
Abstract
HIV/AIDS scourge remains high in most countries of sub-Saharan Africa such as Nigeria, which is home to about 3.3 million HIV positive individuals and represents the second largest burden of HIV/AIDS care, treatment and demand worldwide after South Africa. Anti-retroviral treatment options though a welcome development, has increased the number of people living with this chronic illness, and most of them depend on family members for physical and emotional support. Traditional gender norms in Nigeria ensure that legitimately, women and girls are the first options for caregiving roles. This mandatory role has in turn imposed psychosocial disruption in the lives of female family members in Calabar, Nigeria. This descriptive study utilized convenient sampling technique, Zarit Burden Interview scale and semistructured questionnaires for data collection (260 respondents), and data analyses were achieved using SPSS16.0. The study showed that a significant (p < .05) proportion of women (91%) were involved in providing care, including children from 10 years and above. Caregivers had minimal social support which increased the burden they experienced. The need for policy that recognizes and supports female caregivers (“silent cornerstone”) to reduce burden and ensure high quality care of people living with HIV/AIDS (PLWHA) in Nigeria is advocated.
Introduction
Providing care to a sick family member is a tradition embedded in African culture. It is regarded as an age-old act of kindness, love and loyalty, which bind family members together (Asuquo, Adejumo, Etowa, & Adejumo, 2013; Smith & Segal, 2013). With sub-Saharan Africa accounting for 69% of people living with HIV, coupled with advancement in medical treatment and improvement in life expectancy, many more persons will assume caregiving role of people living with HIV/AIDS (PLWHA; Singh, Chaudoir, Escobar, & Kalichman, 2011; UNAIDS, 2012). Studies have shown that most HIV infected individuals return to their homes for care and psychological support (Bachmanna & Booysenb, 2006; Global Coalition on Women and AIDS, 2004; Grunfeld et al., 2004; Kipp, Nkosi, Laing, & Jhangri, 2006; VSO, 2006; WHO, 2005). According to Takamura and Williams (1998) in our society, family caregivers often go unnoticed except by those who depend on their care. Similarly, Abasiubong, Bassey, Ogunsemi, and Udobang (2011) asserted that while resolute efforts are made to improve the quality of life of PLWHA in many countries, little or no acknowledgment is given to the supportive role of caregivers or the effect the role is having on them. Habid and Rahman (2010) reported that family caregivers are physically, psychologically and socially disabled due to caring for PLWHA.
Health systems in most developing countries do not have the capacity to provide long-term care and support to PLWHA, and patients are discharged without contact with family caregivers (Tshililo & Davhana-Maselesele, 2009). Patient discharge is based on the implicit assumption that, family members are always available to provide care at home to the dependent ill, without adequate educational preparation of family members on their expected roles (VSO, 2006). Reinhard, Given, Petlick, and Bemis (2008) observed that a serious health care gap exists as health professionals’ fail to recognize caregivers as “hidden” patients even with numerous research evidence on adverse physical and mental health consequences from physically and emotionally demanding work of caregiving. The physical tasks performed by the caregivers transcend minor to complex tasks, which is similar to those carried out by paid health or social service providers. These impart a great degree of burden on the caregivers especially, as they combine the caregiving services with their official roles in the society. Caregiving has increased the burden of care on many households particularly the females, by worsening their economic status and subjecting them to imminent poverty. The need for heal thcare system and government to promulgate policies that will support female caregivers and also enhance quality of care to PLWHA in Nigeria becomes imperative. This study therefore highlights the extent of burden experienced by female caregivers compared to male counterparts and the support available to all caregivers of PLWHA in Calabar Municipality, Nigeria.
Women and Burden of Care
Women constitute about 50% of the people living with HIV today worldwide (WHO, 2013). In 2007, the prevalence of HIV infection had been on men than women (UNAIDS, 2008), but with the turn of events women now bear the burden of this devastating disease more than men (WHO/UNICEF/ UNFPA/World Bank, 2010). In sub-Saharan Africa, women constitute 60% of people living with HIV and the proportion of women living with HIV has been increasing in the last 10 years (WHO, 2013). These figures vindicate the words of Lewis (2005) that HIV/AIDS in Africa has a “female face.” Apart from biological vulnerability of women to HIV, the African traditional gender norms stipulate caregiving as female normative role where women and girls in the various communities become caregivers, while still needing care themselves, and possibly being HIV positive also (UNAIDS, 2008; UNIFEM, 2005; VSO, 2006). These “traditional gender norms” also exclude men and boys becoming caregivers, exacerbating the burden for females. Many women and girls have left work and school to provide care, and most have taken on this role in addition to their existing reproductive and primary roles as housewives/housekeepers (VSO, 2006).
Encouraging care provision in homes is regarded as a cost-effective strategy for governments and the private sector, but little consideration is given to the physical, emotional and economic costs to households and the caregivers who take on the additional burdens, many of whom are often poor and living below US$ 1.00 to US$1.25 per day (Asuquo, Etowa, & Adejumo, 2013; United Nations, 2012; United Nations Development Progress, 2013). Mbirimtengerenji (2007) asserted that not only does correlation exist between poverty and HIV infection but HIV remained the exact outcome of poverty in the sub-Saharan region with sexual trade, migration, polygamy, and teenage marriages as its predictors. According to VSO-RAISA (2007) and UNAIDS (2008), the impact of HIV and burden of care is greater in resource-poor settings, particularly for rural and grass-root caregivers. UNAIDS (2008) reported that women in Africa make up 70% of the world’s poor and two thirds of the world’s illiterate and accounts for two thirds of all caregivers for people living with HIV in Africa. The unique contribution in ameliorating the impact of HIV is not only peculiar to African women alone. Global Coalition on Women and AIDS (2004) asserted that about 90% of the care due to HIV infection is provided at home by women and girls in addition to other tasks they already perform. Arno (2002) and Family Care Alliance (2003) have also reported that women caregiving provides the backbone of support to the complex system of long-term care and the value of the informal care that women provide ranges from US$148 billion to US$188 billion annually. Although annual monetary value of unpaid caregiving in Nigeria has not yet been quantified, the global estimated value of unremunerated work by women is 11 trillion dollars (UNAIDS, 2008).
Forever Young Information (FYI, 2013) affirmed that females assume caregiving role at a young age and take an active interest in their love one’s health and maintain this role as they grow older. Between the ages of 30 and 55 years, women become primary caregivers in Ontario households and assume the responsibility of health care decisions for their children, siblings, spouses and parents (FYI, 2013). Canadian Caregiver Coalition (2013) noted that about 4 to 5 million people serve as caregivers with the majority being women and they provide more than 80% of the care needed by HIV individuals. These “long-term” conditions and constitute more than US$5 billion of unpaid labor annually to the health care system. Hence, family caregivers (women) are the invisible backbone of the health and long-term care system which signify need for support to reduce negative consequences on their health.
Caregiving and Support
Caregiving in the Nigerian society though associated with some rewarding experiences, is laden with chronic life strains from excessive job responsibilities. Caregivers attempt to balance caregiving with their other activities such as work, family and leisure, to meet the demands of daily living. Inability to strike a balance results in experiences of negative reactions such as increased sense of burden (Argimon, Limon, Vila, & Cabezas, 2004; Pavalko & Woodbury, 2000; Stephens, Townsend, Martire, & Druley, 2001). According to Reinhard et al. (2008) both negative and positive consequences of providing care may exist simultaneously. The negatives consequences emanate from excessive life stressors which require daily readjustments, which if not may result in interference with performance of role-related activities (Thoits, 1986). Excessive caregiving stress could result in physical, social and emotional consequences which manifest as low perception of health status, perceived high stress levels, deep unhappiness, social anxiety, depression and induced changes that could degenerate to heart disease, hypertension, increase rate of physiological illness and suppressed immune responses (Abasiubong et al., 2011; ANON, 2009; Kipp et al., 2006; Kurtz, Kurtz, Given, & Given, 2005; Montgomery, Rowe, & Kosloski, 2007; National Alliance for Caregiving (NAC) & AARP, 2009; Zarit, 2004).
The need to support caregivers’ well-being and that of care recipient becomes imperative especially with the advent of antiretroviral therapy. Supporting caregivers’ entails providing coping assistance, or involving significant others in an individual’s stress-management efforts (Hornillos & Crespo, 2011; Thoits, 1986). Turner and Street (1999) asserted that support could be through instrumental aid (actions or materials provided to ensure attainment of role responsibilities), socioemotional aid (infer the assertions or demonstrations of love, caring, esteem, sympathy, and group belonging), and informational aid (communications of information that makes life challenges easier). These three measures will help the caregiver to change the situation, meaning attached to the situation, emotional reaction to the situation, or to change all three thereby reducing the perceived burden (Thoits, 1986). Thoits added that social support buffers the detrimental effects of caregiving stress.
Female caregivers of PLWHA who combine caregiving with their reproductive and productive activities, need support for continual adaptation to task changes and to reduce the burden of care on them and enhance quality care to the care recipient. The conceptualization of support as coping strategy or the active involvement of significant others in the caregivers’ ability to manage stress is the principal theme that is exemplified in this study.
In this regard, the level of burden experienced by all caregivers of PLWHA was examined to (a) compare the degree of perceived burden of caregiving work experienced by female and male caregivers, (b) assess the duration of care by both male and female caregivers, (c) assess the availability of support to caregivers, and (c) the willingness of caregivers to continue caregiving in the future.
Materials and Method
Location of the Study
The study was carried out in Calabar Municipality, Cross River State of Nigeria from June to December 2009. In Calabar, there exist the University of Calabar Teaching Hospital (UCTH; a tertiary institution) which is a referral center to primary and secondary health care facilities in the region. It also provides inpatient and outpatient services as well as collaborates with nongovernmental organizations (NGOs) in the treatment of PLWHA from rural/urban areas and neighboring country. The hospital has been selected by the Federal Government of Nigeria as one of the centers for the management of PLWHA. The study was informed by the high HIV prevalence of 10.4% at the study site (Asuquo, Etowa, & Adejumo, 2013; Federal Ministry of Health [FMOH], 2011).
Study Design and Participants
The study was a cross-sectional descriptive research which utilized convenient sampling technique to generate data from 260 participants who were primary caregivers to PLWHA. The study participants were identified through HIV clinic of the UCTH where some of the researchers worked as employees (Clinical Instructors) and the visitation list of a voluntary caregiver of PLWHA, an NGO (Positive Development Foundation, Calabar, Nigeria). Information letter and invitation for willing participants were posted at UCTH and the NGO office where willing participants contacted the researcher. The participants who met the inclusion criteria and were willing to participate in the study were contacted. As described previously (Asuquo, Etowa, & Adejumo, 2013), the inclusion criteria were: being a caregiver for more than one month and also caring for PLWHA patient with some functional abilities as a family member. The age of caregiver’s cuts across all age brackets, which include children under the age of 16 (Becker, 2007; Robson, Ansell, Huber, Gould, & Van Blerk, 2006), especially in sub-Saharan with high prevalence of HIV/AIDS. There were 299 potential caregivers, who met the inclusion criteria of being primary caregivers, but only 260 completely filled their questionnaires and 11 caregivers did not know the diagnosis or ailment of their care receivers. Twelve (12) refused to participate while 16 did not complete their questionnaires. Being a primary caregiver involved participants who provided unpaid physical support such as helping in activities of daily living, shopping, food preparation, helping in administering medication, overseeing medical appointment, financial, and emotional support to PLWHA.
Confidentiality was ensured through deleting any contact information, retrieving and coding the questionnaires immediately they were completed. The study was submitted to the UCTH Ethics and Research Committee, who gave the approval for conducting the study. Consent was also obtained from the Managing Director of Positive Development Foundation who helped to identify PLWHA caregivers. Informed consent was also obtained from study participants following full description of the aims and objectives of study. Participants were appreciated for their time.
Instrument and Measures
Data was collected using structured questionnaires administered by the researchers themselves and through the help of trained field assistants. Some questionnaires were delivered to the respondents by face-to-face contact, while some were deposited with them to fill and return within one week. All the questionnaires were translated into Efik (the native language of the people) and back-translated into English by experts to ensure that there was no loss of meaning. The Efik (local dialect) version was administered to caregivers with little or no education. The structured questionnaires consisted of 41 items, 7 demographic variables, 22 from Zarit Burden Interview (ZBI) scale and 12 measuring social support. Measurements of the reliability of the instruments were achieved using test–retest method. The instruments were administered to 10 HIV caregivers in Calabar South. Two weeks later, the same instruments were administered on the same subjects. Their responses during the two occasions were correlated using Pearson product–moment correlation to obtain a reliability coefficient ranging from 0.85 to 0.96.
Demographics
The demographic variables consisted of seven items including information on age, marital status, occupation, highest educational qualification, household income level, number of people in the household, and duration of care. Duration of care was categorized into two levels to determine the extent of involvement with caregiving. Duration of care was predefined for the caregivers.
Caregivers Burden
Burden of care was assessed with the ZBI scale. 22 items validated ZBI scale with reliability coefficient ranging from 0.88 to 0.92. This scale is made up of 22 items which measures caregivers’ perceptions as caregiving demands, it reflects the degree of physical, emotional and social impact of caregiving on caregivers while providing care for PLWHA (Zarit, 2004). The respondents indicated the discomfort they experienced of particular items on a 5-point Likert-type scale ranging from 0 to 4. The total score ranged from 0 to 88 and a high score correlated with higher level of burden.
Support
A pilot tested structured questionnaire with a reliability coefficient of .85 to .96 was used to measure social support. The questionnaire consisted of 12 items which assessed the availability of support information, financial help, emotional support available to caregivers and help with caregiving. Respondents indicated the extent of support they received from each item on a 4-point Likert-type scale, ranging from lots of support, some support, very little support and no support.
Data Analysis
Data collected were analyzed using the Statistical Package for the Social Sciences (SPSS 16.0) software to generate the frequency and percentages of the values. By the application of inferential statistics (chi-square test), the level of significance was also determined at the p value of .05. The ZBI scale scores ranged from 0 to 88; 0 to 20 represented little or no burden; 21 to 40, mild to moderate burden; 41 to 60, moderate to severe burden; and 61 to 88, severe burden (Zarit, 2004). The support instrument was summed up into two, availability of support for “lot of support and some support,” lack of support for “very little support and no support.”
Results
Sociodemographic Characteristics
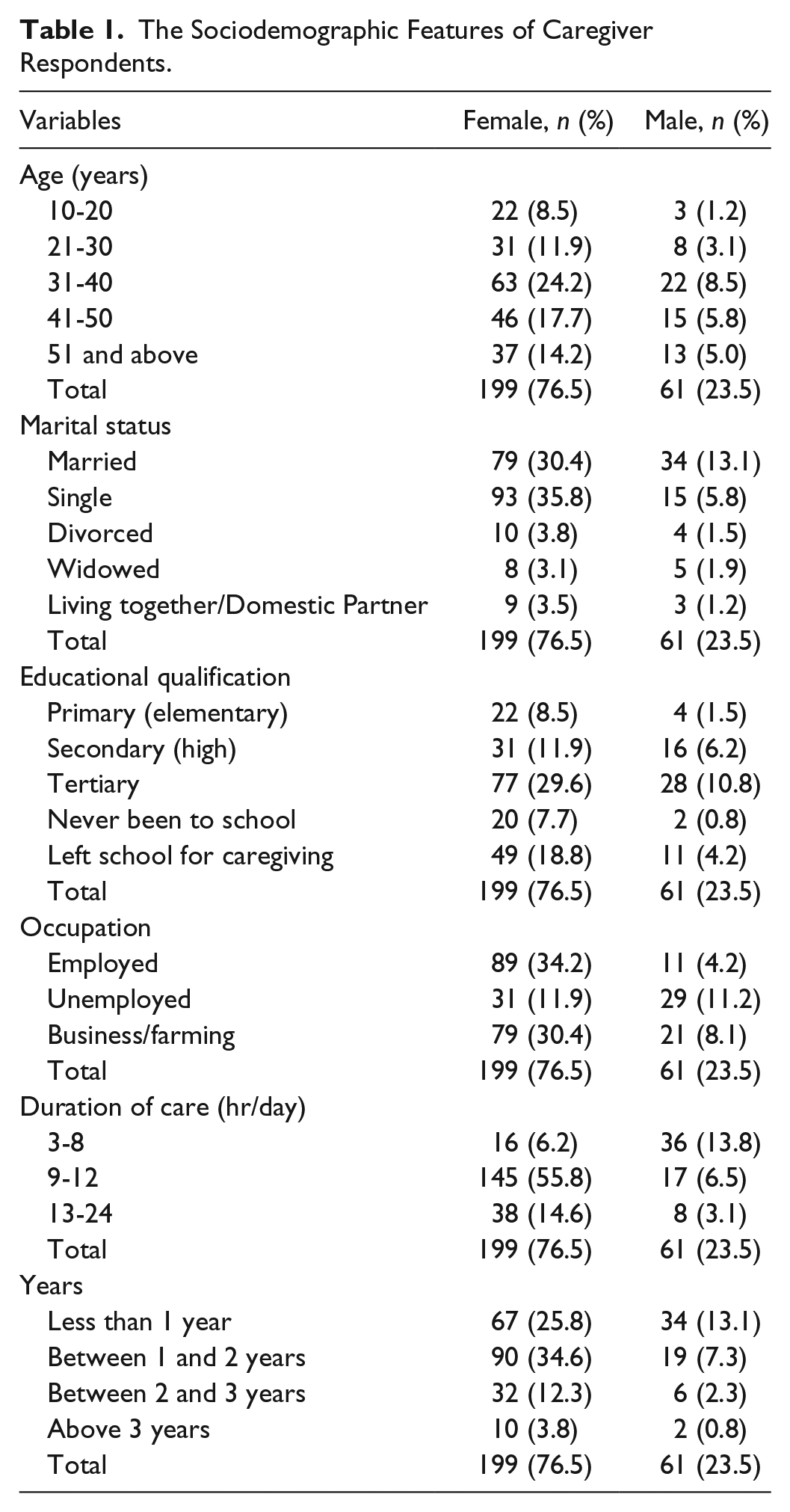
Table 1 shows the sociodemographic variables of 260 caregivers who participated in the study. The majority of the respondents were females 199 (76.5%) while 61 (23.5%) respondents were males who voluntarily took up the caregiving roles. Of the 260 respondents, 22 (8.5%) females and 3 (1.2%) males aged between 10 and 20 years, 31 (11.9%) females and 8 (3.1%) males aged between 21 and 30 years. The majority 63 (24.2%) females and 22 (8.5%) males aged between 31 and 40 years, 46 (17.7%) females and 15 (5.8%) males aged between 41 and 50 years while 37 (14.2%) females and 13 (5.0%) males aged between 51 years and above. The data also showed that majority of respondents were single females (93/35.8%), with tertiary education (77/29.6%) and were employed (89/34.2%). This study shows that 49 (18.8%) females left school to care for PLWHA (Table 1).
The Sociodemographic Features of Caregiver Respondents.
Duration of Care Among Caregiver
The study revealed that majority 162 (62.3%) respondents (145females and 17males) spent between 9 and 12 hr/day providing care to PLWHA. 52 (20.0%) respondents ((16 females and 36males) provided 3 to 8 hr of care, while 46 (17.7%) respondents provided 13 to 24 hr/day care to PLWHA (Table 1).
Majority 109 (41.9%) of the respondents (90 females and 19males) had provided care between 1 and 2 years, 101 (38.9%) respondents (67 females and 34 males) had been caregivers for less than 1 year, 38 (14.6%) respondents (32 females and six males) provided care for 2 to 3 years, while 12 (4.6%) respondents (10 females and two males) provided care for more than 3 years.
Household Income and the Number of People in the Household
The majority 130 (50%) of the respondents lived below a household income of US$6.00/day while only 15 (5.8%) lived with an income of US$14.00 and above. Also, the majority 153 (58.9%) lived in a household of about three to six members and only about 19 (7.3%) lived in a household of one to three persons (Table 2).
Household Income and the Number of People in the Household.

Gender Difference in the Level of Burden
Generally, the results revealed a level of burden ranging between 14 and 71 on ZBI Scale (Table 3); 49 (18.8%) respondents (females 39, males10) experienced no burden while providing care, 67 (25.8%) respondents (females 46 males 21) experienced mild to moderate level of burden, 93 (35.8%) respondents (females 69, males 24) experienced moderate to severe level of burden while 51 (19.6%) respondents (females 45, males six) experienced severe level of burden in providing care to PLWHA.
The Distribution of Burden on Zarit Burden Interview (ZBI) Scale.

The relationship between gender and caregivers burden assessed with students t test gave a calculated t test value of 1.27 and the tabulated value of 1.62 at p < .05, indicating a significant relationship between the levels of burden experienced by gender (Table 4).
The Relationship Between Gender and Caregivers Burden.

Note. T-test Cal. = 1.27. T-test tab. = 1.62, N = 260, p < .05.
Availability of Support to Caregivers
The availability of support was categorized into four sections, namely, providing information on practical and coping skills, financial assistance, help with caregiving and emotional support (Figure 1). Among the 260 respondents, 152 (58.5%) agreed to have received some form of support while 108 (41.5%) received no form of support at all. The form of support received included 6 (0.2%) information on practical and coping skills, 36 (13.9%) financial assistance, 72 (27.7%) help with caregiving, and 38 (14.6%) emotional support. Most caregivers perceived their role to be extremely stressful with adverse consequences on their health, which some form of support from individuals or government could have helped to ameliorate. There was no difference in the types of support by gender.
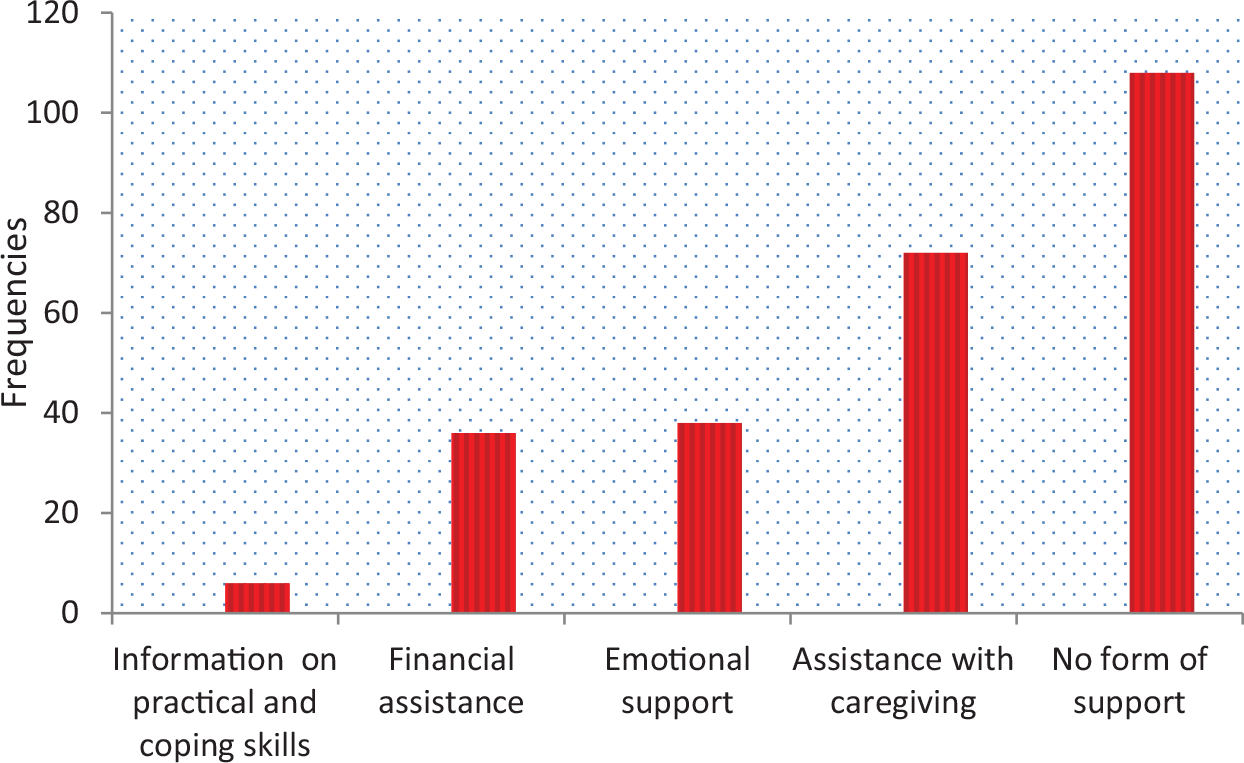
Assessing the extent of support to caregivers of PLWHA in Nigeria.
Willingness to Continue With Caregiving
Among the 260 caregivers, the majority 213 (81.9%) respondents (171 females and 42 males) expressed their desire to continue with caregiving, while 47 (18.1%) caregivers (28 females and 14 males) did not feel like continuing with caregiving role (Figure 2).

The caregiver’s willingness to continue in caregiving role.
Out of 108 respondents who received no support, 12 experienced no burden, 23 respondents experienced mild to moderate burden, the majority 37 respondents experienced moderate to severe burden while 36 respondents experienced severe burden. A chi-square value of 25.1 was obtained at p < 0.05, which showed a significant relationship between availability of support and caregivers burden (Table 5).
The Relationship Between Availability of Support and Caregivers’ Burden.

Note. Figures in parentheses are expected frequencies. χ2 Cal. = 25.1. χ2 Tab. = 7.81, df = 3, N = 260, p < 0.05 where “χ2 Cal.” and “χ2 Tab.” represents Chi square calculated and Chi square tabulated respectively.
Out of 52 respondents who provided care for 3 to 8 hr/day, the majority 28 experienced no burden, 10 respondents experienced mild to moderate burden, eight respondents experienced moderate to severe burden while six respondents experienced severe burden. Out of 162 respondents who provided care for 9 to 12 hr/day, 16 experienced no burden, 50 respondents experienced mild to moderate burden, the majority 73 respondents experienced moderate to severe burden while 23 respondents experienced severe burden. Among 46 respondents who provided care for 13 to 24 hr/day, five experienced no burden, seven respondents experienced mild to moderate burden, 12 respondents experienced moderate to severe burden while the majority 22 respondents experienced severe burden. A chi-square value of 80.0 was obtained at p < 0.05, which showed a significant relationship between duration of care and caregivers burden (Table 6).
The Relationship Between Duration of Care and Caregivers’ Burden.

Note. Figures in parentheses are expected frequencies. χ2 Cal. = 80.0, χTab. = 10.65, df = 6, N = 260, p <0.05.
Discussion
Caring for those with terminal diseases such as HIV/AIDS is intrinsically a demanding exercise that requires empathy, an attribute which is commonly found among the women (Okoye, 2012). This study showed clearly that the burden of care on AIDS affected households, rest more on women and girls than men. These are evident in the number of females who took up caregiving roles in this study compared with males. This is similar to UNAIDS (2008) report that caring for the sick in affected households is relegated to females thereby increasing the burden of care on females than males. This finding also corroborates male dominance in the Nigerian society that culturally assigns caregiving role to women. But in the absence of eligible females, the males are often engaged in the caregiving role. This traditional gender norm allows women and girls to provide care but creates the social barrier against men and boys becoming caregivers, exacerbating the burden for women and girls. This corroborates other reports that women are the primary caregivers in most households and societies (FYI, 2013; NAC & AARP, 2009; UNAIDS, 2008). Takamura and Williams (1998) observed that in most society, these caregivers often go unnoticed except by those who depend on their care. VSO (2006) asserted that the caregiver has a right to be valued, supported and compensated appropriately to ensure that the patient receive a high quality care. Primary caregiver sometimes pays a high price and lose opportunities, because providing care may entail sacrificing school or work to provide care or taking up caregiving role in addition to existing reproductive and household economic roles.
Apart from lost opportunities in caregiving, majority of caregivers experience high burden level as manifested in this study (Table 3). This indicates the degree to which caregiving endeavor impacts on emotional, physical health, financial and social life of the caregiver. The physical labor of attaining to all the activities of daily living, coupled with lack of resources to spend on their own medication, produces detrimental effects on the carer’s own health (Saengtienchai & Knodel, 2001). The physical and psychosocial impacts of caregiving on women’s well-being are rarely acknowledged, as most women often ignore their personal health concerns to consummate the challenges of caregiving (Asuquo, Etowa, & Adejumo, 2013; UNAIDS, 2008; VSO, 2006; WHO, 2003).
There was a significant relationship between the level of burden experienced and gender in this study. This is similar to Allegra (2012) report which asserted that women experienced more burden than men due to their tendency to perform more personal care tasks as primary caregivers and are less likely to obtain formal help. Without appropriate intervention, increased level of burden produces negative consequences which manifest as symptoms of anxiety and depression and induced changes that could lead to heart disease, hypertension, psychological worries, loneliness, increase rate of physiological illness and suppressed immune responses (Abasiubong et al., 2011; Asuquo, Etowa, & Adejumo, 2013; Bevans & Sternberg, 2012; Montgomery et al., 2007; NAC & AARP, 2009; Robison, Fortinsky, Kleppinger, Shugrue, & Porter, 2009). According to Takamura and Williams (1998), it is pertinent to perceive caregivers as potential patients and accord them the necessary support as little can be achieved when their well-being is jeopardized.
Female caregivers spend more hours and years in providing care (Table 2) than male counterparts as observed in this study. This finding is associated with traditional gender norms which appropriates caregiving to women and for the men to provide economically for their families, therefore spending less time in caregiving. This corroborates previous report (Gomo, 2008; VSO, 2006) that men’s low participation in caregiving are sociocultural since they are expected to provide financial spport for their families. Reinhard et al. (2008) affirms that caregiving is a day-to-day obligation and most family caregivers provide 8 or more hours of care per week, and one in five caregivers may provide more than 40 hr of care per week. This finding is comparable with Family Caregiver Alliance (2003) who affirmed that even when men provide assistance, female caregivers spend as much as 50% more time providing care than male caregivers. This study further revealed that providing care ranges from short period of time to full-time commitment and a significant relationship (p <0.05) exist between duration of care and caregivers burden (Table 6). This also agrees to other reports asserting that whether it is for a short period of time or over extended years, caregiving is a normative life challenge which exacerbates the burden of caregivers without adequate coping strategies (Cavanaugh, 1998; Chambers, Ryan, & Millar, 2001).
There was limited support to caregivers in terms of information on practical and coping skills, financial assistance, help with caregiving and emotional support to caregivers (Figure 1). Caregivers took up the caregiving role without educational preparation and in most cases unfamiliar with the type of care they must provide or the extent of care needed. The lack of support may be attributed to the low value placed on caregiving, especially when caregiving is dominated by females.
UNAIDS (2008) and VSO (2006) asserted that gender bias may play a significant role in the none recognition and low value assigned to the “care economy” which is part of the unremunerated work performed by women. The need to acknowledge and celebrate family caregivers as one of the notable strengths of our nation’s families and communities cannot be overemphasized as no one can afford to pay the costs of replacing all informal caregivers with paid personnel (Takamura & Williams, 1998). Chambers et al. (2001) emphasized that it is prejudice to assume that carers have necessary knowledge and skills to care for an ill relative without some form of support or training. Similarly, Rose (1997) affirmed that providing information on practical and coping skills plays important role in caregiver’s effective management of burden and any associated stress the caregiver may experience. The need to support caregivers is consistent with most literatures on support needs. UNAIDS (2008) and Saengtienchai and Knodel (2001) also agreed that without proper training on practical and coping skills, adequate information and supplies, there is the risk of exposure to communicable opportunistic infections. Fear of HIV contagion can cause considerable anxiety on the part of caregivers, especially if they are not well informed about the actual risks (Asuquo, Adejumo, et al., 2013).
This study also revealed a significant relationship (p < 0.05) between support and caregiver’s burden. Therefore, support in form of information and training on caregiving should be given to caregivers before the commencement of caregiving role. Therefore, with the global commitment to attain universal access to prevention, care, support and treatment for those PLWHA, the need to reflect on what these goals might mean in terms of burden on women and girls should be considered (VSO, 2006).
In spite of the high level of burden perceived by caregivers, many still showed the willingness to continue in caregiving role. This may be attributed to strict adherence to cultural expectation, fraternal love for the sick and sheer need. Observations akin to the role theory of Berg-Weger, McGartland Rubio, and Tebb (2000) suggest that caregivers strive to fulfill a normative expectation to avoid criticism by others. Okoye (2012) affirmed that this normative role in Nigeria is backed by persistent influence of traditional norms, values and behavior, practiced as deified and not routines. This also conformed to Davis (2012) empirical study on role theory, which affirmed that a person’s behavior is indirectly or directly influenced by the social environment. But willingness to continue with caregiving role depend on caregivers internalize coping behavior (McKee et al., 1999) and the patient’s symptom may play a critical role in accounting for levels of caregiver’s depressiveness or willingness to continue in caregiving role (Given et al., 2005). Majority of those that were not willing to continue with caregiving role fell among family caregivers that did not receive any form of support, spending more than 9 hr/day in providing care. This is similar to Asuquo, Adejumo, et al., (2013) and Habid and Rahman (2010) who asserted that with increased burden and limited support, caregivers experience serious burnout and are physically and psychologically disabled. UNAIDS (2008) and Zarit (2002) recommended the provision of social support and counseling before role assumption to alleviate burden of caregiving and enhance willingness to continue with role.
Conclusion/Recommendation
Over the past decade, improved antiretroviral regimens, concerns about the cost of inpatient care and consumer’s preferences have shifted HIV/AIDS care from hospitals to home and community settings. This shift has placed heavy burden on the family and friends of HIV positive individuals, and most of them had very little knowledge of HIV management or available resources. Strategies for counteracting caregiving stressors must be addressed by recognizing and supporting family caregivers as well as seeking measures to enhance involvement of male in family caregiving. This could be achieved through campaigns to create awareness on associated burden of care on women and the encouragement of equal distribution of household and caregiving responsibilities. The strengthening of health care systems to provide information on practical and coping skills to caregivers of PLWHA, will reduce the burdens that caregiving poses on them. The government should provide as a matter of urgency hospices where PLWHA can meet with medical professionals for advice. Counseling sessions should be organized regularly to present a forum where caregivers could air their problems and challenges encountered during caregiving services. The need also arises for the recognition of primary caregivers as potential patients, and the formulation of policy that recognizes and support female caregivers of PLWHA in Africa. This will ensure caregiver’s right to high quality care through the development of a standardized assessment format to assess caregivers during each hospital visit.
Limitation
This study was limited to caregivers of PLWHA in Calabar municipality. It was also not possible to identify households that were predominantly male or female controlled. The instrument used did not measure the HIV status of the caregivers.
Footnotes
Acknowledgements
The authors are grateful for information and support received from the Managing Director of Positive Development Foundation, an NGO in Calabar, Nigeria during the course of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: One of us (EFA) received study fellowship grant from the University of Calabar, Nigeria, to whom we are grateful.