
Abstract
To explore the influencing factors causing the change of hospitalization cost (HC) in patients with kidney stone disease (KSD), control the increase of HC and reduce the economic burden of patients. Data were derived from one provincial general public hospital in Guangxi, China. Model of Artificial Neural Networks and Multiple Linear Regression were used in analyze the external factors from 2012 to 2016. From 2012 to 2016, the total cost increased year by year without the influence of prices. In perspective of Artificial Neural Networks model, influencing importance of length of stay (LoS) and year and hospitalization frequency rank the first three places. With the processing of multiple linear regression model, it was found that the factors of LoS and year were positively correlated with HC, while the hospitalization frequency factor was negatively correlated. Due to the two models, LoS and year and hospitalization frequency affect HC. So decreasing LoS and increasing medical service efficiency are meaningful for controlling HC. By comparison of the two methods, Artificial Neural model is more suitable for information of this study, but much information still can not be explained and further study will be made.
Keywords
Introduction
Kidney stone disease (KSD) is one common and frequently occurring disease of urinary system, caused by abnormal accumulation of crystal substances. Across the world, about 1% to15% of people are affected by kidney stones at some point in their lives (Morgan & Pearle, 2016). And in 2015, 22.1 million cases occurred, resulting in about 16,100 deaths (Global Burden of Disease [GBD], 2015a, 2015b). Kidney stones have become more common in the Western world since the 1970s. Similarly, they are also common in eastern world. In China, KSD is one of the most common urological disease. It has obvious regional characteristics, the southern part of China is one of the three major areas with high incidence of KSD in the world (Chen et al., 2013; S. Li et al., 2017). Guangxi province is an underdeveloped southern region where ethnic minorities gather in China. Guangxi is famous for its numerous karst topography with rich limestones. And limestones also lead to more calcium salt in water, and drinking this water for a long time is easier to accumulate kidney stones. According to statistics, Guangxi is one of the areas with high incidence of calculi in China, with an average incidence of 12% to 15%. The incidence of urinary calculi, mainly consisting of kidney stones, is as high as 17%. This value is close to the highest incidence level in China. Almost every 10 people have two cases of calculi in Guangxi. Such a huge group of patients not only increases the government’s health expenditure, but also brings a very serious financial burden to patients.
In recent years, “expensive medical treatment” and “difficult medical treatment” have become the topics of social concern in China. Research shows that the growth rate of medical expenditure in China has exceeded the development rate of the national economy (Yao, 2017).According to the bulletin of statistics issued by the National Health Commission, the average hospitalization cost (HC) in China was $1,254.8 in 2016, and $903.2 in 2010, the growth rate was 38.9%. As to Guangxi province, the average HC was $1,100.1 in 2016, and $734.8 in 2010, the growth rate was 49.7%, which was higher than the national average. The rapid increase of HC not only aggravates the financial burden of patients, but also becomes a huge burden of the national financial finance. In order to reduce the financial burden of medical care for residents and keep the sustainability of the medical insurance fund, Opinions on controlling unreasonable growth of medical expense in public hospitals were issued jointly by multiple sectors in China in 2015 (National Health Commission of the People’s Republic of China, 2015). This policy demands administrative departments to strengthen the supervision and control for medical expense. Next to it, many specific implementation policies were issued by each province or city. Guangxi province issued Implementation Opinions on controlling unreasonable growth of medical expense in public hospitals of Guangxi (Guangxi Zhuang Autonomous Region Health and Family Planning Commission, 2016). This policy made detail requirements for hospitalized patients on the proportion and growth of per capita medical expense. Researches on the influencing factors of HC and the measures of controlling medical expense also became a hot topic discussed by scholars. Furthermore, analyzing the problems in HC structure and its influencing factors has become a important aspect in health system reform. It has great significance for rational utilization of limited health resources and effective control of medical expense.
As one under-developed province in western China, the per capita GPD level of Guangxi is not high, so it is more necessary to reduce the pressure of the cost of disease. In this paper, one provincial hospital whose medical level ranks first in Guangxi province is studied as the research unit, and the hospital expense and its influencing factors are explored and analyzed. Currently, most studies focus on expense control from the perspective of single disease or single payment method (Dong et al., 2015; Tao et al., 2015; Xue et al., 2015), and both domestic and foreign research have its own particularity, which can be only used as reference, but hardly applied in other countries. From the view of the functional orientation, as one medical clinic center, the provincial medical institution is to undertake the work of medical treatment, teaching, scientific research, emergency, health care, rehabilitation, and the treatment of endemic, difficult, and critical diseases around the whole province areas (C. Li, 2009). This article intends to put forward corresponding policy recommendations for controlling HC of patients with KSD based on this public hospital.
Methods
Data Source
Inpatient medical records (2012–2016) from one large provincial general hospital in Guangxi Province was collected as the research data. The hospital is located in the capital of Guangxi Province, which has gathered many high-quality medical resources and superb medical technology. Every year, a large number of patients come to treat the disease. Therefore, enough case data can be collected in the hospital. According to the International Classification of Diseases (ICD-10), patients diagnosed as KSD which was classified as N20.000 before admission were selected. Hospital Information System was used to collect the information from the front sheet of inpatient medical records. The cases with missing data, length of stay less than 2 days or more than 90 days and HC less than ¥100 (i.e., $14.1) were excluded. A total of 2,421 inpatients were entered the study. The choice of indicators is based on the information collected from the First Page of Medical Records. The influencing factors include nine indicators: year, gender, age, race, marital status, blood group, length of stay (LoS), type of payment (ToP), and hospitalization frequency. Value assignment of each variation was showed in Table 1.
Value Assignment of Each Variation.

Date Collection
After confirming the research plan, the data collection process started. In the hospital we investigated, the discharged patients’ payment information was recorded on the First Page of Medical Records managed by the Medical Record Information Management Department (MRIMD). At first, we applied to the leader of this hospital with our research plan and the demand for data. After we got the consent of the hospital and signing the confidentiality agreement, the technical staff of the MRIMD began to extract data from the database and process the data. The technical staff kept the data of HC and indicators in Table 1 and deleted the data containing personal information, such as name, ID number, address, phone number, etc. About 3 days later we got the data. The entire data collection process takes about 1 week.
Data Analysis
Model of Artificial Neural Networks and Multiple Linear Regression were used in analyze the external factors from 2012 to 2016. In order to eliminate the influence of rising consumption price, the HC from 2013 to 2016 were adjusted according to the consumption price index (CPI) of Guangxi residents, and 2012 data was selected as the baseline data. The data of CPI came from the Bureau of Statistics of Guangxi Zhuang Autonomous Region (Guangxi Statistics Bureau, 2017). The equation (1) is as follows and i refers to the year, pi refers to the CPI of the ith year, Yi0 refers to the HC of the ith year, and Yi is the adjusted HC. Microsoft Visual FoxPro 9.0 software was used for data storage. SPSS 19.0 software was used for data selection and statistical analysis. Clementine 12.0 was used for data fitting analysis of Artificial Neural Networks.

Artificial Neural Networks model
Artificial Neural Network (ANN) is a mathematical model simulating biological neural network. It abstracts the neural network of human brain from the perspective of information processing, and forms different network models according to different connection modes. In the mid-1980s, the error backpropagation algorithm was found to train hidden units, leading to a new wave of ANN research and applications. This article uses the Error Backpropagation Training algorithm to train the ANN. The basic idea is gradient descent method, which means gradient search technology is used to achieve the minimum mean square error between expected output and actual output of the network. ANN consists of input layer, hidden layer, and output layer. Each layer contains several neurons. The neurons in different layers are connected by weights. The basic process of ANN includes the forward propagation of information and the backward propagation of errors. When the information is propagated forward, the information is processed from the input layer to the output layer after process of the hidden layer. If the information does not reach the expected level, it will enter in the backward propagation of error. That is to say, the error signal will return along the path of the original information propagating among neurons, and in the process of returning, the weights of neurons in each layer will be modified one by one. The program will loop continuously, and the weight will be constantly adjusted until the error between the actual output and the expected output reaches the allowable range. These steps above are the training process of the ANN (Battiti, 1992; Xie et al., 2014; Zhang et al., 2015). Detailed calculation formula can refer to the relevant literatures (Jiang, 2011; Ye et al., 2013; Zhang et al., 2015). In this paper, the calculation process of ANN was carried out in Clementine 12.0 software.
Multivariate Linear Regression model
Multivariate Linear Regression (MLR) is a method to study the linear relationship between multiple independent variables and one dependent variable. It is a regression analysis based on the known values of multiple independent variables. The mathematical model of MLR is as follows:
Test of the model
Coefficient of determination expressed by R2 was used to test the two models. Coefficient of determination can indicate the quality of model fitting by the change of data. The normal value range of R2 is 0 to 1. In order to compare which of the two models is more suitable for this data, we need to adjust R2, that is, calculate the adjusted R2 (Ra2). The closer to 1, the better the model fits the data. The R2 and Ra2 was calculated using equations (2) and (3), where Yi is the original value,


Result
Basic Information of HC From 2012 to 2016
There was a big increase from 2012 to 2013. Then from 2013 to 2016, the HC of KSD patients was declining, the growth rate is decreasing year by year. The HC of 2016 was still higher than 2012. The HC from 2012 to 2016 is showed in Table 2.
The HC and HC: Adjusted From 2012 to 2016.

Result of ANN Analysis
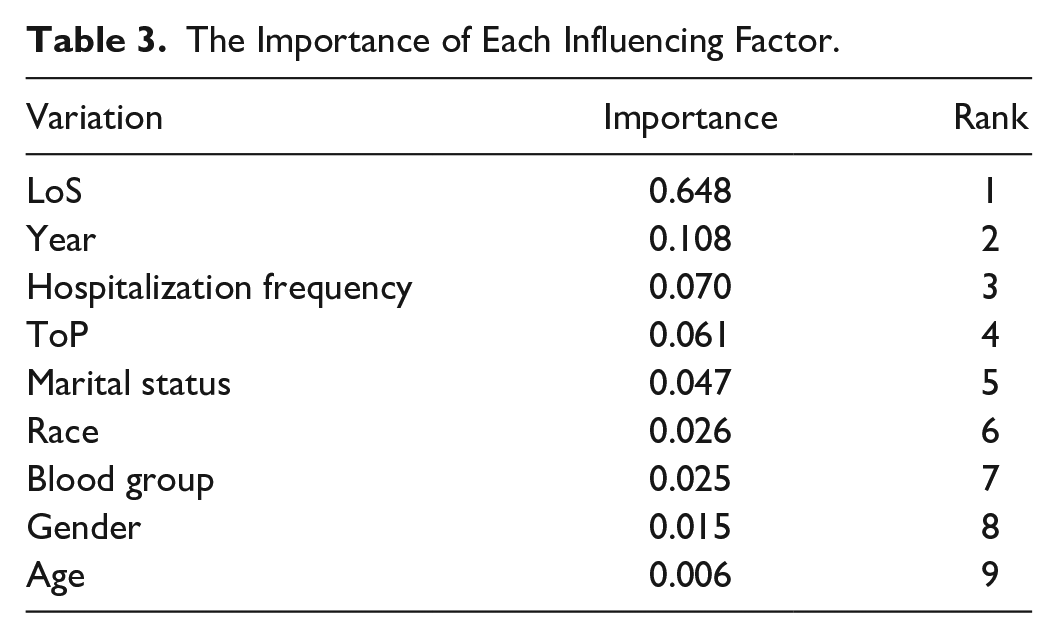
In ANN model, the sample training times are are set 1,000, the learning rate is 0.01, the alpha is .9, the number of training and testing samples are set to 1,695 (70%) and 726 (30%) samples, respectively. According to the operation results of Clementine 12.0 software, the input layer contains 29 units, the hidden layer contains 4 units of two layers, the output layer contains 1 unit, the training accuracy of ANN model reaches 95.891%, and the better training effect is obtained. The importance of each influencing factor is shown in Table 3. In order to prepare for the next step of regression analysis, we first analyze each variable separately. For the categorical variables of marital status, race, blood group, gender, and ToP, K-independent-samples ANOVA were used to analyze the HC differences between different categories. Taking the ToP as an example, the variance analysis results showed that F = 1.581 and p = .136 > .05, which meant there was no difference in HC among different types of payment. Analysis of other categorical variables also showed that there was no statistical significance (p > .05). For the continuous variables of age, LoS, year, and hospitalization frequency, Pearson correlation was analyzed between the variable and HC. The result showed that the variable of LoS, year, and hospitalization frequency were statistically correlated with costs HC (p < .05), and there was no statistical significance between age and HC (p > .05).
The Importance of Each Influencing Factor.
Analysis of MLR
Then the continuous variables of year, hospitalization frequency, and LoS were analyzied in MLR model as independent variables. The HC was logarithmically transformed as dependent variable. The results were shown in Table 4. It can be seen that the LoS, hospitalization frequency, and year variables entered the regression model. The LoS variable is positively correlated with the HC, the standardization coefficient was .670. The hospitalization frequency is negatively correlated with the HC, the standardized coefficient was .039. The influence of the three factors on HC was LoS, year, and hospitalization frequency in turn. The analysis of variance shows that F = 626.622 and p = .000 < .001, which means that the model is statistically significant. In summary, according to the analysis results of ANN and MLR, the main factors affecting HC of KSD are LoS, year, and hospitalization frequency.
Result of MLR Analysis.

Test of Statistical Model
Based on the equations (2) and (3), we calculated the Ra2 of MLR model was .437 and the ANN model was .581 larger than MLR. The Ra2 of ANN was closer to 1, which meant the ANN model was better to fit the HC than MLR model.
Discussion
Both ANN and MLR models were used to explore the influencing factors causing the change of HC in patients with KSD in this article. We can see from the result that ANN model has better fitting degree to the HC. But ANN model cannot calculate the relationship between the HC and influencing factors, while MLR model can. So the combination of the two models can better determine the relationship between influencing factors and HC. Next, we will analyze the results from four aspects.
The Change of HC From 2012 to 2016
After the conversion of HC from 2012 to 2016,There is a big change in the first year afterwards a slow decline is present. We think this change is due to the following reasons. In August 2012, the Notice on the reform of public hospitals in 2012 was published. The notice said that in 2012, all the pilot cities of national contact for public hospital reform should explore comprehensive measures and linkage policies about adjusting the price of medicine, reforming the payment method of medical insurance, etc. The concrete task is reasonably adjusting the price of medical services. And according to the principle of total amount control and structural adjustment, reduce the price of drugs and high-value medical consumables, reduce the price of large-scale medical equipment inspection, but reasonably increase the price of medical services such as diagnosis and treatment fee, nursing fee and operation fee, and cost items reflecting the value of technical services of medical staff, etc. After the implementation of this policy, hospitals began to try to adjust the medical price, but for the lack of experience of hospitals, they did not reduce other costs to the same extent while increasing the price of some medical services, which caused the growth of medical expenses from 2012 to 2013. However, with the continuous adjustment of hospitals and the government’s control over the growth of medical cost, medical expense tend to be stable gradually from 2013 to 2016.
Analysis of Influencing Factors of HC
The greatest impact on hospitalized patients with KSD is the LoS in hospital. This result is relatively easy to understand that with the increase of the number of days in hospital, the basic daily expenses such as bed fee and nursing fee also increase. In addition, the increase of days in hospital will consume more hospital resources, requiring more treatment, medicine, examination, and thus producing more hospital expenses accordingly (Kim, 2005). For hospital, of the three factors, the LoS, year, and hospitalization frequency, only the LoS is a factor that the hospital can control. From this point of view, how to reduce LoS of patients with KSD is of great significance to reduce the HC. On the premise of ensuring medical quality, appropriate reduction of average LoS of inpatients can not only reduce the medical expenses of patients, but also improve the efficiency of the use of beds and reduce the waste of hospital resources.
The second factor affecting HC is the hospitalization frequency, which means the times of hospitalization. From the results of MLR model, it can be seen that this factor is negatively correlated with HC. That is, the higher hospitalization frequency, the lower HC. The reason may be that the more hospitalization frequency, the more understanding of their own diseases. The hospital has stored an early case record, which would avoid some repeated examination and so on. The treatment of patients in hospital is more targeted, and the operation or medication will be more accurate, which would realize the effect of reducing fees. Another influencing factor is the year. The impact of the year on HC can be understood as the impact of factors not included in the study due to some reasons such as not taking into account or being limited by some technical means. For example, policy incentives, upgrading of technology and equipment, adjustment of the cost structure, or changes in the health insurance system and other factors, which also suggest that we still have many factors to be further explored.
Control of Influencing Factors of HC
In general, the LoS is the influencing factor that we need to pay attention to most, and it is also a factor that the hospital can control. Firstly, non-hospital treatments such as day surgery and home beds should be promoted. The LoS is one of the most important influencing factors of hospitalization expenses. Shortening the average LoS can reduce medical expenses. Medical institutions can carry out non-hospital treatments such as day surgery and family beds to control the LoS (Liu et al., 2019). Secondly, studies have shown (Lin, 2015) that the clinical path will not result in differences in LoS or costs due to different patients or doctors, thereby achieving standardized medical behaviors, improving service efficiency, and reducing LoS and waste of medical resources. At the same time, the clinical nursing pathway (CNP) can improve work efficiency, shorten the patient’s waiting time before surgery and hospitalization, which is conducive to reducing related costs (Wang et al., 2015; Ding et al., 2014). Thirdly, it is necessary to rationally allocate limited health resources, optimize the internal processes of the hospital, reengineer the processes, and arrange medical staff scheduling or department bed arrangements. Fourthly, the management of the LoS of patients should be strengthened. The functional departments in the hospital can use the HIS system to monitor the entire process of inpatients and promptly prompt the corresponding departments to take measures for patients who exceed the time limit. Finally, some patients in China have a subjective willingness to think that the longer the LoS, the better it is for the treatment and rehabilitation of the disease, or that they do not trust the doctor’s treatment plan, and actively request an extension of the LoS (Wei et al., 2017). These have become factors that increase the days of ineffective hospitalization, so it is necessary to strengthen communication with patients and cultivate patients’ health literacy.
In addition, the hospital can formulate diagnosis and treatment paths for patients of different ages or genders, so as to provide targeted treatment. It is necessary to rationally allocate limited health resources for different ages or genders, optimize the internal processes of the hospital, reengineer the processes, and arrange medical staff scheduling or department bed arrangements. The health department should develop appropriate single disease cost standards. According to the medical quality management of the disease, the patient’s condition, surgery and treatment methods, the diagnostic standards, and payment standards should be formulated to ensure the efficacy and reduce the medical costs of patients. Hospitals need to establish a comprehensive quality system, strengthen supervision of various medical links, standardize medical behaviors, strictly implement routine diagnostic and therapeutic operations, and ultimately achieve the purpose of controlling the increase in medical costs and reducing the financial burden on patients. Finally, improve people’s comprehensive awareness and disseminate basic information about the disease and their own physical condition, especially for the elderly and women, which will help control the severity of disease in hospitalization patients and promote early prevention, early detection, and early treatment.
Analysis of Other Factors
It is worth mentioning that there are two other factors: age and gender. Although the incidence rate of male is higher than that of female, and young adults are higher than other age groups, there is no significant difference in HC in our research. And there are studies showing that (Tang, 2013), the HC of patients with KSD vary significantly among different age groups. This phenomenon is somewhat different in this study. In the analysis of ANN model, age factor ranks the lowest in the importance of its impact on HC, while in the MLR model, it has no significant impact on HC. Possibly because KSD do not belong to a serious disease. And patients can be treated in county and city hospitals, and the sample selected in this paper is a large provincial third-class hospital. The medical technology level is in the forefront of the province, so the treatment technology, equipment, or drugs used in the province is also more advanced. Patients of all ages are treated with the same high level of equipment, technology, or medicines, and the price is naturally higher than other hospitals. From the patient’s point of view, the patients who choose to visit the hospital are psychologically acceptable to the high prices, while more are considered in the medical technology. This part of patients group has certain economic foundation and consumption capacity, and the age range of these patients is relatively stable, so there are not significant differences of HC among different ages.
Analysis of Model Error
As for the test of two models, the R2 of ANN model is higher than the MLR model, which shows that the ANN model fits the data better. The advantage of the ANN model used in this study is that it is a mathematical model simulating the thinking mode of human brain. It is a large-scale, non-linear, and adaptive system composed of many neurons connected with each other. By continuous learning and training of sample data, the model can fit complex and definite connections of input and output. The ability of processing nonlinear data is stronger than traditional methods (Daniel et al., 1998; Grigsby et al., 2010). Moreover, the ANN model has no requirement for the distribution of data, which is fault-tolerant. Therefore, the ANN model can be used to deal with complex problems. MLR model is prone to be disturbed by the correlation between variables in the process of data fitting, and the results are prone to be affected by the physical values of grades or categories when there are hierarchical or categorized data which leads to deviation (Zhang et al., 2015). Although the R2 of ANN model is higher than the MLR model, there is still a big gap with one which indicate we should do more in-depth research in the future.
Limitations
This study has some limitations. The cost of treatment for patients with KSD includes many aspects, such as inpatient cost and outpatient cost, and even the detailed breakdown of inpatient cost, including treatment cost, nursing cost, medicine cost, operation cost, examination cost, etc., which are all good research perspectives. And the R2 value also indicates that there are still many factors that have not been explored. In future research, we will deepen the research on related costs of KSD. Furthermore, the HC for KSD is related to the location, size, number of stone, renal function, whether combined anatomical abnormality or combined infection, and physical condition of patients, but we can not get these information with our existing data and we will explore them in the future study. Moreover, for any disease, if there is one standard of treatment cost, it is of great significance to control the increase of cost. Therefore, the next step we plan to try to study from this direction as a standard to control the cost growth.
Footnotes
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Thank all participants in this study for their cooperation.
Author Contributions
Hongda Gao conceived and designed the study and wrote the manuscript. He Chen contributed significantly to analysis, manuscript preparation, and revision. Qiming Feng contributed to the conception of the study and conduct the study. Guosheng Luo contributed to the analysis of data. Tingting Xu, Xianjing Qin, and Jun Feng contributed to data preparation and cleaning. Jinmin Zhao performed the research and carried out the study project. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.