
Abstract
Although preconception care is a key element of motherhood health care services, the package is ignored in developing countries including Ethiopia and has not been generally adopted and applied since its aim and purposes are not broadly unstated and incorporated. Therefore, the objective of the current study was to determine the level of preconception care use and its determinants among women in Debre Tabor Town Northwest Ethiopia. From November 1 to 30, 2020, a Community-based cross-sectional study was undertaken in Debre Tabor Town. Overall, 79 (15.8%) with 95% CI [12.6, 19] of women had a good level of practice on preconception care utilization. Age (35–49; AOR = 5.12, 95% CI [2.14, 9.98]), ante natal care (AOR = 8.78, 95% CI [2.66, 28.97]), history of adverse birth outcome (AOR = 4.89, 95% CI [3.09, 17.00]), presence of chronic disease (AOR = 7.51, 95% CI [2.33, 12.13]), and knowledge on preconception care (AOR = 3.55, 95% CI [1.57, 8.02]) were significantly associated with utilization of preconception care. Hence, the government and respective stakeholders must give establish on preconception care strategies and plan that covers all aspects of preconception care. Incorporation of the service with other maternal and child health service will be crucial when developing actual employment policies to scale up acceptance of preconception care.
Introduction
Preconception care (PCC)is a set of the delivery of biomedical, behavioral, and social health interventions to women and couples prior to pregnancy through health promotion, disease prevention, and treating existing illnesses which goals at refining the wellbeing, and minimizing behavioral and environmental hazards that leads to deprived maternal and newborn health consequences (World Health Organization [WHO], 2013 a,b,c).
PCC is crucial for improving pregnancy and delivery outcomes, as well as the health of women, newborns, children, and their families in the future (Dean, Lassi, et al., 2014; Mason et al., 2014). PCC must be seen as an earlier chance, not only for birth control or to decrease maternal and newborn mortality, but also to advance long-term consequences for children, adolescent girls, and women (Dean, Rudan, et al., 2013).
By 2030, the third Sustainable Development Goal (SDG) intends to reduce global maternal mortality to below 70 per 100,000 live births and neonatal mortality to a minimum of 12 per 1,000 live births (WHO, 2016).
Despite the fact that governments, policymakers, and other stakeholders are provided with a priority agenda for mother and child health care services, maternal, and neonatal morbidity and mortality are not at the desired levels (Olayinka et al., 2014).
Preconception healthcare, particularly in developing nations, has not become part of a regular practice worldwide. However, there is a higher rate of maternal, newborn, and child death in this area, with 77% of maternal, newborn, child, and stillbirth deaths and stillbirths preventable by establishing a community, health center, and hospital platform to deliver vital packages (Black et al., 2016).
According to WHO latest data globally, 4 out of 10 women state that their pregnancies were unintended. Due to this, 40% of pregnancies do not receive the required healthcare services prior to pregnancy (Chola et al., 2015). To improve the pregnancy outcome, the Center for Disease Control (CDC) endorses that risk identification and advising for all women is an important component of primary health care (Johnson et al., 2006).
Even though PCC is a vital element of MCH service, it is not well known and practiced in low-income countries including Ethiopia. The main reason is that its aim and goal are not widely understood and embraced (Lu & Geffen, 2007, WHO, 2013 a,b,c).
Since PCC is a pivotal component of health care for women of childbearing age, increasing access and quality of this service can be positively affect the health of the women, newborn, family, and as large community by reducing this risk of adverse health outcomes of the women and newborn. It also improves the health status and enhancing wellbeing of the individual (Johnson et al., 2006; New York State Department of Health AIDS Institute, 2010).
Despite its significance in improving maternal health and promoting to safe outcomes of pregnancy, in Ethiopia it is not well known and well-practiced yet. Identifying factors that hider utilization of PCC is crucial to develop effective implementing strategies that improve its utilization in the years to come. This study was therefore aimed at investigating the use of PCC and its determinants among women in Debre Tabor Town, Northwest Ethiopia.
Methods
Study Design, Period, and Setting
This was a community based cross-sectional study carried out in Debre Tabor Town from November 1 to 30, 2020. Debre Tabor is situated 665 km northwest of Ethiopia’s capital, Addis Ababa and 103 km southwest of Bahir Dar. It is the headquarters of south Gondar zone and divided in to six kebeles. According to 2019 data from the town health department, there were a total of 19,936 households (HH) and 85,727 peoples of which 49.6% (42,521) and 50.4% (43,206) were men and women, respectively. Of the total 43,206 women, 20.96% (17,968) are found in childbearing age group (i.e., 15–49 years; Ayele, Mihretie, et al., 2021).
Population
The target population was all childbearing age women residing in the town while the study population comprises women who were residing in the selected kebeles. Women with a history of pregnancy (current or past) and residing in selected kebeles at the time of the study were included, while seriously ill (bedridden) and live less than 6 months in the town were omitted form the study.
Sample Size Determination and Sampling Procedure
A total of 504 samples were selected by using Epi-Info version 7 statistical software with the following assumption: 18.2% of women had utilized PCC (Asresu et al., 2019), 95% Confidence interval, with a 5% margin of error, design effect of 2, and adding 10% of non-response rate.
A multistage random sampling technique was applied to select the calculated 504 women. Out of the six kebeles, four of them were chosen by chance using lottery methods and included in our study. A total of 13,225 households and 11,848 childbearing women were living in the selected four kebeles (Town Administration Health office of Debre Tabor [Debre Tabor], 2019).
The sampling unit was the household, and samples were distributed proportionally to each kebeles depending on the total number of households. The kebeles registration book provided the number of women and their home numbers. The study households were then drawn from each of the specified kebeles using a simple random selection procedure based on a table of random numbers starting at a kebele one from a random starting point.
A random lottery method has been used to select the first household in each selected kebeles. In each home one woman was interviewed. In case more than one woman were eligible in the same household, only one was enrolled using lottery method and if no appropriate woman was obtained in the identified household, the subsequent eligible household located in the clockwise direction was contacted and involved until the required samples were met (Ayele, Beyene, et al., 2021).
Data Collection Instrument and Technique
An interviewer-administered, structured, and pre-tested questionnaire was used to collect data.
Two different language experts who speak both English and Amharic perfectly developed the questionnaire in English first, then translated it to the local language, Amharic, for simplicity, and finally back to English for consistency. The questionnaire had five components including socio-demographic characteristics, obstetrics and reproductive characteristics, medical and health facility characteristics, knowledge related characteristics, and utilization asking questions. Four diploma health professionals who have prior experience were participated in the data collection process and two BSc health professionals were supervised the process (Ayele, Beyene, et al., 2021).
Data Quality Control
The instrument was developed following a detailed review of relevant literature in order to maintain the data’s quality. The questionnaire was pre-tested on 5% of the sample size (25 women) at Worota Town, which is close to the study location. Modifications and adjustments to phrasing, logical ordering, and skip sequences were done promptly based on the pre-test. Before the actual data collection, data collectors and supervisors were briefed for 1 day on the purpose of the study, the contents of the instrument, confidentiality, and informed consent. The completeness and accuracy of the gathered information have been cross-checked, cleaned, and verified on a regular basis by supervisors and the lead investigator (Ayele, Beyene, et al., 2021).
Operational Definitions
Preconception care
Any counseling or treatment and lifestyle change interventions obtained by women about components of PCC before the occurrence of conception (Ayalew et al., 2017).
Component of preconception care
In the current study, the components of PCC includes (micronutrient supplementation (iron and folic acid), vaccination, screening and treatment of infectious disease (STI/HIV), screening and management of chronic disease, counseling on balanced diet, reproduction health planning and implementation, advice on cessation of excessive alcohol use, advice on cessation of cigarette smoking, counseling and advising of social and mental health concern, stop taking illegal drugs, and protection from environmental hazard exposures (WHO, 2013 a,b,c).
Preconception care utilization
The practice of PCC was evaluated based on correct response regarding components of preconception. Each correct and incorrect response was received a value of 1 and 0, respectively, and rated as good and poor practice based on the mean score.
Good practice
Women who achieved a score that was higher than or equal to the mean score.
Poor practice
Women who achieved less than the mean score.
Knowledge on preconception care
Women’s knowledge of PCC was determined based on correct response of PCC knowledge-related questions. Each correct and incorrect response was a score of 1 and 0 point. respectively. Using 50% as the cut of point women’s knowledge was divided into two (Kassa & Yohannes, 2018).
Good knowledge
Women who answered 50% and above on knowledge measuring questions.
Poor knowledge
Women who answered less than 50% on knowledge measuring questions.
Analysis and Interpretation
The collected was cleaned, coded, and entered using Epi-data software version 4.2, and analyzed by statistical package for social science (SPSS) version 23. Descriptive statistics was used to describe the study populations using frequency tables and percentages. We ran both bivariable and multivariable logistic regression analyses. Variables with a p-value of <.20 in binary logistic regression analysis were added into a multivariable logistic regression analysis model for additional investigation. Finally, a significant association was determined based on a .05 p-value and adjusted odds ratio (AOR) at a 95% confidence interval (CI; Ayele, Beyene, et al., 2021).
Ethical Considerations
Ethical approval was obtained from Debre Tabor University College of Health Sciences Ethics Review Committee. Also, a letter of cooperation was approved by the administrative office of the town. Informed consent was available from each respondent. To maintain privacy and to ensure confidentiality, all personal identifiers have been omitted.
Results
Socio-Demographic Characteristics
This research included a total of 500 women with a response rate of 99.2%. More than half of the participants 284 (56.8%) were in the 25 to 34 years age group with the mean age of 27.19 (SD ± 4.72) years. The majority of the respondents, 482 (96.4%) were Amhara by ethnicity and orthodox Christian followers, 453 (90.60%). More than one third of the respondents, 193 (38.6%) had attended college and above. About 394 (77.8%) of participants were married and 171 (34.2%) was a private business woman by occupation (Table 1).
Socio-Demographic Characteristics Study Participants in Debre Tabor Town, Northwest Ethiopia, November 1 to 30, 2020 (N = 500).

Oromo, Tigray, and Gurage.
Protestant and Catholic.
Widowed and divorced.
Reproductive and Obstetrics Characteristics of Participants
Of 500 women, 264 (52.8%) and 220 (44%) were multigravidas and multiparas, respectively. About 260 (52.0%) of the respondents had less than or equals to two children. About 317 (76.9%) of the participants had a history of ANC follow-up in their recent pregnancy. One-fourth of the participants (25.6%) had a history of at least one adverse birth outcomes. Abortion 55% and low birth weight 23% were among the frequently experienced adverse birth outcomes by the women (Table 2).
Obstetric and Reproductive Health Characteristics of Study Participants in Debre Tabor Town, Northwest Ethiopia, November 1 to 30, 2020 (N = 500).

Uterine rupture, gestational trophoblastic disease.
Medical and Health Facility Related Characteristics
Among the total participants, 86 (17.2%) of them had a chronic disease. Of those respondents who had a history of chronic disease, 26 (30.2%) and 24 (27.9%) of respondents mentioned that they had a chronic health problem of hypertension and renal problem, respectively. Regarding availability of a health facility, all the participants (100%) approve that health facility is available in the area (hospital/health center). On the subject of where they access PCC, 59 (60.2%) gained the PCC service from the hospital. The majority of 470 (94.0%) and 453 (90.6%) of the respondents stated that adequate medication and laboratory service were easily accessible (Table 3).
Medical and Health Facility Related Characteristics of Study Participants Live in Debre Tabor Town, Northwest Ethiopia, Novemeber 1 to 30, 2020 (N = 500).
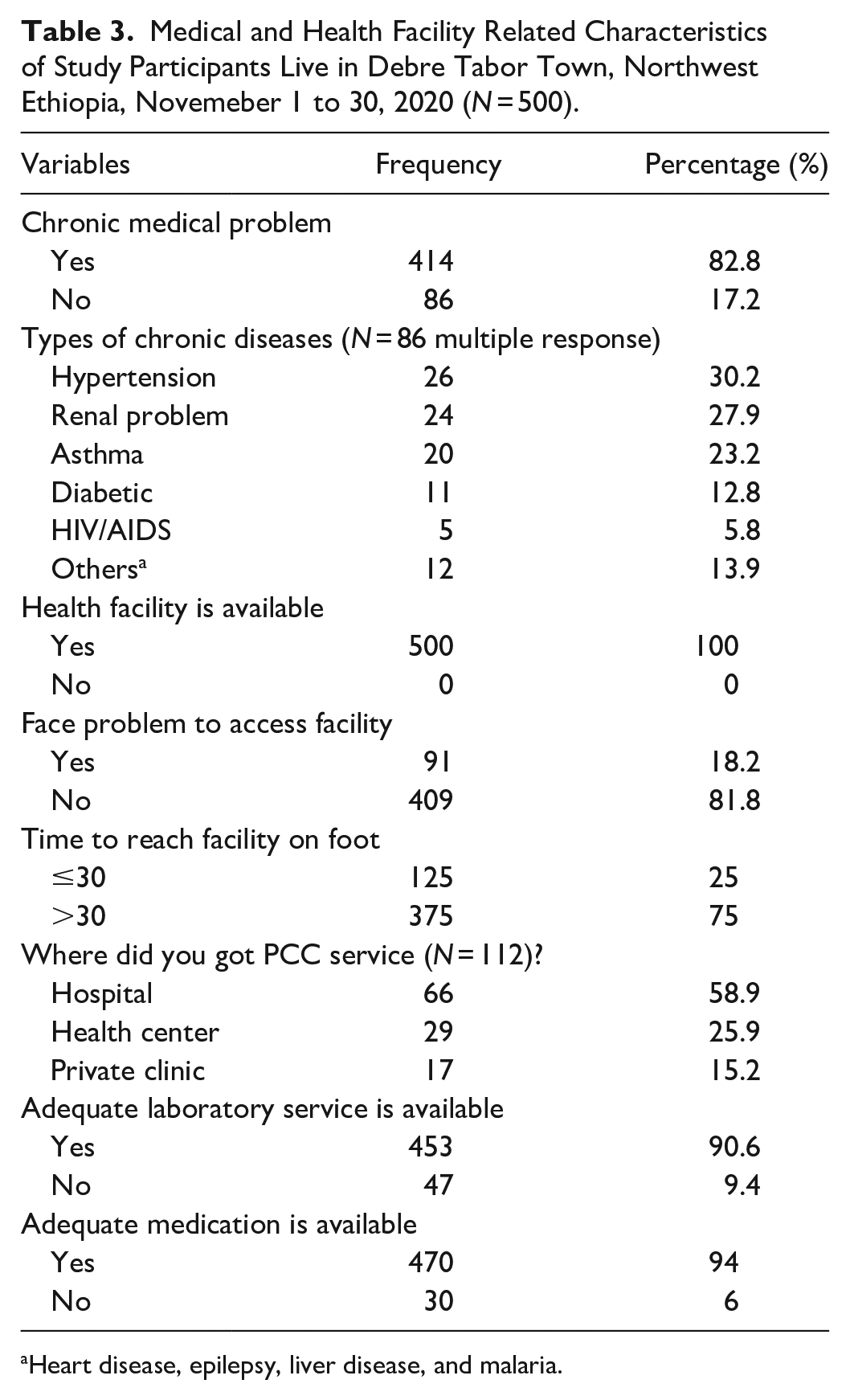
Heart disease, epilepsy, liver disease, and malaria.
Women’s Knowledge Toward PCC
Near to two-third of the participants, 345 (69%) had poor knowledge toward PCC, whereas 155 (31%) of the participants had a good level of knowledge about PCC.
Utilization of PCC
According to this study, 112 (22.4%), 102 (20.4%), 98 (19.6%), 92 (18.2%), and 85 (17%) of women were utilized at least one, two, three, four, and five components of PCC, respectively. Overall, 79 (15.8%) with 95% CI [12.6, 19] of the study participants had a good level of practice on preconception care utilization (Table 4).
WHO Preconception Care Component Utilization Of Study Participants Live in Debre Tabor Town, Northwest Ethiopia, Novemeber 1 to 30, 2020 (N = 112).

Factors Affecting Participants Utilization of PCC
Women’s age, educational status, occupation, ANC follow-up, history of adverse birth outcome, presence of chronic disease, and knowledge of PCC were statistically significant with PCC utilization in binary logistic regression analysis. Whereas women’s age, ANC follow-up, history of adverse birth outcome, presence of chronic disease, and knowledge of participants about PCC were remained statistically significant with utilization of PCC in multivariable logistic regression analysis.
According to the current study, those women who has advanced age (35–49) years old were five times (AOR = 5.12, 95% CI [2.14, 9.98]) higher the odds of utilizing PCC ae compared to their counterparts. Women who had attended ANC visits in recent pregnancies had nearly nine times (AOR = 8.78, 95% CI [2.66, 28.97]) higher odds to utilized PCC than their counterparts. When compared with those women who had no history of adverse birth outcomes, women who had a history of at least one adverse birth outcome were nearly five times (AOR = 4.89, 95% CI [3.09, 17]) more likely to utilize PCC. The result of this study also noticed that presence of chronic disease was another predictor of utilization of PCC. Women who had chronic disease were seven times (AOR = 7.51, 95% CI [2.33, 12.13]) more likely to utilize PCC before the occurrence of conception as compared to their counterparts. Lastly, respondents who had good knowledge about PCC were three times (AOR = 3.55, 95% CI [1.57, 8.02]) higher the odds of service utilization as compared to respondents who had poor knowledge about PCC (Table 5).
Bivariable and Multivariable Analysis of Factors Affecting Utilization of PCC of Women Live in Debre Tabor Town, Northwest Ethiopia, November 1 to 30, 2020 (N = 500).
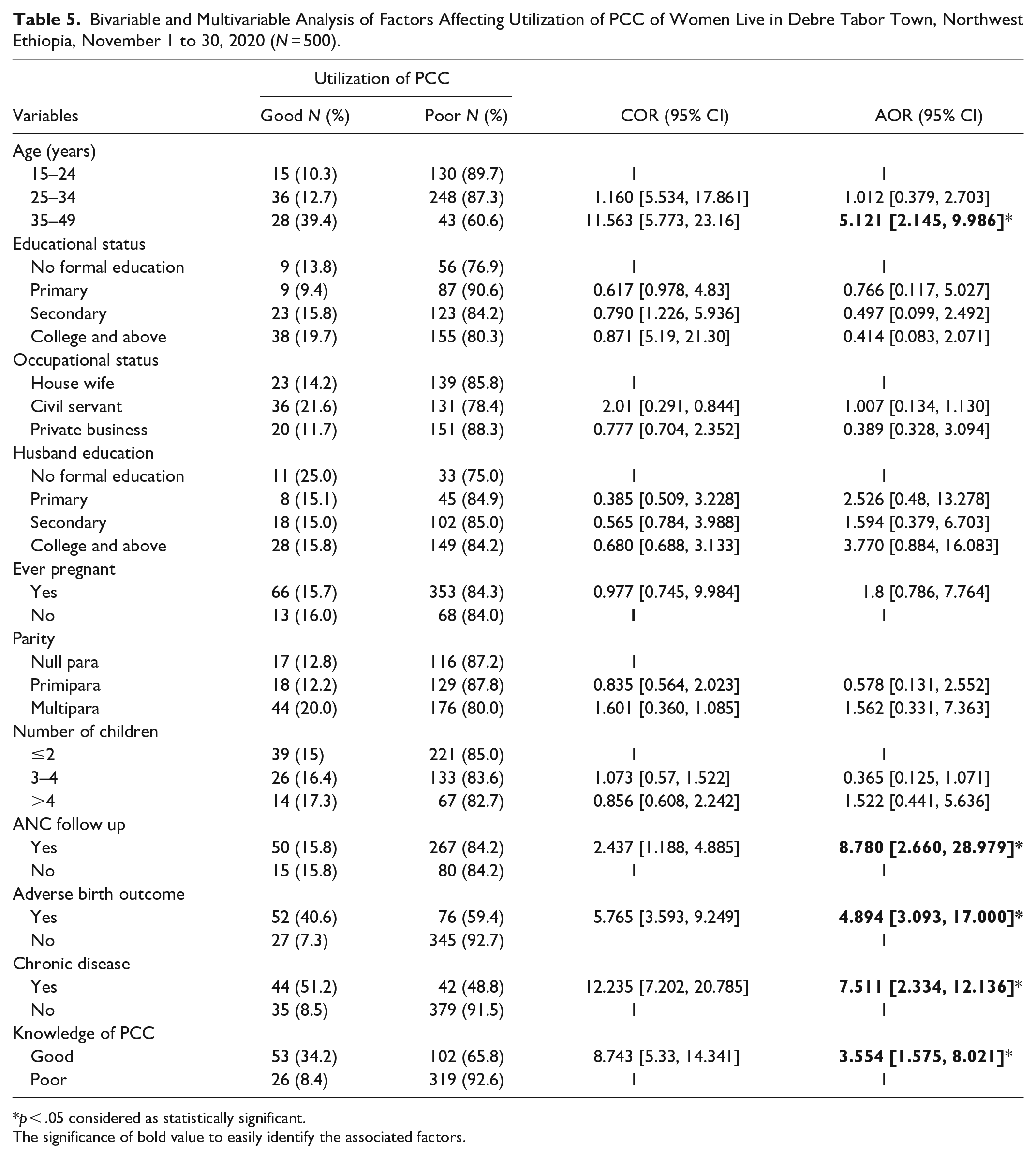
p < .05 considered as statistically significant.
The significance of bold value to easily identify the associated factors.
Discussion
Preconception care can address a full range of women’s and couple’s health needs to produce healthy newborn, family, and a large community. According to our finding, only 15.8% (95% CI [12.6, 19.0]) of women were adequately practice PCC. This was consistent with a study finding from Brazil 15.9% (Borges et al., 2016), Mekele 18.2% (Asresu et al., 2019), West Shewa Ethiopia 14.2% (Fekene et al., 2020), and Debre Birhan 13.4% (Demisse et al., 2019).
However, the current finding was lower than a study carried out in China 20.6% (You et al., 2015), London 27% (Stephenson et al., 2014), Maryland 33.1% (Connor et al., 2014), Canada 44% (Best Start Resource, 2009), Los Angeles 28.8% (Batra et al., 2016), USA 35% (Case et al., 2007), British Colombia 49.4% (Morin et al., 2001), Zambia 33% (Mutale et al., 2017), and Nigeria 34.1% (Olowokere et al., 2015). The low level of PCC uptake might be due to the low sociodemographic status, inadequate infrastructure of the health sectors, and lack of promotion and recognition of PCC with mass media. The health-care system also devotes minimal attention to PCC, there is no preconception clinic at the health-care institution level, and health-care providers are under-dedicated due to a high client load. Besides, lack of appropriate strategies and guiding principles for preconception care in Ethiopia has also its contribution for low utilization of PCC, in Nigeria; there is a strategy to create awareness regarding utilization of PCC. Once more study participant variations may also be another possible reason as evidenced by participants from Zambia were diabetic mothers. This is because mothers with a preexisting chronic health problem need special attention and follow up before conception.
On the contrary, our finding was higher than the previous studies done in Sudan 9% (Ahmed et al., 2015) and Adet Town Ethiopia (Goshu et al., 2018). These discrepancies might be explained by variations in educational status, culture, study participants, and study setting.
Women with older age (35–49) years old were five times more likely utilized to PCC than their counterparts. Similarly, a study conducted in Brazil (Borges et al., 2016), Okhlama (Preconception Care Among Oklahoma Women, 2008), USA (Bennett et al., 2013), Debre Birhan (Demisse et al., 2019), and Adet north west Ethiopia (Goshu et al., 2018) were consistent with our finding. But this was inconsistent with a study done in China (You et al., 2015) and Utah (Maine et al., 2012). This might be due to the fact that when women’s ages increase, their fertility rate decreases and they become more vulnerable to pregnancy complications; as a result, they are more likely to utilize PCC.
According to this study finding, ANC service was another significant factor responsible for the utilization of PCC. Women who had attended ANC visits in recent pregnancies had nearly nine times higher odds to utilized PCC than their counterparts. The possible explanation might be justified by during ANC follow-up women might get an opportunity to discuss with health professionals regarding their reproductive health, gynecological and obstetric history, and family history. At the time of ANC visits, women can also acquire information concerning their health status, means of disease prevention and improving health, as well as birth preparedness and complication readiness. Once more, it may also be that women who have attended ANC visit may have a higher awareness that may a positive effect on their overall lifestyle.
Women who had a history of at least one previous adverse birth outcome were nearly five times more likely to utilize PCC. This finding was supported by a study conducted in Los Angeles (Batra et al., 2016) and Mekele (Asresu et al., 2019) which reported that history of adverse birth outcomes was associated with improved odds of having utilized PCC in the most recent pregnancy. This might be possibly women who had previous experience of adverse birth outcomes were strongly alert and needs PCC in their next attempt before conception.
Similarly, women with previous history of chronic health problems were more utilized PCC. This was in agreement with a study done in Mekele (Asresu et al., 2019). One potential rationale might be because women with the preexisting medical problem need a special follow up and consultation. In addition, to minimize medical complications exacerbated with pregnancy and to get a healthy newborn their medical problem must be stabilized before conception by offering preconception medical checkups and treatment.
Lastly, our study revealed that women’s knowledge had a strong association with PCC utilization. Those women who had a good knowledge of PCC service were three times more likely to utilized PCC than their counterparts. Similarly, findings from China (You et al., 2015), Saudi Arabia (Madanat & Sheshah, 2016), France (Hillemeier et al., 2008), Philadelphia (Mazza & Chapman, 2010), Nigeria (Lawal & Adeleye, 2014), Mekele (Asresu et al., 2019), and Debre Birhan (Demisse et al., 2019) were also comparable with the current finding. Detailed knowledge of PCC may improve women’s awareness of the objective and significance of PCC. In addition, women with some basic level of knowledge had a better understanding of the costs related with not utilizing PCC service. Moreover, good and comprehensive knowledge of PCC may scale up a woman’s perception and awareness which can have a positive impact on the overall healthy life of women, newborns, and the large population.
In general, while Ethiopia’s health policy establishes or states various policies and principles to reduce maternal mortality, such as optimal use of family planning, ANC, and institutional delivery, there is no practical change or commitment in the preconception health care service; therefore, the future policy and strategy should focus on practical implementation regarding preconceptional health care.
The current study was tried to identify predictors associated with PCC service utilization. But it has its limitations. First, since it was entirely a quantitative study, this may lack the capacity to dig out the numerous contextual and social-cultural factors that may be restricting women’s PCC service utilization, so it would be very advisable to recommend future qualitative research. Second, recall bias may be present since the women were interviewed on the previous experience.
Conclusion
In conclusion, the utilization of preconception care was significantly low. Women’s age, ANC service follow-up, history of adverse birth outcome, presence of chronic disease, and knowledge on PCC were the significant factors that affect women’s utilization of preconception care.
Recommendations
The authors suggest that the government and respective stakeholders formulate PCC strategies and policies that can incorporate all elements of the PCC. It is also important to align the program with other maternal and child health programs while developing successful implementation strategies to increase PCC uptake. In addition, promoting women’s education, the development of awareness, and growing ANC service is very imperative. Finally, we proposed that research on mixed approaches, program reviews, and longitudinal research projects be launched to discover and resolve the PCC imperative.
Footnotes
Acknowledgements
The authors would like to recognize Debre Tabor University for ethical approval and Debre Tabor Zonal Health office and town administration for providing the necessary preliminary information. We would also extend our appreciation to all participants, data collectors, and supervisors for their genuine participation in this study.
Author Contributions
All the authors contributed from the beginning to the final writing of the article.
Availability of Data and Materials
The data set using in the study are available from the corresponding author upon a reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
Ethical approval was obtained from Debre Tabor University College of Health Sciences Ethics Review Committee. Also, a letter of cooperation was by the administrative office of the town. Informed consent was available from each respondent. To maintain privacy and to ensure confidentiality, all personal identifiers have been omitted.