
Abstract
This study examined the effects of perceived financial costs on caregiving burden experienced by family caregivers. The target population was family caregivers for older adults who were 65 years of age and older in Calgary, Alberta. Telephone interviews were conducted using a structured questionnaire, with a random sample of 340 family caregivers. The financial costs associated with family caregiving were a significant factor in caregiving burden, both for the male and female caregivers, even when controlled for most of the demographic characteristics of the caregivers, and the demographics, health, and caregiving needs of the care receivers. While caregiving is creating burden and financial consequences for family caregivers, the effects of financial costs should not be understood only in financial terms. Policies and programs to alleviate the financial burden and to provide social and financial support for these family caregivers are equally important for both family caregivers and their care receivers.
Introduction
Family caregivers for older adults provide care and support in health, social, emotional, and financial domains, particularly for those who are frail or suffer from chronic illness (Koh & MacDonald, 2006). While family caregivers often act as a social safety net for older care receivers (Lubben, 1988), research findings consistently indicate the associated caregiving burden that family caregivers experience (Braithwaite, 1996; Pakenham, 2001; Stolley, Reed, & Buckwalter, 2002). Family caregiving can be costly (Acton & Kang, 2001; Aoun, Kristjanson, Currow, & Hudson, 2005; Hickenbottom et al., 2002; Langa, Valenstein, Fendrick, Kabeto, & Vijan, 2004; Panda & Coleman, 2001), but little empirical research has examined the effect of financial costs on family caregiving burden. This article explains the effect that the financial costs of caregiving have on the level of burden that family caregivers experience.
Literature Review
Financial Costs and Impacts of Caregiving
Caregiving affects a caregiver’s work and family financials, such as balancing a job and providing care to family members (Haddock, Zimmerman, Lyness, & Ziemba, 2006). Financial costs refer to direct momentary costs related to paying for the caregiving expenses while some are related to the forgone financial or monetary costs in employment due to one having to perform a caregiving role. Not all the financial costs could be measured by momentary values as some costs are subjectively indicated by individuals as perceived financial costs.
Research findings in the United States estimated significant costs of caregiving to employers, due to lost productivity, and for caregivers due to the loss of income (Metropolitan Life Insurance Company, 1999). Some researchers note that the time required to competently care for a frail elderly relative often amounts to a full-time job (Schulz et al., 2003). Compared with coworkers who are not caregivers, family caregivers had to take more time off work, were interrupted at work more often regarding family matters, missed more days at work, took more time off without pay, and ultimately worked fewer hours than desired (Addington-Hall et al., 1992; Brienbaum & Clarke-Steffen, 1992; Brooks, 1989; Covinsky, Goldman, & Cook, 1994; Ferris et al., 1991; Grunfeld, 1997; Neal, Chapman, & Ingersoll-Dayton, 1988; Scharlach & Boyd, 1989; Schulz et al., 2003; Stommel, Given, & Given, 1993; Stone, Cafferata, & Sangl, 1987). Studies found that the level of productivity at work was affected by the workers who were family caregivers, because family caregivers were more tired, had to take more days off, and had to leave work earlier to attend to their care recipient (Enright & Firss, 1987; Neal et al., 1988). Caregivers may miss out on career advancement and promotion opportunities because of their caregiving obligations at home, while some have left the job to focus more on caring for their frail elderly relative (Enright & Firss, 1987; Gibeau & Anastas, 1989; Stephans & Christianson, 1986; Stone et al., 1987).
The finances of family caregivers can also be affected by the daily costs of caregiving (Fast, Williamson, & Keating, 1999; Hayman et al., 2001; White-Means & Rubin, 2004). Other related caregiving expenses such as transportation, nonprescription medications, medical supplies, prescription medications, equipment, and homemaking supplies can also affect financial adequacy (Decima Research, 2002; Hollander, Liu, & Chappell, 2009). Unfortunately, the costs of caregiving are usually not covered by private insurance programs (Arno, Levine, & Memmott, 1999).
The linkage between financial costs of family caregiving and the burden experienced by the family caregivers has not been well established, further justifying the aim of this study to examine the effect of financial costs of family caregiving on caregiving burden as experienced by the family caregivers.
Caregiving and Burden
Caregiving burden is often referred as the family caregivers’ perceived level of distress, demands, and the pressure associated with caregiving roles, responsibilities, and tasks (Gitlin et al., 2003). Previous research has consistently documented caregiving burden and the effects of the burden on family caregivers for older adults, including the psychological, social, and health consequences (Beeson, 2003; Chadiha, Rafferty, & Pickard, 2003; Nijboer, Tempelaar, Triemstra, van den Bos, & Sanderman, 2001; Parrish, Satariano, Freisthler, Feinberg, & Adams, 2005; Pickett-Schenk et al., 2006; Van Wijgaarden, Schene, & Koeter, 2004; Wallsten, 2000; Yajima et al., 2007). Caregivers experienced social strain if they felt frustrated and perceived a lack of caregiving assistance from other family members (Dautzenberg, Diederiks, Philipsen, & Tan, 1999; de Figueiredo & Turato, 2001). Caregiving affects family life because it reduces the caregiver’s time with their family and friends (Coleman, Piles, & Poggenpoel, 1995; Parrish & Adams, 2003). Caregiving is also associated with adverse health effects, including difficulty sleeping, frequent headaches, and weight gain or loss (Hepburn, Tornatore, Center, & Ostwald, 2001; Koopmanschap, Van Den Berg, Brouwer, & Van Den Bos, 2005).
The level of burden family caregivers experience is dependent on a variety of factors associated with both the caregiver and the care receiver. For instance, the primary caregiver is more vulnerable to burden than those who do not play a primary role in providing care (Greenberger & Litwin, 2003). The demographic characteristics of the caregiver such as sex (Knight, Longmire, Dave, Kim, & David, 2007), age (Kim et al., 2006), marital status (Choi & Bohman, 2007), and religion also play a role (Koenig, 2005). Correlates of increased vulnerability to a higher level of burden have been identified. These include being younger, being a woman, being unmarried, having a religion, and being an immigrant (Choi & Bohman, 2007; Kim et al., 2006; Knight et al., 2007; Koenig, 2005; Lai, 2007a; Mendez-Luck, Kennedy, & Wallace, 2008).
Variables associated with care receivers also contribute to caregiver burden. These variables include the types of health problems that the care receivers have, and the type and number of caring tasks the caregiver is required to perform (Sörensen & Pinquart, 2005). A higher degree of mental or physical impairment in the care recipient, more behavioral problems and disabilities, and a higher level of dependency in their activities of daily living contribute to increasing the burden level of caregivers (Knight et al., 2002; Lee & Kolomer, 2005). If the care recipient had more activities of daily living with which they needed help, this was an indicator of more caregiver burden (Mendez-Luck et al., 2008). Having to give constant attention to the care recipients for their well-being was another correlate of a higher caregiving burden (Mendez-Luck et al., 2008).
Social support (Smerglia, Miller, Sotnak, & Geiss, 2007), financial resources (Wakabayashi & Donato, 2006), coping style and strategies (McClendon, Smyth, & Neundorfer, 2004), or the personality type of the caregiver are also related to the caregiving burden level (Koerner & Kenyon, 2007). If the caregiver perceived the caregiving role as a responsibility as a threat, this will contribute toward a higher level of caregiving burden (Van Den Wijngaart, Vernooij-Dassen, & Felling, 2007). Caregivers reporting a lower level of filial piety also reported a higher level of caregiving burden (Lai, 2007a). Caregivers who have a more positive coping style, a higher level of perceived self-efficacy, social support, and instrumental support are more likely to have a reduced level of caregiving burden (Van Den Wijngaart et al., 2007).
Having to balance caregiving with other family responsibilities caused a greater level of burden for caregivers. If sacrifices had to be made to provide care to the care recipient, the level of burden was predictably higher because of the perception of sacrifice (Mendez-Luck et al., 2008). Sacrifices can be associated with time, money, giving up luxury items, and the quality of relationships with others (Mendez-Luck et al., 2008).
Research Methodology
Sampling and Data Collection
The target population was the family caregivers in Calgary who provided care to an older adult 65 years of age and older. For the purpose of this study, a family caregiver refers to a person who provided assistance, in the past 12 months, with at least one caregiving task because of a long-term health condition of the care receiver without receiving any financial payment. Recognizing the fact that many caregiving activities are performed by family members, relatives, friends, and neighbors (Barker, 2002), this study included family caregivers who could be a family member, relative, friend, or neighbor who did not receive remuneration or wages for providing the care. For the purpose of this study, the types of care provided by the caregivers could range from assistance with simple tasks to intensive personal care. These caregiving tasks referred to the duties inside the house, such as meal preparation, cleaning, and doing laundry. They can also refer to providing personal care, such as toileting, bathing, and dressing. There are also duties outside of the house, such as providing transportation, running errands, and doctor visits. The elderly care receiver could be residing with the caregiver in the same place of residence or not residing with them.
The study took place between August 2006 and August 2007 in the Calgary Health Region, which covers the city of Calgary as well as 12 other smaller communities in the surrounding area with a total population close to one million. The research protocol was reviewed and approved by the University of Calgary Conjoint Faculties Research Ethics Board. The family caregiver sample for this study was identified through telephone screening of randomly selected telephone numbers from the local directories of Calgary and the surrounding smaller communities. The use of telephone directories as the sampling framework is not without limitations. This method excludes potential participants who do not own a telephone and those who have unlisted telephone numbers. In this study, telephone numbers published in the local telephone directories were randomly selected, through the paid telephone number selection services provided by a national telephone company. According to the latest census information, Calgary and the other 12 surrounding smaller communities had a total population of 966,949 or 364,005 households. Proportional to the number of households in each of the respective communities, a total of 6,546 telephone numbers were randomly selected from the telephone directory to form the sampling frame, after considering the potential fact that some of the numbers could be invalid and the potential response rate (i.e., set at a conservative level of 35%). Telephone contact was made with each of the randomly selected telephone numbers. Eligible participants who met the initial inclusion criteria of being 35 years and older and were able to communicate in the English language on the telephone were invited to take part in answering the first part of a structured questionnaire in a telephone interview.
The content of this portion included questions on the demographic characteristics of the participants, caregiving roles and responsibilities, and questions on the participants’ self-rated health and well-being. At the end of the questionnaire, there was a question asking the participants whether they were a family caregiver for an older person 65 years or older. Those who answered yes to this question were then further invited to answer the second part of the structured questionnaire geared toward the details of one’s caregiving roles, responsibilities, and experiences. The questionnaire took about 30 min to complete and was administered by trained interviewers.
As a result of the random selection and telephone screening, a total of 6,546 randomly selected telephone numbers were screened, and among them, 2,836 telephone numbers were contacted. Among these 2,836 phone numbers contacted, 692 were found to be ineligible for the study and the remaining 2,144 were eligible in terms of meeting the age requirement of being 35 years and older. Among these 2,144 contacts, 1,378 completed the Part 1 survey, representing a response rate of 64.3%. Through the Part 1 survey, 532 out of the 1,378 (38.6%) participants reported to be a caregiver for someone 65 years and older. These 532 caregivers were then invited to take part in the Part 2 survey and 340 completed the study, representing a response rate of 63.9%.
Measures
A structured questionnaire was used during the telephone survey. For the purpose of this study, only variables relevant to this study were included in the discussion. Caregiving burden was the dependent variable and was measured by the 22-item Zarit Burden Interview (ZBI; Zarit, Reever, & Bach-Peterson, 1980). The instrument covers areas including caregiver’s health, psychological well-being, social life, finances, and the relationship between the caregiver and care receiver. Several authors have examined the factor structure of the ZBI. Some examples are the two-factor model of personal strain and role strain (Hébert, Bravo, & Preville, 2000; Whitlatch, Zarit, & von Eye, 1991), the three-factor model of embarrassment/anger, patient’s dependency, and self-criticism (Knight, Fox, & Chou, 2000), and the five-factor model of sacrifice and strain, inadequacy, embarrassment/anger, dependency, and loss of control (Lai, 2007b). The caregiver was asked to indicate the impact of the care receiver’s condition on his or her life by specifying how often they felt the way that was described by each item. Each of the items is answered on a 5-point scale with 0 = never, 1 = rarely, 2 = sometimes, 3 = quite frequently, and 4 = always. The total score of all the items ranges from 0 to 88 with higher scores representing a higher level of caregiving burden. For the family caregivers in this study, a Cronbach’s alpha of .91 was estimated.
To measure the effects of caregiving on financial costs of caring for an elderly relative, the financial cost dimension of the Cost of Care Index was used (Kosberg & Cairl, 1986). According to the authors, the financial costs of informal caregiving were measured by asking participants the following questions: (a) Do you agree that caring for your elderly relative is causing you to dip into savings meant for other things? (b) Do you agree that your family and you must give up necessities because of the expense of caring for your elderly relative? (c) Do you agree that your family and you cannot afford those little extras because of the expense of caring for your elderly relative? and (d) Do you agree that caring for your elderly relative is too expensive? Participants were asked to respond to each question by choosing an answer among a 4-point scale—strongly disagree, disagree, agree, and strongly agree, with corresponding scores of 1 to 4, respectively. All responses were summed to form a total score range of 4 to 16, with higher scores indicating greater financial costs. For the family caregivers in this study, a Cronbach’s alpha of .90 was reported.
Previous studies by various researchers have examined the factor structure of the ZBI. The two-factor model of personal strain and role strain (Hébert et al., 2000; Whitlatch et al., 1991), the three-factor model of embarrassment/anger, patient’s dependency, and self-criticism (Knight et al., 2000), and the five-factor model of sacrifice and strain, inadequacy, embarrassment/anger, dependency, and loss of control are some examples(Lai, 2007b). Based on these previous studies, none of the factors underlying caregiving burden is related to a specific domain of “financial burden.” The four specific items used for measuring costs of care were related to actual financial spending, such as dipping into savings, giving up necessities, not being able to afford little extras, and costs being too expensive. These items indicate how one rates his or her perception of spending and expenditure patterns related to caregiving. None of them is related to subjective burden, as measured in the ZBI. Therefore, it is clear that the ZBI and financial cost index measures different constructs, and therefore it is appropriate to use the financial cost index as an independent variable of the ZBI.
To examine the factors of caregiving burden, other than the self-perceived financial costs variables, three other groups of variables were examined: (a) sociodemographic characteristics of caregivers, (b) sociodemographic characteristics of care receivers, and (c) health variables of the care receivers. The sociodemographic variables of the caregivers included age, sex, marital status, education, employment status, personal monthly income, self-rated financial adequacy, being primary caregiver or not, length of time that one had been providing care to the care receiver, and other caring roles and responsibilities.
The age of the caregivers was grouped into seven 10-year age groups ranging from “35 to 44 years old” to “85 years and older.” Using age groups with equal age intervals would allow the findings to demonstrate, if there is any, the relationship between each of the different age groups and the dependent variable. The sex of the caregivers was grouped into male and female. Marital status of the caregivers was grouped as single or married. The education level of the caregivers was divided into four groups, ranging from “no formal education” to “postsecondary education and above.” Employment status of the caregivers was grouped as employed full-time, part-time, or not employed. The personal annual income of the caregivers was grouped into nine groups ranging from less than CAD$10,000 to CAD$150,000 and over. The self-rated financial adequacy of the caregivers was measured by asking the participants to rate how well one’s current financial status satisfied one’s needs from a 4-point scale ranging from “very inadequate” (1) to “very well” (4). The participants were also asked to identify whether or not they considered themselves as the primary caregiver who was the key person providing the majority of the caregiving, with the answers being binary coded as yes (1) or no (0). The length of time of being a family caregiver was measured by a question asking how many months the care receiver had received care from the caregiver.
Because caring for additional family members or relatives may add to the burden and financial expenses associated with providing care, a few questions were included to ask the caregivers whether or not they had more than one elderly person in the same household, whether they had to take care of other elderly person(s), whether they had children younger than 13 years of age under their care, and whether they had to care for children between 13 and 17 years of age. The answers to all these questions were binary coded as either yes (1) or no (0).
The sociodemographic characteristics of care receivers included age, sex (male or female), marital status (married or unmarried), and the level of financial adequacy rated by the caregiver. The age of the care receiver was measured by the chronological age at the time of the interview. Financial adequacy of the care receiver was measured subjectively by asking the caregiver to rate the adequacy level of the care receiver’s financial status among a 4-point scale of very inadequate, not very well, adequately, and very well, corresponding with scores of 1 to 4, respectively.
As in previous research (Cullen, Grayson, & Jorm, 1997), in this study, the health status of the care receivers was treated as an independent variable of caregivers’ burden and was represented by the number of illnesses or health problems of the care receivers. It was measured by asking the caregivers to report either yes (1) or no (0) to a list of 15 health problems or illnesses that are commonly used in different health and caregiving studies on different aging populations (Lai, 2007a; Lai & Surood, 2008; Lai, Tsang, Chappell, Lai, & Chau, 2007). A higher score represented more health problems or diseases.
To represent caring tasks and workload, the level of assistance the caregivers provided to the care receivers were also measured with a range of seven Activities of Daily Living (ADLs) and eight Instrumental Activities of Daily Living (IADLs). The ADL items included eating, dressing, grooming, walking, getting in and out of bed, taking a bath or shower, and going to bathroom or toilet. The IADL items included using the telephone, getting to places out of walking distance, shopping, preparing for meals, doing housework, taking medicine, handling money, and the use of transportation. The caregivers were asked to indicate whether the care receiver required assistance with each of the activities. The responses were binary coded with a score of 1 indicating need assistance and a score of 0 indicating requiring no assistance. The scores for the seven ADL items were summed to form the ADL score ranging between 0 to 7, while the scores for the eight IADL items were summed to form the IADL score ranging between 0 and 8. A higher score represents a higher level of assistance required by the care receivers in these two major types of daily living activities. For the participants in this study, a Cronbach’s alpha of .80 was estimated for the ADL items and .89 was estimated for the IADL items.
Data Analysis
Descriptive statistics were used to report the findings on sociodemographic and caregiving characteristics of the family caregivers and their care receivers. Caregiving burden was treated as the dependent variable and it was measured using the ZBI and yielded scores ranging from 0 to 88. The effect of perceived financial costs on caregiving burden was examined by multiple regression analysis using the forced-entry method, with the financial costs variable treated as an independent variable. To control for the confounding effects of other variables, the sociodemographic characteristics of the caregivers and care receivers, health-related variables related to number of health conditions of the care receivers and the level of assistance provided to care receivers in ADL and IADL, and finally the perceived financial costs variable were entered. However, with the sample size available for this study, it was not feasible to include all the potentially confounding factors in the regression analysis. Therefore, this study only focused on factors related directly to selected care receivers’ characteristics as identified in the previous research on caregiving burden.
Previous research literature has shown that there are gender differences in caregiving (Ashley & Kleinpeter, 2002; Bookwala & Schulz, 2000). In terms of caregiving burden, female caregivers tend to report a higher level of caregiving related burden and distress than male caregivers (Bookwala & Schulz, 2000). Factors associated with caregiving burden for male caregivers are different from female caregivers (Gitlin et al., 2003; Lai & Leonenko, 2007). Poor health and lower levels of emotional involvement were correlates of burden for husband caregivers while wives’ burden was associated with poorer health, less emotional involvement, greater spouse impairment, and provision of assistance (Gitlin et al., 2003). It is not unreasonable to expect that the factors associated with caregiving burden could be different between male and female caregivers. Therefore, in addition to running the analysis with the whole sample, separate regression analysis was performed for the male and female caregivers, respectively. Statistical assumptions of multiple regression analysis were examined and multicollinearity of the independent variables was checked using the tolerance measure. Two independent variables, the caregiver’s age and the variable measuring whether the caregiver had more than one elderly person in the same household, were removed from the regression analysis due to the problem of multicollinearity, probably with the care receiver’s age and marital status. For care receivers who are older in age, their caregivers, who are usually spouses or adult children, are usually older. For having more than one elderly person in the same household, this could be highly related to the care receiver’s marital status.
Results
Characteristics of the Caregivers and Care Receivers
The demographic characteristics of the caregivers and the care receivers are presented in Tables 1 and 2. Most (73.2%) of the caregivers were female. Over half (52.6%) of the caregivers were between 35 and 54 years of age, more than a quarter (25.3%) were between 55 and 64 years old, and more than one fifth (22%) were 65 years and older. About three quarters (73.8%) of the caregivers interviewed were married. Close to three quarters of the caregivers reported an education level of postsecondary or above (72%). Among the family caregivers, close to half (41.2%) reported being employed full-time and 20.3% reported being employed part-time. About half (46.8%) reported a personal annual income of CAD$20,000 to CAD$39,999.
Sociodemographics and Caregiving Roles of Caregivers by Gender

Note: CG = caregiver; CR = care receiver; ns = not significant.
p < .01.
Sociodemographics and Health of Care Receivers

Note: CG = caregiver; CR = care receiver; ns = not significant.
p < .01.
Among the caregivers, 37.9% identified themselves as a primary caregiver whereas the remaining participants considered themselves as nonprimary caregivers, meaning that another person was providing the major care responsibilities, and the participant was playing a supplementary role. Most (42.4%) of the caregivers reported being either a daughter or a son of the care receiver. Spousal caregivers accounted for only 7.2% of all caregivers.
In addition, more than one in five (22.1%) reported having to provide care to at least one child younger than 13 years old. In addition, another 17.4% of the caregivers reported having at least one child between 13 and 17 years old. Almost a quarter (23.5%) of the caregivers reported having another elderly person at home in addition to the elderly care receiver for whom they provide care, and 13.2% of the caregivers also have to provide care to another elderly person in the same household.
The average age of the care receivers was 80.03 years. Most (70.6%) of the care receivers were female. Along the range between 1 and 4, the care receivers averaged 3.02 (SD = 0.80) in their level of financial adequacy.
Care Receivers’ Health and Caregiving Needs
According to the caregivers, an overwhelming 99.1% of care receivers reported at least one type of major health problem or illness. Examples of major health problems within the sample of care receivers included problems with joints, the back, and arthritis (74.4%); physical mobility problem (63.2%); high blood pressure (46.6%); eye problems (37.6%); problems with hearing (36.8%); heart disease (33.2%); and problems with depression (32.9%). On average, the care receivers were reported to have 5.1 of health problems or chronic conditions (SD = 2.42).
The portion of the care receivers who required assistance with basic personal care ADLs ranged between 23.7% and 58.3%, and these activities were reported as follows: (a) walking (58.3%), (b) taking a bath or shower (54.4%), (c) going to bathroom or toilet (40.2%), (d) dressing and undressing (32.6%), (e) getting in and out of bed (29.8%), (f) grooming appearance (27.5%), and (g) eating (23.7%). However, a relatively larger portion of the caregivers (ranging between 33.2% and 85.7%) reported providing help with IADLs such as (a) doing housework (85.7%), (b) shopping for groceries or clothes (79.3%), (c) using transportation (74.1%), (d) getting to places out of walking distance (68.1%), (e) preparing meals (66.2%), (f) handling money (55.0%), (g) taking medicine (53.2%), and (h) using the telephone (33.2%).
Perceived Financial Costs and Caregiving Burden
The caregiving burden scores reported by the family caregivers ranged from 0 to 68, with a mean of 19.49 (SD = 13.84). To measure the perceived financial costs of caregiving, the financial dimension of the Cost of Care Index was used (Kosberg & Cairl, 1986). Along the potential score range between 0 and 4, a mean score of 1.52 (SD = 0.66) was reported. However, no gender differences were reported in the financial cost scores that the male and female caregivers reported. The results of the individual items indicated that 40.3% of the family caregivers agreed that caregiving for the care receiver was causing them to dip into savings. Again, 40% of the family caregivers indicated that they and their families could not afford those little extras because of the expenses to care for the care receiver. Over a third (38.5%) indicated that their family or they had to give up necessities because of the expense to provide care. Another similar proportion (36.8%) of the caregivers indicated that caring for the care receiver was too expensive.
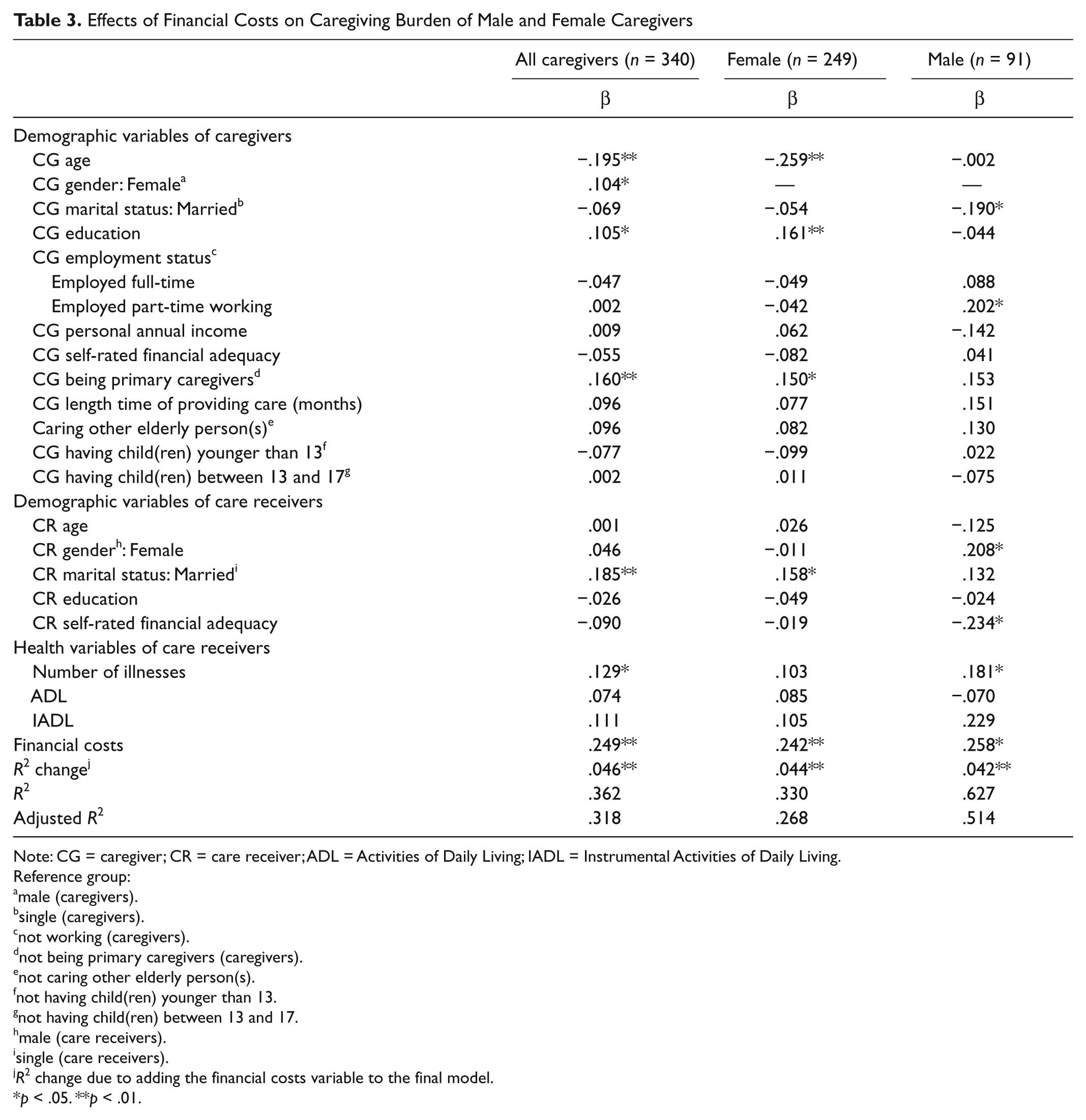
The results of the multiple regression analysis are presented in Table 3. When all caregivers were included in the analysis, caregivers who were younger in age, female, better educated, and were primary caregivers reported a higher level of caregiving burden. In addition, the caregiving burden reported by caregivers who provided care to a married care receiver was higher than those who provided care to a single care receiver.
Effects of Financial Costs on Caregiving Burden of Male and Female Caregivers
Note: CG = caregiver; CR = care receiver; ADL = Activities of Daily Living; IADL = Instrumental Activities of Daily Living.
Reference group:
male (caregivers).
single (caregivers).
not working (caregivers).
not being primary caregivers (caregivers).
not caring other elderly person(s).
not having child(ren) younger than 13.
not having child(ren) between 13 and 17.
male (care receivers).
single (care receivers).
R2 change due to adding the financial costs variable to the final model.
p < .05. **p < .01.
Consistent with previous research on caregiving (Marvadi et al., 2005), caregivers providing care to care receivers who were reported to have more health problems or illnesses also reported a higher level of caregiving burden. When controlled for the confounding effects of the demographic variables of the caregivers and care receivers, as well as the health variables of the care receivers, financial costs was the most important predictor of caregiving burden with the highest standardized coefficient (.249) reported (refer to Table 3). In this regression model, all the factors accounted for 31.8% of the variance in the family caregiving burden.
For the male caregivers in this study, those who were married reported a lower level of caregiving burden when compared with those who were not married, probably as noted in previous research, due to the support provided by their spouses or due to the high endurance level of the caregivers who provide care to their spouses (Faison, Faria, & Frank, 1999). Male caregivers who provided care to a female care receiver reported a higher level of caregiving burden than providing care to a male receiver. Employment status is a significant correlate of caregiving burden for the male caregivers working part-time. Caregivers providing care to care receivers with a lower level of financial adequacy rated by the caregiver also reported a higher level of caregiving burden than the caregivers who provided care to care receivers with a higher level of financial adequacy. The number of health problems or illnesses also related positively to the level of caregiving burden. Finally, the self-perceived financial cost reported by the caregivers was positively related to caregiving burden, with the largest standardized coefficient (.258) among the other factors. These significant factors explained 51.4% of the total variance in caregiving burden of the male caregivers.
For the female caregivers, those who were younger in age had a higher education level and those who were the primary caregivers reported a higher level of caregiving burden. In addition, female caregivers providing care to a married care receiver reported a higher level of caregiving burden than the caregivers providing care to a single care receiver. None of the variables related to the care receivers’ health was significantly related to caregiving burden. However, when controlled for the confounding effects of other independent variables, self-perceived financial costs correlated positively with caregiving burden, once again, with the largest standardized coefficient (.242). The significant factors explained 26.8% of the total variance in caregiving burden of the female caregivers.
Discussion
Whereas previous research on caregiving burden focuses primarily on factors such as sociodemographic characteristics of the family caregivers and the health status of the care receivers (Prigerson et al., 2003; Wallsten, 2000; Zhan, 2005), this study has brought forth new findings to enrich the understanding of the relationship between financial costs of caregiving and caregiving burden of the family caregivers. Although research studies on family caregiving have indicated the financial costs associated with family caregiving (Keefe & Medjuck, 1997; Langa et al., 2004; Meddaugh, O’Bryant, & Straw, 1991), the empirical linkage between financial costs and caregiving burden has not been examined adequately. Unlike most other descriptive studies (Brienbaum & Clarke-Steffen, 1992; Covinsky et al., 1994; Stommel et al., 1993), this study went further to analyze the effect of perceived financial costs on caregiving burden. It has contributed to fill a research literature gap by providing new research findings on the empirical relationship between perceived financial costs and caregiving burden. It also paves the way for future studies to examine specific monetary values of these financial costs, so as to further identify and quantify the details of such impact.
This finding echoes the findings in some previous research studies that the traditional role of caregiving is often expected of and performed by females (Calasanti & King, 2007; Keefe & Medjuck, 1997; Lawrence, Goodnow, Woods, & Karantzas, 2002; Lutzky & Knight, 1994; Ory, Yee, Tennstedt, & Schulz, 2000). Other explanations of the higher levels of caregiving burden experienced by female caregivers probably include, as indicated in previous studies, the multiple caring roles of women (Wallace, Dilworth-Anderson, & Goodwin, 2003) and other gender-related challenges, such as spending more time with care receivers than men caregivers (Chiou, Chen, & Wang, 2005), receiving less assistance with caregiving tasks (Lutzky & Knight, 1994), and spending more time on intensive personal care and domestic chores (Zhan & Montgomery, 2003). All these point to the need for support for female family caregivers. Service providers have to consider the specific gender-related challenges in family caregiving and to design programs for the family caregivers.
The findings have also indicated similarities in the significant factors of caregiving burden identified for male and female caregivers, with both groups reporting a higher level of caregiving burden if their perceived level of financial costs was higher. The effect of financial costs on caregiving burden, as demonstrated through the standardized coefficients, appears to be similar for both male and female caregivers.
Being younger in age and having a higher education level were significant in affecting mainly the female family caregivers’ burden. These findings are consistent with previous research studies (Fruhauf, Jarrott, & Allen, 2006; Lyonette & Yardley, 2006). A reason that younger family caregivers feel more burdened may be due to the lack of psychological preparation and experience, because younger family caregivers often take up the role without much preparation. These younger family caregivers, as indicated in previous research findings (Fruhauf et al., 2006; Hayden & Heller, 1997), may have children and careers, while having to provide family caregiving to adults. Family caregivers with a higher education level may be engaged in employment that could be more demanding, resulting in a higher level of stress in combination with caregiving responsibilities, therefore reporting a higher level of caregiving burden (Himes, Jordan, & Farkas, 1996; Stolley et al., 2002).
Support for family caregivers should not be limited to providing instrumental assistance and respite in daily personal care provided by the family caregivers. Younger female caregivers encounter multiple demands as mothers providing care to their children, while some may have to attend to demands in their employment. Particularly for female caregivers with younger children, support for child care could also be useful to meet the needs of these family caregivers (Orel, Landry-Meyer, & Spence, 2007; Stoller & Pugliesi, 1989).
Male caregivers working part-time reported a higher level of caregiving burden. The type of family caregivers has most likely adjusted their employment situation due to the family caregiving need (Gignac, Kelloway, & Gottlieb, 1996; Mosher & Danoff-Burg, 2004). To further verify the role of employment status on caregiving burden, future research using a longitudinal method to track changes in employment status is recommended. Programs and services to support employed caregivers should be advocated. Employment policies to better accommodate the caregiving responsibilities of the employees should also be considered by employers (Krach & Brooks, 1995; Liebig, 1993).
Being a primary caregiver is a significant correlate of caregiving burden and this finding is understandable as primary caregivers usually take up more key responsibilities in providing care (Krach & Brooks, 1995). Practitioners working with the primary family caregivers should consider the development of strategies and programs to strengthen the support that family caregivers can receive in the course of providing care. Family caregivers are also likely to appreciate the assistance from their own family and informal support networks (Scharlach et al., 2006). Service providers should develop strategies for facilitating the development of such networks and informal support mechanism for the primary caregivers.
Female caregivers of care receivers who are married reported a higher caregiving burden than those caring for a care receiver who is not married. For many female caregivers, caring for a married care receiver may mean having to negotiate and interact with the spouse of the care receiver, creating further interpersonal communication issues and potentially role disputes, resulting in a higher level of burden. For female spousal caregivers, it is likely that there are issues related to the spousal caregiving role that has added additional burden and stress. An implication is that the needs of the female caregivers, no matter whether they are daughters, daughters-in-law, or spouses, should not be overlooked. Our society tends to feel very comfortable with treating spousal care, particularly care provided by females as a familial obligation (Chappell & Kuehne, 1998), without paying adequate attention to the needs of the female caregivers. It is important for services to address the unique caregiving stresses and challenges that female caregivers in different relationships with the care receivers face while providing care. Some examples of needs are related to intimate personal care (Wong, 2005), spousal relationship (Calasanti & Bowen, 2006; Gregory, Peters, & Cameron, 1990), sexual relationship (Litz, Zeiss, & Davis, 1990), and health deterioration of the care receivers. Further research with a larger sample size is also needed to examine the specific effect of the caregiver–care receiver relationship on caregiving burden experienced by both female and male caregivers.
Male caregivers who provide care to receivers with more health problems or illnesses have reported a higher level of caregiving burden. This finding is consistent with those reported in previous research as care receivers with poorer health often require more assistance (Archer & MacLean, 1993), resulting in a higher level of burden for the caregivers. However, in this study, the health of the care receivers has demonstrated no significant effect on the level of burden reported by the female caregivers. This may be due to the fact that as a group, female caregivers are more accustomed to providing care in their traditional social role (Jutras & Veilleux, 1991; Lai, Luk, & Andruske, 2007), disregarding the health condition of the care receivers. It is important to know that although the female caregivers may be quite accustomed to the knowledge, skills, and social expectation of the caregiving role in providing care to care receivers with different health needs, their sense of burden may not necessarily be lower than the male caregivers. Female caregivers may often face other gender-related disadvantages, such as social, financial, and emotional pressures associated with multiple family-caring roles, the unfavorable health disparity between the female and male caregivers, and the gender inequity faced by female caregivers when attempting to access support services for themselves or their care receivers. All these are untapped research focuses that future studies should continue to examine.
Although many family caregivers are committed to taking care of their older family members and relatives, their commitments and filial obligations should not be taken for granted. These financial challenges and impacts, if unaddressed, would further hinder their capacity and endurance to support the elders in their community. Policies and programs are needed to address the financial needs and security of these family caregivers. It is particularly important to address the context of the family caregivers who are female, who in addition to their caregiving challenges, often face multiple demands in employment and caring for their own family, when attempting to secure gainful employment and financial stability.
Limitations of the Study
As in many other survey research studies, there are limitations in this one also. Although a randomized sample was used, the localized nature of the sample did not allow the findings to be generalized to family caregivers in other localities in Canada. The use of a telephone survey may have excluded family caregivers who were too exhausted to attend to telephone calls, those who were not at home when the interviewers called, or those who do not have English language fluency to take part in the telephone survey. The use of telephone directories as the sampling frame could also have excluded family caregivers who had unlisted their telephone numbers, those who did not have a telephone, or those who used a mobile telephone rather than a landline telephone. The use of the caregivers as a proxy to collect data on the number of illnesses that the care receivers have may not accurately capture the health status of the care receivers, which could have a direct impact on the financial consequences of family caregiving. Also, the study was general and did not specifically address the type and amount of financial costs of family caregiving associated with specific health problems, diseases, or illnesses.
Another limitation is that resulting sample in this study consisted of a relatively small portion of spousal caregivers. Therefore, the results were unable to provide an accurate representation of this group of caregivers who are the most common type of family caregivers providing care to an older adult.
The resulting regression models reported accounted for less than half of the variance, meaning that other potential factors that could have been related to caregiving burden were not included in the analysis. A key reason for this is that the sample size of only 340 cases did not allow many factors to be included in the regression model. For example, factors related to the original health status of family caregivers, social support they have received, coping style, and other service utilization variables of both the caregivers and the care receivers were unable to be included in the analysis. The level of use of formal services was also not included in the analysis. Some people may argue that level of service use would affect the financial costs. However, an overall assessment of the perceived financial costs should have been captured when the caregivers provided answers to the Cost of Care Index that assesses the various dimension of perceived financial costs related to providing care.
The results obtained in the regression analysis of the gender groups have to be interpreted with caution, particularly because the male caregivers make up a relatively small part of the sample. Future studies with a larger sample size are recommended, so that the effect of financial costs can be examined after considering the influence of more of the other potentially confounding factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research funding for this research was received from the United Way of Calgary and Area and the Mann Foundation.