
Abstract
Caregivers for dialysis patients have endured tremendous burden and responsibilities in their daily lives from caregiving. Interventions that cater to them are essential, considering that they play an essential role in the illness management of patients. The purpose of this review is to examine the interventions implemented among the caregivers caring for patients diagnosed CKD and its effectiveness in alleviating the caregiver burden. PRISMA-ScR checklist was utilized as the reporting standard. Past studies were searched in four major citation databases (MEDLINE, Cochrane Library, PubMed, and Web of Science) in the timeframe of February 2022. Nine studies were identified, comprised of randomized controlled trials (RCTs) and quasi-experimental studies. The types of intervention programs reviewed were educational programs, supportive programs, family-centered programs, and psychological interventions. The evidences have suggested that these programs are effective in reducing caregiver burden among the caregivers of CKD patients.
Introduction
Individuals who are diagnosed with the last stage of chronic kidney disease (CKD) are characterized by permanent loss of renal functions and require renal replacement therapy (RRT), such as hemodialysis (HD), peritoneal dialysis (PD) or kidney transplantation (Hosseinigolafshani et al., 2020), leading to increased dependency on their caregivers in daily activities (Adejumo et al., 2019). When a person is diagnosed with a chronic illness such as CKD, life changes not only occur for the patient, but also for those who are emotionally and physically involved in their care (Gayomali et al., 2008). The term “informal caregiver” is defined as an individual, such as a family member, friend or neighbor who is primarily responsible for caring and supporting the patients’ daily needs and most of their medical activities without any reimbursement for their caregiving tasks (Alnazly, 2016; Avşar et al., 2015; Cohen & Germain, 2014).
Given the complexity of CKD and dialysis treatment modalities, significant impacts on the physical and psychological well-being of patients and caregivers have been observed (Adejumo et al., 2019; Ae-Ngibise et al., 2015; Avşar et al., 2015; Goh & Griva, 2018; Lee et al., 2013; Mosleh et al., 2020). Caregivers have to face additional stress and responsibilities in their everyday life due to patients’ medical treatments, dietary requirements, clinic appointments, psychosocial issues (Tong et al., 2008), transportation, and personal care (Sherwood et al., 2005). As the consequences, the caregivers frequently experienced a high level of caregiving burden in caring for patients undergoing dialysis (Abbasi et al., 2011). Care burden is a highly subjective perspective (Gérain & Zech, 2019). The term “caregiver burden” refers to the negative subjective perception experienced by the caretakers during the provision of care for patients (Abbasi et al., 2012) and the extent of caregiving having significant effect on their emotional, social, financial, physical, and spiritual well-being (Da Silva-Gane et al., 2012; Hildebrand, 2016; Nogueira et al., 2012).
Caregivers’ well-being is often neglected and under-prioritized in the management of CKD as past studies had mostly emphasized patients’ perspectives rather than caregivers’ in alleviating their caregiver burden. Nevertheless, support for caregivers is vital as they play a pivotal role in the illness management of the patients (Belasco et al., 2006; Noble et al., 2013). Over the years, intervention programs catered toward the caregivers have gradually increased, and Bártolo et al. (2022) stated that these educational and psychological interventions were shown to be able to significantly alleviate caregiver burden in their daily life and significantly improve their quality of life. However, to the authors’ knowledge, a review that assesses the effectiveness of these interventions targeting the caregivers of patients diagnosed with CKD has not been conducted thoroughly. The most cited paper for systematic review, assessing the interventional programs for caregivers of patients with CKD was conducted by Tong et al. (2008) with only three included studies. There are possibilities that several studies related to interventional programs for care burden catering toward CKD caregivers have been widely published after the year 2008, despite this, these studies after the year 2008 are not being systematically reviewed.
On the other hand, Bártolo et al. (2022) have conducted a systematic review to examine the efficacy of psychosocial interventions on the burden and quality of life among the caregivers of hemodialysis patients. Despite this systematic review being conducted recently, it mainly focused on caregivers of the hemodialysis population, disregarding the care burden faced by caregivers of peritoneal dialysis, transplantation patients, or CKD patients. On the other hand, the systematic review conducted by Hovadick et al. (2021) to investigate the effectiveness of interventions in improving the well-being of the caregivers of dialysis patients, the review also largely emphasized on the caregivers caring for hemodialysis patients. Therefore, the caregivers of CKD population have been overlooked in the past reviews conducted by Bártolo et al. (2022) and Hovadick et al. (2021). This suggests the need for a review that encompassed all the caregivers of CKD patients (pre-dialysis, hemodialysis, peritoneal dialysis, and transplantation), to synthesize a holistic and comprehensive view within this field of study. Hence, the authors intend to evaluate the current state of literature targeting the CKD population which includes the caregivers caring for pre-dialysis, dialysis, and transplantation patients. Therefore, the objective of this scoping review was to examine the interventions implemented among the caregivers caring for patients diagnosed with CKD and its effectiveness in alleviating the caregiver burden.
Research Questions
What interventions have been implemented among the caregivers of CKD patients in reducing their caregiver burden?
What is the effectiveness of these interventions in alleviating the caregiver burden among the caregivers of CKD patients?
Method
Research Design
The authors used a scoping review methodology to summarize the research findings from a variety of sources as well as to identify the research gaps in the existing literature (Arksey & O'Malley, 2005). A scoping review is a type of evidence synthesis which the objective of identifying and mapping relevant evidence that meets the pre-determined inclusion criteria related to the topic, context, concept, or issue. The research question guiding the scoping review is typically broader than a systematic review (Peters et al., 2021). Also, the present review utilized the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist as a reporting standard (Tricco et al., 2018) in order to enhance the transparency and uniformity as well as to improve the quality and value of the scoping review (Tricco et al., 2018). The PRISMA-ScR is the most updated and advanced standard for scoping reviews which it is mainly based on the PRISMA checklist for systematic review, Joanna Briggs Institute (JBI) critical appraisal checklist, and other checklists for conducting the scoping review (Tricco et al., 2018). The PRISMA-ScR is a supplementary checklist to encourage thorough reporting of methods and findings that may be used in conjunction with other methodological guidelines (Arksey & O'Malley, 2005; Levac et al., 2010; Peters et al., 2015). Therefore, for the methodological approach, the authors followed the methodological framework for scoping studies by Arksey and O'Malley (2005). The authors undertook the following steps in the scoping review based on Arksey and O'Malley’s (2005) framework: (1) identifying the research question, (2) identifying the relevant studies, (3) selecting the relevant studies, (4) charting the data, and (5) collating, summarizing, and reporting the results.
Eligibility Criteria
Studies were included if they fulfilled the inclusion criteria (Table 1). The included studies must be modeled as intervention studies aimed at alleviating caregiver burden, specifically focusing on informal caregivers of patients with CKD. Studies that were not intervention studies on caregiver burden were excluded from the scoping review. The eligibility of the studies was reviewed accordingly based on their title and abstract by utilizing the EndNote 20 reference management software (Clarivate Analytics, 2021). The included studies were examined through their full articles by two authors (SYC and NI) independently to determine if the included articles were relevant to the research questions, based on the suggestion by Arksey and O'Malley (2005). Any disagreements were discussed and resolved through discussion and consensus with the third reviewer (CSS) (Levac et al., 2010).
Inclusion and Exclusion Criteria.

Information Sources and Search Strategy
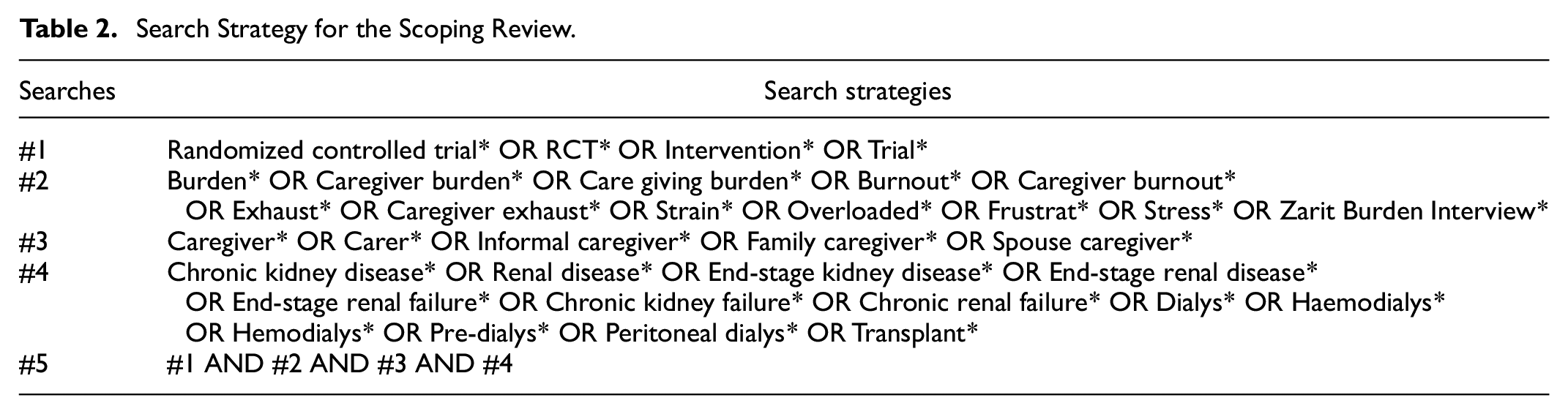
Four major citation databases (i.e., MEDLINE, Cochrane Library, PubMed, and Web of Science) were searched in the timeframe of February 2022 by authors (SYC and NI) to identify relevant studies. The searches included all relevant citations from the year 2008 up until the year 2022. This is to prevent overlapping studies reported in the study by Tong et al. (2008). Using Boolean operators, turnication, and Medical Subject Headings (MeSH) terms respectively in each database’s indexing references (Dinet et al., 2004), synonymic keywords were searched in each database (Table 2). Forward and backward citation from the included studies was also performed to search for potential studies.
Search Strategy for the Scoping Review.
Study Selection and Data Charting
The retrieved studies were exported into the EndNote 20 reference management software (Clarivate Analytics, 2021) and duplicates were automatically removed using the software. Data extracts for the included studies were performed independently by two authors (SYC and NI) and proofread by another author (CSS). Any disagreements and confusion during data extraction were discussed with the third author (CSS) and resolved through discussion (Levac et al., 2010). In the data charting process, two authors (SYC and NI) have collectively involved in constructing the data-charting form in order to identify the variables that should be extracted from the literature which helped to answer the research question. The following characteristics were extracted from the included studies: author(s), year, country, the objective of the study, study design, target population, sample size, mean age, intervention design, methods, and components, length of intervention, outcome measures, and study outcomes. The included studies did not have to undergo quality assessment as suggested by Arksey and O'Malley (2005) and Munawar et al. (2020).
Results
Search Results
Through the initial screening of databases, the authors identified 757 articles related to the search terms as shown in Figure 1. After the removal of duplicates using the Endnote 20 software (n = 353), a total of 404 articles were retrieved for further assessment. The eligibility of the studies was screened through their titles and abstracts; 295 articles were excluded, whereas 109 articles were retrieved for full-text review. The full-text articles were assessed by two authors (SYC and NI) and only nine articles were included in the scoping review. The other 100 articles were excluded due to reasons of either not being an intervention study, interventions implemented were not catered toward the caregivers or their caregiver burden, or lastly, articles were limited to only abstract review.
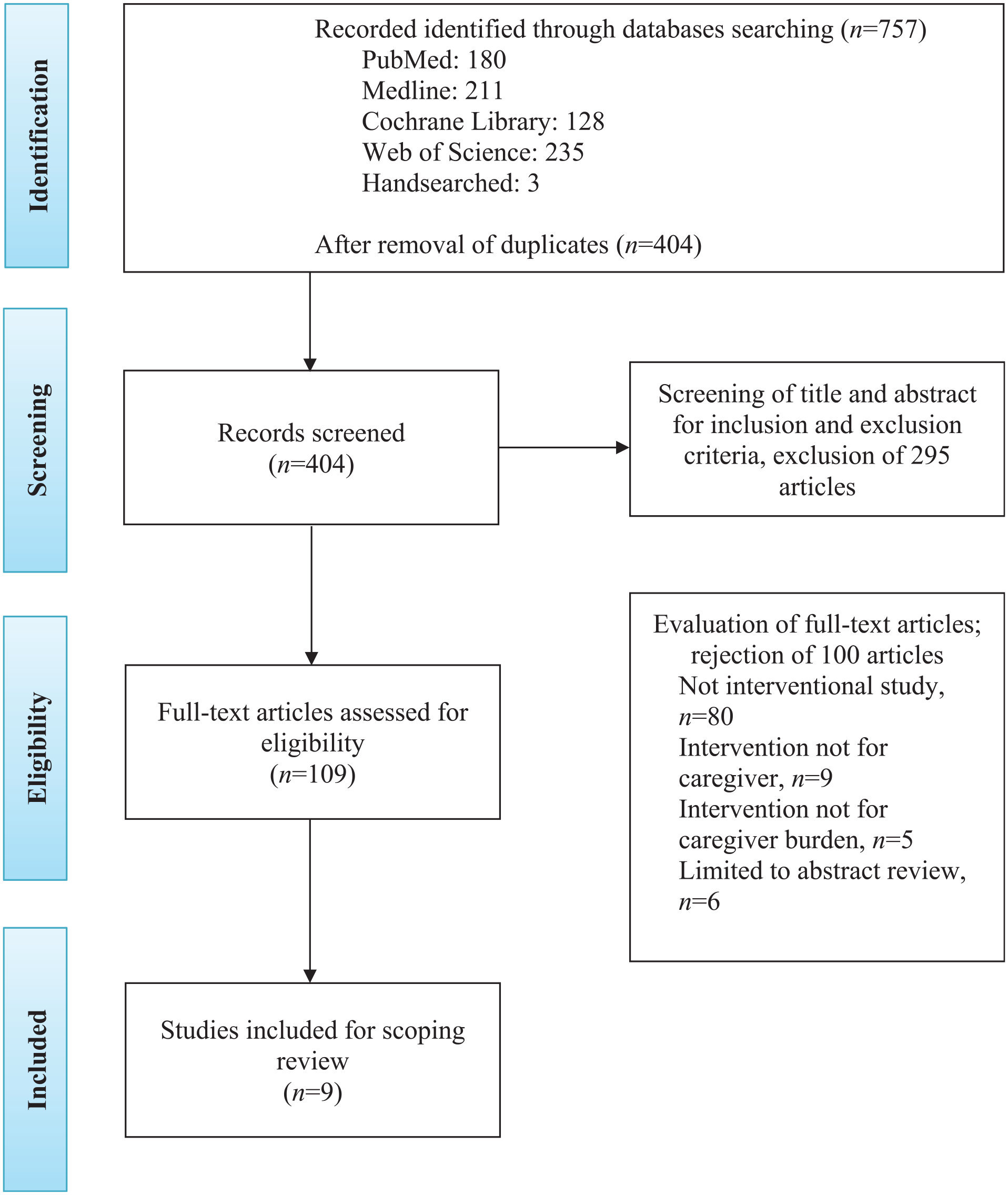
PRISMA flow diagram of the literature screening process.
Description of Studies
A summary of studies included in this scoping review is shown in Table 3. Most of the included studies were randomized controlled trials (RCTs) (n = 6) (Bahrami et al., 2019; Chan et al., 2016; Ghane et al., 2016; Maslakpak et al., 2019; Rabiei et al., 2020; Sotoudeh et al., 2019) and quasi-experimental studies (n = 3) (Alnazly, 2018; Hosseinigolafshani et al., 2020; Mollaoğlu et al., 2013). The included studies were conducted in Iran (n = 6) (Bahrami et al., 2019; Ghane et al., 2016; Hosseinigolafshani et al., 2020; Maslakpak et al., 2019; Rabiei et al., 2020; Sotoudeh et al., 2019), Jordan (n = 1) (Alnazly, 2018), Turkey (n = 1) (Mollaoğlu et al., 2013), and Hong Kong (n = 1) (Chan et al., 2016) and were published between 2013 and 2020.
Characteristics of the Included Studies (n = 9).
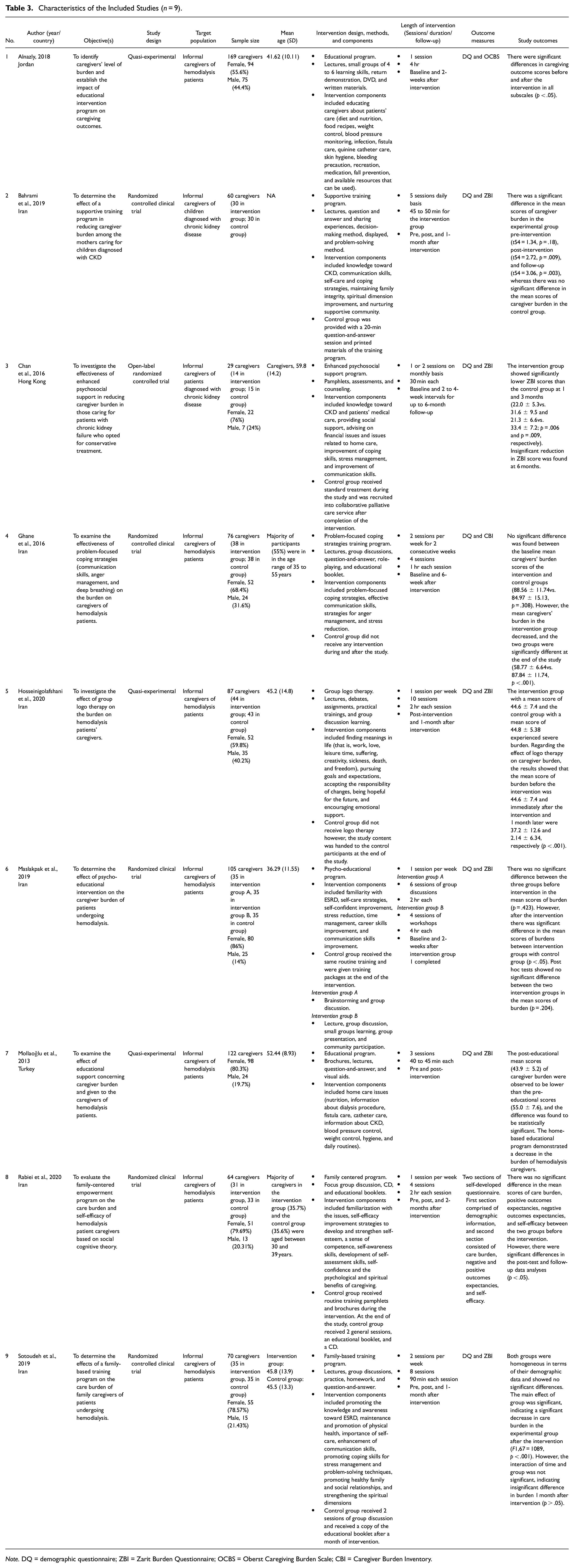
Note. DQ = demographic questionnaire; ZBI = Zarit Burden Questionnaire; OCBS = Oberst Caregiving Burden Scale; CBI = Caregiver Burden Inventory.
Population Characteristics
The target population was caregivers of CKD patients as summarized in Table 3. A majority of the included studies (n = 7) primarily focused on the caregivers of CKD patients (Alnazly, 2018; Ghane et al., 2016; Hosseinigolafshani et al., 2020; Maslakpak et al., 2019; Mollaoğlu et al., 2013; Rabiei et al., 2020; Sotoudeh et al., 2019), meanwhile, the remaining studies (n = 2) involved dyadic samples, that is, CKD child patients with their mothers as the caregivers (Bahrami et al., 2019) and CKD adult patients and their caregivers (Chan et al., 2016). A total sample of 782 caregivers of CKD patients was included in this scoping review and the majority of them were female. The caregivers’ age ranged between 30 and 59 years old.
Description of Interventions
A variety of intervention programs were utilized to reduce caregiver burden, presented in Table 3. The intervention programs included in this scoping review were educational programs (n = 3) (Alnazly, 2018; Maslakpak et al., 2019; Mollaoğlu et al., 2013), supportive programs (n = 2) (Bahrami et al., 2019; Chan et al., 2016), family-centered programs (n = 2) (Rabiei et al., 2020; Sotoudeh et al., 2019), and psychological interventions (n = 2) (Ghane et al., 2016; Hosseinigolafshani et al., 2020). Different approaches or methods were used across the studies to carry out the intervention, such as short slide-based lectures, small group learning, return demonstration, visual aid (DVD, pictures, figures), written materials, question-and-answer, pamphlets/ booklets, assessments, counseling, group discussion, role-playing, debates, assignments/ homeworks, practice, presentation, and community participation. In one of the studies, a brainstorming technique was utilized to improve group discussions (Maslakpak et al., 2019). The components included in the interventions were mostly emphasizing knowledge and awareness toward kidney related disease, educating caregivers on patients’ care, improvement of communication skills, enhancement of self-care and coping strategies, improvement of the spiritual dimension, and stress management. In terms of length of interventions across the included studies, they ranged from one session to six sessions, with each session lasting from 30 min to 4 hr. The control group in the seven studies received standard treatment and they were given materials of the training program and/or received intervention such as question-and-answer session, group discussion, or collaborative palliative care service after the study concluded. On the other hand, Alnazly (2018) and Mollaoğlu et al. (2013) did not report any related information related to the control group due to the reason that these studies implemented their interventions solely on one group of caregivers. The followed-up assessments for caregiver burden ranged from 2 weeks to 6-months across the included studies. Four studies reported that palliative care nurses/nursing students, social workers, nephrologists, psychiatric nurses, hemodialysis nurses, or clinical psychologists were the ones being responsible for implementing the intervention programs (Chan et al., 2016; Ghane et al., 2016; Hosseinigolafshani et al., 2020; Rabiei et al., 2020). Alternatively, interventional programs in the remaining studies were conducted and regulated by the researchers themselves.
Burden of Care Measurement
Three types of tools were used to assess caregiver burden across the included studies: Zarit Burden Interview (ZBI), Oberst Caregiving Burden (OCBS), and Caregiving Burden Inventory (CBI). The most common scale used to assess care burden among the caregivers is ZBI which is translated into various languages, that is, Chinese (Chan et al., 2016), Persian (Bahrami et al., 2019; Hosseinigolafshani et al., 2020; Maslakpak et al., 2019; Sotoudeh et al., 2019), and Turkish (Mollaoğlu et al., 2013), to conform with the cultural standards of the respective countries. Contrarily, Alnazly (2018) and Ghane et al. (2016) have utilized the Arabic version of OCBS and Persian version of CBI, respectively in examining the caregiver burden. Alternatively, a self-developed questionnaire comprised of care burden, negative and positive outcomes, and self-efficacy, was used in the study conducted by Rabiei et al. (2020) (Table 3). The caregivers who experienced a high care burden whilst caring for patients diagnosed with CKD, they have reported higher scores in the ZBI (Chan et al., 2016), OCBS (Alnazly, 2018), and CBI (Ghane et al., 2016) questionnaires.
Description of Study Outcomes
As summarized in Table 3, significant differences were reported across the studies for pre- and post-intervention. All the nine included studies reported that caregivers in the study experienced a decrease in caregiving burden after the intervention programs (Alnazly, 2018; Bahrami et al., 2019; Chan et al., 2016; Ghane et al., 2016; Hosseinigolafshani et al., 2020; Maslakpak et al., 2019; Mollaoğlu et al., 2013; Rabiei et al., 2020; Sotoudeh et al., 2019).
Among the included studies, three assessed the impact of educational intervention programs on the caregiving burden among caregivers of hemodialysis patients (Alnazly, 2018; Maslakpak et al., 2019; Mollaoğlu et al., 2013). A one-group pre-post study conducted by Mollaoğlu et al. (2013) reported that post-intervention mean scores (M2 = 43.9, SD2 = 5.2) of care burden were observed to be lower than pre-intervention mean scores (M1 = 55.0, SD1 = 7.6), therefore demonstrating that the educational intervention led to a reduction of caregiver burden. Similarly, Alnazly (2018) also revealed that at post-intervention, information and educational interventions had a substantial positive impact on caregiving outcomes. Likewise, a clinical trial of three groups utilizing psycho-educational intervention showed that care-training (intervention group 1) and care-based workshops (intervention group 2) for the intervention groups had significantly reduced the severity of caregiver burden (Maslakpak et al., 2019).
Additionally, significant differences in the mean scores of caregiver burden in the experimental group were found between the pre-intervention, post-intervention, and 1-month follow-up scores, indicating that supportive training programs can significantly reduce the care burden among mothers taking care of CKD children (Bahrami et al., 2019). Aligned with this finding, the enhanced psychosocial support intervention with follow up of up to 6 months conducted by Chan et al. (2016) reported only significant reductions in caregiver burden can be observed within the first 3 months of the intervention. Caregiver burden in the intervention group was significantly lower than the control group at 1-month and 3-month follow-ups. However, at the 6-month follow-up, the caregiver burden has increased slightly but was still lower than the baseline and control group scores.
On the other hand, studies conducted by Rabiei et al. (2020) and Sotoudeh et al. (2019) revealed that family-based training programs could significantly reduce the burden of care among caregivers of hemodialysis patients. A significant reduction in caregiving burden was observed in the experimental group immediately after the intervention (F(1,67) = 1089, p < .001). However, the findings for care burden were non-significant at the 1-month follow-up (Sotoudeh et al., 2019). In contrast, Rabiei et al. (2020) reported that the family-centered intervention program conducted led to a significant difference in the mean scores of care burden, positive outcomes expectancies, negative outcomes expectancies, and self-efficacy between the control and intervention groups immediately after the empowerment program and at the 2-month follow-up after the intervention.
Furthermore, Ghane et al. (2016) also found that problem-focused coping strategies could lead to a reduction of burden among caregivers of hemodialysis patients. More than 80% of the family caregivers in the study demonstrated symptoms of severe caregiving burden, at 84.2% and 89.5% in the control and intervention groups respectively. After the problem-focused coping intervention, the mean scores of care burden decreased significantly in all domains for the intervention group with only 5.3% of participants being in the severe category of caregiving burden, whereas the percentage did not significantly change in the control group. Similar to the previous study, a study by Hosseinigolafshani et al. (2020) showed that caregivers in the control (M1 = 44.8, SD1 = 5.38) and intervention groups (M2 = 44.6, SD2 = 7.4) experienced severe burden. Nonetheless, after the group logo therapy, a decrement of caregiver burden could be observed immediately after the intervention (M1 = 37.2, SD1 = 12.6) and 1- month later (M2 = 2.14, SD2 = 6.34).
Discussion
This scoping review examined the types of interventions that have been implemented among the caregivers of CKD patients and its effectiveness in alleviating the caregiver burden. The included nine articles in the current review were conducted within the years of 2013 to 2020. The findings suggested that there were four main specifically-targeted interventions such as educational programs, supportive programs, family-centered programs, and psychological interventions that have benefited the caregivers of CKD patients in terms of reducing their care burden. Most of the caregivers in the scoping review were female and were spouses or children of the patients. This is because women are often regarded as the caregivers as they are more compassionate and empathetic along with having the ability to form closer relationships with the patients as compared to men (Adejumo et al., 2019). At the same time, the studies were predominantly from the Asia region (Iran, Jordan, Turkey, and Hong Kong) and this may probably be due to the collectivistic nature of the Asian culture. The main tenets of collectivism are interdependence and community solidarity (Levine & Hogg, 2009). In that case, caregiving in collectivistic societies is greatly embedded in the sociocultural beliefs revolving around familial obligations (Pyke & Bengtson, 1996). Hence, the spouses or children of the patients are likely to be the primary caregivers to the patients in view of their collectivistic nature.
Based on the review findings, the educational interventional program was reported to be successful in reducing the care burden among caregivers of CKD patients (Alnazly, 2018; Maslakpak et al., 2019; Mollaoğlu et al., 2013). Similarly, the results are consistent with other chronic illnesses such as Alzheimer’s disease, stroke, mental illness, cancer, and heart failure as the caregivers were reported to have reduced care burden after being exposed to educational programs (Ali Desouki et al., 2019; Carrillo et al., 2020; Etemadifar et al., 2014; Farahani et al., 2021; Hsu et al., 2017; Navidian et al., 2012; Sadeghmoghadam et al., 2020; Tanrıverdi & Ekinci, 2012; Tawfik et al., 2021). In contrast, past studies conducted by Liljeroos et al. (2017) and Rodríguez-Gonzalo et al. (2015) amongst the caregivers of patients with heart failure and hospitalized dependent patients, respectively, revealed that educational intervention was not statistically significant in decreasing care burden. Therefore, educational intervention programs have to be specific and carefully catered to the caregivers of different types of chronic illness in order for the intervention to be effective in alleviating caregiver burden. A precisely tailored educational intervention can help educate and equip caregivers with the knowledge and necessary skills, thus leading to less fatigue and positive outcomes from caregiving (Mollaoğlu et al., 2013; Revenson et al., 2016).
In terms of the effectiveness of diminishing caregiver burden, supportive training programs were found to be helpful among caregivers of CKD patients as stated in past studies by Bahrami et al. (2019) and Chan et al. (2016). Likewise, supportive-approach interventions are effective to be applied amongst the caregivers of multidisciplinary diseases as evidence existed, supporting the positive findings as reported by Arbabi et al. (2021), Etemadifar et al. (2014), Farahani et al. (2021), and Rezaee et al. (2017) among the caregivers of heart failure, stroke, Thalassemia disorder, and chronic lung disease. Caregiving is a very stressful and demanding responsibility (Ghane et al., 2016); therefore, through the implementation of supportive interventions such as counseling and support groups, caregivers can share their thoughts and experiences with the experts and/or a group of people with similar experiences as well as morally support each other to cope with the caregiving role. This leads to positive outcomes in caregiving and psychosocial well-being.
Previous literature also reported that family-based training programs could significantly lessen the burden of care among caregivers of hemodialysis patients (Rabiei et al., 2020; Sotoudeh et al., 2019). Consistently, past studies also reported that family-approach interventions are effective in reducing the care burden among caregivers of patients with chronic illnesses such as epilepsy, cancer, dementia, and stroke (Deyhoul et al., 2020; Heidari et al., 2018; Pahlavanzade et al., 2014; Pahlavanzadeh et al., 2010). Concurrently, family-centered intervention programs can reduce the stress, anxiety, and depression levels of the caregivers (Etemadifar et al., 2018). In general, family-approach interventions embrace the perspective of both patients and their caregivers (Gilmer, 2002). Caregiving involves two parties: the patients and their caregivers, therefore, it is important to incorporate patients’ perspectives in the implementation of intervention programs for caregivers. The positive findings received for family-based programs suggested that this intervention can lead to improvements in caregivers’ physical and psychological well-being. Additionally, with the flexibility of family-based intervention programs, it could be easily incorporated with other types of intervention programs such as supportive or educational-based interventions, thus leading to holistic and comprehensive interventions aimed at mitigating the impacts of caregiver burden and enhancing caregivers’ quality of life.
Apart from that, psychological interventions such as coping strategies and logo therapy have also been suggested to be useful in reducing the caregiver burden among dialysis patients (Ghane et al., 2016; Hosseinigolafshani et al., 2020). Several studies have investigated the effectiveness of coping strategies on the caregivers of patients with chronic illnesses including dementia, cancer, and heart failure and these studies have demonstrated similar positive impacts (Chen et al., 2015; Etemadifar et al., 2014; McMillan et al., 2006; Porter et al., 2011). Based on the findings, coping interventions could help the caregivers to minimize their demanding responsibilities and tolerate their stressful situations, therefore enabling them to have better control over their lifestyle and time management. In addition, the use of effective coping skills significantly helps in reducing the care burden, thus improving the physical health and psychological well-being of caregivers (Kazemi et al., 2021). Meanwhile, logo therapy has been applied amongst patients with cancer, and positive effects on their quality of life, anxiety, hope, and resiliency have been reported (Ebrahimi et al., 2014; Kang et al., 2008; Mohabbat-Bahar et al., 2014; Nader et al., 2019). Logo therapy focuses on the meaning of life and advocates that the attempt to find meaning is one of the most powerful motivator factors (Morgan, 2013). One of the main objectives of logo therapy is the creation of hope in an individual, which is a positive motivation that focuses on a clear goal for life (Schulenberg et al., 2008). Hence, logo therapy could help caregivers to seek meaning in their lives, encouraging them to remain optimistic and hopeful toward their life despite the demanding caregiving tasks they bear.
Based on the past literature reviewed in the current study, four types of interventions (educational, supportive, family-based, and psychological) were utilized by the researchers in alleviating the caregiver burden among the caregivers of CKD patients. However, with the distinctive types of interventions implemented among the caregivers and the heterogeneity of the study population included in the current study, there is insufficient evidence to conclude a general framework for the overall study interventions reviewed in the study. At present, the most promising interventions are those consisting of psychosocial (supportive, family-based, and psychological) interventions proposed by Bahrami et al. (2019), Chan et al. (2016), Ghane et al. (2016), Hosseinigolafshani et al. (2020), Rabiei et al. (2020), and Sotoudeh et al. (2019). According to the study interventions, the psychosocial interventions with follow-up studies were effective in reducing the caregiver burden among the CKD caregivers with evidences suggesting that there was a significant decline in caregiver burden between the baseline, post-intervention, and follow-up studies. However, these interventions are unable to be generalization to the caregivers caring for peritoneal dialysis patients since there is a lack of evidence among this population. The reason is that the caregivers caring for hemodialysis and peritoneal dialysis patients along with the caregivers caring for patients diagnosed with CKD greatly differ from one another, hence, the interventions conducted among the caregivers of hemodialysis and CKD patients could not be imposed among the caregivers of peritoneal dialysis patients. Also, as there was insufficient evidence to confirm the benefit of interventions apart from reducing their caregiver burden and the past interventions mainly highlighted on the caregivers of hemodialysis and CKD patients, thus, the authors are unable to conclude a recommendation for the practice.
Strengths and Limitations
This review paper highlights the effectiveness of intervention programs in alleviating caregiver burden. The findings of the review provided consistent results across the different types of intervention used on caregivers of CKD patients due to the similar nature of study design and data collection instruments. Furthermore, the experimental study design used in the included papers is considered as the golden standard of research due to its ability to deliver reliable evidence and eliminate most types of biases in the study. Alternatively, there are several limitations within this scoping review. This review did not cover any gray literature; therefore, the authors could have missed prospective intervention studies that were not peer-reviewed for publication. The exclusion of intervention studies published in other languages or without English language translation might lead this review unable to have a comprehensive review of caregiver burden. Nevertheless, future studies should consider conducting systematic reviews and meta-analyses with more included studies within this field of knowledge to obtain a better comprehension of the interventions that would be beneficial for caregivers of patients with CKD.
Conclusion
Evidence suggested that these interventions showed significant results in reducing the care burden of caregivers of CKD patients regardless of the treatment modality. As a matter of fact, caregiving is a very stressful task and often causes a deterioration in the well-being of the caregivers. In this regard, this review could be used as evidence of the successful implementation of four types of interventions aimed at alleviating care burden among CKD caregivers. However, a general framework could not be drawn from the interventions study as well as insufficient evidence to propose a recommendation for the practice due to the lack of evidence supporting the intervention to be implemented among the caregivers caring for peritoneal dialysis patients. Nevertheless, the insights reported in the review could be served as prospective references to mental health professionals and policymakers to formulate an intervention program that caters to the caregivers of peritoneal dialysis patients.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440231178703 – Supplemental material for Interventions to Reduce Caregiver Burden Among Caregivers of Chronic Kidney Disease (CKD) Patients: A Scoping Review
Supplemental material, sj-docx-1-sgo-10.1177_21582440231178703 for Interventions to Reduce Caregiver Burden Among Caregivers of Chronic Kidney Disease (CKD) Patients: A Scoping Review by Sin Yee Chu, Norhayati Ibrahim, Noh Amit, Abdul Halim Abdul Gafor, Rozmi Ismail, Kai Wei Lee and Ching Sin Siau in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was supported by the Ministry of Higher Education of Malaysia (MOHE) under the Fundamental Research Grant Scheme (FRGS) [FRGS/1/2020/SS0/UKM/02/1].
Ethics Statement
The study was approved by the Ethics Committee of the National University of Malaysia (UKM) [UKM/PPI/111/8/JEP-2021-078].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.