, making the change is difficult and demanding (Beck, 1993; Bowles & Candela, 2005). In Lebanon, the process begins for baccalaureate nursing students with the first clinical placement in the junior year. A Successful transition depends on learning how to work with patients, how to fit into a clinical team, and how to transfer knowledge from the classroom and the simulation laboratory to patient care. The need to become competent while navigating the sensitivities of being an outsider creates tensions and challenges (Sheu, Lin, & Hwang, 2002).
Transition is more successful when faculty and nurse administrators cooperate to support students to achieve clinical competencies (Wu, Enskär, Lee, & Wang, 2015). Variations in the quality of clinical placements and lack of support compromise the transition to practice (Lukewich et al., 2015). Preparing for clinical placements in the simulation laboratory helps, but students struggle to apply what they learn to patient care (Jeppesen, Christiansen, & Frederiksen, 2017). Marginalization of nursing students in clinical settings impedes the transfer of learning (Lovrić, Prlić, Milutinović, Marjanac, & Žvanut, 2017; Mirlashari, Warnock, & Jahanbani, 2017; Molesworth, 2017). The stress caused by transitioning to practice intensifies as the number of patients students care for increases (Ewertsson, Bagga-Gupta, & Blomberg, 2017). Compassion fatigue and burnout can result when stressors become overwhelming (Mathias & Wentzel, 2017).
The stressors students experience reflect differences between knowledge learned in the classroom and the realities of caring for patients. Clinical units are less familiar to students than classrooms and reveal tensions between the professionalism encouraged by instructors and the demands of everyday nursing work (Tiwaken, Caranto, & David, 2015). For learning to occur, it is essential for students to have experiences that match their expectations, receive feedback, and have time for reflection (Karimi, Haghani, Yamani, & Najafi Kalyani, 2017). The gap between student expectations and clinical realities remains the persistent challenge of baccalaureate nurse education (Papathanasiou, Tsaras, & Sarafis, 2014).
In Lebanon, no studies have explored how students transition through baccalaureate nursing programs. It is not known whether students experience the same challenges as those reported in the international literature. We conducted a cross-sectional, multisite, qualitative study to understand the challenges students experience as they transition to practice in their junior year, in their senior year, and during their first year as a registered nurse. In this article, we report on the transition experiences of students in their junior year at four universities. The research questions we address are as follows:
Method
Ethics Approval and Recruitment of Participants
The institutional review boards of the four participating universities approved the study. Flyers were posted to attract students. Students contacted the research team member of their choice for more information. Research team members explained the study, answered questions, and gave details of the date, time, and location of focus group discussions. Written informed consent was taken immediately prior to conducting the focus groups. Participants were reminded of the importance of anonymity and confidentiality. The focus group discussions were audio recorded with the prior consent of participants. The data were stored and analyzed on password-protected computers in private offices at the four participating universities. Only the authors and their research assistants had access to the recordings and transcripts. In this article, we protect anonymity and maintain confidentiality by using pseudonyms beginning with “M” for women and “R” for men.
Focus Group Participation
In total, 35 junior students participated in the study. Women outnumbered male participants (20 women, 15 men). Men were overrepresented in the sample because approximately 20% of nurses in Lebanon are male. The number of focus group members varied from five to 13. Students were eligible for the study if they were enrolled at one of the four universities, if they were in their junior year, and if they had completed not less than 244 and not more than 488 clinical hours.
Conduct of Focus Group
Authors MC and MD facilitated separate focus groups in English. SE and UR conducted two focus groups in Arabic. MC facilitated his focus group in English because he lacks fluency in Arabic. The other three focus groups were facilitated in English or Arabic according to the preferences of the participants. The focal question for participants was: What was is it like for you to learn on the clinical floors this year? Follow-up probes included: What were the challenges? How did you deal with the challenges you faced? MM and two research assistants fluent in Arabic and English transcribed the digital recordings. The research assistants translated the Arabic transcripts into English. The translations were validated independently by three bilingual members of the research team (SE, MD, and UR). The interpretation of the data published here was reviewed, revised, and approved by all five authors.
Data Analysis
Microsoft Word and Microsoft Excel were used to manage the data because the authors worked as a team and used software readily available at the participating universities. The line number function in Word was used to label lines in the transcripts prior to line-by-line coding. Codes indexed to line numbers were copied into Excel to sort and aggregate data. Thematic analysis was used to analyze the data because it is flexible, practical, and its results make sense to participants as well as to investigators (Braun & Clarke, 2006). Unlike grounded theory, thematic analysis does not require construction of substantive theories, it differs from phenomenology in not presupposing a philosophical theory, and is unlike critical discourse analysis in that, it does not privilege language over human subjectivity.
We listened to the audio recordings and read through the transcripts independently. MC and MM developed initial data codes later refined at a team meeting. The agreed on codes were collapsed into broader categories to summarize the data. MC and MM selected exemplary statements to illustrate the descriptive categories. Trial and error was used until consensus was reached on which excerpts best typified the data. The categories were grouped into descriptive themes and subdivided into subthemes when possible. Exemplary statements were moved among themes and subthemes to produce a logical structure for reporting the data. Statements were regarded as credible if they were made by more than one student, as transferable if they were confirmed in another focus group, and dependable if they described first-person experiences. We describe our analytical procedures in more detail elsewhere (Clinton, Madi, Doumit, Ezzeddine, & Rizk, 2018).
Findings
We used thematic analysis to reduce the data to three analytical themes and six descriptive subthemes (Table 1). The first theme, “being unprepared,” summarizes challenges students faced due to prior schooling, self-identified shyness, and anticipated responsibilities for patient care. The second theme, “learning unexpected lessons,” and its three descriptive subthemes, revising expectations, discovering divergence, and self-monitoring, summarize how students responded when their clinical experiences differed from their expectations. The third theme, “taking responsibility,” and its four subthemes, loving nursing, protecting yourself, making the most of every day, and doubting future readiness, sum up how students took control of their learning, while doubting they will be ready for the responsibilities of a registered nurse.
Emergent Themes and Subthemes Based on Line-by-Line Coding.
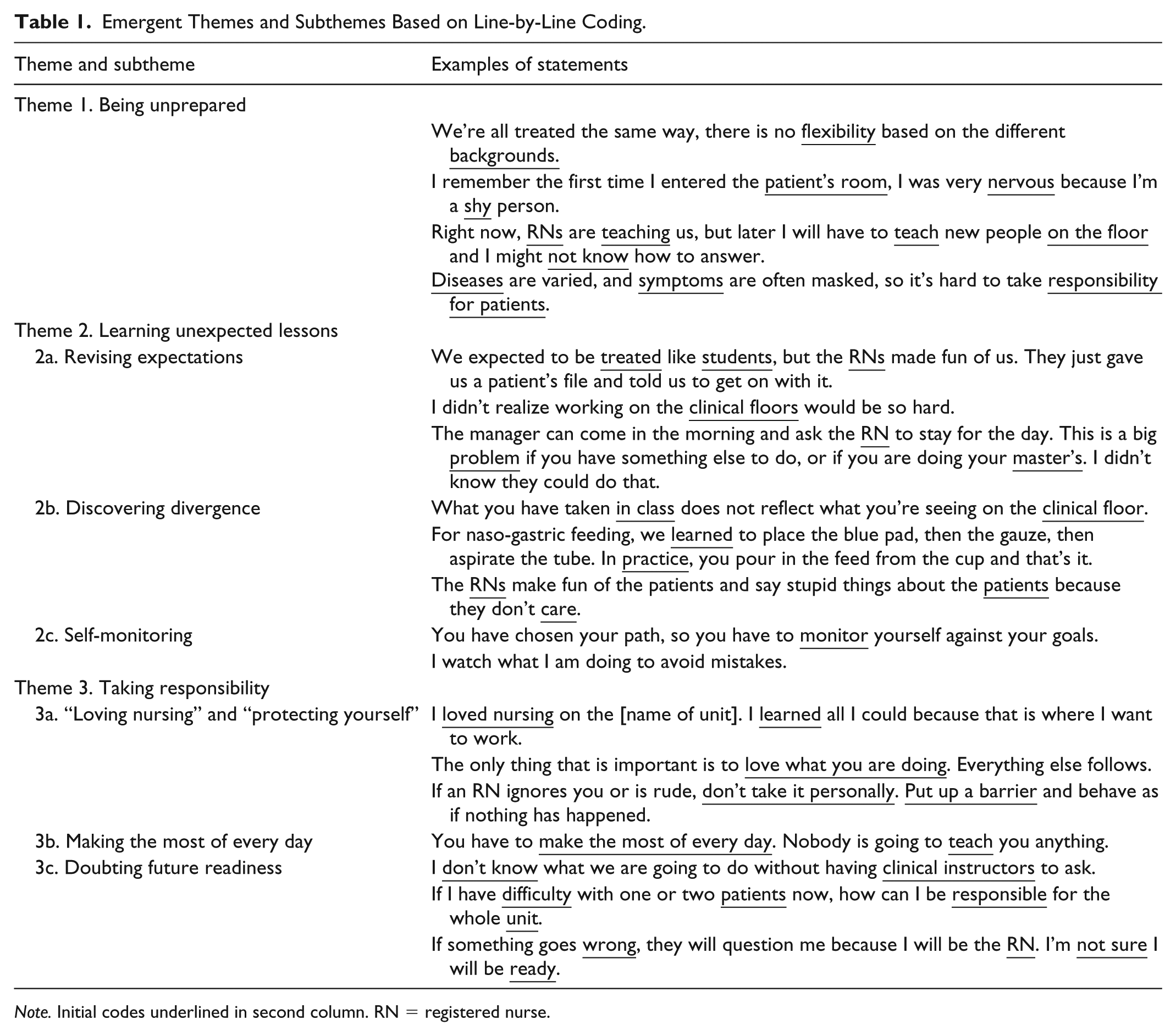
Note. Initial codes underlined in second column. RN = registered nurse.
The exemplar statements in Table 1 answer three questions: What personal challenges do nursing students believe they will face as they transition to practice? How do nursing practices in clinical units differ from what students expected? What do students do to develop the competencies they will need as registered nurses? We show that students have overlooked learning needs, are dismayed by the nursing practices they see on clinical floors, and doubt their future readiness for the responsibilities of a registered nurse. The strategies for successful transition we identify have relevance for baccalaureate nursing education in and beyond Lebanon.
Theme 1: Being Unprepared
Most baccalaureate nursing students in Lebanon are admitted directly from high schools, but a minority enroll after completing a 1-year Technique Supérieure qualification. The difference is that students admitted from high school have no prior exposure to clinical units and working with registered nurses. Not all clinical instructors take this difference into account: I came from a regular high school and had never been to a hospital before, but the clinical instructor did not take this into account. A bigger problem was we didn’t know how to deal with people on the floor. We expected to be treated respectfully, but we weren’t. (Rabi, P.1)
Unfamiliarity with clinical floors is particularly difficult for students who self-identified as “shy.”
The first time we went to the hospital, we had to take a personal history. I found it difficult because some of the questions [questions about sexual history] are personal. For a shy person like me, it would be better if we started out with less sensitive questions. (Majida, P.2)
Nursing students considered themselves different from other university students because they accept responsibility earlier.
The participants perceived that only nursing students have heavy responsibilities at the age of 19 or 20. Having responsibility for patients, coming to terms with the demands of a busy floor, learning how to communicate, behaving professionally are challenging. Other university students are only responsible for themselves. (Rashid, P.19) Preparatory work in the simulation laboratory did not always help: We practice in the [simulation laboratory], but when we go on clinical we find emotional patients who have questions. Last week, I had a patient who was anxious and depressed. I tried to reach out to her, but she was unresponsive. I didn’t know what to say to her. We need to learn more about how to talk to patients before we go to the units. (Rashid, P.19)
What stands out in these statements is that differences in background and self-identified personal traits were insufficiently considered when clinical placements were planned. The attitudes of some unit staff accentuated the challenge of transition. Practice in the simulation laboratory helped, but not enough, to prepare students for talking to patients.
Theme 2: Learning Unexpected Lessons
The theme “learning unexpected lessons” summarizes what students learned about the realities of day-to-day nursing practice.
Subtheme 2.1: Revising expectations
In some hospitals, the scope of nursing practice was narrower than students expected: Some hospitals need a wider range of nursing skills than others. We would like to be exposed to everything that nurses do because we don’t know where we will work. Limiting us to learning what only one hospital needs is unfair. If I go to another hospital, I cannot tell them, “Sorry, I don’t know how to do that because nurses weren’t allowed to do that where I came from.” Rahat (P.20)
Muna (P.15) was more specific: “We won’t be learning wound care because the RNs don’t do wound cleaning. We don’t do blood draws or give blood transfusions because the [medical] residents do them.”
Students expected to establish rapport with patients, but hospital stays were too short. They worried about what will happen when they are required to care for more than one patient: Basically, you’re always talking to strangers because by the time you feel comfortable to talk to a patient, another one has been admitted, and your back to talking to a stranger. (Mubassirah, P.24) Now we’re working with one patient and we try to do everything for that patient. When we have more patients assigned to us we will not be able to do what we do now. It’s unrealistic to think we can (Rafic, P.25)
Subtheme 2.2: Discovering divergence
What nursing students noticed most during their first clinical placement was how nursing practice “diverged” from what they had been taught: We expected the steps we learned in class to be applied correctly. But that wasn’t what happened. Staff in the hospital say practical work is different from the theory we learn. That was our first shocking encounter at the hospital. (Myesha, P.18)
The significance given to patients is another departure from classroom knowledge: The surprising thing is the patient is not always that important. What is important is finishing the work by the end of the shift. Some of the RNs just want to get finished and leave. They don’t care about the patient. (Rakin, P.16)
There is tension with registered nurses when students want to remain faithful to what they were taught: RNs tell you, “Nobody is watching, just do it and let it go.” They don’t appreciate that we don’t care about whose watching. I don’t want to treat people badly because I’m sick of my job or short of time, I don’t want to become like RNs who only want to get through the shift. Muna (P.15)
Subtheme 2.3: Self-monitoring
Students monitor themselves to avoid falling into the practices they criticize and admire attentive registered nurses: I think a lot about what nursing really is and monitor myself to avoid becoming like RNs who have become careless. When I work with competent RNs it is completely different; I see seriousness and enthusiasm rather than carelessness. (Muna, P.15)
Students kept track of nursing procedures and how often they performed them. They were disappointed when their expectations were not met. “I was able to do one blood test,” Murielle (P.17) complained. “[Name of male student] didn’t get to do any. He will go to his senior year without doing any blood tests” (Murielle, P.17).
Some procedures have iconic status. “I need more training on inserting an IV [intravenous] line. I tried 5 times but succeeded only twice. I need more practice” (Mariam, P.10). “During the rotation, I was able to insert a Foley’s catheter and a nasogastric tube. Nurses don’t usually do these things. Getting to do them is a matter of luck” (Maysa, P.11).
The unexpected lessons students learn in the junior year include the importance of a nursing workforce well prepared to meet the specific needs of hospitals and health care systems. The scope of nursing practice is enabled or limited by regulatory requirements and the availability of other health professionals, especially medical residents. Students learn that nurse–patient relationships are not easy to form because patient turnover is high. Although providing holistic care is a priority for students in their junior year, they quickly realize that it is not possible to give patients the attention they need. Students are shocked when they find out that bedside nurses do not follow all the steps when performing nursing procedures. They are even more shocked to learn that patients are sometimes less important than getting through nursing work on time. Students who are concerned about nursing practices monitor themselves to avoid falling similar habits. The final statement from Muna (P.15) in section “Subtheme 2.3. Self-Monitoring” epitomizes this concern.
Theme 3: Taking Responsibility
The theme “taking responsibility” summarizes how students took control of their learning to become proficient.
Subtheme 3.1: “Loving nursing” and “protecting yourself.”
For some students, “loving nursing” was the motivation for “taking responsibility.” For others, the motivation was to acquire skills. Either way, students were aware that they were taking a risk by reacting to the “divergences” they noticed. Rakin (P.9) summed up the need to be careful. “Loving nursing helps a lot, but you need to protect yourself” (Rakin, P.9).
Rahat (P.20) gave an example: I used to go into a patient’s room and the family members would be there. The patient would tell me, “No, I don’t want you, I want the RN.” I learned to tell the family members to leave the room while I did the procedure. At first, I felt like I had been put down, but I learned to accept whatever patients say, hurtful or not. I am feeling better because I love nursing and my skills are developing every day.
Subtheme 3.2: Making the most of every day
Students tried to make the most of every day because “We know we are going to take a lot of responsibility and need to be ready” (Majida, P.2): Overcome your hesitation. Go to the RN and say, “If you have medications to give, I’d like to give them with you.” If an RN has done an assessment, check the chart and ask questions. If you see a procedure, ask for tips about how to do it when it’s your turn. You must make the most of what’s going on around you. (Manar, P.8)
Making the most of every day includes preparing for tomorrow: “Learn about your patient when you go off shift. Do the all-nighters with your books and lots of coffee. Figure out what you need to do tomorrow and why” (Ma’isah, P.23).
Subtheme 3.3: Doubting future readiness
Despite “taking responsibility,” students worried about being able to cope with the responsibilities of a registered nurse. “Will I be able to make decisions when faced with cases I didn’t see as a student or didn’t cover in class?” (Majida, P.2) “Will I be ready to apply critical thinking?” (Medina, P.13) “Will I be able to be fair to patients and still finish on time?” (Myesha, P.18, Rakin, P.9)
From the beginning of their studies, baccalaureate nursing students are profoundly aware of the responsibilities of registered nurses. Being ready to accept the responsibilities of a registered nurse is a constant worry for them. They are concerned about being responsible for patient safety and worry about whether they will be ready when they graduate. Their anxieties drive them to take responsibility for developing the competencies they will need in the future. They seek out learning opportunities, shadow registered nurses to learn how to do procedures, and keep track of what they can and cannot do.
Discussion
The study findings clearly indicate that more needs to be done to identify the personal challenges junior baccalaureate nursing students anticipate when beginning the transition to practice. Unless faculty and clinical instructors do more to help students with no previous experience of hospitals and clinical units, it is unlikely that competency development can be optimized. Whereas the differences in learning needs of students admitted directly from high school compared with those who have completed a Technique Supérieure qualification are specific to Lebanon, readiness to learn during periods of clinical experience is an issue relevant to all baccalaureate nursing education. Learning outcomes are enhanced when instruction is individualized (Durkin & Feinn, 2017; Esmaeili, Cheraghi, Salsali, & Ghiyasvandian, 2014). Individualized instruction is essential for those students who self-identify as shy (Antohe, Riklikiene, Tichelaar, & Saarikoski, 2016; Arkan, Ordin, & Yılmaz, 2018; Condon & Ruth-Sahd, 2013; Dimitriadou, Papastavrou, Efstathiou, & Theodorou, 2015).
The unexpected lessons students learn in their junior year are not limited to Lebanon. The unwelcoming attitudes of registered nurses to students has been reported repeatedly (Courtney-Pratt, Pich, Levett-Jones, & Moxey, 2018; Kang, Jeong, & Kong, 2018; Seibel & Fehr, 2018). Similarly, what participants in our study referred to as “divergences” between classroom knowledge and nursing practice in busy clinical units are all too common. The growing literature on missed care confirms the ubiquity of registered nurses missing steps to cope with high workloads and organizational pressures (Bragadóttir, Kalisch, & Tryggvadóttir, 2017; Jones, Hamilton, & Murry, 2015; Scruth & Pugh, 2018; Smith, Morin, Wallace, & Lake, 2018). Our findings show that students are not only shocked when they become aware that registered nurses miss steps when doing nursing procedures, they come to believe that holistic care is unrealistic when there are mutliple patients to care for.
Our most significant finding was the willingness of students to take responsibility for their learning from early in the junior year. By becoming proactive, they compensated for deficiencies in their clinical placements (Alotaibi, 2016). Clinical instructors can help students who accept responsibility for their learning by encouraging them to use support networks, by facilitating peer-to-peer coaching, by cultivating students’ reflective skills, and by facilitating informal learning (Corrigan & Curtis, 2017; Thomas & Asselin, 2018). For those students who are not ready for independent learning, clinical instructors can maximize guided practice and hands-on learning (Murray, 2018).
Readiness for independent learning should not be confused with resilience. Resilient students may survive stressful clinical placements by developing coping strategies that help to mitigate criticism, high workloads, and concerns about day-to-day realities of nursing practice (Thomas & Revell, 2016). Students who accept responsibility may develop similar strategies, but the crucial difference is that they remain sensitive to and accountable for the nursing care they provide because their concerns go beyond their personal needs. Clinical instructors have an essential role in promoting compassionate nursing care because without their influence, students could become indifferent to patients if they are overly preoccupied with their own needs (Kornhaber & Wilson, 2011).
Unlike those reported by Günay and Kılınç (2018), our findings stress the importance of nurturing students to take responsibility for their learning as the primary strategy for overcoming deficiencies in clinical education. We differ from Labrague, McEnroe-Petitte, De los Santos, and Edet (2018) by not pathologizing students’ stress. Our conclusions support those of Perry, Henderson, and Grealish’s (2018) by calling on stakeholders to foster student responsibility and independence. Taking responsibility differs from resilience, in that, it goes beyond the idea of coping with stress to emphasize accountability for how one’s conduct as a nurse affects patients.
Limitations
The study has important limitations. All the participants were recruited from four universities and their experiences may not be typical of junior baccalaureate nursing students in Lebanon. Our focus group questions, which referenced “challenges,” may have encouraged students to describe negative rather than positive experiences of transition. We did not collect observational data, or conduct focus group discussions with registered nurses, preceptors, clinical instructors, faculty, nurse managers, or directors of nursing. Our analysis viewed the data through the lens of university teachers responsible for nurse education, but not routinely engaged in practice.
Conclusion
The divergence of nursing care from expectations formed in the classroom was the most impactful lesson students learned in their junior baccalaureate year. Troubled by their experiences, students monitored themselves to avoid falling into the divergent practices of overworked registered nurses. Concerned about their future readiness to assume the responsibilities of a registered nurse, students took responsibility for their learning. They sought opportunities to practice nursing procedures. By taking responsibility for their learning, could students learn the skills they will need in the future. Faculty, clinical instructors, hospital administrators, nurse managers, and registered nurses need to do more to support students to take control of their learning. Our findings imply that fostering student responsibility and independence has promise as the first-line intervention for overcoming the persistent challenges faced by baccalaureate nursing students.
Footnotes
Acknowledgements
We would like to thank the students who attended our focus group discussions for taking time out of their studies and busy lives to talk to us about their experiences of transitioning to practice.
Author Contributions
All authors made substantial contributions to all the following: (a) the conception and design of the study, or acquisition of data, or analysis and interpretation of data; (b) drafting the article or revising it critically for important intellectual content; and (c) final approval of the version to be submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.