
Abstract
Globally, Philippine-educated nurses have made vital contributions to health care; however, there is a lack of in-depth knowledge about emigrating nurses’ initial motives to become nurses, their educational experience and their transition in the host country’s health care context. This research aimed to explore Philippine-educated nurses’ educational experience in their home country and their expectations of competence in Norway. The study utilized an explorative design consisting of qualitative interviews with 10 Filipino nurses. A hermeneutic approach was used to analyze and interpret the empirical material. The findings and interpretations underline that Philippine-educated nurses mainly are externally motivated; their educational program is very demanding, but their level of competence does not meet the competence expected in the host country. Although these nurses lack training in elderly care, the Philippine nursing curriculum emphasizes patient care and mastery of basic nursing skills, which are qualities that should be valued and utilized in host countries.
Introduction
The shortage of nurses is a worldwide challenge; thus, over the past several decades, countries in the global north have strategically recruited nurses from the global south to establish an adequate nursing workforce (Bautista et al., 2019; Drennan & Ross, 2019). Foreign-educated health professionals represent more than a quarter of the medical and nursing workforce of Australia, Canada, the United Kingdom, and the United States, with the majority originating from the Philippines (Kingma, 2018; Table, 2019). Since 2000, the globalization of female-dominated professions has primarily consisted of nurses seeking work in countries other than their homeland; 79% of the South-East Asian nurses that have immigrated to other countries around the world have been female (Statista, 2021).
Internationally, the nursing profession holds an important social mandate, and formal higher education is a qualification for this profession. The acquisition of scientific knowledge and practical skills occurs both in formal educational settings and in clinical practice (Mausethagen & Smeby, 2017), and various laws and regulations control the possibilities of working as a nurse in different countries. In Europe, all nurse education programs are required to follow the professional Qualifications Directive (EU Directive, 2005/2013), which makes it possible for nurses to be licensed and work across borders in Europe. These regulations are used to assess the competency of all nurses, educated outside of Europe, that want to work in a European Economic Area (EEA).
Over the last 20 years, nursing education has increased in popularity in the Philippines partly because of its social benefits and prestige and the opportunities it offers for professional mobility and individual freedom (Eder, 2016). In the Philippines, nursing education is influenced by the nursing curriculum in the United States, and English is the official language. In 2018, the nursing education requirements in the Philippines changed from mandating 10 years to 12 years of primary school education, and from needing a 4-year bachelor’s degree in nursing to needing a 3-year bachelor’s degree in that field (NOKUT, 2020). The Philippine nursing curriculum is based on the core values of care, love of God, and humanity. It consists of 29 detailed courses with a strong focus on scientific knowledge and basic nursing theory; for example, 23 U.S. nursing theorists are described in the curricula (Nursing Program Philippines, 2009).
Approximately 80,000 nurses graduate each year in the Philippines, and the number of nursing education institutions increased from 40 universities/colleges during the 1980s to 470 in 2006; since 2017, 80% of the country’s 1943 colleges and universities have been privately owned (Ortiga, 2018). This increase led to a commercial market for nursing education (Masselink & Lee, 2013; Ortiga, 2014). According to a qualitative study that included 58 faculty and administrators, in the Philippines, nursing education is based on the Western world’s need for nurses, and the instructors reported that the students often received training in using equipment that is not used in the Philippines (Ortiga, 2014). Based on these qualitative findings, Ortiga (2014) finds that when the content of the education is not in accordance with the current health care context, the status of autonomy and professional values in nursing education is negatively affected when it is partly based on exportation of nurses.
Annually, 19,000 Filipino nurses leave their home country to work overseas (Danny, 2019). Unfortunately, nurse emigration can lead to health policy challenges as the country is drained of its nurse resources (Masselink & Lee, 2010; Ortiga, 2014). However, in countries such as the Philippines, the economy relies on money being sent home by workers that have immigrated to other countries (i.e., remittance), and 10% of the Philippine gross domestic product (GDP), more than 3 billion Euros, are transferred through remittance (Masselink & Lee, 2013; United Nations Association of Norway, 2016). Other factors that motivate Filipino nurses to immigrate are difficulties in finding paid work after graduating from nursing school, low salaries, increasing workloads, understaffing, lack of professional and personal opportunities, and lack of organizational support (Falguera et al., 2020; Ortiga, 2014). Foreign-trained nurses are considered to be a valuable workforce in the host countries (Drennan & Ross, 2019); however, foreign-born nurses frequently report difficulties with discrimination, underestimation of competence, credentialing and different views concerning clinical practice as well as other cultural challenges (Nortvedt et al., 2020; Pung & Goh, 2017). Prior educational and clinical experiences may influence how migrant nurses cope with these challenges in the health care setting (Pung & Goh, 2017). The associated stress has been reported to negatively affect the nurses’ mental health and create emotional distress; subsequently, it has a negative impact on patient safety (Chun Tie et al., 2019; Dahl et al., 2017; Eriksson et al., 2018; Moyce et al., 2016). Health care managers and recruiters are in a unique position to establish support and follow-up for migrant nurses to ease their transition to the host country and their adaption into a new working environment. However, health care managers are often unfamiliar with the challenges experienced by foreign-trained nurses and they lack knowledge about their prior educational context. This lack of knowledge and awareness may affect the nurses, as their ability to cooperate with their host country peers, ask for assistance, advocate for their patients and speak up for themselves when necessary, might be deficient (Xu et al., 2008).
Thus, this study aimed to explore the educational experiences of Filipino nurses in the Philippines and expectations of their competence in Norway. Specifically, the objectives were to explore the nurses’ (a) motivation for becoming a nurse, (b) educational experiences during their nursing program in the home country, and (c) transition experiences into the host country’s health care context.
Method
This study utilized an explorative design consisting of qualitative interviews with 10 Filipino nurses (Table 1). The nurses were recruited through a university database.
Characteristics of the Participants.

Participants
Thirty participants who have been or were affiliated with the university as a student or who attended a course were purposively selected and were invited to participate in the study via email sent to them by the student administrative staff. Ten nurses accepted the invitation to participate in the study, seven women and three men, with an average age of 30 years (range: 27–38 years). All the participants had obtained permanent residency in Norway, had lived there between three and eight years, and had graduated from a Philippine nursing program between 2007 and 2012. Three nurses had received their authorization as a registered nurse (RN) at the time of the interview.
Data Collection
The interviews were conducted individually during autumn 2017 by three researchers: four interviews by the first author and the last author and two interviews by the third author.
A semi-structured interview guide was developed based on themes from prior research about International Educated Nurses (IENs; Dywili et al., 2013; Moyce et al., 2016; Salami et al., 2014) and on two of the researchers’ experiences of teaching Filipino nurses at a Norwegian university program for supplementary education for nurses educated outside the European Union/European Economic Community (EU/EEC).
The interview prompts included Can you tell me why you chose to study nursing? How did you experience studying nursing in the Philippines? Please tell me about the credential assessment process in Norway.
The interviews lasted between 35 and 60 min and took place in a setting chosen by the participants, mainly on the university’s premises. The interviews were digitally recorded and transcribed by a professional agency.
Data Analysis
Analysis and interpretation of the empirical material were performed using a hermeneutic approach to the text (Ricoeur, 1976). All the co-authors contributed to the discussion of the analysis and the findings. The research goal was to interpret the informants’ motivation for becoming a nurse, their experiences during their nursing study program in the Philippines and their transition experiences into the health care context in Norway. Hermeneutics is a methodological approach that is useful for interpreting interview texts. Knowledge is created through the exchange of ideas: meaning emerges through a dialogue or hermeneutic conversation between the text and the inquirer (Koch, 1999). The analysis steps were conducted based on Wiklund et al. (2002), where the four researchers read the interviews several times to achieve what Ricoeur (1976) referred to as “a naïve grasping of the meaning” (p. 74), obtaining an overall impression. We then prepared a structural analysis that involved categorizing and articulating the themes that emerged, and we conducted the main analysis. The last step was to apply a common holistic understanding of the text by reading the text again, in its individual parts and as a whole, by considering our prior understanding regarding what we knew about Filipino nurses and nurse education in the Philippines.
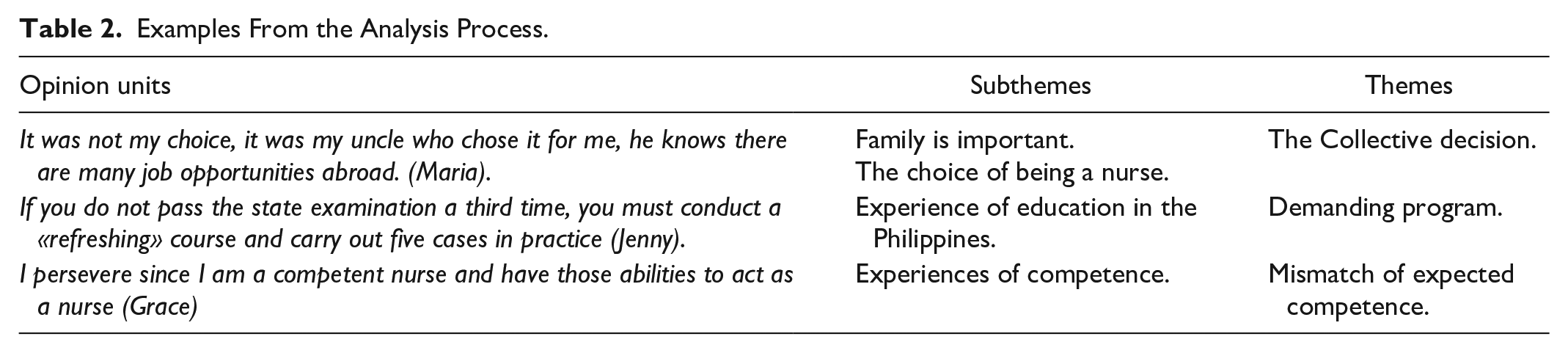
The meaningful entities were marked in the transcription and later inserted into a table. The texts were extracted from the meaningful condensed entities. The condensed meaning units were then labeled with subthemes (e.g., education is demanding, the importance of the economy and family relationships are crucial). The subthemes represented the essence of the condensed meaningful entities. The extraction continued, and the tags were divided into themes. The themes constitute the manifest content of the text (Table 2). A researcher’s journal was kept throughout the study to track the developing thoughts and themes. In the end, three themes were identified: (a) Becoming a nurse: a collective decision; (b) Perception of their educational journey: a demanding program; and (c) Mismatch of expected competence. In this article, the quotations from the interviews are italicized and cited using the pseudonyms of each participant.
Examples From the Analysis Process.
Ethical Considerations
The study was registered with and confirmed by the Norwegian Social Science Data Services (NSD), (project no. 53131), and confidentiality was maintained at every stage of the research process. All the interview transcripts were anonymized and treated in the strictest confidence. The researchers continuously reflected on and discussed how language, culture and the asymmetric power relationship between the participants and researchers might influence the results (Brinkmann & Kvale, 2015). This was particularly important as the researchers and the students have been affiliated with the university where the study was conducted. As recommended (Brinkmann & Kvale, 2015), open-ended questions were used so as to avoid leading the conversation in one direction during the interviews.
The participants were informed about the aim of the study and the possibility to withdraw at any time. They were told that participating in the project would not negatively or positively affect their credential assessment process or immigration status.
Findings
Three themes emerged from the analysis: (a) Becoming a nurse: a collective decision; (b) Perception of their educational journey: a demanding program; and (c) Mismatch of expected competence.
Becoming a Nurse in the Philippines: A collective Decision
Initially, the participants expressed the desire to help others as a motivation to become nurses. One participant, Grace, said, “I am happy about becoming a nurse especially when the patients thank you for doing a good job.” However, the most valuable motivation was to have a profession that would enable them to help their family financially. Furthermore, many of the participants chose private and religious-oriented colleges. For example, Angel stated, “We are Adventists and went to Northern Luzon Adventists College and lived in a boarding school. There is no free education in the Philippines; the public is cheaper, but my parents would rather have me in a private college.”
The participants’ decisions were mainly based on their family’s financial needs as well as their desire for a better future by traveling abroad and sending money home. Several participants have health care personnel in their immediate family. About her decision to become a nurse, Maria said, “The choice was not mine—my uncle chose for me, and he knows that there are many job possibilities for nurses abroad.” Grace supported her family’s decision, too, stating, “My relatives are in the health care service, some doctors, pharmacists, dentists. At first, I wanted to become a civil engineer but then it became nursing for my sister and myself.” Her comment indicates that she would like to have become something other than a nurse if she could choose freely.
Similarly, several of the participants had initially chosen a different course of study, such as nutritional physiology or law, but accepted their family’s decision to become a nurse to be able to emigrate and secure a job. The reason for the family’s choice to pursue a career in nursing is often determined by the fact that it is a profession in which other family members, such as a son, daughter, brother, niece or nephew, also work, and it provides the opportunity to travel abroad and send money home. According to one of the participants, It was my sister who took the nursing education first and said that maybe I could start too; so, I said OK, hee- hee, but it was not my first choice. But I thought maybe it’s easier to travel from the Philippines and get a job and because our aunt is in Norway. I started sending money home last year since my mom got cancer and there is no free healthcare. Chemotherapy costs a lot of money every three weeks. My brother and I share the costs.
Several of the nurses explained that media, family, and friends recommended becoming a nurse so they could have the opportunity to work abroad. However, the decision can sometimes be haphazard. As Rose noted, It is just a coincidence that I decided on Norway. A friend and I wanted to travel out of the country and one day we saw in a newspaper that Norway will need many nurses in the next 30–35 years.
Rose’s comment shows the randomness of the country of destination, but several of the participants stated that they had wanted to travel to an English-speaking country.
Perception of Their Educational Journey: A Demanding Program
The participants all agreed that Philippine nursing education is very demanding; they described an educational environment with strict discipline. They reported how difficult it is to gain admittance to a university/college; theory and clinical training are mandatory and very challenging, and they must obey the teacher’s demands and follow their wishes. For example, Mark said, “It is a lot to read, and the professor expects you to read before you get to school . . . kind of spoon-feeding, you know.” Rose said, “If you are ill one day in clinic, you have to replace this and work two or three shifts and pay the clinical instructor to get clinical training approved.” When asked about well-being at school, several of the nurses reported that they felt better after a while, but that the strict requirements could make them feel uncomfortable. Rose said, “It is too difficult because the teacher may suddenly come unexpectedly with a quiz to test you.” This highlights the strict discipline and teacher-driven practice associated with nursing education in the Philippines.
Many of the participants mentioned the clinical instructor and noted that a teacher from the school who is responsible for their instruction is always present at the clinical site. The participants all made it clear that it is hard work and impossible to have a paying job in addition to completing their studies. Furthermore, they described the different methods used in their education, such as lectures, role-playing, writing care plans, case solutions, and many presentations of tasks and cases. The relationship between being in school and the clinic appears to be different throughout the 4 years of their nursing program. The participants mentioned municipal health care training together with the amount of theory they need to learn during the first 2 years. Justine said, Professional training takes place Monday to Friday 7–15, but sometimes we may also attend school one day a week at the same time as we attend the surgery ward for six months. When we are placed in primary healthcare, it is all very different because we attend many clinical places; we may, for example, move to two or three different municipalities.
Several of the nurses noted that their education program placed great emphasis on natural science knowledge. As Melvin said, “We are very concerned about diseases and so on, we were almost like doctors.” They all described the final and demanding state exam, and it appears that the examination results are publicized with ranking as well as the number of people that did not pass. Jenny said, “780.000 candidates were taking the state exam in 2011, and 70% did not pass. I was ranked no. 19.” Competition within the nursing education program is striking. Jasper noted, “We had a case competition about leptospirosis, and in the entire university we won.” Justine said, “We memorised and worked in the middle of the night and got a medal, which we gave to mom and dad who were very proud.” Several participants also described how difficult it is to be accepted into the school and that many students drop out during the program. Although Philippine nursing programs facilitate high academic achievements, most of the participants experienced unemployment in the Philippines and many worked without pay after graduation. However, they appreciated their educational background because it provided them with more opportunities to emigrate and find work abroad.
Mismatch of Expected Competence
Despite feeling very proud of their acquired nursing competence, most of the participants expressed frustration over the nurse credential assessment process in Norway, and they felt devalued by the health authorities. Grace said, “I persevere since I am a competent nurse and have those abilities to act as a nurse.” Others expressed frustration over not being qualified as a nurse in Norway, and they stated that the host country belittled their hard work, knowledge and nursing competence. Justine noted, “It is a lot to read at school in the Philippines, not as in Norway—every day is mandatory” and “it is totally different in the Philippines where we work seven hours shift, six months in surgery with both clinical and theoretical studies.” Justine’s comments demonstrate that she perceives the Philippine program as being more demanding than the Norwegian nursing program.
Furthermore, the participants found it to be very frustrating to be a nurse and work as an auxiliary nurse. Grace said, “It is frustrating to pretend I do not know things and it affects my self-confidence.” Pretending to have a lower nursing competence than you actually possess is problematic. Some of the nurses did not understand why they were required to complete complementary courses; however, others tried to stay positive. Angel said, “I am very interested in supplementary study if I fit in.”
Some of the nurses did not obtain relevant work in the health service. One of the participants said, I applied for many different jobs when I came to Norway, but everything was just no, and then I started at a bakery, and then I lost it and then worked in cleaning service—yes it was a bit tough because it is not my profession.
However, most of the participants worked in elderly care as an auxiliary nurse after different kinds of jobs, and they did not understand why they needed supervised practice to obtain authorization as a nurse. One of the participants said, “I do not think I have anything to learn in nursing homes in clinical studies, I have worked and have a lot of experiences in elderly care.” These findings indicate that the difference between paid work and supervised practice in elderly care in Norway is not clear to the participants. Most of the participants noted that there is a lack of clear communication about why they need additional theoretical courses and/or supervised clinical practice in selected areas to be qualified as an RN in the host country.
Discussion
Our findings suggest that the immigrant and transition experiences of the Philippine-educated nurses are influenced by their academic journey prior to emigration and the mismatch between their competence and the expected competence in the host country. They described a demanding educational program characterized by hard work and competition, which made them stronger and more independent, and helped them overcome the challenges they encountered after they immigrated. The Filipino nurses perceive their education and nursing competence as being almost equal to nurses in the host country, and they refer to the characteristics of their bachelor’s degree. It is not clear to them why they need additional theoretical courses and/or supervised clinical practice in selected areas to become an RN, and there is a mismatch between the competence they experience and the requirements that are set in the credentialing process.
Consistent with the literature, the family network has a strong effect on the intention to emigrate and external factors, such as financial incentives, were the most important drivers of becoming a nurse and of immigrating (Bautista et al., 2019; Dywili et al., 2013; Hofstede et al., 2011). The participants’ stories highlight the obligation they feel toward their families at home in the Philippines. They are expected to provide for them. Thus, the decision to become a nurse is mostly financial and externally motivated. It enables them to find work abroad, when they experience unemployment in the Philippines, and send money home even if doing so entails personal costs (Falguera et al., 2020; Masselink & Lee, 2010; Ortiga, 2014). These results are in accordance with the findings reported by Ramos and Habig (2019), were students scored higher on external motivation than internal motivation. Nurse migration is becoming a dominant part of the pattern of international migration (Moyce et al., 2016) and negative consequences are frequently described (e.g., push-and-pull factors). However, recent studies have emphasized the positive effects of highly skilled emigration and they have shown that the option to emigrate incentivizes people to invest in their education (Walerych, 2020), as was noted by the participants in our study. In relation to these findings, it is not the case that everyone who invests in education emigrates, which implies that the possibility of emigration has a positive impact on nurse professionalization in the home country.
This study extends the current understanding of the supports that are essential during different phases of the migration process. Our findings suggest that it is important to be aware of Filipino nurses’ educational competence when they enter the host country’s health care system to ensure that they have the competence they need to obtain nursing authorization. Our findings and interpretation indicate that nurses immigrating from the Philippines perceive their education to be almost equal to that of Norwegian nurses; they are proud of their education and they describe a program characterized by a focus on academic achievements and success—which are virtues that should be recognized and valued (Factor & de Guzman, 2017). A review of the Philippine and Norwegian nursing curricula indicates that values, such as nursing holistic care, management, research, tuition, ethics and morals, personal development, quality development, communication and cooperation, are similar in both programs (Nursing Program Norway, 2008; Nursing Program Philippines, 2009). Both programs emphasize a holistic view of nursing, which is consistent with the core values of the International Council of Nursing (ICN; ICN Code of Ethics, 2012). This substantiates the findings reported in other studies that claim that core values in nursing are somewhat similar worldwide (Leininger & McFarland, 2006). However, the Norwegian nursing curricula have a more individualistic focus, which emphasizes autonomy and self-determination in contrast to the more collectivistic and religious perspective of the Philippine curricula (Hofstede et al., 2011; Nesje et al., 2017; Ortiga, 2014). The discipline and respect for authorities in college that the participants described can be linked to a more collectivist way of thinking, and it can be perceived to be the opposite of an individualistic perspective (Hofstede et al., 2011). Furthermore, many of the participants have studied at religious and private colleges, which is also common in Norway, but it is not stipulated in the common Norwegian program plan as it is in the Philippines.
The level of details in the Philippine nursing curriculum is advantageous for host countries because authorities can regulate and compare it with their curricula; however, the equality assessment can be time-consuming and complicated. Moreover, the universities and colleges in the Philippines can develop and implement their own version of the curriculum, which further complicates the review process (Nesje et al., 2017; Ortiga, 2014). The Philippine nursing curriculum (Nursing Program the Philippines, 2009) primarily includes detailed descriptions of medical knowledge and nursing theory, which emphasize caring for people suffering from acute illnesses but lacks a focus on elderly care and comorbidity. According to Ortiga (2014), much of the theoretical foundation of Philippine nursing education was inspired by the United States, and this is comparable to the situation in Europe in the 1970s and 1980s. For example, in Norway, nursing education has moved from a medical natural science focus in the 1980s to a more professionalized and academic emphasis toward the humanities and sociocultural attention at the college and university level (Mausethagen & Smeby, 2017). In contrast, in the Philippines, nursing education still emphasizes medical traditions, and as one of the participants argued, “We were almost like doctors.” However, medical and natural science knowledge is important for all nurses, and the Filipino nurses contribute with important knowledge that may have been lost in the pursuit of academic nursing in Europe (Kyte et al., 2009). Biomedical knowledge is one part of this model, and one challenge is how to emphasize the different parts of the whole. This will probably depend on the context in which nursing is practiced.
Our findings and interpretations indicate that dedicating resources to underpin and ease the transition process for immigrant nurses, such as language support and academic counseling, can generate a significant return on investment. The requirements and procedures related to the RN-authorization process need to be clearly communicated.
Evidently, Philippine nursing education lacks structured clinical training in elderly care, which is mandatory in most European nursing programs, and this is the most frequent reason why Filipino nurses are not authorized as RNs in Norway (Klaus, 2018). In the Philippines, the family has a collective responsibility for the elderly, and geriatric care and nursing homes are rare (Alvarez et al., 2017). Therefore, clinical training at these institutions is not part of the Philippine nursing education curriculum, and it may explain the contrast between the nurses’ training environments and the nursing context encountered in host countries in the Western world. A more structured transition program that focuses on elderly care would be beneficial, particularly for the Filipino nurses that work as auxiliary nurses while waiting for RN authorization (Fagertun & Tingvold, 2018; Nortvedt et al., 2020). The majority are recruited to work in community health services, and institutions, such as nursing homes or home care services, often rely on immigrant nurses (Klaus, 2018). Moreover, a structured transition to clinical practice may reduce associated stress, ease the transition process and reduce staff turnover (Garcia, 2018).
Strengths and Limitations
The researchers aimed to describe the findings of the study as precisely as possible and they have followed all the steps in a pre-defined analysis process. To strengthen the study’s reliability, all the researchers participated in the analysis by creating an analytical space with more room for nuances with frequent discussions and continuous dialogue to establish relationships between the differences and similarities of the empirical material that was obtained. Similar findings from other studies with IENs also strengthen the reliability of our research.
A limitation of the current study is the few number of participants (10) and consequently the gender perspective is therefore difficult to discuss. However, the researchers experienced data saturation related to the aim of the study mainly through several meetings and discussions during the different analytical steps. Furthermore, the digitally recorded interviews were not transcribed by the researchers; thus, nonverbal information may have been lost.
Conclusion
Our study underlines the importance of viewing foreign-educated nurses in a broader perspective. The Philippine-educated nurses have a wide-ranging theoretical and clinical background. Although they lack training in elderly care, the Philippine nursing curriculum emphasizes patient care and mastery of basic nursing skills, which are qualities that should be valued and utilized by the health care team in host countries. The study’s findings and interpretations emphasize the need to highlight differences in the nursing education programs in the Philippines and Norway so that the experience of competency mismatch might not be challenging. Conclusively, the need for additional theoretical courses and/or supervised clinical practice needs to be more clearly communicated and investigated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.