
Abstract
Preconception care can play a critical role in reducing maternal and child mortality and morbidity. It provided by knowledgeable healthcare providers is very important to reduce maternal and child mortality and morbidity. However, there are no available detailed review articles in Ethiopia. Therefore, the purpose of this study was to ascertain the pooled knowledge of preconception care and related factors among Ethiopian healthcare providers. A variety of data sources, such as PubMed, Scopus, Embase, and African Journal Online were used to identify studies. A web search engine was used to search for relevant articles from January 1, 2023 to March 2, 2023. The data were extracted by Excel and analyzed using Stata 11 software. Pooled effect sizes were calculated based on the pooled prevalence of knowledge of preconception care and odds ratios for associated factors, with a 95% confidence interval indicating statistical significance. To evaluate statistical heterogeneity, the Cochrane Q test and I2 statistic were used. Newcastle–Ottawa Scale was used the quality appraisal. Eight studies involving 3,848 healthcare providers were included. The pooled prevalence of a good knowledge of preconception care among healthcare providers in Ethiopia was 53.54 (95% CI [45.09, 61.98]), p < .0001. Healthcare providers who had a degree and above educational status (AOR = 4.83; 95% CI [1.80, 12.96]), working at hospital health facilities (AOR = 2.97; 95% CI [2.07, 4.27]), ever reading preconception care guidelines (AOR = 3.49; 95% CI [2.39, 5.07]), availability of libraries at health facilities (AOR = 5.59; 95% CI [2.84, 11.04]), trained healthcare providers on HIV counseling and testing (AOR = 6.86; 95% CI [3.75, 12.53]), and trained healthcare providers on preconception care (AOR = 6.19; 95% CI [4.23, 9.06]) were predictors of a good knowledge with preconception care. Nearly half of healthcare providers do not have good knowledge of preconception care in Ethiopia. Therefore, healthcare providers’ knowledge of preconception care should be improved through preconception care and HIV counseling and testing training and access to guidelines, libraries, and the internet at nearby health facilities, especially at health centers. Finally, stakeholders collaborate with policymakers to develop strategies to improve healthcare providers’ preconception care good knowledge.
Introduction
According to the World Health Organization (WHO), preconception care comprises a range of interventions aimed at identifying and modifying medical, behavioral, and social health risks during reproductive age groups in years (World Health Organization, 2013. Some reproductive healthcare systems include screening for preventing risk factors, managing medical conditions, providing immunizations, supplementing iron and folic acid, modifying lifestyles and behaviors, and treating psychosocial problems (Ministry of Health Ethiopia, 2021). For these reasons, preconception care (PCC) is pivotal for improving pregnant women’s childbirth outcomes and family health (A. Kassa et al., 2018).
The leading cause of maternal fatalities worldwide is hemorrhage (27%), followed by preexisting diseases (15%), hypertension (14%), sepsis (11%), abortion (8%), and other indirect causes (7%; World Health Organization, 2016). Approximately 4 million children die in the first month of life, accounting for 40% of all deaths under the age of 5 years, with nearly all (98%) occurring in developing nations (Majella et al., 2019). During the period from 2018 to 2020, the death rate for children under 5 years of age was 42.5 per 1,000 live births (Myat et al., 2021). Each year, 527,000 pregnant women die from pregnancy-related problems in sub-Saharan Africa (Alamneh et al., 2021). Providing preconception care for reproductive-age couples is very important for improving the health of women, newborns and children (Ayele et al., 2021).
Although the Ethiopian Ministry of Health has launched new preconception care clinical guidelines (Ministry of Health Ethiopia, 2021) for improving reproductive health for women and couples, reducing maternal mortality and improving childbirth outcomes have not been achieved as sustainable goals (Ukoha et al., 2022). These new guidelines state that preconception care (assessing poor obstetric outcomes, such as early neonatal death, frequent abortion, stillbirth and birth defects, gestational diabetes mellitus, preterm birth and small for gestational age babies) should be provided by knowledgeable and skilled clinicians before conception (Kassie et al., 2023). For these reasons, preconception care has become a standard procedure and can be applied to every health facility (Biratu, 2017; Munthali et al., 2021). By setting up preconception care, a platform and implementing necessary packages at health facilities can reduce the risk of maternal, newborn, child, and stillborn infants (Lassi et al., 2014; World Health Organization, 2018). However, there are still challenges in reducing maternal and childbirth mortality (Abebe et al., 2019). Summarized evidence, like this review is needed to address these challenges to improve the quality and efficiency of healthcare service provision within the health care delivery system. Even if some clinical guidelines are incorporated into maternal and child healthcare systems, maternal and child mortality are not significantly lower in Ethiopia (Ethiopian Public Health Institute, ICF, 2019). According to a systematic literature review of Ethiopian countries, the maternal mortality rate was 267 deaths for every 100,000 live births, the neonatal mortality rate was 29%, and the under-five mortality rate was 67 deaths for every 1,000 live births (Izedonmwen & Izedonmwen, 2023), 77% of which could be avoided by providing comprehensive healthcare services, such as preconception care (Black et al., 2016; Ebrahim et al., 2006); however, maternal and neonatal mortality reduction has not reached the intended level at the national level (Ojifinni & Ibisomi, 2020; Ukoha & Mtshali, 2021). The findings showed that the prevalence of knowledge of preconception care among Ethiopian women was 30.95% (Ayele et al., 2021). This finding showed that women’s knowledge of preconception care was significantly low.
According to some primary studies, the knowledge of healthcare providers is affected by a lack of healthcare providers’ awareness, inaccessible new guidelines, poor infrastructure for preconception care, and a lack of training, specifically about how to manage reproductive health problems in individuals who have poor obstetric care (Ayalew et al., 2017; Hebo et al., 2019; Wilson, 2020; Wondaferash, 2012). Moreover, preventive measures at the national level are heavily dependent on integrating preconception care into the regular practices of healthcare providers (HCPs) to prevent this negative obstetric outcome (Loya et al., 2020). Although some primary studies have been conducted on HCPs’ knowledge and associated factors, the studies on total healthcare providers in Ethiopia are inconsistent (Abayneh et al., 2022; Asfaha et al., 2022; Bekele et al., 2020; Belay et al., 2020), which implies that there is no comprehensive review of the available evidence. Therefore, the purpose of this study was to evaluate healthcare providers’ knowledge of preconception care and its associated factors in Ethiopian public health institutions.
Methods
The current study examined healthcare professionals’ knowledge of preconception care and related aspects while they were employed by Ethiopian public health institutions. Letters, reviews, cases and commentaries were not included in the study. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used for the systematic review and meta-analysis (Subirana et al., 2005; Supplemental Material S1-(PRISMA) check list). The protocol for the review was registered with the PROSPERO database with the number: CRD42024505460.
Data Source and Search Strategy
Search Strategy and Review Process
The authors conducted a comprehensive search of using electronic databases (PubMed/Medline, Scopus, African Journal Online, and Embase) were used from January 1,2023 up to March 2, 2023. To ensure that no primary studies were overlooked, a confirmatory Google Scholar search was conducted. We looked through the digital holdings of the Ethiopian University of Science and Technology to find gray literature.
We authors have used the following keywords during our search; ((knowledge) AND (preconception care)) AND (associated factors)) OR (determinants)) OR (predictors)) AND (healthcare providers who worked in public health facilities))) OR ((health workers who worked at governmental health facilities))) AND (Ethiopia). Then systematic review and meta-analysis protocol was performed. The modified population-intervention-comparison-outcome-type of study-context (PECOT) framework (see Table 1) was used to construct the qualifying parameters for this review.
Framework for Determining the Eligibility of Studies (PECOT).

The search was restricted to research involving healthcare providers who worked in Ethiopia’s public health facilities and had a solid understanding of preconception care and related factors. Any differences were settled by consensus-building and discussion based on predetermined standards, or by all investigators in the event that a consensus could not be formed.
Inclusion and Exclusion Criteria
Primary Studies That Used Different Methods to Measure the Prevalence of Knowledge of Preconception Care Among Healthcare Providers, in Ethiopia, 2023.

Results
A total of 28,800 articles related to healthcare providers’ knowledge of preconception care and associated factors in public health institutions in Ethiopia were initially assessed. After removed, 1,237 duplicate articles, 24,750 papers were excluded based on their titles and abstracts. Among the 51 studies that underwent full-text review, 43 were excluded due to differences in study participants and missing outcome variables. Finally, only eight studies met all eligibility criteria and were included in the meta-analysis (Figure 1).

Flow chart showing records considered for systematic meta-analysis of knowledge of preconception care and its associations with healthcare providers in Ethiopia.
Characteristics of the Included Studies
All included studies used a facility-based cross-sectional study design to estimate the knowledge of preconception care. All studies were performed from 2018 to 2022. Five of the studies used simple sampling techniques (Abayneh et al., 2022; Asfaha et al., 2022; Belay et al., 2020; Sori et al., 2021), and three used multistage sampling techniques (Bekele et al., 2020; A. Kassa et al., 2018; Nega, 2021). From an estimated 3848 healthcare providers, a total of 3,768 participants were involved, with an estimated sample size ranging from 156 (Abayneh et al., 2022) to 664 (Nega, 2021). The included studies reported that knowledge of preconception care ranged from 31.0% (A. Kassa et al., 2018) to 97.1% Abayneh et al., 2022. All the studies were performed in six Regions (Amhara, Oromia, Addis Ababa, Southern Nations Nationalities, Harreri, and Hawassa). Three of the studies included in this review were conducted in the Amhara Region (Bekele et al., 2020; Belay et al., 2020; Nega, 2021; Table 3).
Summary of the nine observational studies included in the meta-analysis assessing healthcare providers, preconception care in Ethiopia, 2023.

Note. SRS = systematic random sampling; MSR = multistage random sampling.
Preconception Care Knowledge
The overall pooled good knowledge of preconception care among healthcare providers in Ethiopia was 53.5%. Substantial heterogeneity across the included studies was presented (I2 = 69.5%; p < .002) in the estimation of the pooled prevalence of preconception care good knowledge among healthcare providers. For this reason, a random effects model was employed to determine the pooled prevalence of preconception care good knowledge among healthcare providers (Figure 2).

Forest plot of the pooled knowledge of preconception care among healthcare providers in Ethiopia.
Subgroup Analysis
Subgroup analysis was carried out basis of on the sampling technique used in the primary studies. Accordingly, the highest pooled prevalence of good knowledge of preconception care was observed with simple random sampling techniques at 59.73% (95% CI [51.80, 67.67]), and the lowest pooled prevalence of good knowledge of preconception care was observed with multistage sampling techniques at 42.84% (95% CI [31.10, 54.59]; Figure 3).

Subgroup analysis (by sampling technique) of studies included in the meta-analysis on knowledge of preconception care among healthcare providers in Ethiopia.

Graphical representation of publication bias using funnel plots of all included studies.
Factors Associated With Knowledge of Preconception Care
This comprehensive review and meta-analysis revealed that good knowledge of preconception care among Ethiopian healthcare providers was strongly associated with educational status, healthcare providers who worked at hospital facilities, healthcare providers who read preconception care guidelines, those trained on HIV counseling and testing, those receiving preconception care, and those with access to a library near a health facility.
According to this study, four studies indicated that healthcare providers who had a degree and above education had a significant association with good knowledge of preconception care. The odds of having good knowledge of preconception care were 4.83 times greater (AOR = 4.83; 95% CI [1.80, 12.96]) among healthcare providers who had a degree-and-above holders’ education status in preconception care than among those who had below-degree holders’ education status. The studies included in this meta-analysis were marked by heterogeneity (I2 = 97.0%, p = .000). As a result, a random effect model was performed (Figure 5).

Forest plot showing the pooled odds ratio of the association between healthcare providers who have a degree and above educational status and good knowledge of preconception care in Ethiopia.
Four studies indicated that healthcare providers who worked at hospital health facilities had a significant association with good knowledge of preconception care. The odds of having good knowledge of preconception care were 2.97 times (AOR = 2.97; 95% CI [2.07, 4.27]) greater among healthcare providers who worked at hospital health facilities than among those who worked at health centers. In this meta-analysis, the included studies exhibited heterogeneity (I2 = 68.1%, p = .024; Figure 6).

Forest plot showing the pooled odds ratio of the association between healthcare providers who worked at hospital health facilities and good knowledge of preconception care in Ethiopia.
Among six studies indicated that healthcare providers who had ever read PCC guidelines had a significant association with good knowledge of preconception care. Hence, healthcare providers who read preconception care guidelines were 3.49 times (AOR = 3.49; 95% CI [2.39, 5.07]) more likely to have good knowledge of preconception care than those who did not read the preconception care guidelines. A random effects model was used in this meta-analysis because of the included studies were characterized by the existence of heterogeneity (I2 = 77.9%, p = 000; Figure 7).
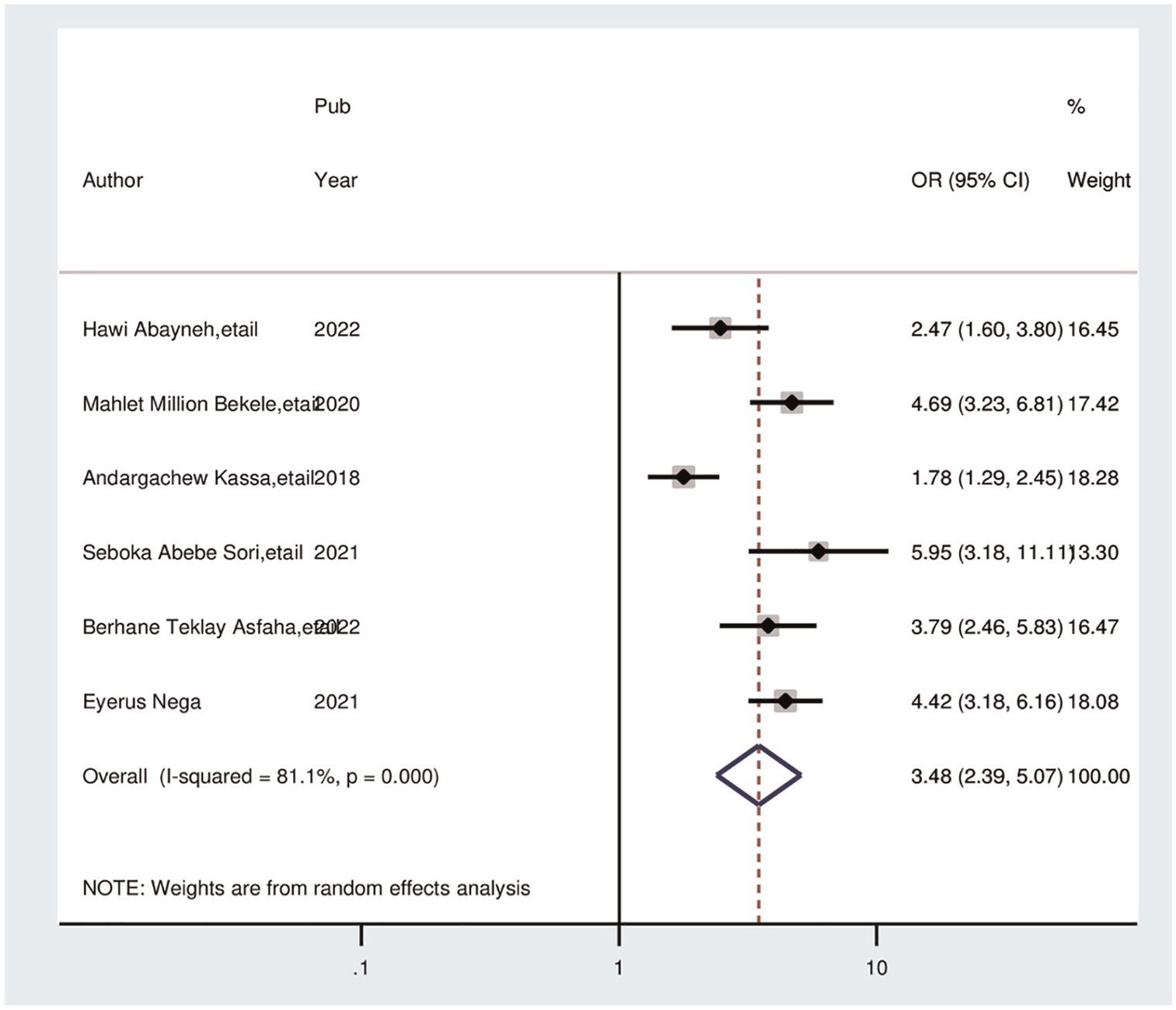
Forest plot showing the pooled odds ratio of the association between healthcare providers who read preconception care guidelines and good knowledge of preconception care in Ethiopia.
Three studies also showed that healthcare providers being trained in HIV counseling and testing was associated with good knowledge of preconception care. The odds of good knowledge of preconception care were 6.86 times greater (AOR = 6.86; 95% CI [3.75, 12.53]) among healthcare providers who were trained on HIV counseling and testing than among their counterparts. A random effects model was used in this meta-analysis due to the presence of heterogeneity (I2 = 86.6%, p = .001; Figure 8).

Forest plot showing the pooled odds ratio of the association between healthcare providers who trained on HIV counseling and testing and good knowledge of preconception care in Ethiopia.
Moreover, five studies also showed that the availability of libraries at health facilities was associated with preconception care and good knowledge. The odds of having preconception care knowledge were approximately 5.60 times greater (AOR = 5.59; 95% CI [2.84, 11.04]) among healthcare providers who had libraries than among their counterparts. We used a random effects model to reduce the presence of high heterogeneity (I2 = 93.1%, p = .000; Figure 9).

Forest plot showing the pooled odds ratio of the association between the availability of libraries for health stakeholders and good knowledge of preconception care in Ethiopia.
Finally, five studies revealed a correlation between healthcare providers who were trained in preconception care and those who trained in preconception care. Hence, this association showed that healthcare providers who were trained in preconception care were more knowledgeable than their counterparts. The odds of knowledge about preconception care were approximately 6.20 times greater (AOR = 6.19; 95% CI [4.23, 9.06]) among those trained on preconception care healthcare providers than among those did not trained in preconception care. We also performed a meta-analysis and employed a random effects model to prevent high levels of heterogeneity across the included studies (I2 = 82.8%, p = .000; Figure 10).

Forest plot showing the pooled odds ratio of the association between healthcare providers who received preconception care training and those with good knowledge of preconception care in Ethiopia.
Discussion
The purpose of this systematic review and meta-analysis was to determine the good knowledge and its associated factors in preconception care among healthcare providers. The evidence provides a basis for good knowledge and determinants of preconception care among healthcare providers who work at health facilities in Ethiopia. Accordingly, healthcare providers are attempting to gather sufficient knowledge on preconception care, which plays a crucial role in good birth outcomes. This meta-analysis revealed that 53.53% (95% CI [45.09, 61.98]) of healthcare providers had a good knowledge of preconception care. This finding implies that the need for preconception care awareness and the implementation of the Ethiopian Ministry of Health’s preconception care guidelines for all healthcare providers, as well as healthcare, will help promote preconception care at the healthcare system level. Furthermore, this finding infers the need to make plans once knowledge gaps are identified. Strengthening preconception care by focusing on determinants of good knowledge among healthcare providers is one of the most important components for improving the quality of preconception care (Asfaha et al., 2022). Healthcare providers’ knowledge of preconception care and associated factors is needed to achieve good long-term maternal and child health outcomes.
Although preconception care services are available for all healthcare system providers and different primary studies were available, no comparable meta-analysis has been carried out on this topic at the national level. This finding is in line with those of studies conducted in Nigeria (58.3%; Karalolo et al., 2021) and Quatar (53.7%; Bener et al., 2006). These similarities might be due to the similarities in educational status, policies and guidelines used, and healthcare approaches used in developing countries. This result suggested that preconception care strategies/activities for raising awareness were insufficient, but further studies are needed to increase healthcare practitioners’ knowledge of these strategies/activities. To effectively implement preconception care at every health facility, it is necessary to involve both governmental and nongovernmental stakeholders to provide preconception care.
However, this figure is lower than that of survey studies carried out in China (90%; Ding et al., 2015), Canada (70%; Funk et al., 2015) and the USA (76%; Coonrod et al., 2009). The possible reasons might be the low socioeconomic status, differences in the infrastructure of the health sector, lack of health promotion of preconception care reported in the media coverage for preconception care across the county, lack of preconception clinics at the health institution level, and low commitment of healthcare workers due to the high case flow of clients in Ethiopia, which could be contributing factors to the low level of knowledge reported in this study.
This good knowledge of healthcare providers (53.53%) was also higher than that reported in a study conducted in sub-Saharan Africa (24.5%; Ameh et al., 2016) and studies among women in Ethiopia (35.7%; Ameh et al., 2016). These discrepancies could be due to differences in the educational status of the study participants. This funding implies that our study participants were healthcare providers, which may increase their knowledge of preconception care and its implementation by the national healthcare system. Therefore, multiple stakeholders need to be involved to further improve the knowledge of healthcare providers about preconception care.
This meta-analysis revealed that healthcare providers who had a degree and above were nearly five times more likely to be knowledgeable than healthcare providers who had a below-degree education (AOR = 4.83; 95% CI [1.80, 12.96]). Similar findings were comparable to the outcomes reported in studies in Sudan (Shannon et al., 2014), Africa (Tekalign et al., 2021), and America (Walter et al., 2020). These results might be explained by the fact that as the educational level of healthcare providers increases, so do professionals’ positive attitudes toward preconception care. More highly educated (degree and above) healthcare providers might therefore be more inclined to offer preconception care. Additionally, more educated health professionals can have easier access to or a stronger desire to seek out sources of knowledge pertaining to their well-being and have better preconception care management strategies for their reproductive health system.
Similarly, healthcare providers who worked at hospital health facilities were almost three times more knowledgeable about preconception care than those who worked at health centers were (AOR = 2.97; 95% CI [2.07, 4.27]). The findings presented here were in parallel with studies conducted in the United States (Johnson et al., 2006) and England (Stephenson et al., 2014). This study suggested that providing preconception care at hospital health facilities may involve more experienced physicians and more accessible medications than preconception care at health center facilities. Healthcare providers know that healthcare providers who work at comprehensive hospital levels may have much work experience and increased good knowledge of preconception care.
The current meta-analysis also indicated that healthcare providers who had ever read preconception care guidelines were 3.49 times more likely to have good knowledge of preconception care than their counterparts were (AOR = 3.49; 95% CI [2.39, 5.07]). This finding is supported by study performed in Australia (Harrison et al., 2021). Moreover, this study demonstrated that healthcare providers from health institutions that had plans for preconception care were more knowledgeable about preconception care than their counterparts. This is supported by the fact that healthcare providers should read preconception care guidelines (Sattarzadeh et al., 2017). Policies, guidelines, recommendations and services related to preconception care are crucial for identifying, controlling, and treating risk factors that have an impact on obstetric outcomes (Z. Kassa, 2021; Shawe et al., 2015). Therefore, healthcare providers who have ever read such guidelines may have good knowledge and motivation to implement preconception care.
The current meta-analysis also revealed that knowledge scores increase with training on HIV testing and counseling to provide preconception care. As a result, healthcare providers who trained on HIV testing presented with good knowledge scores on preconception care (AOR = 6.86; 95% CI [3.75, 12.53]) and 6.19 times (AOR = 6.19; 95% CI [4.23, 9.06]) more good knowledge about preconception care among trained healthcare providers on related preconception than did their counterparts. This might be due to the impacts of the attention given to the prevention of HIV/AIDS transmission and improving birth outcomes, as government agenda implementation enables health providers’ knowledge to improve preconception care (Bekele et al., 2020; Tekalign et al., 2021). As a result, healthcare providers may gain a good knowledge about overall gynecological and obstetrical healthcare services.
Moreover, the availability of a library at a health facility was approximately 5.60 times greater when preconception care was provided than when healthcare providers did not have a library at a public health facility (AOR = 5.59; 95% CI [2.84, 11.04]). This association might be due to the library’s access to preconception care information. These associations are supported by a systematic review among reproductive-age women and couples, which showed that those available in the library at a health facility had a broader understanding of complications associated with being unable to receive preconception care than their counterparts (Alemu et al., 2021; Tekalign et al., 2021). A Healthcare providers’ good knowledge of healthcare providers about preconception care services should be improved by reading preconception care guidelines at the library or by using smartphones. For these reasons, the Ethiopian Ministry of Health should design libraries and implement important preconception care guidelines at nearby health facilities.
Despite its considerable value, this systematic review and meta-analysis has several limitations. The result variable may be influenced by other confounding variables, such as misunderstandings, knowledge, and accessibility of the service, as all of the research included in this review was cross-sectional. Second, the small sample sizes of some of the primary studies included in this systematic review and meta-analysis could have affected on the true knowledge at the national level. Third, because of the various categories, a few significant variables were overlooked. Fourth, only five regions and one administrative town in Ethiopia were included in this study’s review because of the nation’s small number of primary studies.
Relevance to Research
The findings of this study will serve as a roadmap for future research to provide an in-depth understanding of preconception care and its variables in Ethiopia. Future policymakers should pay special attention to lowering maternal and child morbidity and death associated with the inability to provide preconception care. Research should also concentrate on advancing the understanding of the sociodemographic and other factors associated with poor preconception care to tailor health promotion initiatives for the most vulnerable segments of the reproductive-age population and future generations and to provide individualized coaching and information to improve nutrition and lifestyle during the preconception period.
Conclusions and Recommendations
Nearly half of healthcare providers do not have a good knowledge of preconception care in Ethiopia. For this low knowledge about preconception care; healthcare providers’ low educational status, lack of training in preconception care, HIV testing, absence of guidelines, libraries, and lack of internet access at nearby health facilities were significant factors. Hence, stakeholders and policymakers should work on strategies and policies to improve healthcare providers’ knowledge of preconception care by accessing internet services and mini-libraries nearby health facilities. In addition, we wish to recommend to the Ethiopian Ministry of Health and Health Bureaus that they organize and provide continuous refreshment training on preconception care, HIV counseling, testing and making the available guidelines for diploma-level health workers. Moreover, to obtain more comprehensive evidence, we recommend further scoping reviews.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251334881 – Supplemental material for Healthcare Providers’ Preconception Care Knowledge and Associated Factors in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-sgo-10.1177_21582440251334881 for Healthcare Providers’ Preconception Care Knowledge and Associated Factors in Ethiopia: A Systematic Review and Meta-Analysis by Agerie Mengistie Zeleke, Worku Chekol Tassew, Yosef Aragaw Gonete and Yeshiwas Ayale Ferede in SAGE Open
Footnotes
Acknowledgements
The authors would like to thank the authors of the included primary studies, which were used as sources of information to conduct this systematic review and meta-analysis.
Author Contributions
Agerie Mengistie Zeleke: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing. Worku Chekole Tassew: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing. Yosef Aragaw Gonete: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing. Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing. Yeshiwas Ayele Ferede: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study were derived from previously published systematic reviews and meta-analyses, which were cited within this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.