
Abstract
COVID-19, which has become a worldwide pandemic, prompted various healthcare organizations to take measures to stop or slow its spread. These measures require behavioral change. According to the health belief model, knowledge and awareness are needed to establish an assessment of threat and determine whether a behavior will be changed. Since the situation is related to a viral infection, it is expected that people with health backgrounds will have more knowledge and awareness about COVID-19. This study aims to compare the levels of COVID-19 knowledge and awareness of faculty, staff, and students in health sciences and non-health sciences disciplines at an all-female college in Dubai. This will help anticipate the risk for individuals, and predict compliance with regulations. A cross-sectional study was conducted using a self-administered online questionnaire. The results were analyzed using chi-square or Fisher’s exact test. Participants’ knowledge and awareness regarding contagiousness, transmission, incubation period, recovery and mortality rate, susceptibility of elderly people, and the stay-at-home policy were generally high, regardless of their background. This high level of knowledge could be attributed to the rapid dissemination of information through social media. Participants from the health sciences were significantly more knowledgeable about certain preventive measures, the causative pathogen, and its transmission through animals (p < .05). Overall, there was a high level of knowledge and awareness among the participants, regardless of their background, yet there are some areas that needs enhancement. Assessing knowledge and awareness is important for ensuring that people understand and change their behavior to mitigate its spread.
Background
The novel coronavirus SARS-CoV-2 was first identified in December 2019 in Wuhan, China, resulting in the outbreak of a respiratory illness known as COVID-19. In general, coronaviruses can cause several respiratory infections in humans, ranging from a common cold to more severe diseases, such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS; Raoult et al., 2020). According to the World Health Organization (WHO), fever, fatigue, and dry cough are the most common symptoms of COVID-19 (Coronavirus Disease Pandemic—WHO, 2020a; COVID-19 Situation Reports—WHO, 2020b; Disease Background of COVID-19—ECDC, 2020). More serious symptoms might also emerge, such as difficulties in breathing or shortness of breath, chest pain, and loss of speech or movement, which require immediate medical intervention (Coronavirus Disease Pandemic—WHO, 2020a; COVID-19 Situation Reports—WHO, 2020b; Disease Background of COVID-19—ECDC, 2020). The virus is transmitted rapidly, resulting in an exponential increase in the number of cases worldwide (Gates, 2020). There is strong evidence suggesting that it can be transmitted by people with mild symptoms, or during the incubation period before symptoms are shown (Bi et al., 2020). Hence, COVID-19 is more difficult to contain than MERS or SARS (Gates, 2020).
Awareness plays a pivotal role in preventing and controlling infection, and the behavior of individuals influences the spread of infectious agents (Liu et al., 2013). Most strategies and measures recommended by authorities are, in essence, behavioral acts (e.g., wearing masks and physical distancing; Burns, 1992). For this reason, the health belief model (HBM) was used to scaffold this study. The HBM suggests that the threat of an illness combined with a belief in the effectiveness of the recommended behavior—in this case, preventive measures—predicts the likelihood of adopting a certain behavior (Figure 1; Becker, 1974; Hayden, 2009). The likelihood of adopting a certain behavior is based on an individual assessment of threat, which involves evaluating the likelihood of getting the disease and its severity (Becker, 1974; Hayden, 2009). In addition, individual factors (e.g., age, gender, ethnicity, socioeconomic status, knowledge, and awareness), cues of action, and the benefits and feasibility of adopting a behavior help to predict whether preventive measures will be adopted (Becker, 1974; Hayden, 2009). Knowledge and awareness related to all constructs in HBM (Figure 1) help individuals carry out an assessment, which results in either adopting a new behavior or not (Becker, 1974; Glanz & Bishop, 2010; Hayden, 2009; Rosenstock, 1974; Singer & Benatar, 2001).

The health belief model (Becker, 1974; Hayden, 2009).
In the context of this research, the new behavior refers to compliance with regulations (e.g., wearing personal protective equipment, maintaining physical distancing, and obeying lockdown mandates; Becker, 1974; Glanz & Bishop, 2010; Hayden, 2009; Rosenstock, 1974; Singer & Benatar, 2001). Since the topic of study is a viral infection, it is expected that people with health backgrounds will have more knowledge and awareness about COVID-19, and that their assessment and compliance with regulations will differ.
Therefore, this study aims to compare the levels of COVID-19 knowledge and awareness reported by faculty, staff, and students in health sciences and non-health sciences at all-female college in Dubai. The hypothesis is that there is a difference in the level of knowledge and awareness of COVID-19 between participants with a health sciences (HS) background and those without a health sciences (non-HS) background, which will consequently be seen in their adoption of preventive measures.
Methodology
Study Design
This research is a cross-sectional study conducted at an academic institution (females college) in Dubai. It utilized an electronic questionnaire designed in accordance with the CHERRIES checklist, as described in this section (Eysenbach, 2004).
Data Collection
A self-administered electronic questionnaire (19 items) was used as a data collection tool. It was administered over a period of 2 weeks between the end of March and the beginning of April 2020, during the first 2 weeks of online/virtual classes. To participate, the participants had to consent electronically, which they confirmed by clicking “Start the Survey.” The questionnaire was designed using HBM to assess participants’ knowledge and awareness, which was expected to affect their assessment of threat and danger and, consequently, compliance with regulations (Figure 1). The following information was gathered during the survey:
- Demographics
- Sources of information
- Medical knowledge of COVID-19
- Knowledge of transmission modes
- Knowledge of protection methods
- Knowledge of treatment, recovery, and prognosis
Sample
- Recruitment
Convenience sampling was used, and participants were approached in two ways.
(a) Electronic invitations were sent via email containing a direct link to the questionnaire and a quick response (QR) code that could be scanned using a cell phone camera, directing participants immediately to the questionnaire.
(b) During virtual lectures, instructors in different programs and departments displayed the QR code at the beginning of the session for students to scan and proceed to the questionnaire.
Participation was entirely voluntary, and participants were informed that they could withdraw at any time.
Characteristics
Participants had to meet the following inclusion criteria to be eligible to participate: adults of any gender aged 18 or older, with at least a high school education, in any specialty, program, or department. They had to be either studying or working at all-female college in Dubai, and consent electronically to be eligible for participation and access the survey.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for Social Science (SPSS) software program for Windows (version 26.0). Frequencies and percentages are described. Hypothesis testing was completed using either chi-square or Fisher’s exact test for categorical data to compare the differences. The significance level was set at p < .05, and anything above this was considered not significant.
Ethical Approval
This study was approved by the Institutional Research Committee of the Higher Colleges of Technology, and electronic consent forms were obtained from the participants before they answered the questionnaire. The consent form incorporated information about the study aim, protection of anonymity, and usage of data. This study was conducted according to the Declaration of Helsinki.
Results
Participants’ Demographics
A total of 212 participants answered the electronic questionnaire. The majority of respondents were female (84%). Most of the respondents were 30 years old or younger (71.5%), and more than half reported high school as their highest educational attainment (53.3%). Participants from more than seven different divisions or programs participated, as shown in Table 1.
Demographics.

Sources of Information
When participants were asked about the source from which they obtained COVID-19-related information, they were able to choose one or more options. Most participants obtained their information from social media (n = 172; 81%), followed by other media channels, including TV, radio, and newspapers (n = 145; 68%). Family, college, and friends were also found to be important sources for 53%, 49%, and 48% of participants, respectively (Figure 2).

Sources of information.
General Knowledge About COVID-19
Source of pathogen
About 68% of participants (n = 144) correctly identified the causative pathogen as a virus. A significantly higher percentage of HS participants answered correctly (p < .05), with 79% selecting this answer, compared to 63% of the non-HS respondents (Figure 3). Hence, this hypothesis was supported.
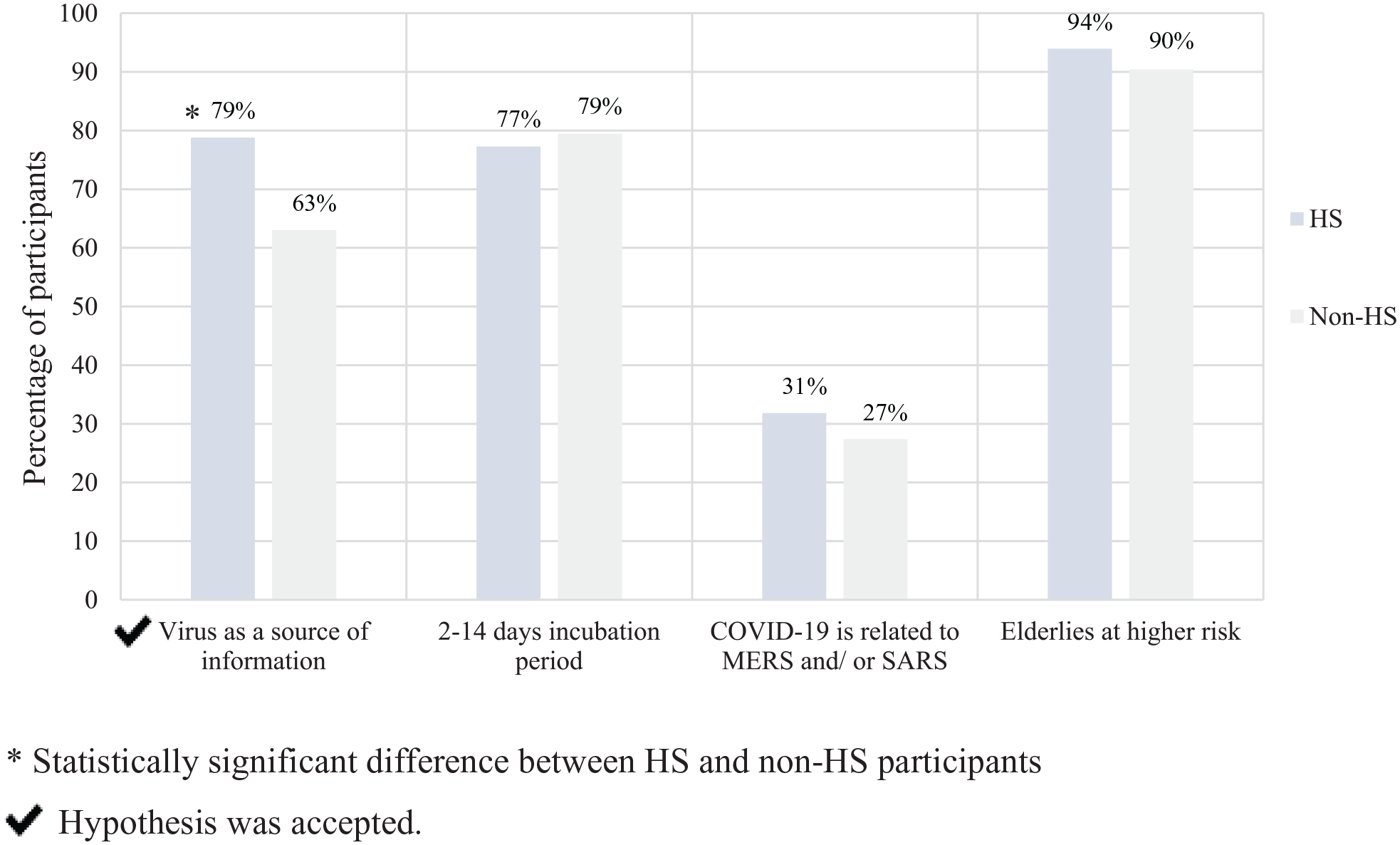
General knowledge of COVID-193.3.2 incubation period.
Most participants (n = 144; 79%) correctly identified the duration of virus incubation (2–14 days). Their knowledge was consistently high in both subgroups (77% in HS and 80% in non-HS), and this minor difference was statistically insignificant, as shown in Figure 3. Therefore, the null hypothesis was accepted.
Symptoms
About 95% of the participants (n = 201) correctly responded that COVID-19 symptoms were similar to those of a common cold. The difference between the subgroups was minor and statistically insignificant (96% in HS and 95% in non-HS); therefore, the null hypothesis was accepted.
Is the causative agent of COVID-19 the same as the one causing MERS or SARS?
About 71% of the participants (n = 151) responded correctly that the causative agent of COVID-19 was different from MERS or SARS. It was found that 69% of the HS participants and 73% of the non-HS participants answered this incorrectly. As the difference was not found to be statistically significant, the null hypothesis was accepted.
The elderly and their susceptibility to COVID-19 infection
Most of the participants (n = 194; 92%), irrespective of their backgrounds, responded that elderly people were at a higher risk of getting infected with COVID-19, including 94% of HS and 90% of non-HS participants. The difference was not found to be statistically significant; hence, the null hypothesis was accepted.
Knowledge About Transmission of COVID-19
Is COVID-19 highly contagious?
Irrespective of participants’ backgrounds, the majority (90%) were aware that COVID-19 was highly contagious. There were no statistically significant differences between the groups, so the null hypothesis was accepted.
Transmission routes/modes
Most participants responded that contaminated surfaces (67%), droplets of saliva or discharge from the nose (60%), infected family members (66%), and patients (52%) were major sources of transmission for COVID-19. Both groups correctly identified almost all the transmission routes, with no statistically significant differences between their responses, as shown in Figure 4. Therefore, the null hypothesis was accepted for all except the question related to animals. HS participants identified animals as a potential transmission route more often than non-HS participants; therefore, demonstrating significantly (p < .05) stronger knowledge regarding animals as a route of transmission (27%) than non-HS participants (13%). For this item, the hypothesis was accepted.

General knowledge about transmission of COVID-19.
Global risk assessment of COVID-19
About 88% of the participants (n = 187) correctly identified that the global risk assessment declared by the WHO for COVID-19 was “very high” (89% HS, 88% non-HS). The difference was not found to be statistically insignificant, and accordingly, the null hypothesis was accepted.
General Knowledge About Protection Methods Against COVID-19
Protection methods
The overall knowledge of participants regarding protection methods was generally high, with 78% correctly identifying the protective and precautionary measures recommended by the WHO. In general, 88% agreed with washing hands thoroughly with soap and water and 81% identified the importance of avoiding contact with anyone who was sick. Overall, 75% believed that they should wear masks for protection and cover the nose and mouth when coughing or sneezing. Social distancing, avoiding handshakes and hugs, and avoiding touching the face were also indicated by most participants (73%, 75%, and 72%, respectively). Only 6% were unsure about the protective measures (Figure 5).

General knowledge about the protection methods against COVID-19.
The analysis of subgroups results showed that there was significantly higher knowledge and awareness among HS participants regarding the protection methods overall (p < .05). Therefore, the hypothesis was accepted. For two specific items, the differences between the subgroups were not statistically significant: avoiding touching commonly used objects (73% in HS and 62% in non-HS) and avoiding handshakes and hugs (77% in HS and 75% in non-HS). For these, the null hypothesis was accepted.
Stay-at-home policy
The results showed a very high awareness level (97%) regarding the “stay-at-home” policy to minimize public gathering as a protective measure, with no statistically significant difference between groups. Here, the null hypothesis was accepted.
Knowledge About the Treatment, Recovery, and Prognosis of COVID-19
COVID-19 recovery rates
Most participants (88%) believed that many people who had been infected or diagnosed with COVID-19 had recovered or were recovering. The difference between HS and non-HS participants was not statistically significant, which led to acceptance of the null hypothesis (Figure 6).

Knowledge about the treatment, recovery, and prognosis of COVID-19.
COVID-19 mortality rates
Although the participants’ knowledge about mortality rates was high, only about one-third of the participants (n = 82; 39%) identified that the mortality rate of COVID-19 was 2–5%, as shown in Figure 3. More non-HS participants were aware of the mortality rate (35% in the HS group and 56% in the non-HS group), although the difference was not found to be statistically significant. Accordingly, the null hypothesis was accepted.
Does the influenza vaccine protect against COVID-19?
Overall, the majority (n = 184; 87%) were aware that the influenza vaccine did not protect against COVID-19. The difference in knowledge between the subgroups (14% in HS and 13% in non-HS) was not statistically significant, so the null hypothesis was accepted.
Discussion
In general, the findings revealed that there was a high level of knowledge and awareness among participants, regardless of their background, with some exceptions. To the best of our knowledge, this is the first study conducted in the United Arab Emirates to compare the COVID-19 knowledge and awareness of those with HS and non-HS backgrounds. HBM was used for the first time to guide a study targeting knowledge and awareness about COVID-19, and to analyze the findings through the lens of the model (Figure 7). The items that were used in the survey were added to the model within the construct to which they belonged. As per the HBM model, knowledge and awareness are crucial for people’s ability to undertake an appropriate assessment of threat susceptibility and severity, and for weighing the benefits against the barriers. This assessment ultimately leads or does not lead to behavioral change and compliance with regulations (e.g., wearing personal protective equipment, maintaining physical distancing, or obeying lockdown mandates; Becker, 1974; Glanz & Bishop, 2010; Hayden, 2009; Rosenstock, 1974; Singer & Benatar, 2001).
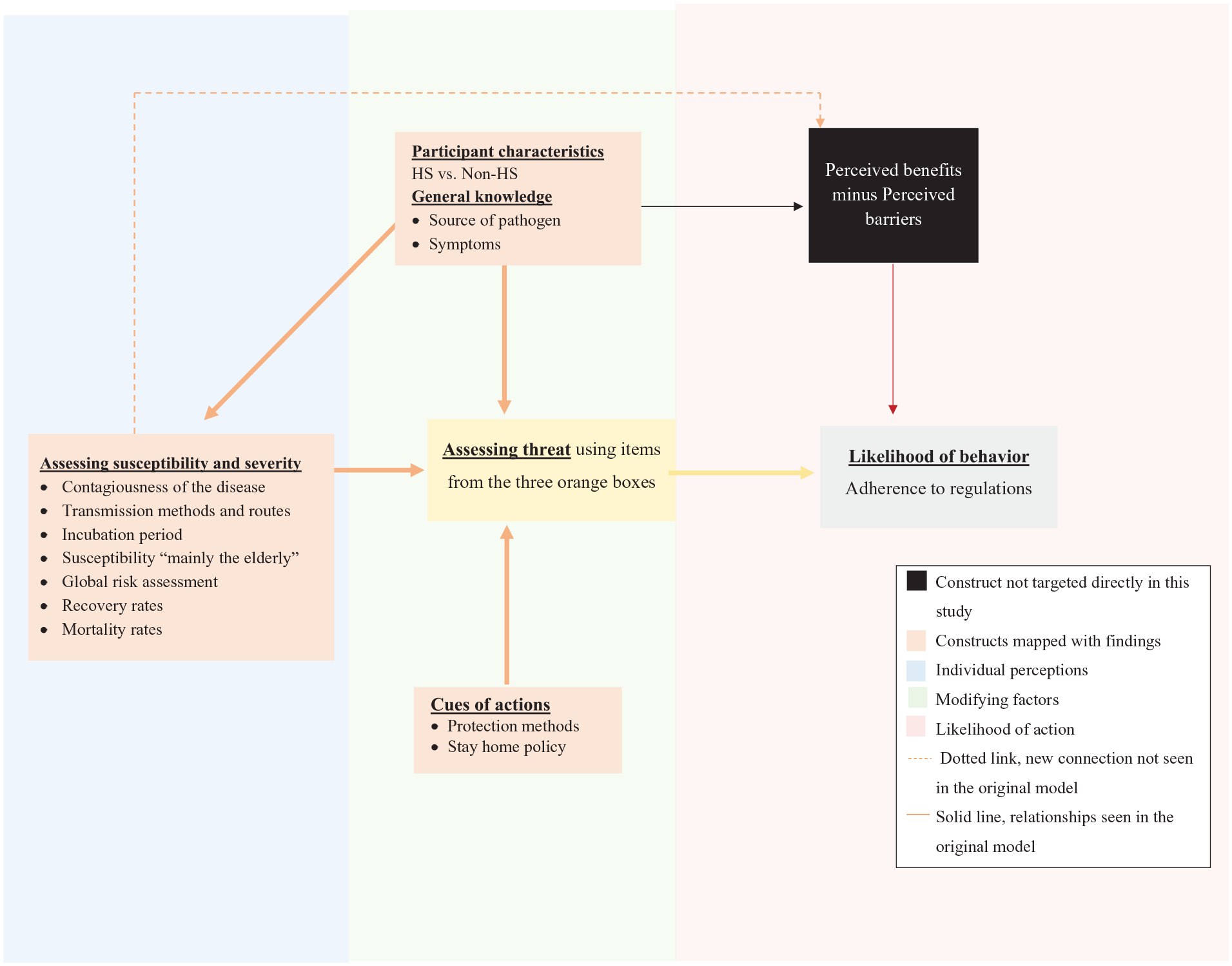
Findings mapped with HBM.
Since knowledge and awareness are cornerstones of HBM, the sources of participants’ information were explored. Social media platforms were found to be the most popular sources of information about COVID-19. In fact, social media was flooded with information about COVID-19, and was considered to be the most convenient source of information, rendering it favorable for participants (Hernández-García & Giménez-Júlvez, 2020; Olum et al., 2020; Rosenberg et al., 2020; Rovetta & Bhagavathula, 2020). Similar findings have been reported in previous studies, including one conducted in medical schools in Uganda (Olum et al., 2020), another in Iraqi Kurdistan (Ahmad & Murad, 2020), and a Saudi Arabian study related to the Zika virus (Ibrahim et al., 2018). Although social media provides an opportunity to communicate health information directly to the public, the danger of disseminating inaccurate information is high (Cuan-Baltazar et al., 2020; Hernández-García & Giménez-Júlvez, 2020; Rovetta & Bhagavathula, 2020). This can increase the chance of incorrect assessments of risk. The following section discusses the accuracy of information and knowledge of participants.
The results of this study revealed that the HS participants had more accurate knowledge regarding the causative pathogen than the non-HS participants. This is in line with the findings of studies targeting medical students in Jordan (Khasawneh et al., 2020), Uganda (Gao et al., 2020), and China (Geldsetzer, 2020), in which they demonstrated accurate knowledge and deep understanding. Similarly, a study on the Zika virus confirmed that having a health sciences education resulted in more extensive knowledge about Zika (Argüelles-Nava et al., 2018). However, one study of Nigerian undergraduate dental students found that their knowledge regarding the causative pathogen was not as strong, with 40% answering questions incorrectly (Umeizudike et al., 2020). Having accurate information about the causative pathogen, as per the HBM, could help participants assess threat, especially in terms of understanding the rapid nature of viral transmission.
When the participants in this study were asked about the incubation period, symptoms, differences with MERS-CoV and SARS, and susceptibility of elderly people, their knowledge and awareness were high regardless of their background. This could be due to the accessibility of information. Similar findings have been observed among Chinese medical and non-medical students, whose knowledge about risk perception, symptoms, transmission routes, and susceptibility of the elderly was found to be very good (Geldsetzer, 2020). The findings of two other studies conducted with the general public also found that their knowledge about COVID-19 symptoms and susceptibility was relatively strong (Kebede et al., 2020; Olapegba et al., 2020). This is beneficial in helping people carry out accurate risk assessments, leading to likely compliance with regulations. This is not limited to medical professionals; extensive public knowledge of COVID-19 is essential for improving public compliance (Figure 7). It must be noted here, however, that focusing on the elderly as the only susceptible population may lead people from other age groups to assume that they are at a lower risk, potentially reducing their compliance with regulations.
The knowledge and awareness of participants from both subgroups about contagiousness, transmission methods, infection sources, treatment, recovery, and fatality rates were generally moderate to high (above 50%). With a closer examination of the findings, although participants’ awareness of global risk and contagiousness of COVID-19 was high (≥85%), they were less aware that transmission could occur through family members, healthcare professionals, contaminated surfaces, droplets, and animals. People who are less aware are more likely to carry out an assessment that results in incorrectly perceiving minimal threat and susceptibility.
Overall, our findings of moderate-to-high levels of knowledge and awareness regarding transmission and contagiousness are in line with the literature (Geldsetzer, 2020; Kebede et al., 2020; Olapegba et al., 2020). A good understanding of disease contagiousness, transmission methods, infection sources, treatment, fatality rates, and the high global risk assessment should result in accurate perceptions of COVID-19 as a threat, which is expected to result in a moderate-to-high likelihood of compliance with regulations.
HS participants demonstrated more knowledge about most of the protective methods and techniques, apart from avoiding handshakes and contact with common surfaces. However, in two other studies, the public was found to be well aware of the most common protective techniques (Balkhy et al., 2010; Kebede et al., 2020). This could be attributed to the nature of the pandemic in comparison to other epidemics (Argüelles-Nava et al., 2018; Centers for Disease Control and Prevention [CDC], 2020). In the case of COVID-19, information about precautionary measures was made highly available to the public via different platforms, including global regulations that affected everyone. As per the HBM, awareness of protective techniques means that the cues of actions are also optimized, which may result in greater compliance with regulations among groups with greater knowledge. If participants erroneously believe that COVID-19 is associated with a high recovery rate, this might undermine threat assessment and consequently affect behavior in terms of protective techniques.
Crowded places should be avoided (Kebede et al., 2020; Olapegba et al., 2020), and participants in this study demonstrated strong awareness of the physical distancing (stay-at-home) policy. This policy was enforced by lockdowns, with closure of almost all public areas and amenities except for supermarkets, pharmacies, and hospitals, as well as implementation of working from home arrangements and distance learning. In this case, the government and health authorities assessed the threat and enforced physical distancing through these regulations. Most participants in both groups were aware that other vaccines, such as the influenza vaccine, did not provide protection against COVID-19. Although this information is correct, it might also result in people not receiving the influenza vaccine, which is recommended by authorities (Novel Coronavirus—Ministry of Health and Prevention, 2020).
In general, a high level of knowledge and awareness of COVID-19 was demonstrated by most participants. Social media has helped with the dissemination of information. This awareness could be linked to the nature of the global pandemic, with health organizations and governments around the world launching programs to educate people about safety measures and minimizing transmission (Jager et al., 2017). In the UAE, the Ministry of Health and Prevention (MoHP) conducted a series of virtual campaigns through its website and social media to enlighten the public about preventive actions in an attempt to control and minimize the spread of COVID-19. MoHP and other health authorities hosted virtual conferences and workshops to raise public awareness, and updates regarding COVID-19 were a standing item in the daily news.
In the college studied in this paper, two practices were implemented: distance learning and working from home. COVID-19 protection guidelines were shared with all students and staff, which contributed to heightening their knowledge and awareness, and consequently improving their adherence to regulations. Certain actions or behaviors were enforced, such as physical distancing and protective measures, which may be helpful in demonstrating the seriousness of the threat.
In addition, as seen in Figure 7, while assessing susceptibility and severity, participants also weighed the benefits, risks, and barriers related to a course of action or behavior. In other words, if the perceived benefit is lower than the barriers and risks, people may be less compliant. This was seen in our study when participants labeled the elderly as the most susceptible, which could downplay the risk of COVID-19 in other age groups. Individuals who do not live with elderly people may perceive a lower threat than those who live with elderly people and care for them.
Limitations
This study is not without limitations, including the study location being an all-female campus. The majority of participants recruited were Emirati females, which might hinder the generalizability of the findings. However, given the restrictions imposed during the lockdown, this was the most convenient and feasible location for the researchers, who worked on this campus. Another limitation was the convenience sampling recruitment technique. As the name implies, participants were included because they happened to be present at the time of recruitment during lectures or received their emails (Denscombe, 2010). Hence, there was a risk of unintentionally excluding potential participants who were not present during the recruitment phase. The decision to use convenience sampling was due to feasibility, and this method of recruitment has been used in previous studies of knowledge and awareness (e.g., AlMohaissen, 2017; CDC, 2020; Denscombe, 2010). Additionally, there was less participation from staff than students, which could be attributed to the fact that the questionnaire was administered at the beginning of the transition to online education when academics and staff were under tremendous pressure.
Conclusion
Our findings suggest that there is a high level of knowledge and awareness about COVID-19, irrespective of people’s backgrounds. Given that the pandemic has affected everyone directly, this was to be expected. There were some areas in which those with a health sciences background had more knowledge than those without, and other areas in which knowledge was found to be low for both groups. This should be addressed through awareness campaigns, as knowledge is important for informing an appropriate assessment of threat and adherence to guidelines that help contain the virus. Furthermore, governments should develop strategies to mitigate these concerns, and health authorities need a more proactive and agile public health presence on social media to combat the dissemination of inaccurate information. This study can serve as a reference point for future education and public awareness programs, whether for COVID-19 or other conditions. It can also inform researchers about the usefulness of theories and conceptual frameworks to guide and analyze findings of observational quantitative studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.