
Abstract
The development of physicians’ core competency is related to the quality of medical practice. Accordingly, knowing how to cultivate and evaluate core competency is an important issue for medical education and management. This study used the comprehensive core competency framework proposed by the Accreditation Council for Graduate Medical Education (ACGME) and employed fuzzy AHP (FAHP) and DEMANTEL methods to analyze the weight and priority, as well as the cause-and-effect cluster. The FAHP analysis yielded the following rankings of factors’ importance: (1) patient care (C1; 27.83%), (2) medical knowledge (C2; 20.77%), (3) professionalism (C5; 17.93%), (4) interpersonal and communication skills (C4; 17.41%), (5) practice-based learning and improvement (C3; 15.52%), and (6) systems-based practice (C6; 8.233%). In terms of the DEMANTEL, the effect cluster included patient care (C1), professionalism (C5) and systems-based practice (C6), and the cause cluster included medical knowledge (C2), practice-based learning and improvement (C3), and interpersonal and communication skills (C4). The findings showed that patient care (C1) results from attitudes, patience, and the other five ACGME Core Competencies. Furthermore, emergency physicians’ development also requires humanities and ethics training and practice to ensure practice-based learning (C3). This study demonstrates the importance of various factors in developing emergency physicians’ core competencies, and the findings may provide a reference for future attempts at such competency development.
Introduction
Since 1999, the Accreditation Council for Graduate Medical Education (ACGME) has used the American Board of Internal Medicine (ABIM) as the project outcome for evaluating the Resident Training Program, through which physicians should develop six core competencies (Kissela et al., 2006). The Association of American Medical Colleges (AAMC) has pointed out that 27% of medical graduates have never been evaluated by the attending physician as meeting medical standards when conducting a full medical interview or physical examination (Barnsley et al., 2004). The ACGM has since become a litmus test for whether residents have been trained in the hospital appropriately and developing the necessary core competencies. The ACGME’s six core competencies necessary to be a qualified physician include patient care, medical knowledge, interpersonal communication skills, practice-based learning and improvement, professionalism, and systems-based practice.
The development of physicians’ core competencies is related to the quality of medical learning. The hospital is the most important environment in which physicians cultivate their core competencies. Hospitals’ training plans, organizations’ learning environment, and whether organizations can develop physicians’ core competencies further validate them are important issues in medical management and education. This study examined the ACGME’s six core competencies among emergency physicians and attempted to identify priorities and interdependent relationships among these criteria.
Literature Review
Core Competencies
The ACGME takes the ABIM as a case and evaluates the results of the Resident Training Program (project outcome). A competent physician should possess six core competencies (Kissela et al., 2006).
Most existing literature discusses physicians’ necessary core competencies with respect to the United States’ medical education evaluation board (ACGME). This board proposes effective methods for both assessing and improving core competences (Frey et al., 2003; Johnson et al., 2004; Joyner, 2004; Leach, 2002; Ogrinc et al., 2003). Frey et al. (2003) have discussed the relevant literature focusing on “The Education and Training Methods to Enhance Core Competence,” mentioning that providing good clinical experience and mixing practical operations in different fields can improve resident physicians’ core competencies. They have also pointed out that the ACGME aim to confirm whether residents have established core competencies. Moreover, Massagli and Carline’s (2007) questionnaire study found that senior residents had higher grades than less experienced residents. Additionally, their factor analysis results indicated that ACGME’s comprehensive core competencies can assess residents’ capabilities effectively. Powers et al. (2013) also observe that evaluation of electronic portfolios pertaining to ACGME’s core competencies may require a stronger vocabulary to create conceptual identifiers that can respond to competency background issues. Table 1 presents the six core competencies developed by the ACGME in 1991.
ACGME’s Six Core Competencies for Physicians.

Source. Accreditation Council for Graduate Medical Education.
Methodology
This study evaluated the relative importance of different core competencies for emergency physicians in Taiwan (N = 31; see Table 2 for demographics). We used two multi-criterion decision-making methodologies—fuzzy AHP (FAHP) and DEMATEL—and consulted expert opinions to make these determinations regarding relative importance.
Demographics for Study Participants (N = 31).

Note. According to 2020 statistics from the Taiwan Ministry of Health and Welfare (https://www.mohw.gov.tw ), the total number of registered emergency physicians is 2,045 (male: 1,636 (80%), female: 409 (20%), indicating that Taiwan’s emergency physicians are still predominantly men. According to 2021 statistics from Taiwan Ministry of Health and Welfare (https://service.jct.org.tw/tjcha_CERT/ha.aspx), the total number of teaching hospitals is 113 in Taiwan.
First, we examined the ACGME’s six core competency items (Figure 1) using FAHP (Herrera-Viedma et al., 2004; Saaty, 1980). Appendix A lists these questionnaire items.

Hierarchical model of ACGME criteria.
Second, based on the DEMATEL framework (Tzeng et al., 2007), we designed the questionnaire shown in Table 3. The DEMATEL questionnaire makes pairwise comparisons to evaluate each competency’s relative influence, with scores including 0 (no influence), 1 (low influence), 2 (high influence), and 3 (extremely high influence; Tamura & Akazawa, 2005).
DEMATEL Questionnaire.

We collected data teaching hospitals in Taiwan from the attending physician (Visiting Staff) supervising and education the emergency physicians. Because we did not obtain medical records, there was no need to secure approval from the ethics committee. All respondents participated in the study voluntarily.
Results
Fuzzy AHP Analysis
Following the FAHP calculation process (Saaty, 1980), we found that CI = 0.09591 (<0.1), CR = .0773 (<.1), and eigenvector (λmax) = 6.48, which were deemed acceptable (Appendix B). As shown in Figure 2, the highest-ranked factor was patient care (C1; 26.62%), followed by medical knowledge (C2; 21.54%), professional literacy (C5; 15.64%), interpersonal and communication skills (C4; 16.68%), practice-based learning and improvement (C3; 15.52%), and systems-based practice (C6; 9.03%).

Criteria weights and rankings.
DEMANTEL Analysis
The steps of the DEMANTEL analysis procedure (Tzeng et al., 2007) and the results are described next.
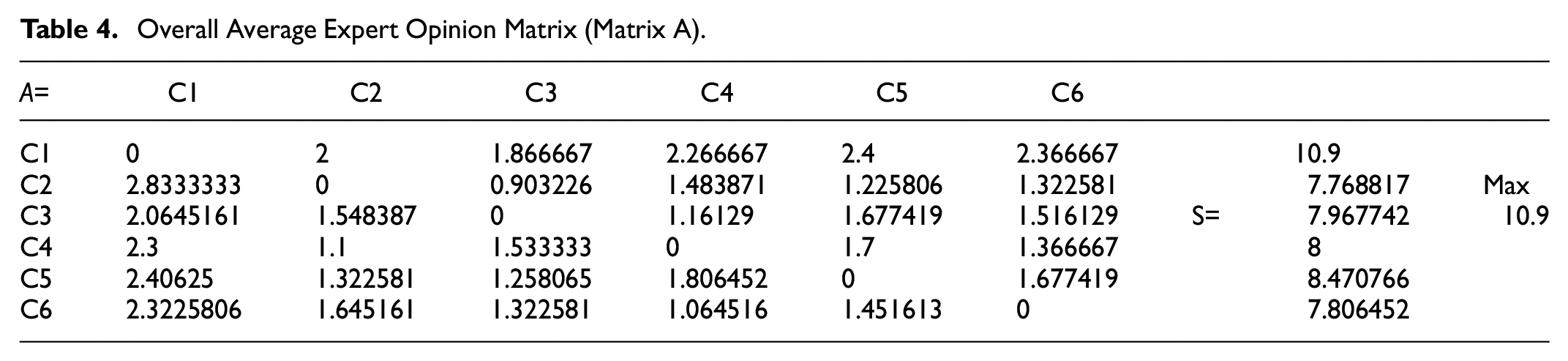
Step 1: Compute the average initial matrix A with the questionnaire responses (N = 31; see Table 4).
Overall Average Expert Opinion Matrix (Matrix A).
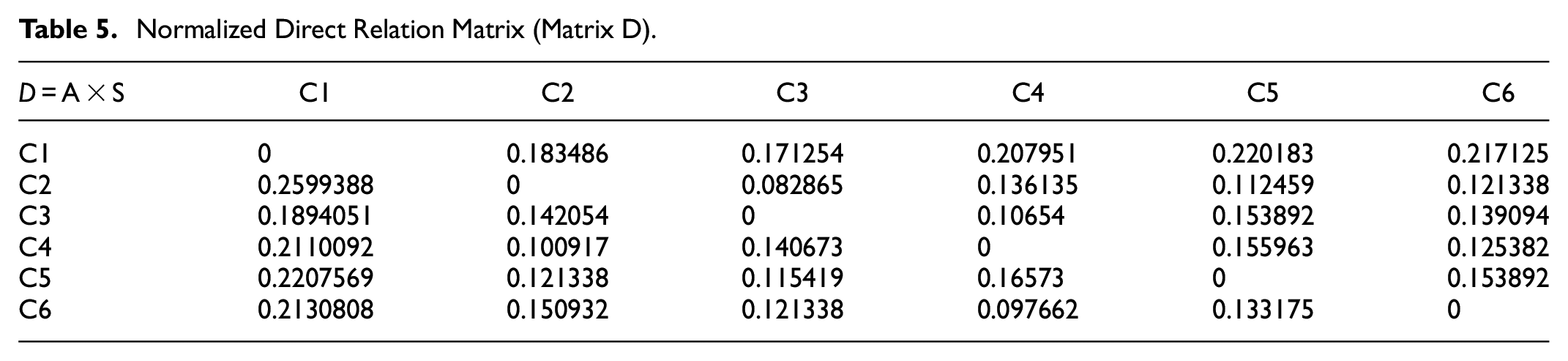
Step 2: Compute the normalized initial direct relation matrix D with the questionnaire responses (Table 5).
Normalized Direct Relation Matrix (Matrix D).
Step 3: Compute the total relation matrix T with the questionnaire responses (Table 6).
Total Impact Matrix (Matrix T).

Step 4: Draw the DEMANTEL causal diagram
Analyze and Compute the Degree of Relationship With the Central Role
Next, we can compute the degree of central role (Dx + Rx) and (Dx − Rx) values. The degree of central role (Dx + Rx) and (Dx − Rx) in the DEMATEL model represents the strength of influences both transmitted and received (Table 7). Note that (Dx + Rx) is positive when the evaluation criterion x influences other evaluation criteria more than it is influenced by them, and (Dx − Rx) is negative when the evaluation criterion x is influenced more by other evaluation criteria than it influences them.
Degree of Central Role (D + R) and (D − R).

Draw the DEMATEL Cause-and-Effect Diagram
The next step is to draw various criteria on the two axes highlighting the horizontal axis (R + D) and the vertical axis of net cause and effect (R − D), which here follow the results presented in Table 7. Constructing a causal relationship diagram (as shown in Figure 3) is a representation of the form and graphical relationship. This makes the structure and relationships of the criteria clearer.
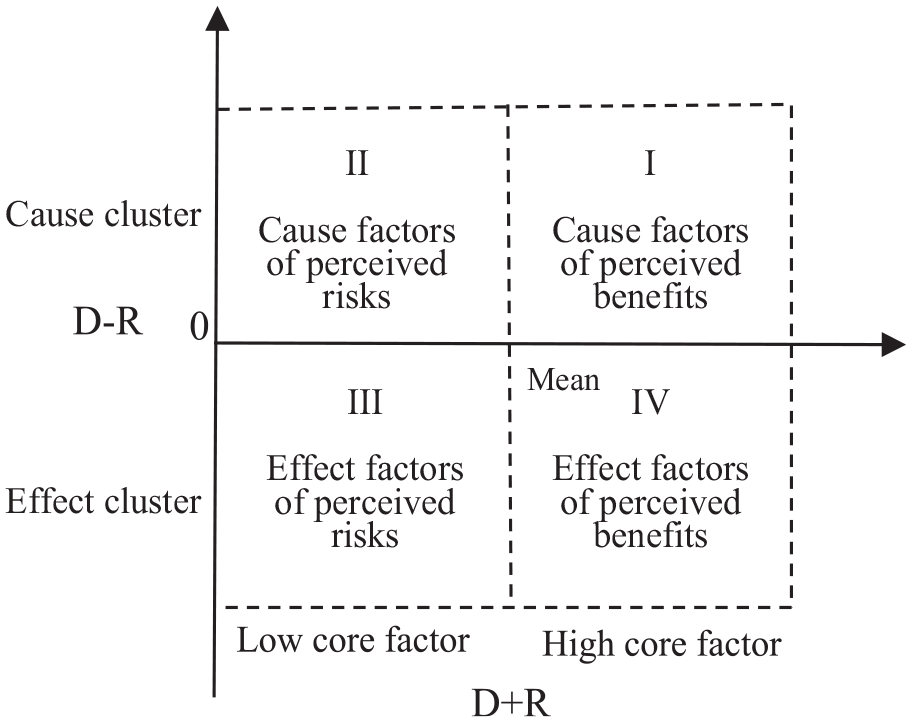
The DEMANTEL cause-and-effect diagram.
We observed the division of regular clusters into causal groups. The effect cluster included C1, C5, and C6, and the cause cluster included C2, C3, and C4. The causal relationships among the core competency selection criteria are depicted as a causal diagram.
Discussion and Conclusions
This study used fuzzy AHP and the DEMATEL model to analyze the relative importance of Taiwan emergency physicians’ core competencies. Our results are expected to aid in the development and assessment of these competencies.
From the fuzzy AHP analysis, we found that the top three most important competencies are patient care, medical knowledge, and professionalism, respectively. Therefore, medical education managers should pay special attention to patient care in training new physicians (Michael et al., 2019). Swing (2002) study show the new medical students graduates’ ability to meet the demands of today’s practice environment. The competencies emphasize Practice-Based Learning, Improvement and Systems-Based Practice, and Patient Care and Medical Knowledge.
As for the DEMATEL analysis, Figure 4 summarizes the relationships among the core competencies. We can generally delineate clusters and causal groups. The effect group includes patient care, professionalism, and systems-based practice. The cause cluster includes medical knowledge, practice-based learning and improvement, and interpersonal communication skills. Practice-based learning and improvement has the greatest impact on and the closest connection with the other criteria. Practice-based learning and improvement may directly or indirectly influence other characteristics such as medical knowledge and interpersonal and communication skills (C4). One major limitation is the evaluation effort required with these techniques. Any combination of the other ACGME criteria reflects all competencies except practice-based learning. This deficiency can be corrected with revision of portfolio guidelines (Jarvis et al., 2004). Patient care results from attitudes, patience, and the other five ACGME core competencies. Therefore, the development of emergency physicians also requires humanities and ethics training and practice to fulfill the practice-based learning criterion. Doukas et al. (2013) study show that concept requires physicians to make three commitments: (1) evidence-based, rigorous, and accountable, (2)the physician’s primary concern is protect and promote the patient’s health-related interests, secondary is keeping self-interest systematically; and (3) to maintain, strengthen, and pass on medicine to future physicians, patients, and society as a public trust, rather than viewing medicine as a self-interested merchant guild that makes protecting the economic, social, and political interests of physicians paramount.

DEMANTEL causal diagram of Taiwan emergency physicians’ core competencies.
Iserson et al.’s (2008) study shows that medical educators can give physicians-in-training an understanding of and appreciation for these fundamental responsibilities. By focusing attention on the medical consequences of disasters, both professional societies and teachers can help physicians examine the scope and limits of their professional responsibility. For example, the Icahn School of Medicine at Mount Sinai in New York, planned in advance and determined the possible hospitalization length of COVID-19 patients. Upon observing an increase in the number of hospital admissions, through empathetic, patient, and timely collaboration among emergency physicians, nursing, hospice, and public works information units, the hospice ward was converted to an intensive care unit for COVID-19 patients to maintain energy in the regular ICU (Apoeso et al., 2021).
Although we used fuzzy AHP and DEMATEL as a general method to evaluate the relative importance of Taiwan emergency physicians’ core competencies, there are other multi-attribute decision-making methods, such as fuzzy ANP, TOPSIS, and ELECTRE that can be used for this purpose. In future research, it may be helpful to compare these methods’ effectiveness.
Limitations
This research is a quantitative research, and the survey is carried out in the form of a Fuzzy AHP and DEMATEL questionnaire. It is impossible to gain an in-depth understanding of the interviewed emergency physicians’ like an interview, and it is impossible to expand the scope and sample number of investigations. The research scope is only limited to teaching hospitals in Taiwan from the attending and physician (Visiting Staff) supervising and education the emergency physicians, and its representativeness is also the limitation of this research.
Footnotes
Appendix
Synthetic Pairwise Comparison Matrices.

| Synthetic pairwise comparison matrices with geometric means (integrated fuzzy numbers) | Geometric row means | Fuzzy weight | Crisp weights | Ranking | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C1 | C2 | C3 | C4 | C5 | C6 | r | w | BNP | ||||||||||||||||||
| C1 | 1 | 1 | 1 | 0.934 | 1.128 | 1.353 | 1.730 | 2.113 | 2.542 | 1.795 | 2.200 | 2.643 | 1.040 | 1.211 | 1.429 | 2.893 | 3.576 | 4.233 | 1.435 | 1.683 | 1.950 | 0.1887 | 0.2585 | 0.3514 | 0.266 | 1 |
| C2 | 0.739 | 0.887 | 1.071 | 1 | 1 | 1 | 1.775 | 2.211 | 2.638 | 1.234 | 1.514 | 1.841 | 0.749 | 0.851 | 0.984 | 2.042 | 2.500 | 3.008 | 1.163 | 1.360 | 1.577 | 0.1530 | 0.2089 | 0.2843 | 0.215 | 2 |
| C3 | 0.393 | 0.473 | 0.578 | 0.379 | 0.452 | 0.563 | 1 | 1 | 1 | 0.591 | 0.715 | 0.882 | 0.987 | 1.197 | 1.456 | 0.987 | 1.197 | 1.456 | 0.664 | 0.777 | 0.921 | 0.0874 | 0.1193 | 0.2625 | 0.156 | 5 |
| C4 | 0.378 | 0.454 | 0.557 | 0.543 | 0.661 | 0.810 | 1.134 | 1.399 | 1.692 | 1 | 1 | 1 | 1.398 | 1.775 | 2.200 | 1.398 | 1.775 | 2.200 | 0.877 | 1.048 | 1.243 | 0.1154 | 0.1610 | 0.2241 | 0.167 | 4 |
| C5 | 0.700 | 0.826 | 0.962 | 1.016 | 1.175 | 1.335 | 0.687 | 0.835 | 1.013 | 1.170 | 1.441 | 1.738 | 1 | 1 | 1 | 1.108 | 1.346 | 1.625 | 0.927 | 1.078 | 1.242 | 0.1219 | 0.1657 | 0.2238 | 0.170 | 3 |
| C6 | 0.236 | 0.280 | 0.346 | 0.332 | 0.400 | 0.490 | 0.687 | 0.835 | 1.013 | 0.455 | 0.564 | 0.715 | 0.518 | 0.615 | 0.738 | 1 | 1 | 1 | 0.483 | 0.565 | 0.670 | 0.0635 | 0.0867 | 0.1208 | 0.090 | 6 |
| λ > 6.356 | CI > 0.07117 | CR > .0574 | ||||||||||||||||||||||||
Acknowledgements
The authors are grateful for the important input provided by the teaching hospitals in Taiwan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.