
Abstract
Despite the significant benefit of postpartum modern contraceptives to avert the problems related to short interpregnancy intervals and unintended pregnancy, still the uptake remains low in Ethiopia. The aim of the study was to assess the magnitude of family planning use during the puerperium period and the factors associated with it in the Benchi Sheko zone of Southwest Ethiopia. From 10th March to 10th May/2021, 385 mothers were enrolled in a community-based cross-sectional study. Participants were nominated using simple random sampling. To collect the data, an interviewer-administered questionnaire was used. To identify the factors associated with the utilization of postpartum contraceptives, bivariate and multivariable logistic regression analyses were used. The statistical significance level was determined at p-value < .05. The overall utilization of postpartum modern family planning utilization was 50.4% (95% CI: 45.3, 55.3). Maternal education (AOR = 2.26, 95% CI; 1.03–4.95), informed on family planning (AOR = 0.34, 95% CI; 0.13–0.91), counseled on contraceptives during Antenatal Care (ANC) (AOR = 1.82, 95% CI: 1.05–3.17), previous family planning utilization (AOR = 0.45, 95% CI: 0.28–0.73), counseled on contraceptives at the time of PNC (AOR = 1.70, 95% CI: 1.07–2.71), and resumption of sexual intercourse after delivery (AOR = 4.17, 95% CI: 1.57–11.08) were the major factors hindering the utilization of modern contraceptives. the overall magnitude of modern contraceptive utilization during the puerperium period was low. Having counseling, information, and previous experience in family planning, and time to sexual intercourse resumption were clinical predictors of family planning utilization. A concerted effort to incorporate contraceptive services into maternal, neonatal, and child health (MNCH) service units should strengthen much, and counseling gives due emphasis.
Introduction
Family planning is defined as “the decision-making process by couples, together or individually, on the number of children that they would like to have in their lifetime, the age interval between children, and the timing of their births by using contraceptive methods” (Bongaarts et al., 2012). Postpartum family planning (PPFP) is defined as women who have used any type of family planning method within the first 12 months after birth (WHO, 2013). For women, children, families, and countries at large, the utilization of contraceptives have advantages (WHO, 2016). Despite their best needs, millions of women in the world are lacking safe and effective methods of family planning (WHO, 2016).
Postpartum family planning could avert maternal and childbirth-related problems globally, which are linked with closely spaced births; for instance, maximizing the risk of failed vaginal birth after cesarean delivery (VBAC), childhood undernourishment, stunted growth, underweight, prematurity, and death of child (Kassebaum et al., 2014). Utilization of contraceptives halts more than three million under-five deaths and 109,000 maternal deaths. However, as evidenced by a finding from 57 countries, 62% of women had experienced contraceptive unmet needs (Rossier et al., 2015). The indicator of family planning in Sub-Saharan Africa (SSA) were manifested by very low utilization (33%) and high unmet need (24%) (WHO, 2016) Among women with unmet contraceptive needs, 82% of the pregnancies were unintended and it also became a major contributor to unsafe abortions, unplanned births, and maternal mortality (Tesfaye et al., 2017). If all unmet contraceptive needs were satisfied, mortality of women would decrease by almost one-third of current trends, and unplanned pregnancies and unsafe abortions would minimize by more than 90% (Sundaram et al., 2010).
Even though pregnancy not intended during conception occurring in the early postpartum period is correlated to adverse outcomes, the proportion is still alarmingly high. Globally, due to low family planning uptake during the postpartum period, about 80 million pregnancies were unintended (Tolefac et al., 2017). Of the total women experiencing unmet needs for family planning 40% were contributed by postpartum women in SSA (Dulla et al., 2017). Ethiopia is grouped under one of the countries having high maternal mortalities; 412 per 100,000 live births (Csace, 2016) with high family planning unmet needs resulting in around 38% of pregnancies being unplanned and 13% of unplanned pregnancies in 2014 were ended with induced abortion (Moore et al., 2016). In Ethiopia, the demand for family planning among women who were married scaled up over time from 45% in 2000 to 58% in 2016, and the met family planning need has also scaled up over the same time period from 8% to 36%. Even though the family planning uses scaled up over the years, the unmet family planning needs remained high, 22% in 2016 (Csace, 2016). Postpartum women in Ethiopia are experiencing high unmet family planning needs and the shortest birth interval of fewer than 24 months after the preceding birth (47%) (Anya et al., 2008). Since two-thirds of maternal and neonatal deaths happened within 1 year after childbirth (Matijasevich et al., 2009), appropriate uptake of postpartum contraceptives during this time period can halt those bad consequences (Mathe et al., 2011; Tekelab & Berhanu, 2014). Provision of information about family planning and linking women to postpartum contraceptive services as a continuum of care along with the maternal and neonatal health services units like immunization services were recommended by WHO (Gaffield et al., 2014). Nevertheless, findings in SSA, revealed poor information dissemination about contraceptives or/and women did not get ample information about FP or services from these services provision clinics (Lauro, 2011; WHO, 2002).
In 2020 a review conducted in Ethiopia, found that the uptake of contraceptives during the first year after childbirth was 48.11% (Mehare et al., 2020). Also, different studies conducted in Ethiopia found low uptake of modern contraceptives within 1 year after childbirth (Abraha et al., 2017; Demie et al., 2018; Gejo et al., 2019; Nibret Mihretie et al., 2020; Tegegn et al., 2017; Wassihun et al., 2021) and socio-demographic (i.e., educational status, religion, and poor economic status), and other influencing factors like menses returned, sexual intercourse started, desired to be fertile, antenatal care service uptake, delivered at health facility, age of woman, postnatal care and having knowledge were identified as major factors hindering the uptake of modern family planning within the first year after childbirth (Abraha et al., 2017; Bwazi et al., 2014; Demie et al., 2018; Eliason et al., 2013; Fantahun, 2015; Gejo et al., 2019; Nibret Mihretie et al., 2020; Tegegn et al., 2017; Wassihun et al., 2021).
Even though the magnitudes of unmet family planning needs have been well-assessed overall, there is a dearth of information on modern contraceptive usage and factors hindering its uptake among mothers within the first 1 year after childbirth at the country level in general and Bench Sheko Zone in particular. Therefore, the aim of the study was to determine the magnitude of modern contraceptives utilization among mothers who gave birth in the last year and identify factors hindering its uptake in the study area that are of paramount importance in designing, implementing, and monitoring evidence-based interventions in the locality to enhance the use of postnatal modern contraceptives. Also, it was used to determine the strength of continuity of care given to maternal and child health facilities.
Method and Materials
Study Setting, Design, and Period
A community-based cross-sectional study was employed among mothers who gave birth within the last 1 year in the Bench Sheko zone, from March 10 to May 10, 2021. The Bench Sheko zone is found 561 km far from Addis Ababa. The zone had a total population of 847,168, of whom 429,417 were females as evidenced by the population projection report released by Central statistical agency (CSA) for 2014 to 2017 (Ababa, 2014). It has a total of 169,284 households, 92.6% of the total catchment populations have been addressed by primary health services, and most of the populations were rural residents. It also has one city administration, six Woredas (districts), and 246 kebeles (smallest administrative units). The zone has 2 Hospitals, 26 health centers, and 182 health posts (Zone, 2015).
Population
The reference populations were all mothers who gave birth in the last 1 year before the data collection period in Benchi Sheko Zone, and the study populations were mothers who gave birth in the last 1 year before the data collection period in the selected Woredas (districts). All postpartum mothers who lived in the district for at least 6 months before the data collection period were enrolled in the study, whereas critically ill and unable to communicate mothers were not enrolled in the study.
Sample Size Determination
The representative sample was estimated using the single population proportion formula, n = (Z α/2)2 P(1−P)/(d 2) (Lemeshow et al., 1990). The following parameters have been considered to calculate the sample size; the prevalence of postpartum contraceptive uptake in Arba Minch town, Ethiopia was 44.1% (Wassihun et al., 2021), the confidence interval was 95%, the margin of error (d) was 5% (Hajian-Tilaki, 2011), and the 5% buffer for non-response rate, giving the final sample size was 398.
Sampling Procedure
Multistage random sampling technique was applied. First, using the lottery method, two Woredas (Sheko and Shey Benchi) and Mizan-Aman town administrations were picked. Next, from each selected Woredas, 30% of Kebeles (smallest administrative units) were selected. In all selected kebeles, to identify women who fulfill the inclusion criteria by having registered the birth date of the last child from the family folders which was found from health extension workers, a sample frame was prepared. House-to-house observation was made using the sample frame with their respective household identification number. Then, participants from each selected Kebeles, were determined using proportional to size allocation technique. Lastly, mothers whose last delivery was within the last 1 year before the data collection periods were nominated by a simple random sampling technique. If the participant in the selected household was not available at the time of data collection, three revisits were made to interview the woman, and if the interviewers failed to find the participant after three visits, the next mother was incorporated. One mother was nominated using lottery method when there were two or more participants avail in one household.
Variables
The dependent variable was the utilization of modern contraceptives after childbirth (yes/no), and the independent variables were socio-demographic related characteristics such as the woman’s age, the status of marriage, the status of education, religion, mother occupation, husband’s education, and occupation; reproductive and maternal health service uptake-related factors like the number of children, the interval between birth, discussion about postpartum family planning, contraceptive used previously, ANC, PNC, delivered at the health facility, counseled about family planning, birth attendants, started menstruation, pregnancy plan, fertility desire, resumed sexual intercourse; and knowledge on modern contraceptives.
Operational Definition
Modern contraceptives: “Sterilization (male and female), intrauterine devices, implants, oral contraceptives, condoms (male and female), injectables, and emergency contraceptive pills” (Hubacher & Trussell, 2015).
Postpartum period: “the time from birth up to one year” (Tesfaye et al., 2017).
Postpartum modern contraceptive utilization: “when a woman stated that she used any type of modern contraceptive method by herself or jointly with her husband from data collection time to the last 12 months after birth” (Abraha et al., 2017).
Knowledge of postpartum contraceptives was evaluated by a set of seven questions and finally, it was grouped into good and poor depending on the mean knowledge score as a cutoff point (Tafa & Worku, 2021).
Antenatal care follow-up was defined as “the uptake of any of ANC services provided by skilled health personnel in the health institution” (Abebe et al., 2019).
Sexual intercourse started after delivery was assessed based on self-reported initiation of sexual intercourse and categorized as less than 6 weeks and ≥6 weeks (Demie et al., 2018).
Data Collection Tools and Techniques
The data were taken using an interviewer-administered structured, and pretested questionnaire adapted from other similar research with some contextual modification (Abraha et al., 2017; Belete et al., 2019; Demie et al., 2018; Gebremedhin et al., 2018; Gejo et al., 2019; Nibret Mihretie et al., 2020; Tegegn et al., 2017). To determine its consistency, the questionnaire was initially prepared in English and translated to the local language (Amharic), then back to English by language experts. The data were collected by six health extension workers and supervised by three BSc midwives. Four parts had been incorporated under the questionnaire. The first part addressed the socio-demographic variables. The second part assessed obstetric related issues and mothers’ health service uptake-related information. The third part addressed mothers’ knowledge and current practices regarding postpartum modern contraceptive uptake. The fourth part addressed previous experiences with modern contraception services and sexuality-related issues, for instance, counseled for contraceptives in the last 1 year after delivery, experienced problems with past modern contraceptive uptake, whether menstruation had resumed or not, and whether the participant had resumed sexual activity since the last birth.
Data Quality Assurance
During collection, entry, and analysis, data quality was ensured. Also, to secure the data quality obtained from the research, training was provided to the data collectors and supervisors about the overall data collection procedures, the techniques of interviewing, and how to keep the confidentiality of the information gained from the respondents. Before the actual data collection, on 5% of the sample questionnaire pretest was done in the adjacent district (Chena district) to determine the clarity of the questionnaire, check the wording, and confirm the logical sequence of the questions. Based on the pretest an appropriate modification was made. For the knowledge questionnaire, the Cronbach’s Alpha coefficient was calculated and it was 0.744. Day-to-day on-site supervision during the whole period of data collection was made by the principal investigator and supervisors. The questionnaires’ completeness and accuracy were reviewed and checked by the supervisors and investigators at the end of each day. Then the corrective discussion was undertaken.
Data Analysis
EpiData version 4.2 was used to code the data set and SPSS version 24 software was used for data analysis. To summarize the data, descriptive statistics were calculated. To examine the crude association of each predictor with postpartum contraceptive utilization bivariate analysis was done. Variables having p-values ≤ .25 on bivariate logistic regression analysis were candidates for the multivariable analysis to adjust the effect of confounders. The main assumptions of the logistic regression model (no outliers, multicollinearity, and interaction among independent variables) were checked and fulfilled. Multicollinearity was evaluated using variance inflation factor (VIF) and all independent variables having VIF with a value up to 5 were tolerated. The fitness of the logistic regression model was evaluated using the Hosmer–Lemeshow statistic and it was fitted (p = .24). The presence and strength of association between postnatal modern contraceptive utilization and the factors hindering it were assessed using adjusted odds ratios (AORs) with 95% CIs. Statistically, significant association was determined when the 95% CI of the AOR did not contain 1.
Results
Socio-Demographic Characteristics of the Study Participants
Of the total invited mothers, 385 completed the questionnaires, giving a 96.4% response rate. The respondents’ average age was 27.3 (±4.5 SD) years with the age range of 18 and 42 years. A majority (92.5%) of the respondents were married and rural dwellers (65.5%). Of the participated mothers, 235 (61%) were Orthodox Christian religion followers, and 344 (89.4%) did not attend formal education (Table 1).
Socio-Demographic Characteristics of the Respondents at Bench Sheko Zone, Southwest, Ethiopia, 2021 (n = 385).

Reproductive and Maternal Health Service Uptake-Related Characteristics of the Study Participants
Of the total participants, 162 (42.08%) had only one child and about one-third, 102 (26.5%), had a lapse of 4 to 6 months since their childbirth. The majority of the mothers had four and above antenatal care visits during their last pregnancy, and 270 (74.4%) were informed on contraceptives methods during their antenatal visit. Three hundred eighty-one (99%) of the respondents had delivered at health facility, and 193 (50.1%) counseled on family planning during postnatal care. Regarding the birth interval between the recent and previous birth of the respondents, 167 (43.4%) gave birth for the first time, and 74 (19.2%) had less than 2 years. One hundred nine (42.6%) of the participants’ menses were resumed before 3 months and 288 (95.4%) had started sexual intercourse after 6 weeks, and the rest were commenced before 6 weeks (4.6%) (Table 2).
Reproductive and Maternal Health Service Uptake-Related Characteristics of the Study Participants in Bench Sheko Zone, Southwest Ethiopia, 2021 (n = 385).

Knowledge, and Source of Information About Postpartum Modern Contraceptives
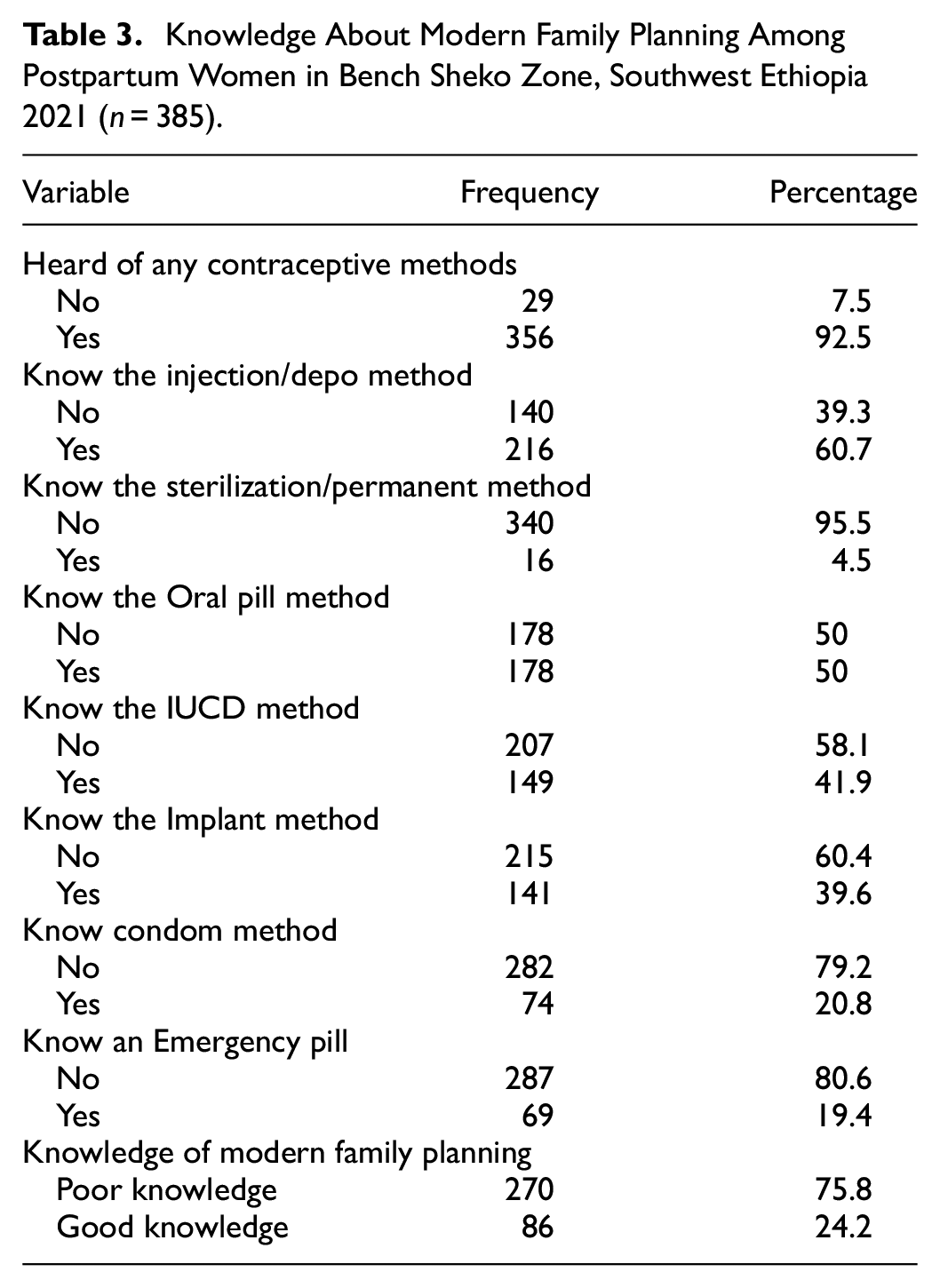
Of the total respondents, 270 (75.8%) had poor knowledge of modern family planning methods. As calculated from the seven knowledge questions, the average of the correctly answered questions was 1.24 (SD ± 0.429). The majority of the respondents (92.5%) heard at least one modern family planning method. Two hundred sixty (60.7%) of the respondents know the Injection/Depo method of contraceptive followed by oral pills (50%), whereas only 16 (4.5%) were informed about permanent methods (Table 3). Of the total respondents who had heard about modern contraceptives, 125 (35.1%) had got information from health facilities, 99 (27.8%) from mass media, 50 (14%) from health extension workers, 38 (10.7%) from friends, and 37 (10.4%) from family.
Knowledge About Modern Family Planning Among Postpartum Women in Bench Sheko Zone, Southwest Ethiopia 2021 (n = 385).
Modern Contraceptive Methods Utilization During the Postpartum Period
In this study, the magnitude of utilization of modern contraceptive among mothers in period of postpartum was 50.4% (95% CI: 45.3, 55.3) (Figure 1). The most preferable method to be used was injectable 87 (44.8%) followed by oral pills 52 (26.8%), implant 45 (23.2%), and IUCD 7 (3.6%) respectively. Of the total respondents who didn’t currently use it, the main reasons for not using it were fear of side effects 43 (22.5%) followed by fear of change in breast milk 39 (20.4%), partner opposed to using family planning 35 (18.5%), want to have another child soon 31 (16.2%), due to amenorrhea feeling of not prone to the risk of pregnancy 24 (12.6%), and thinking of not prone to the risk of pregnancy due to breastfeeding18 (9.4%).

Utilization of postpartum modern contraceptives in Benchi Sheko Zone, Southwest, Ethiopia, 2021 (n = 385).
Associated Factors of Postpartum Modern Contraceptives Utilization
Maternal education, having information about postpartum contraceptives, counseled toward postpartum contraceptives by the time of ANC, history of contraceptive uptake before current birth, counseled toward postnatal contraceptives during PNC, and timing of sexual intercourse resumption were significantly associated with utilization of contraceptive during the period of postpartum on multivariable logistic regression analysis at p-value < .05 and 95% CI (Table 4).
Bivariate and Multivariable Analysis of the Utilization of Modern Contraceptives During the Postpartum Period With its Predictor Variables in Bench Sheko Zone, Southeast Ethiopia, 2021 (n = 385).
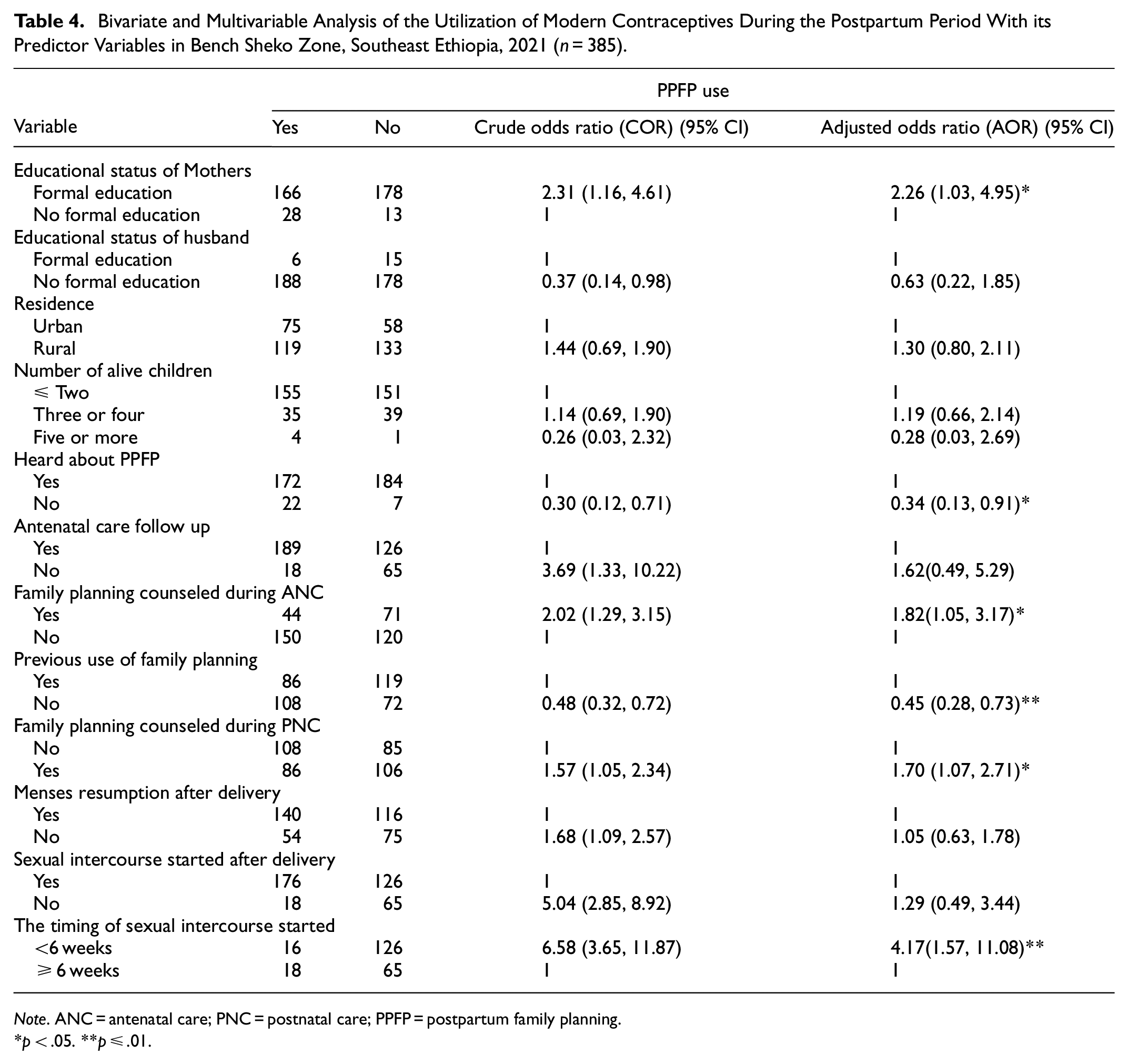
Note. ANC = antenatal care; PNC = postnatal care; PPFP = postpartum family planning.
p < .05. **p ≤ .01.
Mothers who did attend formal education were more likely to utilize modern contraceptives during the period of puerperium than their counterparts (AOR = 2.26, 95% CI; 1.03, 4.95). Mothers who haven’t had information about contraceptives were 66% less likely to utilize postpartum modern family planning than mothers who have had information (AOR = 0.34, 95% CI; 0.13, 0.91). Mothers who have had contraceptive counseling during ANC were two times higher to uptake modern family planning in the period of postpartum as compared to those who haven’t had (AOR = 1.82, 95% CI: 1.05, 3.17). The odds of utilizing modern contraceptives among postpartum mothers who have had a history of family planning uptake before current birth were 55% more likely as compared to those who haven’t had (AOR = 0.45, 95% CI: 0.28, 0.73). Women who have had counseling on contraceptives during PNC were more likely to use modern contraceptives during the period of postpartum than those who did not (AOR = 1.70, 95% CI: 1.07, 2.71). Mothers who started sexual intercourse less than 6 weeks after recent birth were more likely to uptake contraceptives than those who started ≥6 weeks (AOR = 4.17, 95% CI: 1.57, 11.08).
Discussion
Even though postpartum contraceptives uptake plays a vital role in meeting the unmet need of family planning and attaining optimally spaced births, till the uptake is poor. In this study, the prevalence of the utilization of contraceptives during the period of postpartum was 50.4% (95% CI: 45.3–55.3). The result was consistent with studies investigated in Ethiopia, for instance, the South Gondar (54.7%) (Nibret Mihretie et al., 2020), Gondar town (45.8%) (Abera et al., 2015), and Aksum (48%) (Abraha et al., 2017). It was also supported with researches done in Kenya (46%) (Mai & David, 2013), and Mexico (47%) (Ringheim et al., 2007). However, the finding of the study was higher than studies done in Arba Minch (44%) (Wassihun et al., 2021), Debre Birehan town (41.6%) (Demie et al., 2018), Arsi Zone (17.46%) (Jima & Nemo, 2020), Dabat (10.3%) (Mengesha et al., 2015), Lode Hetosa District (15%) (Jima & Garbaba, 2020), Somalia region (12.3%) (Nigussie et al., 2016), Nepal(32.8%) (Joshi et al., 2020), and Uganda (28%) (Rutaremwa et al., 2015). The potential difference could be due to the gaps in the period of the studies, study location, and the investigation of some misconfigured socio-economic, reproductive, and service uptake characteristics among participants.
On the other hand, the uptake of modern postpartum contraceptives in the study was lower than in findings reported in Ethiopia like Debre Tabor town (63%) (Taye et al., 2019), Hossana town (72.9%) (Gejo et al., 2019), and Addis Ababa (80.3%) (Gebremedhin et al., 2018). It was also lower than findings reported in Malawi (75%) (Kopp et al., 2017) and South Africa (89.0%) (Crede et al., 2010). This difference could be due to the discrepancy in the socio-demographic manifestation of the participants, studies period gaps, and the study populations; in which all of the participants in the previous studies were urban resident whereas 65.5% of the mothers who participated in our study were rural dwellers. So, the higher utilization of postpartum family planning found in the previous studies might be explained by mothers who were from the town who have better availability to the health institution, and are easily exposed to media outlets to be familiarized with the merit of up taking of contraceptives during the puerperium and its related health outcomes both for the mother and her child than mothers in a rural area. Furthermore, the difference might be due to partner active engagement in urban areas than with rural areas.
Our study revealed that mothers who attended formal education were more likely to uptake modern contraceptives as compared to their counterparts during the period of postpartum. The result was in agreement with studies done in Gondar (Nibret Mihretie et al., 2020), and Uganda (Rutaremwa et al., 2015). This could be justified by educated mothers are more likely to have good knowledge and better ability to decide on uptake of contraceptives and other reproductive health services during the period of postpartum. It might also be due to educated mothers gathering evidence toward the benefit of uptake of postpartum family planning from broachers, printed materials, and social Medias.
In this study, mothers who haven’t had information about postpartum family planning were 66% lower to uptake of contraceptives than women who have had information. The result was consistent with a research done in Addis Ababa (Tafa & Worku, 2021). This could be because mothers who had information about the benefits of uptake of postnatal family planning have better knowledge, and are motivated to utilize it.
Mothers who have had postpartum contraceptives counseling during ANC follow-up were higher odds of using family planning during the period of postpartum compared to those who haven’t had it. This was supported with findings of researches done in Ethiopia; Arsi Zone (Jima & Nemo, 2020), Injibara town (Belete et al., 2019), and Axum town (Abraha et al., 2017). The possible explanation could be that mothers who were counseled on contraceptive used during the period of puerperium during antenatal care have a better scope of understanding of the benefits of using postnatal modern contraceptives, the appropriate time when to start postpartum contraceptives, and will be encouraged to utilize them.
Mothers who had history of contraceptives use before current birth were 55% higher odds of utilizing modern contraceptive during the period of postpartum as compared to those who didn’t. The result was consistent with studies done in Addis Ababa (Gebremedhin et al., 2018), and Debre Tabor town (Taye et al., 2019). This could be due to mothers who had history of previous uptake of contraceptives have better knowledge, and experience on the different choices of the methods along with the cons and pros that will enhance their decision-making ability toward postpartum contraceptives utilization.
Mothers who have had counseling on contraceptives during the postnatal care were higher odds of using modern contraceptives in the period of postpartum than those who did not. This was supported by research findings reported in Addis Ababa (Tafa & Worku, 2021), Gondar town (Abera et al., 2015), and Axum town (Abraha et al., 2017). This might be justified by mothers who take maternal and newborn health services (i.e., postnatal care, delivery at health facility, and immunization) are a better opportunity to uptake postpartum family planning services during the period of postpartum, or they have more chances to be convinced to utilize, provided with a method, and reduces missed opportunities.
Consistent with a study done in Debre Berhan town (Demie et al., 2018), women who started sexual intercourse within the first 6 weeks after recent birth were higher odds of utilizing modern contraceptives during the period of postpartum than those who started sexual intercourse ≥6 weeks. This is likely because mothers who started sexual intercourse early may consider themself as they are at risk of having pregnant, and promoted to use of family planning promptly.
Despite the high rate of a skilled birth attendant (99%) and PNC (96.6%) noted in our finding, only three-fourths (74.4%), and a half (50.1%) of the mothers were counseled on PPFP during their ANC and PNC, respectively. This shows that there was a discontinuity in the continuum of care, and leads to a missed opportunity as the ANC, childbirth, and early PNC services are an entry point where mothers are supposed to get counseling on postnatal family planning.
Limitation of the Study
Our research found pertinent findings that have paramount merits for the postpartum modern family planning strategies and programs. As a limitation, owing to the cross-sectional nature of the study, the exact cause-effect correlation between uptake of modern contraceptives and major factors associated with it doesn’t exist and recall bias might be introduced.
Conclusion and Recommendation
The result of the study depicted that the magnitude of utilization of contraceptive during the period of postpartum was low as compared to others’ studies. Maternal education, having information about postpartum family planning, counseling toward family planning during ANC, previous family planning utilization, counseling toward family planning during PNC, and time to sexual intercourse resumption after delivery were the major factors associated with uptake of postnatal contraceptives. Therefore, enhancing female education and providing modern contraceptives during maternal and child health services units should be strengthened to maximize contraceptive uptake during the period of postpartum in Southwest Ethiopia. Mothers would be addressed during antenatal care, postnatal, immunization units, mother group meetings, and during home observations via health extension workers. In addition, continuous community-based counseling and interventions which encourage the active participation of husbands, religious leaders, and elderly people would be developed by healthcare providers and policy-makers. Moreover, further qualitative study will be done to identify problems related to institutions, health care providers, and male partners, influencing the uptake of contraception during the period of postpartum.
Footnotes
Acknowledgements
We would like to address our gratitude to our colleagues for the effort they made to enrich our research with important guide and input. We are thankful to our data collectors, supervisors, and study participants. Bench Sheko Zone Health Offices staff help us by providing preliminary information and sharing valuable data when needed which lay a base for the finalization of this research finding.
Author Contributions
GF was involved in the conception and design of the study. All authors (GF, MS, DG, AA, and YN) contributed to the execution, acquisition of data, analysis, interpretation of the result, and drafting of the article. All authors participated fully in revising the article, have agreed on the journal to which the article will be sent for publication, gave final approval of the version to be published, and agreed to take responsibility for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board at the College of Medicine and Health Sciences of Mizan Tepi University before commencing data collection. An official letter of permission was obtained from the Department of Midwifery to the Zonal administration authorities. Informed written permission was also obtained from the district administrative authorities. Informed consent for more than 18 years old and assent for less than18 years from their family was obtained from each study participant after explaining the objectives, risks/benefits, rights, confidentiality, nature of the study, and the scope of their involvement in the study. To keep confidentiality, the names of respondents were substituted by code numbers.
Consent for Publication
This is not applicable.
Statement of Data Availability
The datasets generated for the current study are available from the corresponding author upon reasonable request via Email.