
Abstract
Nurses can understand and evaluate the impact of neuroscientific and neurotechnological advancements (NNA) from multiple standpoints given their roles as patient liaisons, advocates for their profession and their clients, leaders, and educators as well as their interactions with NNA such including deep brain stimulation and neuroimaging. We conducted semi-structured interviews with Canadian nurses to understand their perspectives on their roles in and outside the workplace, their familiarity with NNA and their ethical, legal, and social implications, their participation in NNA governance discussions and how lifelong learning can be applied to empower their participations in NNA governance discussions. Participants felt that nurses had the potential to meaningfully involve themselves in NNA governance discussions if given a greater opportunity. Participants were not offered lifelong learning surrounding the ethical, legal, and social implications of NNA. It would be fruitful to facilitate and empower nurses as contributors to NNA governance and ethics discussions.
Background
With over 300,000 active professionals, registered nurses (RNs) are Canada’s largest group of healthcare providers (Canadian Institutes of Health Research, 2020). Nurses are exposed to and interact with many scientific and technological advancements that include neuroscientific and neurotechnological advancements (NNA), technological advancements that interact with the human nervous system (Barbe et al., 2014; Ong et al., 2017; Vidal et al., 2013). Neuroethics and neurogovernance are two discourses that emerged to engage with the associated ethical, legal, and social implications and governance of NNA (Garden et al., 2016; Garden & Winickoff, 2018; Northoff, 2009). In their occupations, nurses are expected to uphold multiple formal and informal roles including being leaders, political activists, advocates patient liaisons and educators (Downey et al., 2011; Gregor, 2001; Tourigny & Pulich, 2005). Outside of their occupation, nurses are also members of society and therefore can also have a role as active citizens. Lifelong learning opportunities are a means to enhance and develop the roles that nurses hold as professional and active citizens (Garden & Winickoff, 2018; Racine, 2015). Stakeholder engagement is one main focus of the neuroethics and neurogovernance discourses (Garden et al., 2016). Given the roles expected to be fulfilled by nurses and their exposure to NNA, nurses should have a stake in how NNA are discussed in neuroethics and neurogovernance discourses. However, nurses are still invisible in neuroethics and neurogovernance discourses, (Deloria & Wolbring, 2019). The objective of our study is to explore the familiarity of nurses with NNA and their implications; examine the perspectives of nurses on their roles within their occupation and in relation to NNA, neuroethics, and neurogovernance discourses and furthermore, understand the current lifelong learning processes in place for nursing professionals and the potential of lifelong learning to entice and empower nurses to contribute in a meaningful way to NNA, neuroethics, and neurogovernance discussions.
Nursing Role
Canadian nursing standards and leadership outline that nurses encompass a variety of roles in their occupation that include employee/worker, advocate, authority, educator, active citizen, and leader (Canadian Nurses Association, 2009, 2015, 2017). Nursing practice constantly changes and has expanded outside of hospital settings to also impact faith communities, schools, professional organizations, government agencies, and outreach whereby nurses are expected to adapt and deploy a variety of skills to fit each setting (Canadian Nurses Association, 2015). Specialty practices and certifications provide nurses with expertise related to certain populations or health concerns that include age (e.g., geriatrics) and type of care (e.g., palliative care, public health, psychiatry etc.) (Canadian Nurses Association, 2015).
Nursing and Active Citizenship
“Nursing is a practice discipline and it is also a political act” (Canadian Nurses Association, 2009).
The nursing practice immerse nurses in a variety of roles and skills that are not limited to medicine. Political activism and nursing are familiar intersections throughout history. Historical nursing figures such as Florence Nightingale (1859) exercised their political advocacy and activism to shape the climate of nursing as it stands today. Florence Nightingale (1859) understood that societal changes were necessary to navigate and implement appropriate healthcare standards and sanitation for clients in the clinical setting and the greater public. Today, it is standard practice for nurses to exercise advocacy in their roles for their clients, for themselves and for their staff (Abbasinia et al., 2019; Tomaschewski-Barlem et al., 2018). Nursing advocacy can be broadly defined as the promotion of the nursing profession towards the greater public or the nurse acting on behalf of their clients their families, and greater society (Hanks, 2008). It is noted that nurses are best suited for patient advocacy due to their close proximity to patients (Des Jardin, 2001; Mahlin, 2010). Although nurses promote advocacy in their clinical settings, social advocacy, and political activism does not end in their professional roles. Active citizenship can be promoted through advocacy. Active citizenship takes individual values and promotes them through democratic, non-violent means in the individual participation in political life, civil society, and their surrounding communities (Hoskins et al., 2006). Active citizenship is guided through the collective and authoritative action of the public to push forth their interests and further enhanced by learning opportunities. Nurses are expected to act as active citizens to utilize the collective and authoritative action as members of the public to push forth their interests outside of their profession (Bauer et al., 2012; Canadian Nurses Association, 2009; Stivers, 1990). It has also been recognized that lifelong learning is a tool that can be used to build up nursing role competencies that include political activism and advocacy (Ellenbecker et al., 2017; Williams et al., 2018).
Lifelong Learning
The Canadian Nurses Association (2004, 2007, 2009) acknowledges the importance of lifelong learning initiatives towards the quality and competencies of nurses across Canada.
Lifelong learning and professional development are regarded as integral to the practice of nursing. It is recognized that nursing does not end at the undergraduate and pre-occupational levels (Kapborg & Fischbein, 1998). Lifelong learning initiatives allow nurses to feel competent and well-prepared in their roles, maintain overall job satisfaction and be up to date in a constantly changing healthcare environment (Baker, 2010; Danielson & Berntsson, 2007; Gould et al., 2001, 2007; Shermont et al., 2009). As well, lifelong learning opportunities provide the needed knowledge for nurses to take an active and political role in and out of their occupation (Faulk & Ternus, 2004; Gehrke, 2008; Staebler et al., 2017). Lifelong learning initiatives are reflected in the quality of nursing profession through updated patient care, awareness of new innovations and technologies, development and acquiring skillsets, and obtaining the relevant knowledge needed for change and advocacy (Canadian Nurses Association, 2004, 2007, 2009; Gopee, 2005).
NNA, their Governance, and Nursing
NNA are products and processes that stimulate, enhance, or connect with the nervous system (Garden et al., 2016; Müller & Rotter, 2017). Many nurses are exposed at work to NNA that include, deep brain stimulation (Lanier & Buffum, 2011), transcranial magnetic stimulation (Bernard et al., 2009; Fitzsimons et al., 2009), neuromodulation (Mendez et al., 2012), neuroimaging (Holohan et al., 2013), and virtual reality (Choi, 2017; Elliman et al., 2016). In recent years, neuroethics and neurogovernance discourses emerged to investigate the ethical, legal, and social implications and the governance of NNA (Garden & Winickoff, 2018; Northoff, 2009; Roskies, 2002). The societal discussions of science and technology advancements should be a constant endeavor (Cheung & Wolbring, 2017; Einsiedel, 2004). Neurogovernance and neuroethics fields note that it is important to integrate the issues associated with NNA into education platforms so that the public and professionals can anticipate change and impact (Garden & Winickoff, 2018; OECD, 2002; OECD’s Centre for Educational Research and Innovation [CERI], 2005).
Given the potential exposure to various NNA in their occupation and role expectations such as leaders, educators, and advocates for their clients and their profession, it can be suggested that nurses also have a role as relevant influencers in neuroethics and neurogovernance discourses. Furthermore, as NNA also impact society outside of the clinical setting, nurses also have a role to play in NNA public debates as active citizens. Lifelong learning and professional development procedures used by nurses to stay up to date for their work can be used to entice and empower nurses to be influencers of neuroethics and neurogovernance discourses. In recent years, various studies have looked at the linkage between healthcare professionals and the ethical, legal, and social implications of NNA (Bell et al., 2009, 2016; Bell & Racine, 2013; Deloria & Wolbring, 2019; Villamil & Wolbring, 2019). The objective of our study was to add to the literature engaging with health professionals and NNA whereby we investigate the perspectives of nurses to understand their perspective on their roles as professionals and active citizens in neuroethics and neurogovernance discussions and the utility of lifelong learning to empower their involvement in neuroethics and neurogovernance discussions.
Methods
Design
The qualitative method for this study followed role theory to analyze how the nurse identity was shaped by the roles they associate with and the language used to frame their identity in relation to their occupations, lifelong learning, active citizenship, and NNA (Biddle, 1986). We employed semi-structured qualitative interviews to investigate how nurses perceive NNA, their roles as nurses and how these may apply to NNA and the neurogovernance and how these concepts interact in their occupation and their personal lives.
Data Collection
Purposive sampling was employed, and participants were recruited through email and word of mouth (Palinkas et al., 2015). Inclusion criteria required participants to identify as a nurse licensed to practice in Canada. Given that this study aimed to recruit a relatively homogenous population, the saturation of data was estimated to appear around 10 interviews (Boddy, 2016; Sandelowski, 1995). This number was reflective of gathering a sufficient size for appropriate thematic qualitative data analysis to capture the aspects of the group. To offer room for flexibility, a total of 12 Canadian nurses were recruited for the study and included nurses in Alberta and Manitoba. All participants had the option to conduct the interview through phone or in-person. Of the 12 participants, the 11 participants in Alberta opted for a face-to-face format and the 1 participant in Manitoba requested a phone interview.
Interview
Data were drawn from one interview with each participant conducted at settings chosen by participants for convenience and comfortability that included homes, libraries, and cafes as well as a phone interview, no follow up interviews were conducted. All 12 interviews ranging between 45 and 60 minutes were conducted between May 2019 and July 2019, and each interview was subsequently audio-recorded and transcribed verbatim (Yoosefi Lebni et al., 2020). A semi-structured interview format was employed to guide the flow of conversation and clarify meanings. A 41 question research protocol was developed by the researchers making use of prior research and knowledge of the researchers identifying gaps in the literature; focusing on nurse’s views on emerging NNA, and their ethical, legal, and social aspects, the understood role of the nurse in general and in relation to neuroethical and neurogovernance discussions and their views on lifelong learning within the nursing profession and its utility for enhancing the abilities of nurses to take part in neuroethical and neurogovernance discussion.
Ethics
This study received ethics approval from the University of Calgary Research Ethics Board (REB17-0785). All ethical concerns including privacy and confidentiality were outlined in the informed consent form provided to participants prior to the start of the interview. Participation in the study was completely voluntary, and participants were able to withdraw from the research process at any point until the completion of the interview. Prior to completing this interview, participants were asked to confirm their responses, or make any changes as needed. Throughout the interview process, all participants were assigned pseudonyms to uphold confidentiality and privacy, and no questions were linked to an identifiable person or associated with any response.
Data Analysis
The audio files from the semi-structured interviews were orthographically transcribed by the author using the Express Scribe playback software and Microsoft Word and then saved into a PDF format (Davidson, 2009). Raw data from the transcribed interviews were organized, analyzed, and coded using the ATLAS.Ti 8™ qualitative analysis software. Themes and concepts were then derived through the thematic content analysis of decontextualization and recontextualization of the raw interview data. Both authors first read through the interviews to familiarize themselves with the content. The first author conducted a content analysis of the transcribed interviews using the ATLAS.Ti 8™ software to organize ideas and concepts coded throughout each interview. Themes were grouped according to relevance, meaning, the research questions, and frequency.
Trustworthiness Measures: Peer Debriefing
The trustworthiness measures outlined by Guba and Lincoln (1994), were employed for qualitative analysis. Confirmability, as noted by Lincoln and Guba is achieved once transferability, dependability, and credibility measures are ensured during the research process (Lincoln, 1985). Confirmability is achieved when researchers’ interpretations are clearly derived from the data (Tobin & Begley, 2004). A latent coding process was performed on the 12 interview transcriptions to identify themes and ideas. To enhance credibility, the two authors working on this project engaged in peer debriefing. The authors engaged in a peer debriefing process to develop new themes and codes as well as settle differences in understanding and interpretation of the interviews. Themes generated by each author were regularly discussed to create a cohesive and encompassing interpretation of the data. Reflexivity and confirmability was practiced by the authors through the recognition of positionality throughout the project and the research process (Bourke, 2014). Both authors do not identify as nurses, and the study is approached by both authors as learners to recognize the expertise that lies in the participants experiences. As qualitative interviews were conducted, the interpretations of each author were considered to confirm meaning and definitions as indicated by interviewees and remain as accurate as possible to the stories expressed by participants. Reflexivity throughout the data analysis process was practiced through the consistent recording of thoughts, feelings, and interpretations. Each author created an audit trail through notes and codes in ATLAS.Ti 8™ to ensure that they were communicating ideas and thoughts throughout their own coding process for dependability measures (Koch, 1994). This study was not intended to be generalizable due to the specifics and nature of the sample; however, the data provided allows for transferability of relevant information needed for the public to decide whether to utilize a similar investigative process.
Results
The results of this study will outline participant backgrounds, and then further outline key themes and subthemes that were identified during the interviews (Table 1).
Overview of the Themes and Subthemes Outlined by the Views of Canadian Nurses.
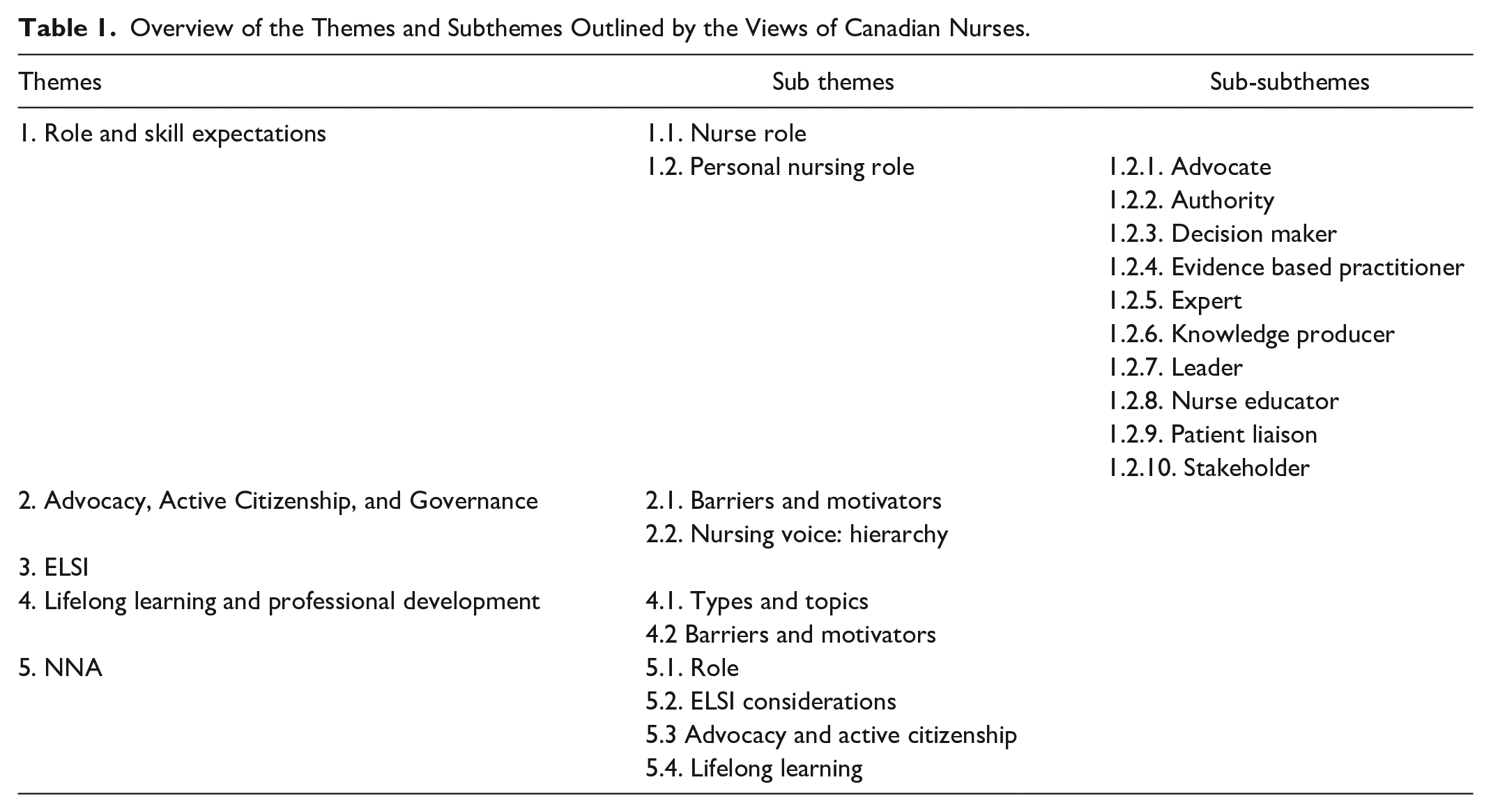
The majority of participants (n = 11 out of 12 participants) in our study were female and undergraduate degree holders (Table 1). The participants ranged from their early twenties to their late fifties and held multiple occupational backgrounds throughout their nursing career that included palliative care, public health, post-secondary education, and neuro (Table 1). Formal workplace roles identified by participants included bedside nurse, researcher, and unit manager (Table 2).
Participant Characteristics.

Note. IEN = internationally educated nurse; BCN = bridge to canadian nursing program.
Role and Skill Expectations
Participants determined the role expectations that they held for nurses in general and the expectations that they held for themselves in their current profession. In some cases, participants held onto the notion of ideal roles for themselves and their colleagues, but relented that due to their scope of practice, the formal role that they had as well as the fear of burn out discouraged them from practicing certain skills or roles they wanted.
Nurse Role
Participants were asked what critical skills and roles they determined nurses should uphold. Participants identified that clinical skills such as dressing changes, and patient assessment were critical for nurses to practice (n = 11 out of 12), however they also identified that professionalism (n = 2 out of 12), accountability (n = 3 out of 12), communication skills (n = 8 out of 12), research experience (n = 2 out of 12), task orientation (n = 1 out of 12), empathy (n = 3 out of 12), and holistic knowledge (n = 6 out of 12) were also important skills for a nurse. The participants were further asked of their opinions on nursing leadership and framework of practice for Canadian nurses (Canadian Nurses Association, 2015; Huston, 2008).
All nurses responded positively to the roles and skills outlined and indicated that this was the ideal role that nurses should uphold in practice. However, some nurses (n = 7 out of 12) indicated that although this sentiment was ideal, it was not necessarily achievable.
All participants identified strongly with being a nurse and they emphasized the importance of their roles as nurses. However, potential for burnout and lack of passion for nursing was identified to be a threat. Participants (n = 10 out of 12) identified that the environment that they are placed in has a large role in shaping the motivation and drive for their occupation.
Personal Nursing Role
Participants identified skills and expertise that were unique to their unit specialty and their formal occupational roles. These expectations became more specific depending on the role that a nurse was in. The participants identified that for certain roles, additional certification and learning was required. Although basic knowledge and training is consistent, the expectations for a psychiatric unit nurse, for example, differed from a vaccine coordinator. The nurses were asked if they identified with a list of roles that they were provided with and were asked to justify their responses (Table 3).
Nursing Roles Participants Identified With.

The majority of participants saw themselves actively using these roles inside and outside of their occupation.
Advocate
Within their occupation, all participants outlined that they were advocates for their client’s safety and quality of care. Participant’s advocacy reflected their current occupations and the type of clients that they interact with. All participants indicated that they were not only advocating for the patients that they interact with, but also for the staff and fellow nurses.
Authority
Participants who identified as authorities were hesitant to fully accept the role as an authority (n = 7 out of 12).
Participants reasoned that due to experience, knowledge, or formal occupational role, others would perceive them to be an authority. One participant outlined that their authority was relative and was present both within their occupation as a nurse and outside of their occupation as a mother.
Decision maker
Participants identified as decision-makers given their occupational roles and responsibilities (n = 11 out of 12).
One participant relented that although they made nursing decisions, they were not in the position to be the ultimate decision-maker and acknowledged other roles and individuals to be responsible for the highest level of decision making.
Evidence-based practitioner
All participants indicated that they were evidence-based practitioners and indicated that this was necessary due to the changing nature of healthcare to continue to provide updated and quality care for their clients as well as understand their practice and the importance of their roles.
Expert
All participants acknowledged that they were experts in their areas due to their skills, knowledge, experience, and passion for their roles. One participant indicated that although they did not have much experience, expertise is determined through the ability to be open to change and development as a nurse.
Knowledge producer
Participants who acknowledged themselves to be knowledge producers (n = 10 out of 12) indicated that they were conducting research formally or disseminating and developing knowledge from their experiences and expertise in the field.
Some participants identified knowledge production to be a formal process and moved away from the title knowledge producer (n = 2 out of 12).
Leader
All participants were more accepting of the term leader over authority. Participants indicated that they were leaders formally through their occupation role or informally through seniority communication and mentorship.
Nurse educator
Participants identified as a formal nurse educator (n = 7 out of 12) or an informal nurse educator (n = 5 out of 12). Participants indicated that formally and informally they were educating clients on treatments, communicating with staff, and also mentoring students and junior staff.
Patient liaison
All participants identified as a patient liaison in their occupations even though some participants did not work with patients directly in their formal roles. Participants identified themselves as interpreters for the patients and other staff members to ensure that patients understand and are acknowledged.
Stakeholder
Participants identified that they were stakeholders in their occupation and that their voices were valuable and necessary as health professionals (n = 10 out of 12).
Some participants (n = 3 out of 12) identified that their stake is multifacted they carried their role as a stakeholder in different areas of their occupation and outside of their occupation as well. However, others expressed that due to their positions and limited expereience, they were not in the position to be relevant stakeholders (n = 2 out of 12).
Advocacy, Active Citizenship, and Governance
Most participants (n = 11 out of 12) viewed themselves as potential active citizens inside and outside of their workplace. Participants expressed that they had a multi-faceted role that allowed them to participate and advocate for separate topics in the workplace and in their personal lives. Inside the workplace, participants expressed that they were passionate about ethical practice, particularly patient and client safety as well as preventing burnout and fighting for staff rights. Some nurses acknowledged that active citizenship is a multi faceted role and outlined issues that they were active outside of the workplace.
Participants outlined that they hold different priorities and roles inside and out of the workplace and these conversations differ on the environment that they are part of. Participants (n = 7 out of 12) indicated that their roles inside and outside of their occupation were balanced when trying to influence policy.
Barriers and motivators
Participants were currently active in issues related to their occupation (n = 11 out of 12) however, other participants however expressed that it was difficult to be active outside of their occupation, and this is not a huge priority at the time (n = 7 out of 12). Participants reasoned that there was limited time at the moment to further participate in their community given their circumstances as a parent and time spent at work, however hoped that this sentiment would change through time. Participants who were older expressed being more involved in the community against counterparts who had younger children.
One participant indicated that there were constraints within their role in their occupation that limited what they felt that they were able to speak out about in policy.
Nursing voice: Hierarchy
Participants all expressed that they had a voice and their opinions were relevant and important, however they expressed that their voice was not necessarily acknolwedged by others. Participants reasoned that this limited the magnitude of nursing voices in policy and discussions.
Two participants expressed the struggle for nursing involvement in boards and discussions. If nurses felt passionate about a topic, the limited room for involvement in higher discussions was a deterrent to get involved.
Participants expressed that they would relent issues to higher powers such as their boards to become the voice for them if the did not feel that they were heard. If participants were not confident in particular areas, they felt that they needed to defer to and learn more before they felt comfortable enough to be a relevant voice.
ELSI
Participants were asked about their understanding of ethical, legal, and social issues in their occupation and how these manifested. Participants were asked to provide scenarios on areas where there would be ELSI concerns and considerations and how important it was for them to consider them in their current roles or in nursing in general. All participants outlined how important ELSI was in their occupations and the impacts of their decisions in practice. Most participants (n = 8 out of 12) recognized that although the principles underlie their practice, ELSI is not always a main thought. It was acknowledged by these participants (n = 8 out of 12) that the daily workload for nurses leaves little room for them to critically think and consider the impacts of their work.
Participants indicated that patient safety, respect, delivery of services, and informed consent were ethical factors that they considered. All participants indicated that they had a legal obligation as nurses to practice safely and ethically. In comparison to ethical implications, participants indicated that the legal aspects of care were not necessarily practiced or considered as often. Some participants (n = 7 out of 12) indicated that for example, informed consent, privacy, and appropriate documentation were legal considerations that they took in their occupation. The social, broader impacts of their occupation were not as heavily considered as the ethical impacts. Nurses indicated that interpersonal impacts and impacts in their occupation have the potential to affect a larger picture and affect the lives of individuals and the quality of care that they receive.
Lifelong Learning and Professional Development
Participants were asked about the lifelong learning and professional development opportunities in their occupation and if engagement with these opportunities enhanced their occupational roles. All the participants deemed lifelong learning as an important and necessary component of their practice. Participants indicated that due to the changing nature of medicine and society, it was imperative that they constantly engage in lifelong learning to remain competent and competitive in the workforce. Participants who were in formal leadership and education positions (n = 7 out of 12) indicated that they needed to constantly build on their knowledge in order for the information to trickle down appropriately.
Types and topics
The following Table 4 outlines the types of lifelong learning opportunities and the topics that participants were aware of and engaged with. Participants all agreed that there were lifelong learning opportunities always available in their occupation with a variety of topics offered.
Types and Topics of Lifelong Learning Opportunities Expressed by Participants.

Barriers and motivators
Participants in academia and in the private sector had a greater opportunity and benefits to accessing educational opportunities (n = 3 out of 12). One participant in academia indicated that alongside professional development days, they were provided with a professional development account with funds allocated to finance various conferences, seminars, or workshops that they wished to attend. Those who were employed under the public health services (n = 8 out of 12) were offered three lifelong learning days and had access to online learning platforms. Those in the private sectors (n = 1 out of 12) had access to lifelong learning on online databases and were offered professional development days. However, frontline nurses (n = 9 out of 12) indicated that staffing and external expenses associated with conferences and workshops were not always guaranteed and therefore limited the amount that they were able to access. Participants indicated that although these opportunities were available, pursuing lifelong learning was difficult for those on the frontline (n = 10 out of 12). Some participants revealed that although they were aware of opportunities, they have not pursued more education themselves due to factors such as limited funding, and lack of paid time off. Participants identified that factors such as time, financial constraints and interest in the opportunities deterred them from pursuing more lifelong learning opportunities (Table 5).
Barriers and Motivators to Lifelong Learning and Professional Development.

One participant identified that the environment on the unit is a large influence on pursing learning opportunies, and found that it was sometimes frowned upon to pursue further learning.
Some nurses (n = 8 out of 12) outlined that because educational opportunities are often taken outside of work and into personal time, it causes potential for disinterest and burnout.
Participants (n = 5 out of 12) indicated that aside from financial support, a positive learning environment and support for learning was an important motivator to pursue learning opportunities.
NNA
Participants were given the NNA topic to gauge their awareness and understanding of various societal issues and how they applied their roles and lifelong learning to this issue. Many of the nurses (n = 9 out of 12) engaged positively with role expectations and lifelong learning initiatives in general but were hesitant to apply such areas if they did not currently witness NNA impacting their occupations. Participants were given a list and asked what types of NNA they were familiar with (Table 6).
Participant Familiarity with NNA.

The participants were asked if they interacted with these technologies in their occupation. Many of the participants indicated that they were aware of the uses of NNA and were aware that some clients went off unit to receive therapies related to NNA, however most participants (n = 8 out of 12) themselves did not interact or administrate these therapies to clients aside from utilizing virtual reality as a teaching tool for upcoming nurses (n = 1 out of 12) or providing cognitive enhancement medication (Adderall, Vyvanse, etc.) for patients that required this treatment (n = 3 out of 12). One participant in psychiatry outlined another NNA not indicated on this list, electroconvulsive therapy, and its potential uses on clients on the unit. Although other nurses indicated that there were potential uses for virtual reality in their occupations, they did not interact with these technologies themselves.
Role in NNA
Participants were asked if they saw their current roles apply to NNA. Many of the nurses were unfamiliar with NNA and did not seem themselves exercising these roles in relation to this area (n = 7 out of 12). Those who identified as having roles in relation to NNA were those in leadership positions (n = 5 out of 12) where it would be necessary to take on a greater role and voice in regard to NNA impacts in their occupation. However, all participants indicated that in the future if NNA become more involved in their occupation, they would adapt and develop a more active role in relation to NNA.
ELSI considerations
Participants raised ELSI considerations involving NNA as it pertained to their occupation. Participants extended concerns towards job security (n = 5), playing god (n = 2), privacy (n = 8), replacing human interaction (n = 8), clinical side effects (n = 4), and whether the technology itself will benefit or harm the patient (n = 12).
Advocacy and active citizenship
All participants acknowledged that they would be advocates for their patients and clients if there were affected by NNA. Outside of the occupation, most nurses (n = 11 out of 12) did not see any role that NNA could take so they were less passionate or active in relation to NNA affecting greater society. In terms of NNA conversations, participants did not feel confident in leading discussions surrounding NNA, but they understood that they had a relevant voice and would make it heard if needed. All participants indicated that they needed more knowledge on the topic and would feel more comfortable allowing experts and researchers in NNA to make decisions surrounding the development and impacts of NNA.
Lifelong learning
All participants indicated that more education was necessary to form a solid opinion on the impacts of NNA on their occupations.
However, participants (n = 10 out of 12) also indicated that it would be difficult to get nurses to engage in professional development opportunities for concepts and ideas that were not currently relevant or interesting especially when the topics that they were interested in were not available or accessible.
Discussion
Nurses retain multiple roles in their professions that allow them to engage in a number of opportunities. The nurses in our study reflect that as a multifaceted and diverse practice, the nursing profession can provide but also hinder opportunity for the nurse’s roles. On one hand there is an expectation that nurses retain critical roles and have an untapped potential that is unrecognized by other professionals and higher ups that should be acknowledged more. On the other hand, nurses are expected to maintain a multifaceted role that contributes to increased role ambiguity, burnout, and job dissatisfaction. It was found that the nursing profession has an untapped potential to critically engage with NNA, neuroethics, and neurogovernance discussions, however their work environments and roles posed barriers to their active participation in policy, lifelong learning and NNA, neuroethics, and neurogovernance discussions. Our findings are discussed through the role expectations of nurses, their roles as active citizens, and lifelong learning opportunities.
Role Expectations of Nurses
Role theory is based on the idea that individuals retain certain roles that are expected of them by society, and these expectations shape the roles that they expect from themselves (Biddle, 1986). Nursing role expectations have been noted to create role conflict, role ambiguity, and influence overall job satisfaction and burnout (Cunningham & Slevin, 2005; Tunc & Kutanis, 2009; White & Kudless, 2008).
Findings from this study indicate that a disjoint exists between the expectations that society and the profession holds for nurses and the expectations that they hold for themselves. On one end, participants felt that nurses are not considered to be a meaningful voice and are not often sought to be involved in various conversations and discussions. Through our conversations with nurses, there was recognition that they had the capacity to do more in a given role and to fill more roles, but the environment and positions constrained them from reaching their potential. Köppen et al. (2018) revealed that although nurses were highly motivated to pursue new roles, there was a mismatch between motivation and the availability of opportunities, and in addition to this, workforce shortages were noted to be a large barrier for nurses, as nurses take on core nursing tasks when shortages are presents. As Köppen et al. (2018) reveals, there is a need to retain sufficient staff levels to offset workplace load when introducing new roles. It has been noted in the academic literature that nurses are often not considered to be a meaningful voice and are not often sought to be involved in conversations and discussions surrounding leadership and policy (Köppen et al., 2018), as well as neuroethics and neurogovernance discussions (Deloria & Wolbring, 2019).
Our participants expressed similar frustration at the lack of recognition be higher powers, and their exclusion from boards and committees. Participants indicated that at times, they felt that nursing was considered to be an assistant role in comparison to other professions.
On the other end, nurses are expected to exercise a variety of roles in practice, keep ELSI considerations paramount and retain passion and drive for their occupation. However, through our conversations with nurses it became evident, that although these concepts are ideal, they get lost in translation at the frontline. The participants in this study placed a large emphasis on the impact of lifelong learning and professional development in their occupation, and their potential to meaningfully involve themselves in discussions at the political and governance levels, although this was not often acted upon. From the interviews with participants, it is seen that nursing as a profession encompasses many responsibilities and roles and nurses struggle to keep up with a constantly changing environment and meet the responsibilities that they should fulfill in the moment. By nature as a nurse, you are a leader, you are a stakeholder, however it is difficult to develop and home in on these roles in an occupation that leaves little room for change or development (Brown et al., 2000; Cunningham & Slevin, 2005).One study by White and Kudless (2008) expressed that the leaders of interdisciplinary teams were non-nurses, and participants were frustrated because, “. . .while nurses said they believed they were recognized for their overall contributions, they thought they were not recognized for their full scope of preparation and skills, mainly because these were not understood by others. ‘A nurse is a nurse is a nurse’ was echoed by many focus group participants”. This same line was reiterated by participants in our study when expressing their frustrations towards how they were acknowledged in their occupation.
Given the many problems linked to role expectations of nurses a lot of work has to be done to entice and empower nurses to partake in a meaningful way in neuroethics and neurogovernance discussions. For example, enabling frontline nurses to take part in neuroethic and neurogovernance discussions has to involve deconstructing a multilayer of factors such as burnout and role ambiguity (Mudallal et al., 2017; Tunc & Kutanis, 2009; Wang et al., 2015; Yao et al., 2018).
Nursing Advocacy and Active Citizenship: Political Involvement Inside and Outside of the Profession
Nurses can carry their skills used to advocate in their occupations, outside of their occupation towards the development of active citizenship and political involvement. All of the nurses in our study expressed. that they were advocates in their field for their patients, however less than half (5 out of 12) of the participants expressed that they carried this advocacy outside of their occupation as active citizens. Through increased participation in civil life, citizens are able to advocate and push forward their rights to further foster good governance and policy (Clarke & Missingham, 2009; Hoskins et al., 2006).
However, there are various barriers. A study by Vandenhouten et al. (2011) analyzed the level of political participation among Midwest RNs. The majority of respondents participated in smaller activites, that included voting, political discussions, and contacting their elected officials, however, they also indicated that barriers such as time, and money hindered thier involvement. Another study noted, “Political involvement is further weakened by role ambiguity, role issues, and role incongruity. The role of the nurse must be balanced with the needs and complexity of getting things done politically. The role of the nurse politician adds further uncertainty and incongruity to the practice of the nursing profession” (Boswell et al., 2005).
The nurses in our study also expressed that their multi-faceted roles also included increased responsibilities that may hinder active participation and civic engagement. Our participants expressed frustration at the lack of value and recognition from higher powers, and their exclusion from boards and committees. The study by Vandenhouten et al. (2011), also revealed that less than 50% of respondents felt that they had an impact on local policy, and even less participants felt that they could impact government decisions. Other studies found that instances where frontline nurses were involved in policy making, were limited to implementation, rather than the concptualization and policy creation (Barzegar Safari et al., 2020; Bell et al., 2016; Kunaviktikul et al., 2010; Shariff & Potgieter, 2012). Florell (2021) describes the antecedents towards nursing activism, noting that empowerment for nurses should be in place to act, and nurses must recognize their potential, and abilities to confront existing power structures. However, existing hierarchies and narratives around nursing hinder the idea of taking part in political advocacy and governance. A similar sentiment has been proposed in relation to governance education for nurses. Sundean et al. (2019) acknowledged that nurses retain the capacity to engage with governance, however as they were not formally educated about governance concepts, and do not see governance leadership as part of the nursing identity, they do not pursue governance opportunities.
Interestingly nurses have been emphasized as a critical voice in policy development, reform, and leadership (Barzegar Safari et al., 2020; Patton et al., 2018; Turale & Kunaviktikul, 2019). Nurses have made strides in health policy development and reform, have contributed valuable research, and pioneered policy change (Ellenbecker et al., 2017; Hanks, 2013; Kelo et al., 2013).
Active Citizenship: Facilitating Neuroethic and Neurogovernance Involvement
There has been interest towards greater public involvement in neuroethics, and neurogovernance discussions (Garden & Winickoff, 2018; Racine, 2012; Racine et al., 2005). Nurses are relevant stakeholders as professionals and active citizens that should have a voice in neuroethics and neurogovernance discussions given their roles as leaders, educators, and liaisons as well as the emphasis of political involvement and advocacy in their occupations (Canadian Nurses Association, 2009; Huston, 2008). However, as one scoping review noted, there is no academic literature in this regard that links the political, advocacy, and policy roles of nurses to neuroethics and neurogovernance discussions and how to enable nurses as professionals and as active citizens in this regard (Deloria & Wolbring, 2019). Our study suggests that Deloria and Wolbring (2019) were right in their assumptions that nurses can fulfill much more and have the capacity to do so if given the opportunity. Most participants in this study hesitated towards involving themselves in neuroethics and neurogovernance discussions given their experiences, knowledge on the topic and involvement with these technologies.
Given the motivation and interest, the nurses in our study demonstrated that they are able to think about, engage with, and further involve themselves in discussions surrounding NNA. We suggest that more must be done to facilitate the participation of these professionals in NNA, neuroethics, and neurogovernance discussions. Experts in NNA, neuroethics and neurogovernance discourses should encourage greater involvement from a diverse spectrum of participants, including frontline and nursing leaders. Such participation would enrich the NNA discourses, and benefit patients, health professionals, and the public.
Lifelong Learning
Learning about NNA, neuroethics, and neurogovernance is a prerequisite to partake in discussions surrounding NNA. As well, lifelong learning is a mechanism used by the nursing profession to keep nurses up to date. The participants in this study placed a large emphasis on the impact of lifelong learning and professional development in their occupation, and their potential to meaningfully involve themselves in discussions at the political and governance levels, although this was not often acted upon.
At the same time, participants expressed stress at finding and completing lifelong learning opportunities that they needed for their current occupations citing restrictions that were in place in their personal lives, lack of emphasis from employers and a lack of accountability from staff, and that there was little room to explore other options for areas that they did not deem directly applicable to their work or were not of interest to them. Nurses expressed that they needed to be picky with what opportunities they chose because of the limitations that their employment offers them to expand on their knowledge. The barriers outlined by our participants fits with existing studies acknowledging the barrier to effective lifelong learning such as costs, travel, available content, occupational and personal responsibilities, motivation, and time away from work (Bahn, 2007; Cleary et al., 2011; Cooper, 2009; Gould et al., 2007; Griscti & Jacono, 2006; Kubsch et al., 2003; Nalle et al., 2010; Schweitzer & Krassa, 2010).
In a study by Bell et al. (2016), it was indicated that,
“Trainees from diverse healthcare professions (eg, nursing, social work, physiotherapy) are not well prepared to handle many of the ethical issues associated with psychiatric DBS because, among other reasons, they may be unprepared to engage in ethical reflection, they have a limited understanding of issues associated with scientific uncertainty, and they may lack an interdisciplinary understanding about ethical issues”.
When prompted, nurses engaged with ethical and critical thinking considerations with NNA even when these advancements were not applied to their occupations. With more developed lifelong learning initiatives and opportunities for knowledge development, nurses can be a critical and important role and provide meaningful input as professionals and active citizens in neuroethics and neurogovernance discussions. However, there was a lack of internal motivation among nurses when considering lifelong learning in general, and in relation to NNA, neurogovernance, and neuroethics. NNA was not an interest or did not seem to have a large impact in their current roles and thus nurses were hesitant to pursue these opportunities for further learning and involvement given all the problems they already faced.
Aside from the fact that continued education was mandatory for their occupation the participants indicated that their nursing environment did not foster excitement for learning, whether it was lack of enthusiasm shown by staff or the mode of delivery of nursing content through online platforms. This sentiment is outlined in other studies that emphasize that nurses wanted stimulating environments through mentoring and support as well as engaging and interesting delivery and content of learning (Danielson & Berntsson, 2007).
Given that academic literature does not engage with the involvement of nurses as professionals and active citizens in neuroethics and neurogovernance discussions it seems reasonable to assume that there is no mentorship available in the workplace of our participants and others to encourage contribution to NNA, neuroethics, and neurogovernance discourses.
Limitations
All participants in this study were collected through purposive sampling and account for a small section of the nursing profession. The views of these participants do not encompass the opinions and roles of the entire profession; however, the opinions of these nurses provide information rich insight into their voices and perspectives surrounding their roles, lifelong learning, and the engagement with NNA discourses. Follow-up studies are encouraged to gain a broader understanding on nursing involvement in NNA discussions.
Conclusion
Although studies have been published on lifelong learning and role identity for nurses, the considerations on how these interact with NNA, neuroethics, and neurogovernance fields were yet to be understood. The findings of this study indicate that nurses are ideal candidates for participation in NNA, neuroethics, and neurogovernance discussions however the complexities and problems systemic in their frontline work deters them from taking interest and integrating the appropriate knowledge and tools to effectively take part in these discussions inside and out of their occupations. It is indicated that potentially these frontline factors need to be rectified before fruitful consideration and involvement for nurses in NNA, neuroethics, and neurogovernance discussions can take place. Institutional change is warranted to allow for frontline nurses to be able to take an active part in lifelong learning opportunities and political advocacy. Changes should include continuous engagement with frontline nurses to create suitable lifelong learning delivery and opportunity that would best suit their needs. As well, fostering the potential of nurses should include providing increased exposure to political involvement at the educational and practice level, this would include creating seats at ethics boards and leadership teams to include nurses at the frontline, as well as actively seeking out and respecting the nursing voice in higher, policy matters. Further recognition and research on the disjoint between nurse self perceived role and their expected roles are needed to reconcile these differences and foster an environment for nurses to thrive and encompass all the roles as expected of them.
Footnotes
Author Note
This study was approved by the Conjoint Health Research Ethics Board (CHREB) at the University of Calgary on February 23, 2018 (REB17-0785).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Government of Canada, Canadian Institutes of Health Research, Institute of Neurosciences, Mental Health and Addiction ERN 155204 in cooperation with ERA-NET NEURON JTC 2017.