
Abstract
The quality of sexuality education is significant in encouraging and expanding the knowledge of sexual and reproductive health (SRH). Parents’ attitudes and beliefs toward sexuality education contribute to the effectiveness of sexuality education in schools. Consequently, there is a need to provide a validated instrument to investigate parental attitude and beliefs toward school-based sexuality education. The objective of this study is to describe the development and test the psychometric properties of an instrument that measures the attitudes and beliefs of parents toward the implementation of sexuality education in primary schools within Malaysia. Items for the instrument in this study were developed through literature review via the deduction method. Data collection was conducted in two phases. The first phase involved 174 parents with children who were attending primary schools through convenience sampling. Then, the multistage sampling method was employed to collect data from 350 parents. Results from the exploratory factor analysis have identified four latent dimensions, which are attitude toward sexuality education, perceived benefits, perceived barriers, and self-efficacy, that support the SRH learning among primary school children. Confirmatory factor analysis demonstrates a good overall fit with the application of post hoc modifications. The results also indicate that the instrument has high internal consistency, as well as convergent and discriminant validity. Findings from this study have indicated that the instrument can be used as a valid and reliable measure to examine the attitudes and beliefs of parents toward sexuality education in primary schools within Malaysia.
Keywords
Introduction
The sexual and reproductive health (SRH) among adolescents have always been one of the most significant concerns of public health. Healthy young adults are essential for the development of a country. Thus, the efforts and time needed to invest in the SRH and well-being of this age group are relatively crucial for a country to progress, whereby the provision of good quality and comprehensive sexuality education empowers young people to make healthy and responsible choices with regards to sexuality (UNESCO, 2018).
The school has been widely recognized as the most appropriate place in providing and exposing information and knowledge of SRH to young adolescents (Do et al., 2017; Makol-Abdul et al., 2009). Nevertheless, the effectiveness of sexuality education can be influenced by multiple factors. According to past literature, parental attitudes and objections have been reported as the recurring challenges of implementing sexuality education in schools. School teachers are worried about the backlash from parents if sexuality education is introduced in schools. A study in Australia has indicated that external pressures from parents and community are likely to influence the willingness and confidence of teachers as well as their topics selection in implementing sexuality education (Smith et al., 2011). Hence, a collaboration between the parents and the social community of young adolescents with the schools is helpful to implement quality school-based sexuality education. Walker and Milton (2006) have found that teachers in Australia and the United Kingdom appreciate parental involvement and engagement in the teaching and learning of sexuality education. Through active participation in their children’s learning about SRH, parents are able to develop a better understanding of the curriculum to realize the importance of the program. This collaboration has subsequently contributed to positive attitudes and support for the implementation of sexuality education in schools.
In Malaysia, the provision of sexuality education remains a controversial issue due to sensitivity and cultural stigma. Khalaf et al. (2014) had interviewed a panel of 15 key professionals which included government officials, healthcare providers, social scientists, woman rights activists, social workers, and researcher from United Nations Population Fund Malaysia as well as counselors from government-based facilities for youth to reveal the potential issues and barriers for provision of sexuality education in Malaysia. The professionals have asserted that the multicultural nature of Malaysia could be a barrier in implementing national sexuality education. The population in Malaysia comprises of three main ethnicities with different religions, cultures, and backgrounds, which have a distinct interpretation of sexuality within the cultural context. Thus, a “one-size-fits-all” approach in delivering sexuality education might be inappropriate to the socio-cultural values of the population (Khalaf et al., 2014). Parents and caregivers are holding to conventional and cultural beliefs on sexuality education that could hinder the implementation of the curriculum in Malaysian schools. Some parents have even rejected the provision of sexuality education due to the belief that early exposure to this aspect of human development can lead to premature sexual debut that can deprive the innocence of young children (Makol-Abdul et al., 2009).
Parental support is deemed vital to the success of child-related policy and programs (Puhl et al., 2017; Pyper et al., 2016; Van Hoof et al., 2010). However, most of the past literature discussed the perception of sexuality education from the perspectives of young people (Allen, 2005; Javadnoori et al., 2012; Opara et al., 2012) and teachers (Cohen et al., 2004; Peskin et al., 2011). Parent’s perception, especially their beliefs toward sexuality education in primary schools, have not been adequately addressed to the knowledge of this study. Although instruments of measurement that evaluate parental attitude toward sexuality education are available within this area of research interest, yet most of the instruments emphasize on parent’s approval toward specific content in sexuality education (Jankovic et al., 2013; Peter et al., 2015). Hence, the existing instruments may fail to capture the underlying factors that could lead to formation of parental attitude toward implementation of sexuality education. Hence, the development of an instrument that measures parental attitude is timely and essential to complement the existing literature.
Literature Review
While a number of measures that examine parental attitude toward sexuality education exist, these measurements suffer from a number of limitations. For instance, many studies had considered parents’ preferences and self-rated importance toward inclusion of certain topic content in sexuality education as parental attitude toward sexuality education (Depauli & Plaute, 2018; Fisher et al., 2015; Jankovic et al., 2013; Makol-Abdul et al, 2009; Peter et al., 2015; Steadman et al., 2014). Nevertheless, the number of the sexuality education topics parents agreed to be covered in curriculum do not necessary equivalent to their attitude toward implementation of sexuality education in schools.
In addition, when developing these measurements, most researchers were targeting on parents of high school students (Odebode, 2019; Peter et al., 2015; Welshimer & Harris, 1994) with limited evaluation tools for parents with children attending primary schools. Parents’ expectations for sexuality education could be varied based on physical and mental maturity of their children (Barr et al., 2014; Yeo & Lee, 2020). Parents with older children might think sexuality education is more relevant to their children’s need. Thus, it is obviously not appropriate to blindly adopt these instrument to measure parental attitude toward sexuality education in primary schools.
Additionally, there is a lack of sufficient research investigating the attributes of parental attitudes toward school-based sexuality education. Most of the measures used in prior studies are emphasizing on a single dimension of parental attitude toward sexuality education without consideration of the role played by parental beliefs in shaping their attitudes (Depauli & Plaute, 2018; Jankovic et al., 2013; Makol-Abdul et al., 2009; Oluyemi Adetunji, 2013; Peter et al., 2015; Steadman et al., 2014; Welshimer & Harris 1994).
Meanwhile, some studies had decided to remove sensitive terms such as “sexuality education” to prevent emotion-eliciting situations among the parents. For example, a study conducted in Croatia had utilized parents’ supports for health education as a proxy to study the parental attitudes about sex education to avoid public controversy and sensitivity toward the issue (Igor et al., 2015). Inappropriate usage of term in the measurement could provide misleading information when exploring parental attitude toward sexuality education. Valid tools to be able to examine the aspects of parental attitude and beliefs would be useful in providing the information.
Attitude could be defined as “a relatively enduring organisation of beliefs, feelings, and behavioural tendencies towards specific significant objects, groups, events or symbols” (Hogg & Vaughan, 2018, p. 154). In terms of attitude toward sexuality education, parents had generally been supportive or exhibited positive attitudes to have the relevant knowledge included in the school curriculum. Parents believed that young people would more likely be able to protect themselves from sexual exploitation, as well as make healthy decisions related to sexuality if sexuality education was provided (Eko Jimmy et al., 2013; Fisher et al., 2015). However, some studies had reported that some parents had a negative attitude toward sexuality education and perceived sexuality education would lead to earlier sexual debut and immorality (Akpama, 2014; Nyarko et al., 2014). Attitude composed of three components; cognitive components, affective components, and behavioral components (Rosenberg & Hovland, 1960, pp. 1–14). Beliefs, thoughts, and attributes associated with attitudinal objects were part of the cognitive components, which can also be considered as the antecedents of attitudes (Underwood, 2008). Hence, the investigation of personal beliefs on sexuality education among parents and the role of these personal beliefs in shaping the attitude of an individual adolescent was imperative in this study.
The Health Belief Model (HBM) had been used as the underpinning model for this study in exploring the personal beliefs of parents toward the implementation of school-based sexuality education. HBM was developed by Rosenstock (1974) that described the beliefs upheld by an individual could be used to predict positive health behavior. Further, the HBM has also been extended to study factors related to parent involvement in prevention programs for improving their children’s well-being (Randolph et al., 2009). The HBM constructs, which were perceived susceptibility, perceived severity, perceived benefits, and perceived barriers, can be applied individually, or in combination, to explain health behavior (Hayden, 2019, p. 58). On the other hand, there are evidence suggested that perceived susceptibility and severity did not exhibit significant relations with parents’ intention for involvement in child-related program (Salari & Filus, 2017). Therefore, three dimensions had been identified as potential health beliefs that could contribute to the attitudes of parents toward school-based sexuality education, which are perceived benefits, perceived barriers, and self-efficacy.
Perceived benefits had been one of the most essential predictive determinants in the HBM. The measures in assessing positive perception was a major topic of discussion among theorists and researchers as behavior was believed to be determined by an individual’s cognition in terms of acceptability, motives, and attitudes toward the behavior. Based on the review of past literature, parents with children in primary schools believed that sexuality education could help the students in making an informed healthy decision, learn about their bodies, as well as prevent sexual abuse (Fisher et al., 2015). A study that had examined parents with children in secondary schools also reported that the parents felt sexuality education could potentially reduce the risks of engaging in sexual behaviors, teenage pregnancy, and sexually-transmitted diseases among adolescents. Parents also perceived that healthy and positive attitudes toward sexuality could be developed by having good quality sexuality education (Constantine et al., 2007).
Perceived barriers involved the evaluation of potential negative aspects, which may act as obstacles in the adoption of new behavior. Past literature had reported on parents being worried about the backfire in introducing sexuality education as primary school children were too young (Stone et al., 2014) and may not be able to handle the knowledge about sexuality (Robinson et al., 2017). Moreover, parents were also found to perceive that the introduction of sexuality education in schools could encourage adolescents to explore sexuality and contribute to early sexual debut (Lukolo & van Dyk, 2015; Makol-Abdul et al., 2009). Other potential barriers to implementing sexuality education as highlighted in past studies included parents lack SRH knowledge, absence of communication skills (Lukolo & van Dyk, 2015; Pariera & Brody, 2018), religion and cultural stigma (Jerves et al., 2014; Makol-Abdul et al., 2009; Robinson et al., 2017). Fisher et al. (2015) had developed an instrument consisting of 23 close-ended items to examine perceptions of elementary school children’s parents regarding sexuality education. Thirteen items were established to evaluate parents’ perceived benefits and perceived challenges to teaching sexuality education in elementary schools. Yet, the psychometric properties of the instrument was not reported. The researchers also briefly mentioned that the questionnaire was pilot tested for stability reliability using a convenience sample of 25 parents with elementary age children. It is arguable whether such a small size was adequate for validation of a questionnaire with 23 items.
Self-efficacy was added to HBM as one of the constructs by 1988 to describe the motivating factor that encouraged the extensive adoption of health behavior (Champion & Skinner, 2008). Self-efficacy refers to personal belief in one’s own ability to do something (Bandura, 1977). Individuals would more likely engage in a new behavior if they perceived that they have the capability to perform a task. Brock and Beazley (1995) had designed an instrument with nine items to evaluate perceived self-efficacy for parental involvement in home-based sexuality education. Nevertheless, the psychometric properties of the instrument was not described. Additionally, the instrument developed was aimed to measure self-efficacy among parents of ninth grade students. Past studies illuminate that parental self-efficacy varies as a function of the child’s age (Glatz & Buchanan, 2015) and the support provided would be greatly different according to the physical and mental maturity of the child too. This further indicates a need for reliable instrument to capture parents’ self-efficacy in supporting their children’s learning of sexuality education.
Through HBM that was selected as the theoretical framework, this study aimed to develop an instrument to measure parents’ attitudes and beliefs toward sexuality education in Malaysia. This study intended to also examine the psychometric properties of the instrument by using exploratory factor analysis (EFA) and confirmatory factor analysis (CFA).
Methods
Item Development and Validation
The initial items of the instrument were established by using a deductive method, which involved extensive literature review and assessment of existing scales (Boateng et al., 2018). The items were categorized into four categories; parents’ attitude, perceived benefits, perceived barriers, and self-efficacy, toward school-based sexuality education. The items were measured in a continuous scale that ranged from 1 to 10, with a higher score indicating a higher level of agreeableness toward the item. The generated items were then evaluated by experts from various areas of expertise, which included educational psychology, health education, and sexuality education, to ensure the items were measured as intended.
For parental attitude toward sexuality education, the researcher had adapted and designed nine items based on the existing scales and literature. For example, the item “Teaching of sexuality education in school is as important as teaching of reading, writing and arithmetic” was adapted from a study that examined attitudes of mothers toward sex education (Block, 1979). Based on the study by Kristo et al. (2016), three items were adopted and modified to fit the context of sexuality education. Thus, the original item of “I consider the introduction of health education in elementary schools as very important.” was modified to “I consider the introduction of sexuality education in primary schools as very important.”
The following three sections, which were perceived benefits, perceived barriers, and self-efficacy related to sexuality education, were developed based on HBM, as the underpinning model of this study (Rosenstock, 1974). On the other hand, seven items were designed for perceived benefits to measure the expected positive outcomes of introducing sexuality education in primary schools. The construct, perceived barriers, was measured using nine items that were developed based on past literature to capture the evaluation by parents, specifically in terms of negative consequences that could be triggered if sexuality education was implemented. The last dimension, self-efficacy, consisted of six items that examined the extent parents perceived their ability (e.g., knowledge, communication skills, comfortableness) to support the acquisition of SRH knowledge.
The items in the instruments were edited upon discussion with experts of face and content validity. An item was added for perceived benefits dimension, while two items were added in perceived barriers dimensions. These amendments were made due to the items being ambiguous and carry excessive information, which should be separated into two items. Nevertheless, an item was deleted from the self-efficacy construct due to redundancy in meaning. Wordings of the items had also been modified and improved according to recommendations by the experts. Finally, the items were translated into the Malay language, Mandarin, and Tamil, which were also validated by language experts. Some discrepancies in wording were identified and revised to ensure the accuracy of the items.
Data Collection
The targeted population of this study was parents with children in primary school who had been introduced to sexuality education in Johor, Malaysia. Data collection was carried out in two stages. At the pilot study stage, a total of 260 paper-based questionnaires were distributed to parents of year five primary students through convenience sampling method, with 186 questionnaires returned. From this total of questionnaires, 174 responses were valid for exploratory factor analysis. At the second stage, the samples were recruited through the multistage sampling method. The population units were arranged based on hierarchy, and the samples were selected accordingly at each level. The samples involved 20 schools selected from three districts in southern Malaysia. About 1,100 questionnaires were distributed to the parents through the help of health education teachers. The questionnaires were given to students for their parents to complete and were to return to the teachers. The response rate achieved was moderate at 56.09% (617) based on the valid questionnaires that were returned. This study randomly selected 350 responses for confirmatory factor analysis, while the remaining responses were used in structural equation modeling.
Results
Exploratory Factor Analysis
The Exploratory Factor Analysis (EFA) was used to explore the number of factors that influenced the variables and to analyze the shared variance of a factor (Costello & Osborne, 2005). Before the EFA analysis was carried out, the data were examined to identify outliers and extreme scores for each item by using the box plot. Seven outliers were removed from the dataset, and the final sample size for EFA was 167. The determination of sample size in this study was based on the recommendation of a minimum subject to item ratio of 5:1 (Osborne & Costello, 2004). Small sample size in conducting EFA might result in unstable loadings, randomization, non-replicable factors, and lack of generalizability to the population. Based on the recommended 5:1 ratio, the sufficient sample size for 36 items was approximately 180. Hence, a total of 167 parents was considered adequate based on the recommended sample size. Kaiser-Mayer-Olkin coefficient of .852 and Bartlett’s test of sphericity,
Exploratory Factor Analysis and Cronbach’s Alpha Reliability.

The normality of the dataset was examined through the Shapiro-Wilk test, which resulted in the data significantly deviate from a normal distribution. Thus, the principal axis factor was selected as the extraction method for EFA. According to the results of the parallel analysis and Velicer’s Minimum Average Partial (MAP) test, the instrument was proven to measure four different dimensions. Oblique rotation method was used as the rotation solution in this study due to the assumption that the factors were intercorrelated, and therefore, may yield more useful information. Four items (ATT5, BAR1, BAR10, and EFF5) were removed because of low factor loadings, while two redundant items (BEN1 and BEN3) that were initially designed to measure parents’ perceived benefits were also removed. These four factors explained 67.34% of the total variance in parental perception toward school-based sexuality education (Table 1). Thus, the results of EFA supported the items in the current instrument that comprised of four factors, which measured parental attitude, perceived benefits, perceived barriers, and self-efficacy toward sexuality education.
Confirmatory Factor Analysis
Confirmatory factor analysis (CFA) was often used as a powerful analytic tool for the development and refinement in instruments of measurement by examining the nature of and correlations among the latent constructs. Moreover, CFA provides valuable information on the construct validity, method effects, as well as evaluation of factor invariance across groups (Byrne, 2016).
The study sample for CFA included 350 parents for year five primary students that were selected through the multiple-stage sampling method. CFA was performed using IBM SPSS Amos 24. Based on the output that assessed the multivariate outliers, the cases that substantially deviate from all other cases in the data set was identified by examining the Mahalanobis distance among the observations. The output recognized 12 cases as outliers, which were subsequently removed. A critically important assumption of performing CFA was that the data should fulfill the criteria of normality in the data distribution. The univariate normality was achieved when all the variables with kurtosis were less than 7, and the multivariate kurtosis value of 344.954 exceeded the recommended normalized estimates of 5.00. These results suggested that the data were non-normal distributed (Bentler, 2006). On the other hand, the Bootstrapping method was conducted, as suggested by Kline (2016), to address the concern of nonnormality. The bootstrapping result suggested that the model fit was better in larger samples, which indicated that the null hypothesis of the model was accepted and the use of CFA was appropriate. Thus, a total of 338 responses were retained for further analysis.
Convergent validity
Convergent validity was referred to as the extent to which the independent items within the same construct were correlated and was one of the components in construct validity. In CFA, the convergent validity can be assessed by evaluating composite reliability (CR) and average variance extracted (AVE). CR represented the consistency of construct, whereby a greater than the cut-off value of .60 was desirable (Bagozzi & Yi, 1988). The CR values for attitude, perceived benefits, perceived barriers, and self-efficacy were .96, .95, .84, and .92 (Table 2), respectively, which showed good convergent validity.
Composite Reliability (CR), the Square Root of the Average Variance Extracted (AVE), and Correlations Between the Constructs.

Note. The diagonal values in bold are the square root of AVE.
AVE measured the variance attributed to the construct relative to measurement error. The Fornell-Larcker criterion for convergent validity required a minimum threshold of .50 for AVE. However, past literature had also proposed that even if the AVE was less than .50, the convergent validity was still considered adequate when the CR value was greater than .60 (Fornell & Larcker, 1981). In this study, the AVE values for parents’ attitudes, perceived benefits, and self-efficacy were reported above the threshold values, ranging between .74 and .76. On the other hand, the AVE and CR for the construct perceived barriers was .40 and .84 respectively, the AVE level was below the recommended value (Table 2). However, past literature had also proposed that even if the AVE was less than .50, the convergent validity was still considered adequate when the CR value was greater than .60 (Fornell & Larcker, 1981). By considering both CR and AVE values, this study concluded that the instrument exhibited satisfactory convergent validity.
Discriminant validity
Discriminant validity was referred to as the extent of difference between the latent and between the measures of different constructs as the constructs should theoretically not be highly correlated to each other (Hubley, 2014). This study had compared the square root of AVE for the correlated constructs to examine the discriminant validity (Hair et al., 2018). The discriminant validity can be achieved when the square roots of AVE were more significant than the inter-construct correlations. However, Henseler et al. (2015) had proposed a more robust approach to discriminant validity, which was known as the Heterotrait-monotrait (HTMT) ratio of correlation. HTMT values that were close to 1 could be a sign of multicollinearity. Some past studies had also proposed that HTMT values above .85 could be considered as evidence for minimal discriminant validity (Kline, 2016). The output of the HTMT analysis (Table 3) demonstrated that there were no collinearity issues among the latent constructs as all HTMT values were below .85. Based on the criterion discussed above, the instrument displayed good discriminant validity.
Discriminant Validity by Using Heterotrait-Monotrait (HTMT) Criterion.

Goodness of fit
Multiple fit indices, namely Chi-square, RMSEA, GFI, CFI, TLI, NFI, and CMIN/df were used to examine the fitness of the model. RMSEA had been acknowledged as one of the most informative criteria in covariance modeling by highlighting the error of approximation in the population and representing the discrepancy between the proposed model and approximation in the population. On the other hand, past literature had recommended the use of CFI as the index of choice over NFI as NFI tended to underestimate good fit in a small sample (Bentler, 2006). The acceptable cut off values for the fit indices was underlined in table 4 below. Nevertheless, the fit indices did not exhibit a satisfactory level. Thus, the modification indices were examined, which provided a potential solution to treat the discrepancies between the proposed and estimated model.
Post hoc modification approach was used to improve the model fit and generate a more robust model (Figure 1), whereby residual correlations between items within the same construct were added iteratively to the model based on modification indices (Kline, 2016). Residual correlations were also added to several items as these items had referred to a similar context. Examples of these items were BAR 6 (Teaching of sexuality education is not allowed by my religion) and BAR 7 (My culture does not encourage the teaching of sexuality education).
Confirmatory Factor Analysis and Goodness of Fit Statistics.

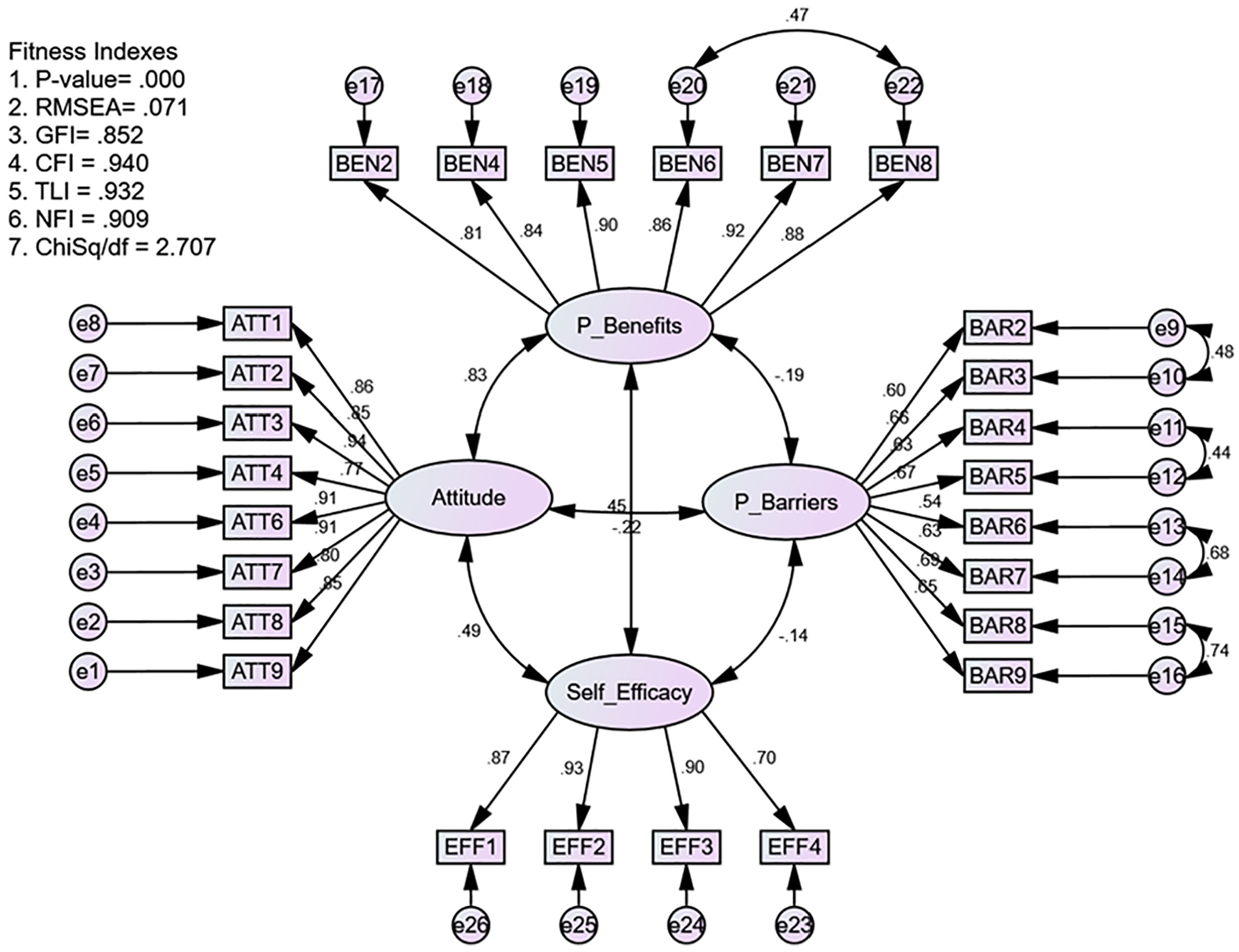
The CFA measurement model for the instrument that measure parental attitude and perception toward sexuality education.
Discussion
Parental attitude is a critical component to ensure the success in implementing sexuality education in schools. Although instruments of measurement that evaluate parental attitude toward sexuality education are available within this area of research interest, most of the instruments emphasize on parent’s approval toward specific content in sexuality education (Jankovic et al., 2013; Peter et al., 2015). Parents’ evaluation of sexuality education in terms of strengths and concerns are frequently integrated into the parental attitudinal scale without proper focus on the contribution of these aspects (Block, 1979; Musa, 2009). Besides, past literature shows that most researches on parental attitude toward sexuality education have rarely highlighted the personal determinants that could have a significant influence. Thus, the purpose of this study is to develop and validate a multidimensional measurement instrument to gain insights on parental attitude and perceptions toward the implementation of sexuality education in primary schools.
The results of EFA show that the instrument, which consists of four factors; attitude, perceived benefits, perceived barriers, and self-efficacy, is aligned with the proposed conceptual framework. In total, these factors have explained 67.34% of the variance in parental perception toward school-based sexuality education. The initially developed scale comprises of 32 items, but the number of items has reduced to 26 after EFA was carried out. The items are removed due to low factor loadings and cross-loading issues. The instrument has also exhibited good reliability with the overall Cronbach’s alpha of .87.
According to the result from CFA, the proposed model (Figure 1) has a good fit of data after post hoc modification. The errors between the item pairs were correlated (BEN 6 and BEN 8, BAR 2 and BAR 3, BAR 4 and BAR 5, BAR 6 and BAR 7, BAR 8 and BAR 9) due to the context of the items. Although some of the residual-correlated items that are removed could improve the model fit, this study has decided to retain the items to avoid any loss of valuable information if these items were deleted. Thus, the residual correlations are added iteratively to improve the model fit. On the other hand, convergent and discriminant validity are two essential components in construct validity. The instrument has displayed satisfactory convergent validity, which shows that the items designed measures the desired latent constructs. The constructs have not shown any multicollinearity issues and achieved good discriminant validity, with the correlation value between the constructs below .85.
The current study contributes to the existing literature by providing a validated instrument in measuring the attitude and perceptions of parents with primary school children toward sexuality education. Although past literature has emphasized the cruciality of parents’ involvement in the success of sexuality education (McKay et al., 2014; UNESCO, 2018), parents are still a relative group that is under-researched within the related aspects. Most of the existing literature has often discussed the perception of sexuality education from the perspectives of young people (Allen, 2005; Javadnoori et al., 2012; Opara et al., 2012) and teachers (Cohen et al., 2004; Peskin et al., 2011). Parent’s perception, especially their beliefs toward sexuality education, have not been adequately addressed to the knowledge of this study.
Wight and Fullerton (2013) have underlined the significance of parental attitudes and values as one of the aspects of family life that impacts and promotes SRH knowledge and health among young adolescents and even adults. Hence, the developed and validated instrument from this study can be used as a useful tool in terms of practical implications to gain a deeper understanding of parental attitude and perceptions toward sexuality education. By establishing a comprehensive understanding of parents’ opinion in this subject, policymakers and implementers can design interventions that better engage parents in the children’s learning of SRH knowledge and skills. Moreover, the instrument allows the users to predict parental attitude by examining their beliefs toward sexuality education. By understanding the correlation between parental attitudes, policymakers, and schools can prepare educational programs for parents to interpret parents’ misconceptions of sexuality education. Through these efforts, parents are hoped to more likely develop a supportive attitude toward sexuality education and be actively involved in facilitating the acquisition of sexuality education among their children. As a result, the effectiveness of sexuality education in schools could be enhanced.
Conclusion
The needs for SRH among young adolescents have become a global concern. Therefore, effective and successful implementation of sexuality education is a collective effort from various stakeholders, including the parents. This study provides a measurement tool with satisfactory reliability and validity to understand parents’ attitude and perceptions toward sexuality education. The use of this instrument can provide insights on parental attitude and perceptions toward sexuality education in primary schools. This knowledge is necessary to facilitate decision making by policymakers and implementers in planning and to execute the related policies and interventions in the future. Despite the strengths, several limitations of this current study need to be addressed. Firstly, the deductive method is used to generate the items in the instrument, whereby a review of past literature has been extensively carried out. Thus, future study is recommended to combine deductive and inductive method to create new measures, which could contribute to a more comprehensive instrument in measuring parental attitude and perception toward sexuality education. Secondly, this study has only involved participants from the southern region of Peninsular Malaysia, which poses a concern for the generalizability of the instrument. Future studies are encouraged to replicate, but with a larger sample size that involves participants from the different geographical regions of Malaysia to provide evidence of generalizability. Another limitation of this study is that the self-reporting questionnaire is used to examine parental attitude and perception toward sexuality education. Parents might respond to the questionnaire in a socially desirable manner which could threaten the validity of the data. Hence, the collection of data from multiple sources such as having teachers’ or students’ evaluation of parental attitudes and opinions toward sexuality education is advisable for future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Author Kee-Jiar Yeo received funding from the Ministry of Higher Education Malaysia (MOHE) under the Fundamental Research Grant Scheme with reference code (FRGS/1/2019/SS05/UTM/01/1). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.