
Abstract
Additive manufacturing (AM), also known as 3D printing, is a promising tool to produce assistive technology. For instance, individuals with deafblindness (concurrent vision and hearing loss) could benefit from tactile AM-based products as touch may be their main gateway to access information. This study thus aimed to synthesize evidence on the current and potential practices involving AM in the context of deafblindness rehabilitation and to inform healthcare professionals and family caregivers on how AM can improve functioning and quality of life. A comprehensive literature search of ten databases (PsycINFO, MEDLINE, Global Health, PubMed, CINAHL, EMBASE, ERIC, Web of Science, Engineering Village, and Scopus) was performed to identify sources focusing on the use of AM toward rehabilitation goals of individuals with deafblindness. Nine of 1,397 studies met the inclusion criteria. The findings reveal that AM can counter barriers to full accessibility by enabling professionals to produce customized adapted material and communication devices, thus assisting individuals with deafblindness in communication, mobility, and learning. However, this review highlights a need for more AM research, resources, and training: interdisciplinary collaborations with AM specialists thus appear essential in improving rehabilitation services with AM.
Keywords
Introduction
Deafblindness is a complex and limiting health condition traditionally defined as the combination of any degree of hearing and vision loss interfering with communication and acquisition of information (Jaiswal et al., 2018; Watters et al., 2004). Consequently, limitations occasioned by deafblindness transcend those caused by both sensory impairments and extend not only to interactions with the environment but to interactions with peers (Dammeyer, 2014; Deafblind International, 2020; Möller, 2003).
According to the World Federation for the Deafblind Global report in 2018, deafblindness affects between 0.2% and 2% of the world’s population, averaging approximately 150 million individuals globally, a number likely to be underestimated (World Federation of the Deafblind, 2018). Deafblindness spans across a large spectrum of varying conditions, creating a heterogeneous population categorized into three main groups (Wittich et al., 2013): Group 1 (congenital deafblindness, usually part of a syndrome, i.e., Congenital Rubella Syndrome); Group 2 (acquired deafblindness, often a single sensory—visual or hearing—impairment from birth followed by the acquisition of the other impairment, i.e., Usher Syndrome); and Group 3 (deafblindness due to age-related conditions, i.e., age-related macular degeneration and presbycusis; Dammeyer, 2014; Jaiswal et al., 2018; Wittich et al., 2012). Deafblindness can therefore vary in its nature, degree, and time of acquisition (pre- or post-lingual), thus posing significantly distinct challenges to the individual (World Federation of the Deafblind, 2018).
As a result, this health condition is often under-researched, poorly understood among the general population (Jaiswal, Aldersey, Wittich, & Mirza, 2020; Wittich, Jarry, et al., 2016) and not well recognized in many countries (World Federation of the Deafblind, 2018). Furthermore, deafblindness is often wrongfully classified as a vision impairment, which greatly hinders rehabilitation services (World Federation of the Deafblind, 2018). Individuals with deafblindness thus experience considerable barriers to communication, interpersonal relationships, and social participation as well as limitations in access to information and challenges during mobility (Jaiswal et al., 2018; World Federation of the Deafblind, 2018), all of which can lead to social isolation, low education, and/or employment outcomes, mental health issues (i.e., anxiety, depression), and overall decreased quality of life (Arcous et al., 2020; Jaiswal et al., 2018; World Federation of the Deafblind, 2018).
Additive Manufacturing as Assistive Technology
Assistive technologies have a mandatory role in improving functioning and social participation of individuals with deafblindness (Jaiswal et al., 2018; Jaiswal, Aldersey, Wittich, Mirza & Finlayson, 2020; Perfect et al., 2019; Wittich, Southall & Johnson, 2016; World Federation of the Deafblind, 2018). These encompass products and services aiming to “maintain or improve an individual’s functioning and independence” (World Health Organization [WHO], 2018) such as glasses, prostheses, wheelchairs, hearing aids, white canes, and other electronic aids (de Witte et al., 2018; Ptito et al., 2021; WHO, 2018). However, many companies do not consider investing and innovating for small disabled populations as a profitable enterprise (De Couvreur & Goossens, 2011), which contribute to the scarcity and over-pricing of technologies adapted for individuals with deafblindness. Therefore, growing numbers of rehabilitation professionals express the need for new assistive technology that is adapted to the digital age, affordable, accessible by touch, and customizable for every individual’s unique goals and abilities (Caporusso et al., 2014; de Witte et al., 2018; Perfect et al., 2019; Wittich, Jarry, et al., 2016). Out of the existing technologies on the market, emerging literature now explores the use of additive manufacturing (AM), commonly named 3D printing, as assistive technology to circumvent this lack (Jafri & Ali, 2015; Knochel et al., 2018; Schwartz et al., 2020).
With the significant AM market growth in the past decade (Lopes et al., 2020), AM has become an increasingly popular, accessible, affordable, and useful technology in many sectors including education where it can be used to produce three-dimensional (3D) models for science, technology, engineering, and mathematics (Ford & Minshall, 2019; Gordy et al., 2020; Horowitz & Schultz, 2014; Jafri & Ali, 2015; Novak & Wisdom, 2018). Moreover, emerging evidence explores the proposition of using AM as assistive technology or as a rehabilitation tool for professionals working with students with disabilities such as vision impairments (Buehler, 2016; Buehler et al., 2014; Schwartz et al., 2020; Xu et al., 2017). AM is viewed as an affordable solution to provide custom tactile models (i.e., floor plans, braille templates, etc.) to learners with vision impairments (Anderson, 2017; Holloway et al., 2019; Jafri & Ali, 2015; Wonjin et al., 2016). However, little research has been conducted on its potential use in the field of deafblindness (Bell et al., 2021). Since the sense of touch often becomes the main gateway to information and communication for those with deafblindness, AM presents itself as a potentially beneficial assistive technology that might enable the production of low-cost tactile material (Wonjin et al., 2016). Furthermore, with its automatic process, ease of use and potential for customizability (Conner et al., 2014), AM could easily adapt to meet the rehabilitation needs of individuals with deafblindness in many life domains.
Conceptual Framework
In this review, the life domains that can potentially be influenced by the adoption of AM within rehabilitation services will be categorized according to the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) framework (WHO, 2002). This framework organizes information on functioning and disability related to health conditions and their context, making it useful and convenient to comprehensively assess the impact of technologies on the individual (Möller, 2003). The ICF framework is comprised of six interconnected components centered around the individual: body structure (anatomical); body function (physical and psychological); activity (execution of a task); participation (involvement in life situations); personal factors (e.g., age and sex); and environmental factors (e.g., physical and social; WHO, 2002). Previous studies have used the ICF framework to describe deafblindness (Jaiswal et al., 2019; Möller, 2003; Perfect et al., 2019; see Figure 1) as an impairment in the structure and functioning of the hearing and visual systems that can impair activity and participation domains such as learning and applying knowledge, general tasks and demands, communication, mobility, self-care, domestic life, interpersonal interactions and relationships, and more (Jaiswal et al., 2018; Möller, 2003, 2008).

ICF framework for deafblindness.
Using this framework, it is possible to provide guidance for the development of technologies destined to individuals living with deafblindness or other disabilities (Möller, 2003; Perfect et al., 2019). The ICF is thus an effective tool to define which activity and participation components can be impacted by AM and to assess its potential to improve functioning and quality of life. For instance, 3D models produced using AM are known to be beneficial instructive tools (Arbes et al., 2018; Lipson, 2007) that are often easier to understand than 2D representations (Teshima, 2010; Thompson & Chronicle, 2006) or to serve functional purposes in daily life tasks (Koslow, 2016; Morgan, 2017). However, the generalization of such possibilities to individuals with deafblindness is debatable as the additional hearing loss leads to new and different adaptation challenges related to the impossibility or difficulty to compensate for both sensory losses (Dammeyer, 2014).
Therefore, this scoping review aims to (1) explore and synthesize the current state of evidence on the present and potential practices involving AM, or 3D printing, as a rehabilitation tool for individuals with deafblindness and (2) to identify which life domains, according to the ICF framework, can be improved by its adoption and implementation. The study findings will inform professionals (in rehabilitation, computer science, engineering, and 3D printing services), organizations and policymakers on how this technology can positively affect social participation and quality of life of individuals living with deafblindness (Bleau et al., 2021).
Methodology
This scoping review was performed following the Arksey and O’Malley (2005) methodological framework for scoping reviews using five stages: “identifying the research question,” “identifying relevant studies,” “selecting studies,” “charting the data,” and “collating, summarizing, and reporting the results.” We complemented this framework by reporting definitions of the “population,” “concept,” and “context” of interest as well as the search strategy, searched databases; inclusion and exclusion criteria, and the methodology on data extraction and mapping according to recommendations from Peters et al. (2015). The reporting of this study followed the PRISMA extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018).
Stage 1: Identifying the Research Question
This scoping review was conducted to answer the following research questions: “What is the present state of evidence on the different uses of AM technology as a rehabilitation tool to assist individuals with deafblindness?” and “Which ICF activity and participation domains could AM improve for individuals with deafblindness?” (Bleau et al., 2021). Following the Joanna Briggs Institute (JBI) Evidence Synthesis guidelines, the study population included individuals with deafblindness, their caregivers, and the professionals providing rehabilitation care to them. The concept was related to AM technology as a tool to assist individuals with deafblindness in their rehabilitation (or “all services that seek to improve the individual’s functioning, independence, participation and quality of life”; Bleau et al., 2021). With respect to context, this review considered studies from across the globe, written in English or French and published before January 2022.
Stage 2: Identifying the Relevant Studies
A broad search strategy was developed in consultation with a trained librarian to retrieve relevant published literature in this field. A three-step search was performed:
The first step was to identify and create an extensive list of relevant key terms, subject headings, synonyms, and variations for the two concepts of the study: “additive manufacturing” and “deafblind.” The expanded concepts were linked together with “AND” (deafblind concept AND additive manufacturing concept), resulting in a comprehensive search strategy (see Supplemental Material 1).
The second step was the development of a broad search string. The search was performed in ten scientific databases: PubMED (NCBI), MEDLINE (NLM), EMBASE (Elsevier), Scopus (Elsevier), Engineering Village (Elsevier), Global Health (PSI), CINAHL (EBSCO), PsycINFO (EBSCO), Web of Science (Clarivate Analytics), and ERIC (IES).
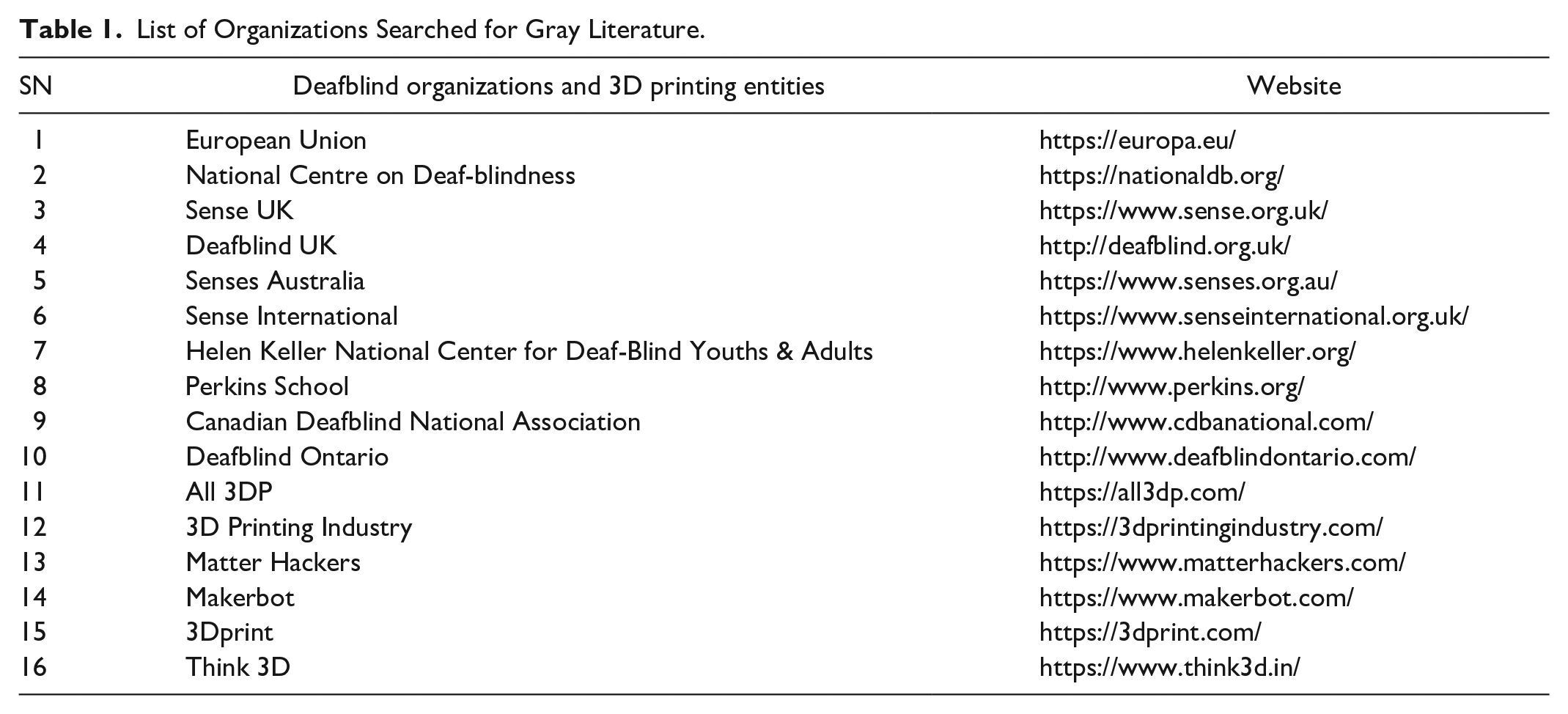
The third step was a “snowballing,” or “ancestry,” method (Atkinson et al., 2015; Jalali & Wohlin, 2012), in which the research team manually searched the reference list of the most relevant articles to find any other relevant article that could be included in the study. In addition, three Google Scholar searches (Blindness AND 3D printing, Deafblindness AND 3D printing, and “Hearing impairment” AND 3D Printing) were performed where the first 100 hits were included in the title and abstract screening. Finally, a gray literature (non-peer reviewed research, unpublished reports, doctoral theses, conferences, etc.) search was performed in deafblindness organizations’ websites (search term: 3D printing) as well as for 3D printing entities (search term: deafblind; Table 1).
List of Organizations Searched for Gray Literature.
Stage 3: Study Selection
All articles identified in the search process were exported to EndNote, a reference management software (Clarivate Analytics, PA, USA), and thereafter exported to Covidence, a screening software for reviews (Veritas Health Innovation, Melbourne, Australia), where duplicates were automatically removed. A two-stage screening process, beginning with the title and abstract screening (in which all studies about vision impairments and AM were pre-included) and then full-text screening, was performed by two independent reviewers to screen and identify the most relevant articles based on the post-hoc inclusion criteria (see Table 2). Any disagreements in the two-stage screening process were resolved by a senior reviewer on the team.
Inclusion and Exclusion Criteria.

Stage 4: Charting the Data
Relevant data from all studies selected through the two-step screening process were extracted into a Microsoft Excel logbook. These data included details such as the name of study and authors, year of publication, study location, study aim, methodology, used AM technology and its application, main outcomes of the study, and any other key findings deemed relevant to answer the research question.
Stage 5: Collating, Summarizing, and Reporting the Results
The findings of this scoping review were presented in tables, graphs, and figures using descriptive numerical analysis and qualitative content analysis (Hsieh & Shannon, 2005). This stage was performed to construct a general portrait of the present literature about the applications of AM technology in the rehabilitation of individuals with deafblindness.
Results
A total of 1,397 studies were identified in the search, of which 1,156 studies were extracted from databases, and 241 were included from Google Scholar, snowballing, and gray literature. After removing 253 duplicates, the remaining 1,144 studies were screened. Finally, nine articles met the criteria and were accepted for data extraction. The rest were excluded because (1) participant samples did not include individuals with deafblindness, their caregivers, or the professionals providing rehabilitation care to them or (2) they did not focus on the use of AM as a rehabilitation tool. Information on the number of studies through all identification, screening and data extraction stages can be found in the PRISMA flow chart (Moher et al., 2009) illustrated in Figure 2.

PRISMA flow chart.
Characteristics of Studies
Of the nine studies that met the criteria, five were empirical studies, followed by three descriptive studies, and one conference presentation. The empirical studies used qualitative methodologies, often including subjective reports in various data collection strategies (e.g., interviews, observations, and workshops). The non-empirical studies were primarily descriptions of devices produced with AM and other technologies (electronics and open-source firmware), and one study included minimum validation of its prototype with participants (opinion on what should be improved). Table 3 provides details on study characteristics such as study location, sample, AM technology and application, and relevant findings. Some studies that focused on individuals with vision impairment as the population of interest have been included in the present review because they involved participants with additional hearing loss or rehabilitation professionals working with clients/students with concurrent hearing and vision impairment (see Table 3).
Characteristics of Included Studies (n = 8).

Most studies (n = 5) were based in Europe, mostly in France (n = 3), Italy (n = 1), and the Czech Republic (n = 1), while two were conducted in the United-States of America and two were collaborations between multiple countries (France, United-Kingdoms, and Australia). One study was published in 2011, while all other studies (n = 8) were published between 2015 and 2021, with 2016 being the year with the most publications (n = 3). None of the studies considered the heterogeneity of the deafblind population (group 1, 2, and 3). One study involved one older adult and one child, four studies involved children, teenagers, and young adults, one involved an adult who was previously deafblind but regained some hearing abilities with the acquisition of hearing aids and, lastly, one study did involve participants with deafblindness, but their ages and condition were not specified. Finally, of nine studies, two used fused deposition modelling (FDM) AM technology, two used colorjet AM technology, and five did not specify the used AM technology.
Identified ICF Domains and Related Uses of 3D Printing
None of the included studies explicitly utilized the ICF framework. However, we were able to categorize studies and their findings into three categories, representing three ICF activity and participation domains (more details in Supplemental Material 2) in which the functioning of individuals with deafblindness can be positively influenced using AM. The main discussed domains were communication (n = 5) and learning and applying knowledge (n = 4), while a third domain, mobility, was identified as a secondary domain in four studies (see Table 3). Furthermore, our team identified three different types of AM applications for rehabilitation. The included studies investigated the use of AM (1) as an independent tool to produce adapted 3D printed material; (2) as a complementary technology to improve or adapt already existing material; and (3) as a technology to be used in conjunction with other Do-it-yourself (DIY) technologies, such as electronic boards and related software to produce custom interactive material. Table 4 summarizes the different AM applications for each of ICF domain.
Applications of AM Technology According to the ICF Domains.

AM and communication
Five studies aimed to develop and present no-tech or low-tech communication devices that are affordable and can improve direct or remote (online) communication (see Table 3). Parker and Sullivan (2018) present the Deafblind Pocket Communicator (https://www.aph.org/product/deafblind-pocket-communicator/), a no-tech and completely 3D printed communication card for the deafblind to communicate with people who do not know any form of tactile sign language. Duvernoy et al. (2017, 2018) present the Hapticomm (http://www.hapticomm.tech/), a low-tech device for independent remote communication co-designed and tested with one author who is deafblind (Duvernoy, 2020). According to the authors, Hapticomm can effectively recognize speech and text and translate it to deafblind tactile fingerspelling language. Bulgarelli et al. (2016) and Johnson et al. (2021) present robotic hands for sign language reproduction, based on the PARLOMA project (https://parloma.github.io/), said to enable independent remote communication (Russo et al., 2015).
As only few individuals with deafblindness were involved in the design process of the Deafblind Pocket Communicator (n = 2) and Hapticomm (n = 1) and in testing the fidelity of tactile hand signs recreated with 3D printable robotic hands (n = 4), these specific AM-based designs remain to be comprehensively tested and validated for their rehabilitation potential in real-life situations. As a result, there is yet no information on the use of low-tech AM-based remote communication devices in rehabilitation services. However, prototypes shown in this review have the potential to enable two-way communication on online platforms with individuals from anywhere in the world without the need for interpreters.
AM and learning and applying knowledge
The other four studies explored the use and utility of AM in the context of education for children, teenagers, and young adults living with vision impairment or deafblindness. Two of these studies (Brule et al., 2016; Voženílek et al., 2011) included deafblind participants. The last two studies (Giraud et al., 2017; Giraud & Jouffrais, 2016) involved rehabilitation and special education professionals who specified working with students that have a vision impairment with additional conditions (i.e., hearing impairment or behavioral disorders). However, all four studies mainly discussed the use of AM for vision impairments and only one reported results obtained from participants with deafblindness (Brule et al., 2016).
Voženílek et al. (2011) tested 3D printed maps to teach hypsometry/orography (or the concept of land elevation, topographic levels of mountains, hills, etc.) in a way that was previously not available and accessible without vision. The three other studies (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016) are from a single research team and investigated the use of AM in the classroom of students with vision impairments (and additional conditions). According to the authors and participants’ reports, AM was considered due to the lack of teaching material that is adapted or touch-accessible and due to the exhaustion expressed by professionals who must manually produce material, which can be expensive and time-consuming. In these studies, various AM-based products (i.e., tactile globes, 3D printed tangibles complementing a tactile map, tactile books, and maps) were introduced to students with vision impairments. The authors concluded that such objects were positively received by students and, thus, increased their motivation to interact with the material provided in class. These also encouraged collaborations between students and allowed for better memorization and spatial learning (Brule et al., 2016).
Furthermore, two studies (Giraud et al., 2017; Giraud & Jouffrais, 2016) focused on the training (i.e., workshops with computer science undergraduate students) of rehabilitation professionals and teachers in using AM in conjunction with other DIY technology (mainly cheap and simple electronic boards) to create interactive prototypes (i.e., tactile books, timelines, city maps, and various tangible landmarks). These prototypes were not tested amongst students with deafblindness but were appreciated by participants for their customizability and adaptability to students’ specific needs. Furthermore, while professionals expressed the need for more training, the use of AM was viewed as empowering, and professionals were prompt to recommend it to colleagues.
AM and mobility
Three studies (Brule et al., 2016; Giraud & Jouffrais, 2016; Parker & Sullivan, 2018) mentioned the potential use of AM to improve mobility. Parker and Sullivan (2018) mentioned the Pocket Communicator’s potential usefulness during daily travels when interacting with the public is necessary (i.e., getting direction information or confirmation in public transports). Two other studies (Brule et al., 2016; Giraud & Jouffrais, 2016) investigated the production of 3D printed tangibles to complement tactile maps. Giraud et al. (2016) reported a scenario where AM was used to represent a bridge on a line map to facilitate the process of learning a route (and the concept of walking underneath the bridge). In Brule et al. (2016), 3D printed tangibles facilitated the acquisition of spatial skills (i.e., cardinal points), enhanced memorization and understanding of spatial data, helped the students learn and prepare a route, and motivated the children to interact with a tactile map (i.e., a student using the 3D printed car as an avatar to move around on the map). However, only one study presented results specific to students with deafblindness (Brule et al., 2016).
Discussion
The goal of the present scoping review was to synthesize the current state of evidence on the present and potential practices involving AM technology as a rehabilitation tool for individuals with deafblindness, and to identify which ICF activity and participation domains can be improved by its adoption within services. According to our search, AM technology has not yet gained the same interest in the field of deafblindness as in vision rehabilitation in general. While evidence of its use for visually impaired individuals is substantial (Jafri & Ali, 2015), studies on deafblindness are still scarce. As of our search, of all 221 studies about AM and vision impairments or hearing loss, we only identified 9 studies corresponding to our criteria and none of these explicitly considered the ICF nor the heterogeneity of the deafblind population (group 1, 2, and 3). While it is clear from the results of this scoping review that there is a lack of research involving AM in service toward rehabilitation goals of those living with deafblindness, its potential applications identified here are important to discuss in the goal to spur further work in this field.
Assessing the Need for AM in Rehabilitation
Full accessibility to services and education still faces practical and financial barriers that are felt and expressed by individuals with deafblindness and rehabilitation professionals (Brule et al., 2016; Wittich, Jarry, et al., 2016). As of our search results, four (Brule et al., 2016; Bulgarelli et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016) out of nine studies explicitly explored the use of AM because of the lack of assistive technology or adapted material that is touch accessible and affordable for individuals and students with deafblindness and/or vision impairments. As a result, individuals with deafblindness, despite their resolve, cannot always access the content they want to learn (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016) and rehabilitation professionals are tasked (or “self-entitled”) with solving this issue using time-consuming strategies that affect their efficiency at work and make them feel “overworked” (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016). The present scoping review has revealed some potential uses of AM as a tool to produce new assistive devices and customizable material to improve the situation of both professionals and individuals with deafblindness.
AM for Communication, Learning, and Mobility
In the present scoping review, the ICF framework was used to classify and evaluate the impact of AM technologies on the functioning of those living with deafblindness. As the results of our search, we were successful at identifying three potential ICF activities and participation domains that can be positively impacted by AM (“communication,” “learning and applying knowledge,” and “mobility”), providing more insights on how AM can be used to improve the quality of life of individuals living with deafblindness in accordance with the Expanded Core Curriculum (Provincial Resource Centre for the Visually Impaired [PCRVI], 2022). AM can improve social interaction skills, compensatory skills, recreation and leisure skills, access technology skills, orientation and mobility skills, and even independent living skills (PCRVI, 2022).
Communication
One of the main limitations that set deafblindness apart from vision impairment is the difficulty to compensate for sensory loss in one sense by using the other impaired sense (Dammeyer, 2014). Relying mostly on the sense of touch to communicate, individuals with deafblindness will learn differently and at a different rate than people with vision impairment alone (McInnes, 1999). To overcome this limitation, AM can help in producing more affordable devices that enable direct and remote communication (Bulgarelli et al., 2016; Chirila et al., 2020; Duvernoy et al., 2019; Johnson et al., 2021) with peers who are inexperienced with tactile sign language (Parker & Sullivan, 2018). Open source projects identified here (Bulgarelli et al., 2016; Duvernoy et al., 2017, 2019) are prime examples of the potential of AM in enabling the affordable production of devices within rehabilitation centers when equivalent technology is lacking or too expensive. Furthermore, AM could give access to products that might not even be commercialized yet, as is the case for robotic hands for fingerspelling (Gilden & Jaffe, 1988; Jaffe, 1994). Thus, AM can be efficient in reducing the communication barrier that keeps individuals with deafblindness from independently interacting with others.
Learning and applying knowledge
AM can be a useful tool for education in the field of deafblindness. For instance, 3D printed models, as they can be automatically produced with varying resolution and complexity, can provide the means for more stimuli and occasions to learn. These models can expand the number of accessible concepts (Voženílek et al., 2011), motivate students, and encourage classroom collaboration (Brule et al., 2016). The studies we identified reveal that AM-based prototypes trigger positive emotions among these students, thus increasing their curiosity, as well as their ability to interact with the learning material, brainstorm ideas, and discuss concepts in the class (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016). It is even testified that it can equip them with material otherwise too expensive and, thus, decreasing the real and felt barriers to accessibility of learning (Brule et al., 2016).
Mobility
AM can also be a useful tool for orientation and mobility (O&M) lessons. Essentially, 3D printed tangibles can be used to improve traditional tactile maps (Brule et al., 2016; Giraud & Jouffrais, 2016). Such tangibles can be customized and interesting for students, thus motivating during the exploration and learning of tactile maps (Brule et al., 2016). A 3D printed object can be used by the student to explore a map (i.e., minifigures), can represent landmarks and facilitate memorization of important spatial information (i.e., route or general lay-out) to stay oriented when the real environment is experienced (Brule et al., 2016; Giraud & Jouffrais, 2016). As a tool for O&M specialists, AM can also facilitate teaching important concepts that are inaccessible with traditional 2D methods, such as occlusion, buildings’ dimensions (i.e., scale, height), or even land elevation (i.e., slopes and curbs), which are useful cues to learn routes (Giraud & Jouffrais, 2016; Holloway et al., 2018; Thompson & Chronicle, 2006; Voženílek et al., 2011; Figure 3).

AM applications and ICF activity/participation domains. We identified applications in three domains: communication, learning and applying knowledge, and mobility.
While this review only identified three ICF activities/participation domains in which AM can have a positive impact, it is possible to hypothesize, given the literature on vision impairments, that AM may also impact other domains impaired due to deafblindness. In learning, AM could be used to enhance braille learning with projects such as Tagalog and Fittle (used in the deafblind program at Perkins School for the Blind, https://www.perkins.org/; Arbes et al., 2018; Jain et al., 2018; Kleck, 2020). AM could also improve functioning in ICF domains such as “self-care” (i.e., 3D printable printlets project; Awad et al., 2020; Wong et al., 2020), “domestic life” (i.e., tagging systems for color and adaptations for appliances; Guo et al., 2017; Ramsamy-Iranah et al., 2016); and even “community, social and civic life” notably by enabling tactile adaptation of popular leisure activities and improving accessibility to art (with the tactile translation of paintings and recreation of sculptures), architecture, and cultural sites (Gabry, 2018; Karastoyanov et al., 2019; Montusiewicz et al., 2018; Rossetti et al., 2018; Voigt & Martens, 2006; Watkin, 2016). Furthermore, even though most AM studies focus on younger populations in the context of education, 3D printed models can also be useful to older people (i.e., group 3 with age-related deafblindness). Since tactile sensitivity is known to decrease with age and/or with other conditions more prevalent in older populations (Stevens, 1992), handling 3D models might prove advantageous as it involves additional proprioceptive feedback (Norman et al., 2011). In practice, emerging projects involving older adults explore the use of AM to design simpler tactile maps with less reliance on abstract symbols (Palivcová et al., 2020), and improve telerehabilitation (Zhang et al., 2020), a now relevant need in the context of the COVID-19 global pandemic. Nevertheless, it is likely that numerous possible applications of AM are yet to be discussed and tested.
Students, Professionals, and Care Providers’ Empowerment
The most promising aspect of AM is its ability to empower professionals by enabling them to produce and customize their own material while also involving their students or clients in the design process (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016; Hurst & Tobias, 2011). AM thereby can create new material and assistive devices that meet the unique demands and needs of their clients. Studies found in this review suggest that taking their ideas into consideration when producing assistive devices and material with AM is found to be more motivating, interesting and engaging, all factors that are known to increase assistive technologies’ adoption rate (Bailey et al., 2015; Brule et al., 2016; Hurst & Kane, 2013; Hurst & Tobias, 2011; Phillips & Zhao, 1993). Furthermore, as AM’s affordable and automatic process can contribute to ease professional’s workload and thus decrease exhaustion (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016), AM shows potential for rapid adoption by professionals and by individuals with deafblindness. Results of this scoping review thus suggest that AM can offer a more engaging and empowering solution to the current lack of adapted material that contributes to the feeling of disability (Brule et al., 2016). AM can allow students to become actors in their own learning process, rather than feeling “disabled” (Brule et al., 2016). However, such projects are still very rare in the field of rehabilitation, notably due to certain significant limitations.
AM Limitations
It is important to note that some factors might limit the adoption of AM within rehabilitation services. The present review identified limitations related to the user experience with AM-based products and intrinsically related to AM technology. Primarily, individuals with deafblindness might not be used to AM-based objects, which can delay or impede the ability to learn from such objects without familiarization or special training (Taylor et al., 2016; Voženílek et al., 2011). The AM process can also cause artifacts that can decrease the usability and appealability of models: these can appear as stringing, apprehended pointy edges (Brule et al., 2016), or lines and rough surfaces that can be confounded with important information (Taylor et al., 2016). Finally, one of the most limiting factors for AM adoption by professionals is the level of skills and expertise it requires. On the one hand, 3D printers necessitate frequent setup, calibrations, and maintenance to assure quality prints (Go & Hart, 2016). On the other hand, adapted 3D models are not always available online: creating and preparing models to print also require new sets of skills and knowledge (Giraud et al., 2017; Go & Hart, 2016). Consequently, professionals can still be reluctant to use AM due to the expertise needed to use it (Giraud et al., 2017).
AM and the Need for Interdisciplinary Collaborations
While studies (Bulgarelli et al., 2016; Duvernoy et al., 2019; Giraud et al., 2017; Giraud & Jouffrais, 2016) identified in this review show that it is possible to produce AM-based assistive devices for the use of individuals with deafblindness, the complexity of using AM and other DIY technologies can be overwhelming for numerous users (Giraud et al., 2017). It is therefore important to highlight the need for collaborations between rehabilitation professionals and other specialists (i.e., engineering and computer sciences) to conceptualize, produce, and validate new AM applications, as well as to train rehabilitation professionals in the use of AM and other DIY technologies. Such collaborations and training easily lead to greater motivation and satisfaction among rehabilitation professionals and make them more eager to seek further expertise that expands their possibilities (Giraud et al., 2017; Giraud & Jouffrais, 2016; Russo et al., 2018). Hence, specialists with expertise in AM should be encouraged to provide tools, resources, tutorials, and workshops to care providers and rehabilitation professionals seeking to better meet the needs of individuals with deafblindness. AM technology, paired with relevant training, could improve the quality of rehabilitation services given to individuals living with vision impairments or deafblindness (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016).
Limitations of the Study
Albeit the increasing number of studies on the use of AM for individuals with vision impairments, the current AM literature offers limited insight on its usability in the field of deafblindness. Only five of the included studies (Bulgarelli et al., 2016; Duvernoy et al., 2017, 2019; Johnson et al., 2021; Parker & Sullivan, 2018) specifically focused on AM for the deafblind, while the other four (Brule et al., 2016; Giraud et al., 2017; Giraud & Jouffrais, 2016; Voženílek et al., 2011) focused on its use for students with vision impairments in general. Consequently, the comprehensiveness of the review’s findings is limited due to methodological constraints (small sample sizes, qualitative paradigms such as observational reports, AM-based devices not comprehensively tested, limited or missing involvement of individuals with deafblindness). As a result, challenges specific to people with deafblindness are not always explicitly investigated and more rigorous research is necessary to validate the potential role of AM in deafblindness rehabilitation. Future work involving participants with deafblindness should consider their distinct challenges and needs (Jaiswal et al., 2018; Jaiswal, Aldersey, Wittich, & Mirza, 2020) to sustain the growth of deafblindness services and research, involving the adoption of AM and AM-based products in the service of their rehabilitation goals (Jaiswal et al., 2018).
Finally, the present scoping review and the comprehensiveness of its findings are subject to limitations related to language and accessibility. First, this study, in its design and in the development of search strings written solely in the English language, was limited to articles published in English or French, although possible studies might be available in other languages. Second, the present study was also limited by the access to studies available through the University of Montreal’s library or through open-access journals and databases.
Conclusion
The present scoping review identified potential uses and benefits of AM for individuals living with deafblindness and for professionals working with them in three main ICF activity/participation domains: “communication,” “learning and applying knowledge,” and “mobility.” The potential of AM mainly resides in its ability to produce custom assistive devices and adapted educational material fitted to individual needs. AM could thus help counter the lack of assistive technology that forms a barrier to full accessibility and contributes to the disabling experience among individuals with deafblindness. However, AM projects involving individuals with deafblindness remain rare, thus showing the need for more research and open-source AM-based assistive technology. Interdisciplinary collaborations for training purposes may also allow rehabilitation professionals to offer better and more personalized services with the use of AM, thus improving the experiences, social participation, and quality of life of people living with deafblindness.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440221117805 – Supplemental material for Applications of Additive Manufacturing, or 3D Printing, in the Rehabilitation of Individuals With Deafblindness: A Scoping Study
Supplemental material, sj-docx-1-sgo-10.1177_21582440221117805 for Applications of Additive Manufacturing, or 3D Printing, in the Rehabilitation of Individuals With Deafblindness: A Scoping Study by Maxime Bleau, Atul Jaiswal, Peter Holzhey and Walter Wittich in SAGE Open
Footnotes
Acknowledgements
We would like to acknowledge the support from Francine Baril in building the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant awarded to WW from the Center for Interdisciplinary Research in Rehabilitation of Metropolitan Montreal (CRIR; Programme «Nouvelles initiatives» 2019–2020). AJ is a recipient of the Health System Impact Postdoctoral fellowship that is jointly funded by the Canadian Institutes of Health Research, the Fonds de recherche du Québec—Santé (FRQS), and the Institut Nazareth et Louis-Braille du CISSS de la Montérégie Centre (INLB; Funding reference number: HI5 166371). WW is supported by an FRQS chercheur boursier Junior 2 career award (#281454).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.