
Abstract
This study aimed to assess the knowledge, attitudes, and practice of preconception care among women of reproductive age in Jordan. A cross-sectional study that included a random sample of 1,368 women of reproductive age (18–44 years) was conducted using an online self-reported questionnaire. Of the total respondents, 48.6% had good knowledge, 48.1% had a positive attitude, and 47.0% had good practice. Participants with poor knowledge were more prevalent in the 35 to 44 age group (37.3%). Participants with good knowledge had a more positive attitude (57.2%) and good practice (63.5%). Married participants had a higher negative attitude (82.9%). Participants with university education had a good practice (44.5%), knowledge (58.5%), and a positive attitude (52.9%). There were positive correlations between knowledge, attitude, and practice. Good preconception care knowledge was higher among participants in the youngest age, while positive attitude was higher in the age group 25 to 29 years.
Introduction
Preconception care is defined as a group of biomedical, behavioral, and social risk interventions that impact the quality of pregnancy (Dean et al., 2014; Mason et al., 2014). Although the term “periconceptional” typically refers to the period from just before conception to organogenesis, it is crucial to highlight that this nomenclature is not always used and is not generally accepted (Freda et al., 2006). The American College of Obstetricians and Gynecologists represents the components of preconception care as periodic assessment, genetic disorders and genetic screening, immunizations and infectious diseases, behavioral/psychosocial factors, and medical history and conditions (Freda et al., 2006; Moos, 2003). The welfares of preconception care for mother and children’s health are to enhance implantation and increase the opportunity of pregnancy (Stephenson et al., 2018), minimize maternal morbidity and mortality during pregnancy or delivery (Atrash et al., 2006), improve the lifestyle of the females willing to become pregnant and help them to cease unhealthy habits (Jones et al., 2016). Furthermore, it allows the mother to have enough time to control pre-existing comorbidities (such as diabetes, hypertension, or autoimmune disease) and regulate environmental interventions such as vitamin intake, smoking cessation, and increasing the chance of breastfeeding post-delivery (Dorney & Black, 2018; Simon, 2019; Whitworth & Dowswell, 2009). Therefore, an addendum of preconception care to reproductive medicine is essential to reach the previously mentioned benefits (Simon, 2019).
Several studies have confirmed the efficacy of preconception care in the mother and children’s health, such as lowering the risk of neural tube defects and recurrence (De-Regil et al., 2015). Furthermore, decreasing the prevalence of adolescent pregnancy encourages contraceptive use, promotes mothers’ good nutritional status, sustains a healthy weight, and prevents communicable and transmittable diseases (Gautan & Dhakal, 2016).
Preconception care is still not available in developing countries, including Jordan, and is not routinely used in obstetrics and gynecology clinics (Yohannes et al., 2019). In addition to unplanned pregnancy, and beginning pregnancy monitoring after half of the first trimester of pregnancy (Brundage, 2002). The preceding organogenesis was already started, exposing the fetus to the risk of congenital malformations in some cases (Brundage, 2002; Moos, 2003). Also, a low level of knowledge and a bad attitude regarding preconception care were reported (Boakye-Yiadom et al., 2020; Kasim et al., 2016). Different social media channels, general practitioners, gynecologists and obstetricians, and nutritionists all play an important role in raising preconception awareness (Kasim et al., 2016). However, a significant increase in the knowledge of American women of reproductive age toward general and personal preconception health risks following brief counseling has been reported (Dunlop et al., 2013). In contrast, several studies in different countries around the world have reported relatively poor knowledge levels and negative attitudes among participants accompanied by poor practice or no practice at all (Boakye-Yiadom et al., 2020; Krishnan et al., 2016; Noble & Smith, 2015; Yohannes et al., 2019). Because little is known about preconception care knowledge, attitudes, and practices in Jordan, the current study aimed to assess the overall provision of preconception care knowledge, attitudes, and practices among reproductive-age women in Jordan.
Material and Methods
Design
The study design was cross-sectional. The study was carried out in Jordan in April 2022. A self-reported online questionnaire was used in a random sample of women of reproductive age (18–44 years).
Sampling and Settings
The sample size was calculated by the online sample size calculator Raosoft (Raosoft, Inc. free online software, Seattle, WA, USA) (Roasoft, 2004). According to the CDC, women of reproductive age are identified as women between 15 and 44 years of age (Graham, 2006). In Jordanian law, the official marriage age is 18 years. Based on the Department of Statistics in 2020 women represented 49.37% (5,084,000) of the total population (10,806,000). Women of reproductive age were 58.6% of total women (2,979,224) (Department of Statistics, 2020). With a 5% error margin, 99% CI, and 50% response distribution, the calculated sample size was 664. A total of 1,368 were enrolled in the study. The study protocol was approved by the Institutional Board Review (IRB) committee. The World Medical Association Declaration of Helsinki concerning ethical research relating to human subjects was followed.
Data Collection and Scoring
Data collection was completed using a structured validated online self-administrated questionnaire. A Google Form of the questionnaire was established and distributed through WhatsApp and a post on the Facebook page. The questionnaire was developed in Arabic after an extensive literature review for correlated investigations. It consists of four sections used to elicit “respondents” information. Section one contains questions about demographic data (age group, educational level, marital status, living area, employment status, and health insurance). Section two contains questions about preconception care knowledge (such as the definition of preconception care, the importance of preconception care, etc..). Section three contains questions about the attitude toward preconception care (such as “Preconception care does not have any effect on pregnancy outcome,”“A hospital setting is the best place to provide preconception care,”“I am not the most suitable person plan to get preconception care,”… etc.), and section four contains questions about preconception care practice (Avoiding bad habits when planned to pregnancy, engaging to exercise, vaccination, smoking cessation, folic acid and iron supplementary intake, total blood test, modification for healthy dietary intake, reaching ideal body weight, ….etc.), (Supplemental File 1). on Facebook, the post engagement was 4,316, and the total responses were 1,368, (response rate was 31.7%. but the response rate by WhatsApp was undetermined.
In the preconception care knowledge section, 21 items were used, and the overall knowledge score was calculated for each participant. The mean of the scores was calculated. Those who had a knowledge score above the mean were categorized as having a “good level of knowledge,” whereas those at or below the mean knowledge score were categorized as having a “poor level of knowledge” (Yohannes et al., 2019). In the preconception care attitude section, six questions on a five-point Likert scale (ranging from strongly disagree, disagree, neutral, agree, and strongly agree) were included. The responses were scored from one to five to a positive statement and reversed in negative statements. The possible minimum calculated score was six, and the maximum calculated score was 30. Those who had an attitude score above the mean were categorized as having a positive attitude, whereas those with an attitude score equal to or below the mean had a negative attitude toward preconception care (Yohannes et al., 2019). The practice section consisted of 15 items. A score of “one” was given for good practice answers and “zero” for poor practice answers. The asked questions asked were concerned about the medical follow-up and check-ups, healthy diets, nutritional balance intake, and healthy behaviors and lifestyles (Kasim et al., 2016). The possible expected calculated scores were between zero and 15. The mean of scores was calculated; those who had a practice score above the mean were categorized as a good practice in preconception care, whereas those who had a calculated score equal to or below the mean were categorized as poor practice in preconception care.
Reliability of the Questionnaire
The questionnaire was pre-tested for reliability on a sample of 30 participants, and those who were not included in the final study sample. Cronbach’s alpha (α) was calculated to assess internal consistency and reliability (Noble & Smith, 2015). The results showed good reliability with a total α = .874 (α was .831 for knowledge, .622 for attitude, and .811 for practice).
Statistical Analysis
Analyses were carried out using SPSS software (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp). Frequencies and percentages for general characteristics were calculated using frequency descriptive statistical tests to describe the sample. The chi-square test was used to assess differences in proportions. Spearman rho test was used to assess the coloration. The p-value of <.05 was considered statistically significant.
Results
Table 1 shows the general characteristics of the study participants. The participants were almost equally distrusted between age groups, with a higher percentage for the age group 35 to 44 years (32.6%). Two-thirds of participants were from central governorates (Amman, Balqa, Madaba, and Zarqa), followed by Northern governorates (Mafraq, Irbid, Ajloun, and Jerash) (25.9%). More than half of the participants had a university education, and 75.9% were married. Also, 65.4% had their preconception preparation information from multiple sources. Of the total participants, 61.8% had followed a pre-pregnancy preparation before. Regarding the preconception care knowledge, attitude, and practice, 48.6% of participants had good knowledge, 48.1% had a positive attitude, and 47.0% had good practice (Figure 1, Supplemental File 2).
General Characteristics (n = 1,368).

The correlation between pre-conceptional care knowledge, attitudes, and practice as well as with other variables is illustrated in Table 2. Knowledge and attitude had significantly a weak positive correlation with both age (r = .157, p
Knowledge, Attitudes, and Practice Correlations With Selected Variables (n = 1,368).

Correlation is significant at the .01 level (two-tailed).
Based on preconception care knowledge classification (Table 3), the prevalence of participants with good knowledge among the age group 18 to 24 years (29.8%) was higher compared to those with poor knowledge (17.2%). In comparison, participants with poor knowledge were more prevalent in the 35 to 44 age group (37.3%, p < .001). The participants with good knowledge had a higher positive attitude (57.2%), good practice (63.5%), and a prevalence of practicing pre-pregnancy preparations before (69.1%) compared to poor knowledge participants.
The Correlation of Preconception Care Knowledge With Other Variables (n = 1,368).
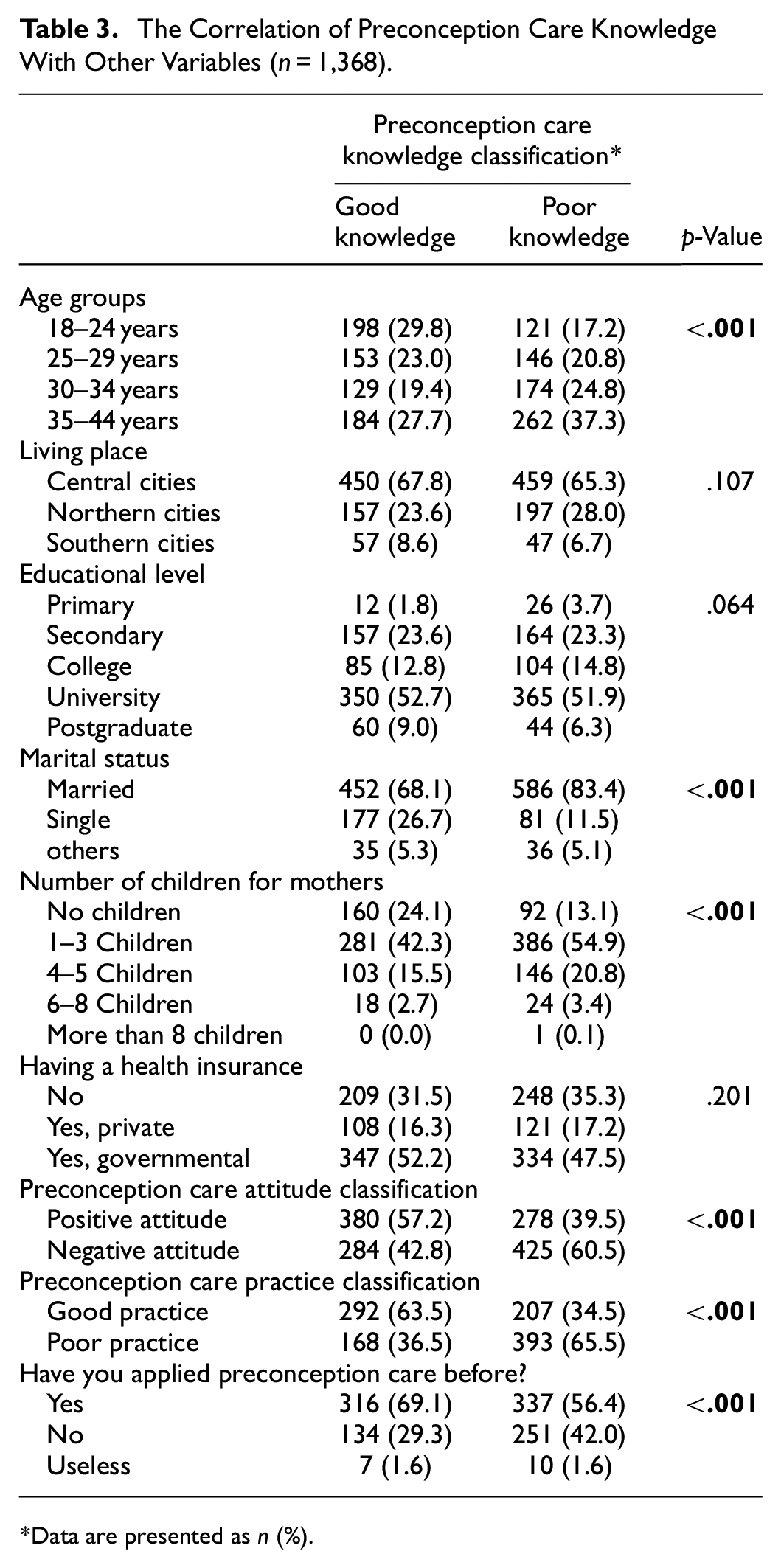
Data are presented as n (%).
The correlation of preconception care attitude with other variables is shown in Table 4. The positive attitude was significantly higher in the participants between 25 and 29 years (23.7%), while lower in the participants between 18 and 24 years (7.8%) and 35 and 44 years (27.7%). Based on the living place, the central cities had a significantly higher positive attitude. While in northern and southern governorates, the negative attitude was the highest Secondary-educated participants had the second higher prevalence of negative attitudes, (27.8%) compared to the positive (18.8%). Married participants had significantly higher negative attitudes (82.9%). On the other hand, single participants had significantly higher positive (26.9%) compared to negative attitudes (11.4%). Based on the number of children, the participants with no children had a higher positive attitude compared to a negative attitude, while those with one or more children had a higher negative attitude prevalence (p < .001). Participants with a positive attitude had a significantly higher prevalence of good practice (57.5%), and good knowledge (57.8%).
The Correlation of Preconception Care Attitude With Other Variables (n = 1,368).
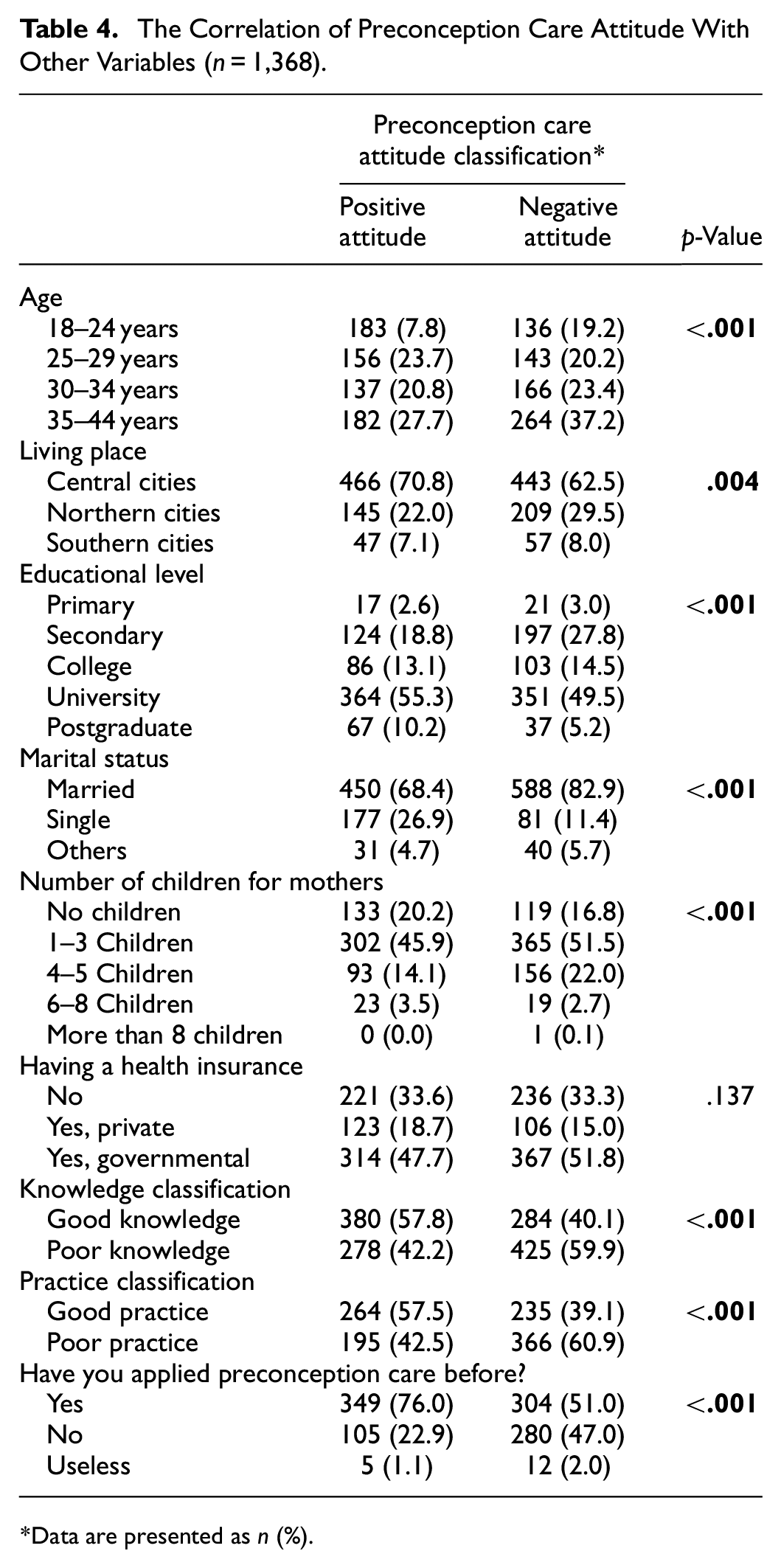
Data are presented as n (%).
In terms of preconception care practice (Table 5), the participants with university education and secondary education. had high negative practices (46.7% and 30.8%; respectively) compared to good practices (44.5% and 25.7%; respectively). On the other hand, participants with primary and college education had higher good practices (4.2% and 19.2%, respectively) compared to poor practices (2.7% and 13.7%; respectively). Regarding insurance, good practice prevalence was higher in those with private or governmental health insurance (19% and 52.7%, respectively) compared to those with poor practice (15.2% and 49.6%, respectively). For those with no insurance, the prevalence of poor practice (35.3%) was higher compared to good practice participants (8.3%, p = .031).
The Correlation of Preconception Care Practice With Other Variables (n = 1,368).

Data are presented as n (%).
Discussion
Women, especially youth, encounter significant obstacles when attempting to receive sexual and reproductive health education and services throughout the Middle East and most of the rest of the world. Many of the obstacles come from the context of service provision and the cultural aspects in the community. In addition, there might not be clear rules for what services should be offered, allowing service providers free to use their discretion or adhere to their own personal values and beliefs (Gausman et al., 2021; Morris & Rushwan, 2015). Until 2015, the provision of reproductive health services in Jordan has been determined to be of poor quality, and a number of issues with provider-client interactions have been observed (Krause et al., 2015). These issues may have a negative impact on the supply of these services. Youth in Jordan have expressed concerns about privacy and confidentiality in the clinic setting due to the strict social and religious norms that forbid sexual activity among young people who are not married, as shown by studies that show that young women are frequently advised against using contraception due to concerns about potential side effects, such as infertility (Al-Shdayfat & Green, 2012; El-Khoury et al., 2015; Khalaf et al., 2010; Krause et al., 2015).
This study assessed the provision of preconception care knowledge, attitude, and practice among Jordanian women of reproductive age. The present findings revealed that 48.6% of participants had good knowledge, 48.1% had a positive attitude, and 47.0% had good practice. The available reported data are conflicting about knowledge of preconception care. The present findings affirm the findings of Al-Akour et al. (2015), who reported that married men and women in Jordan’s center had a 50% awareness prevalence (Al-Akour et al., 2015). In this study, the present level of knowledge was better than the findings in Sudan (11.1%) (Ahmed et al., 2015), Iran (10.4%) (Ghaffari et al., 2014), Nigeria (2.5%) (Lawal & Adeleye, 2014), Turkey (46.3%) (Baykan et al., 2011), and Northwest Ethiopia (27.5%) (Ayalew et al., 2017). However, it was still lower than findings in other countries, such as in British Colombia (71%) (Morin et al., 2001), the low-income Mexican American group in the USA (76%) (Coonrod et al., 2009), Saudi Arabia (84.6%) (Gautan & Dhakal, 2016), Malaysia (98.5%) (Kasim et al., 2016), and the USA (98%) (Coonrod et al., 2009). The current findings of low level of knowledge could be explained by the health sector’s establishment, socioeconomic differences, a lack of preconception services across the country, a lack of promotion of preconception care by the media, and a lack of commitment on the part of healthcare providers (Yohannes et al., 2019).
Despite Jordanian women in the present study having a lower prevalence of good practice (47%), the current findings were better than those in other developing and developed countries. In Sudan (9.0%) (Ahmed et al., 2015), Sri Lanka (27.2%) (Patabendige & Goonewardene, 2013), China (20.6%) (You et al., 2015), UK (27.0%) (Stephenson et al., 2014), and Saudi Arabia (29.3%) (Madanat & Sheshah, 2016). More recently, Mousa et al. (2021) found that half of the respondents do not take complete preconception care (47.2%) in Saudi Arabia (Mousa et al., 2021).
The positive attitude prevalence in the present study was 48.1%, which in line with the results of Boakye-Yiadom et al. (2020), who found that 48.0% of the participants were strongly agreed with and idea concerned about the importance of every woman receiving preconception care before conception takes place (Boakye-Yiadom et al., 2020). More so, data from other studies indicated that most of their respondents showed positive attitudes toward preconception care (Ahmed et al., 2015; Bayrami et al., 2013). Moreover, Yohannes et al. (2019) found that 54.3% possessed a positive attitude toward preconception care (Yohannes et al., 2019). A study conducted by Krishnan et al. (2016) showed that 96.7% of adolescent girls had an unfavorable attitude toward preconception care, though all the respondents (100%) had a favorable attitude during the post-test (Krishnan et al., 2016). The primary source of preconception care information in the present study was from multiple sources (65.4%), followed by social sources (17.5%), instead of obtaining information from health specialists. Notwithstanding, Boakye-Yiadom et al. (2020) reported that the primary source of awareness was from the health facility (20.5%) (Boakye-Yiadom et al., 2020). Similarly, most of the Nigerian participants who seek out preconception care heard about it during their antenatal clinic (Olowokere et al., 2015).
The prevalence of preconception care knowledge in the present data was affected by age group; the highest prevalence of good knowledge was reported in the age group 18 to 24 years (29.8%), while the prevalence of poor knowledge was higher in the age group 35 to 44 years (37.3%). The preconception care knowledge was found not affected by educational level. In contrast to these findings, Boakye-Yiadom et al. (2020) study results revealed a significant association between the educational status (Tertiary level) of the participants and their preconception care awareness, without any statistically significant age association (Boakye-Yiadom et al., 2020). Also, Mousa et al. (2021) reported that educational level is an important effective factor that influences overall public awareness about preconception care (Mousa et al., 2021). In South Ethiopia, 53% of mothers who gave birth in public hospitals had a good level of knowledge of preconception care. Also, they revealed that preconception cares good knowledge had been affected by different variables such as having a radio, planning for pregnancy, and having participated in community consultations related to preconception care (Yohannes et al., 2019).
Not surprisingly, in the current findings, good knowledge participants had a higher positive attitude (57.2%), good practice (63.5%), and a higher prevalence of practicing pre-pregnancy preparations (69.1%). Also, participants with a positive attitude had a significantly higher prevalence of good practice (57.5%), and good knowledge (57.8%). Standing with this, Mousa et al. (2021) revealed that the majority of respondents (73.6%) believed that women don’t undertake complete preconception care due to a lack of knowledge (Mousa et al., 2021). Also, it has been found that preconception care practice had a significant relationship with attitude, and knowledge had a negative correlation with attitudinal disposition (Ogunsanmi Ololade et al., 2021). Unlike Sattarzadeh et al. (2017), who revealed that no significant relationship was found between knowledge and practice (p = .133, r = .238) (Sattarzadeh et al., 2017).
In the present findings, the positive attitude was significantly affected by different variables such as age group (higher in the participants between 25–29 years), the living place (the central cities had a significantly higher positive attitude compared to northern and southern cities, an educational level (secondary-educated participants were the second higher prevalence of the negative attitude), marital status (married participants had significantly higher negative attitudes), and the number of children (the participants with one or more children had a higher negative attitude prevalence). Likewise, it has been reported that women with higher education levels had more positive attitudes toward preconception care than those with a lower education level (Ruechukondamrong & Panichkul, 2011). Kasim et al. (2016) found that younger age group participants did not agree with preconception care as an important health issue, this could be due to the lack of knowledge and fewer encounters with health services (Kasim et al., 2016).
In terms of preconception care practice, the present findings revealed that participants with university education had a higher prevalence of good practices (44.5%). Also, the prevalence of poor practice was significantly higher in those with secondary educational levels (30.8%). This was consistent with the findings of Demisse et al. (2019) who revealed that preconception care practice (utilization) was significantly affected by many factors such as women’s age, knowledge, marital status, and accessibility to preconception care units (Demisse et al., 2019). Furthermore, many studies revealed that practicing preconception care is affected by age group, educational level, employment status, ethnicity, marital status, having a previous problem like miscarriage, stillbirth or abnormality, parity, knowledge of preconception care, availability of the services, and gravidity (Lawal & Adeleye, 2014; Patabendige & Goonewardene, 2013; Stephenson et al., 2014). The present data approved that the prevalence of good practice was higher in those who had governmental health insurance (52.7%) compared to those with poor practice (49.6%). In the same vein, Kasim et al. (2016) revealed that the majority of defendants selected government services as the best choice to receive preconception care advice, as government health centers are easily accessible to the public, the services are also delivered equally, and the affordable low fees for receiving services for everyone compared to private health facilities (Kasim et al., 2016).
This study also showed a significant correlation between women’s knowledge and good practice. The prevalence of poor practice was significantly higher in those with poor knowledge (70.1%) and a negative attitude (65.2%). This was confirmed by Demisse et al. (2019) findings who noted that women with good preconception care knowledge were 6.2 times more likely to practice preconception care compared to those with poor knowledge (Demisse et al., 2019). Also, this is consistence with a finding from Saudi Arabia (Madanat & Sheshah, 2016), and Nigeria (Lawal & Adeleye, 2014). This may be due to the depth of knowledge that might enhance women’s understanding and awareness of the preconception care importance.
As this study is a cross-sectional survey, we acknowledge some limitations regarding the probability of recall and social desirability biases. Also, another possible limitation is the fact that it ’didn’t include the husbands or spouses of the women. The questionnaire was completed in an online format and unofficial collaboration from other people potentially may have occurred. Repeating this survey using face-to-face interviews may increase the generalizability of the results.
Conclusion
In conclusion, this study revealed that almost half of the participants had good pre-conceptional care knowledge, practices, and positive attuited. Education programs and lectures targeting women of production age especially married women with children or preparing for marriage and their husbands are needed. Moreover, these results should be considered by the healthcare educators with needed tools and facilities must be provided in all healthcare centers that deal with pregnancy. Also, governmental and nongovernmental health care providers should be included in the education program concerning preconception care education to help increase the awareness of the importance of pre-conceptional care among the general population, and people of marriage age specifically. Further studies are needed to determine the weak points and difficulties facing good pre-conceptional care knowledge, attuited, and practices.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241245221 – Supplemental material for Assessing the Provision of Preconception Care Knowledge, Attitudes, and Practice Among Jordanian Women of Reproductive Age
Supplemental material, sj-docx-1-sgo-10.1177_21582440241245221 for Assessing the Provision of Preconception Care Knowledge, Attitudes, and Practice Among Jordanian Women of Reproductive Age by Buthaina Alkhatib, Lana M. Agraib, Huda Al Hourani and Hanan Hasan in SAGE Open
Supplemental Material
sj-docx-2-sgo-10.1177_21582440241245221 – Supplemental material for Assessing the Provision of Preconception Care Knowledge, Attitudes, and Practice Among Jordanian Women of Reproductive Age
Supplemental material, sj-docx-2-sgo-10.1177_21582440241245221 for Assessing the Provision of Preconception Care Knowledge, Attitudes, and Practice Among Jordanian Women of Reproductive Age by Buthaina Alkhatib, Lana M. Agraib, Huda Al Hourani and Hanan Hasan in SAGE Open
Footnotes
Acknowledgements
The authors would like to thank The Hashemite University for its support.
Authors’ Contribution
Buthaina Alkhatib, Hanan Hasan, and Lana M. Agraib data acquisition, statistical analysis, and interpreted the results. Buthaina Alkhatib, Huda Al Hourani, Hanan Hassan, and Lana M. Agraib, involved in the concept and design of the study, inducted and drafted the manuscript and reviewed and provided inputs on the manuscript. All authors critically revised the manuscript, approved the final version to be published, and agreed to be accountable for all aspects of the work
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was ethically approved by the Institutional Board Review (IRB) committee of The Hashemite University in 2022 (registration numbers No.21/6/2021/2022).
Consent to Participate
Informed consent was obtained from the participants and informed about the study objectives at the beginning of the questionnaire, then they expressed their informed consent to participate, and their data were anonymous
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.