
Abstract
Young people, as a group, are not strongly incentivised to vaccinate against COVID-19, given how the disease affects them. To discover the factors which help increase people’s intention to take the COVID-19 vaccine, using a variety of dimensions to measure Knowledge (K), Trust (T), the Health Belief Model (HBM), and the Theory of Planned Behaviour (TPB) in Spanish university students as a collective. We analysed the proposed models using multiple-regression analysis, incorporating the variables of the constructs in a hierarchical manner, introducing them in the following order: TPB, K, T. HBM was excluded, given that no significant statistical relationship was found. The data used for the study are drawn from an anonymous questionnaire put to 3,542 students at the University of Salamanca (Spain). Our model accounts for 43.1% of the variance in vaccination intention. Neither severity nor susceptibility, which are fundamental constructs in the health belief model, have an impact on vaccination intention for this group of people. The Theory of Planned Behaviour accounts for 32.1% of the variance. Interesting mediating effects are discovered, indicating that knowledge lowers levels of trust in the Government, but increases trust in scientific experts. Both types of trust have a positive impact on vaccination intention. Messages based on the risk of contracting the disease do not appear to be effective incentives for this group of people to take up the vaccine. Information campaigns need to be transparent and rigorous. This does not mean that they need to go into great depth on a technical level; however, it is advisable that the information come from trustworthy scientific experts.
Plain language summary
Young people, as a group, are not strongly incentivised to vaccinate against COVID-19, given how the disease affects them. Thus, the object of this study is to analyse which factors are predictors of vaccination intention in this group of people, with particular emphasis on knowledge of the vaccination process, and trust in the scientific experts and in the Government. Our objective was to discover the factors which help increase people’s intention to take the COVID-19 vaccine, using a variety of dimensions to measure Knowledge (K), Trust (T), the Health Belief Model (HBM), and the Theory of Planned Behaviour (TPB) in Spanish university students as a collective. We analysed the proposed models using multiple-regression analysis, incorporating the variables of the constructs in a hierarchical manner, introducing them in the following order: TPB, K, T. Our study concluded that messages based on the risk of contracting the disease do not appear to be effective incentives for this group of people to take up the vaccine. Information campaigns need to be transparent and rigorous. This does not mean that they need to go into great depth on a technical level; however, it is advisable that the information come from trustworthy scientific experts.
Keywords
Introduction
It has been over 2 years since the WHO declared COVID-19 a pandemic, and still, we have not managed to eradicate the disease. Over the coming months, a fourth dose of the COVID-19 vaccine will be given to over-60s, as a majority of experts are predicting a new COVID-19 wave this autumn (European Commission, 2022). The emergence of the Khosta-2 virus, which has similarities to SARS-CoV-2 (Seifert et al., 2022), has led researchers to turn their attention to creating a universal vaccine, which defends against coronaviruses as a whole family. Therefore, knowledge about vaccine uptake remains vitally important. Vaccination statistics in Spain are rather good: 90.8% of the population over 5 years old has had at least one dose; 89.4% have been fully vaccinated, but this drops to 54.7% in relation to booster doses. In the last group, the percentage of people having received three doses of the vaccine, in the 20 to 29 age range, is 43%—the lowest statistic among all age ranges. Since the outbreak of the pandemic, this group has been the subject of academic interest (Ding et al. 2020; Hilverda & Vollmann, 2022; Qiao et al., 2022), given their social characteristics. Among young people, university students are a populous group. In Spain, they represent 44% of the cohort between ages 20 and 29 (Instituto Nacional de Estadística (INE), 2022; Ministerio de Universidades, 2022). They travel widely and with ease, and have considerable social contact. Given the features of the disease, they tend only to suffer mild symptoms (Johns Hopkins Medicine, 2023), if any, but they have a high capacity to spread the virus, (Monod et al., 2021) and often, they live with an at-risk population (Instituto Nacional de Estadística [INE], 2021).
The above demonstrates that, for this sector of the population, there are few incentives to vaccinate, and it would be interesting to investigate what the incentives are. Thus, the object of this study is to analyse which factors are predictors of vaccination intention in this group of people, with particular emphasis on knowledge of the vaccination process, and trust in the scientific experts and in the Government.
Our initial hypothesis was that this group would have a low perception of risk. Thus, we decided to combine the health belief model (HBM), which is largely based on risk perception, with the theory of planned behaviour (TPB), which establishes that attitudes are crucially important in health-related behaviour. This has proven to be an effective strategy in previous researches (Chu & Liu, 2021; Shmueli, 2021), which have combined two of the most impactful theories of health behaviour in this manner.
In addition, recommendations to get vaccinated are an example of public communication of science. In fact, in most cases, these communications are based on what is known as the deficit model (which holds that the lack of public support for science is due to a lack of knowledge/understanding about it). It would therefore be interesting to find out whether knowledge was an outstanding factor for vaccination intention. Criticisms levelled at the deficit model hold that the problem which ordinary citizens have in following recommendations from the health authorities is not so much a lack of knowledge, but rather a lack of trust. Consequently, we set out to analyse the role of trust in the decision to get vaccinated.
This study examines the factors associated with vaccination intention among students at the University of Salamanca (Spain). Apart from the constructs associated with the health belief model and the theory of planned action, the study looked at the other two factors felt to be relevant in studies of vaccine hesitancy: knowledge, and trust in the scientific experts, in the Government, and in the doctor (WHO, 2014).
Theoretical Framework
The Health Belief Model
The HBM was developed in the 1950s by the US Public Health Service, in order to understand the failure of the public to participate in disease-prevention programmes (Rosenstock, 1974). Today, the model includes up to six constructs: perceived severity, perceived susceptibility, perceived barriers, perceived benefits, cues to action and self-efficacy. Perceived susceptibility refers to a person’s belief as to the likelihood or risk of contracting a disease. Perceived severity indicates the individual’s belief as to the intensity of the effects of the disease, for themselves. Together, these two metrics make up the perceived threat; these are the two most widely used constructs. Perceived barriers refer to the possible costs of the proposed action. Self-efficacy, which is a construct introduced by Bandura in 1997, refers to an individual’s belief in their ability to successfully perform the required behaviour. Cues to action are the stimuli which would lead the subjects to make decisions relating to their health (Champion & Skinner, 2008).
This approach has been used for a variety of studies concerning COVID-19, drawing the relations between the perceived risk and the likelihood of getting vaccinated. In other words, individuals who believe they highly likely to contract the disease, and also that it would have severe consequences for them, will probably take up the vaccination. Hilverda and Vollmann (2022) show that perceived susceptibility and perceived severity in relation to COVID-19 are predictors of vaccination, as they shape the affective perception of risk (worry) about COVID-19 in young adults between the ages of 17 and 28. Qiao et al. (2022) found a positive association between the perceived severity of COVID-19 and vaccine uptake in college students in South Carolina. Reviewing 16 studies carried out by Limbu et al. (2022), it can be concluded that the HBM is useful in predicting vaccine hesitancy, but, of the seven studies making up the meta-analysis by Wang et al. (2021), four show a positive relation between the worry of contracting the disease and vaccination intention, while the remaining three found no significant relation between the two.
Theory of Planned Behaviour
The theory of planned behaviour (TPB), developed by Ajzen (1985) on the basis of the proposal by Fishbein and Ajzen (1975), is used to predict intention, understood as the immediate precursor to action by the individual, and has been widely applied in various fields to predict subjects’ behaviour—including in the area of health and, specifically, vaccine acceptance (Catalano et al., 2017), including for the COVID-19 vaccine (Chu & Liu, 2021; Shmueli, 2021; Thaker, 2021). This model holds that there are three factors which serve to predict an individual’s intention: attitude, subjective norms and self-control. Attitude is understood as the individuals’ beliefs about the consequences that their behaviour will lead to, weighted by their evaluation of those consequences. Subjective norms refer to an individual’s normative beliefs, concerning the behaviour which is expected of the individual by social convention. Finally, self-control over future behaviour is understood as the perception that the subject has of their own ability to actually carry out the action that is being predicted (Bandura, 1997).
Knowledge
The deficit model of public understanding of science (PUS) holds that the public’s lack of support of science is due to lack of understanding of it, and that with better knowledge will come greater support for science. In relation to vaccines specifically, the argument would go thus: “people who have sufficient knowledge about a particular vaccine can better understand its potential benefits and importance, which would further shape positive beliefs about the vaccine and strengthen trust in vaccination” (Zheng et al., 2021, p. 278). However, this argument, which is in keeping with the deficit model, is not entirely immune from criticism. The first such criticism has to do with the association of fear of a new technology and lack of knowledge: fears may be cultural or be associated with certain worldviews; they may not necessarily stem from knowledge or lack thereof. A second criticism is to do with the selection of appropriate knowledge—in our case, what kind of knowledge about the new vaccines does an individual need to have in order to lower their perceived risk? The third criticism is that the effect of scientific knowledge is overwhelmed by the influence of social trust in perception of the risk of new technologies (Sturgis & Allum, 2004). Despite of the deficit model continues to be present in vaccination campaigns, in fact, the campaigns run by the Spanish Government (Ministerio de Sanidad, 2020) appear to be based on that idea, providing knowledge about the vaccine development process and their possible adverse effects. Those effects actually seemed to generate more distrust among the population. Though there are scales which measure knowledge of subjects surrounding vaccines, these scales are used in research relating to hesitancy to get children vaccinated. They hinge on the most common misconceptions about child vaccination (Zingg & Siegrist, 2012). In the case of COVID-19, the concerns about the vaccine are rather different, relating more to the timescales over which the vaccines have been developed and tested, and their possible side effects.
In addition, it is reasonable to think that there is a difference between an individual’s knowledge, measured by means of a questionnaire, and that individual’s perception of their own knowledge. In relation to vaccination in general, certain studies have shown a relationship between perceived lack of knowledge of vaccines and vaccine hesitancy (Guay et al., 2019), while others find a positive relationship between the feeling of being well informed and vaccination intention (Sherman et al., 2021).
Trust
In the area of decisions on vaccination, trust is defined as “a relationship that exists between individuals, as well as between individuals and a system, in which one party accepts a vulnerable position, assuming the best interests and competence of the other, in exchange for a reduction in decision complexity” (Larson et al., 2018, p. 1599). Trust becomes important when there is a power imbalance, due to significant asymmetry in the information available to the different parties, and the subject has to make a decision which entails certain risks and benefits. In our case, this informational imbalance is manifested by the fact that the lay public cannot possibly know whether the vaccines are effective and safe. That decision is delegated to the experts. In view of the above, it is of interest to us to discover the degree to which our group placed trust in scientific experts. According to Plohl and Musil (2020), those who have most trust in science are more willing to comply with preventive measures against COVID-19. Verger and Dubé (2020) point to the role of the family doctor as an incentiviser to vaccinate, but they also highlight trust in the health system and in those in charge of the vaccination strategy. In addition, the statements by the WHO’s SAGE (Strategic Advisory Group of Experts on Immunisation) highlight the importance of trust in (a) the effectiveness and safety of vaccines; (b) the system through which they are administered, including the trustworthiness and competence of the health services and health professionals; and (c) the motives of the policy-makers who decide on the necessary vaccines (WHO, 2014). In various studies, this has been interpreted as trust in three clearly defined institutional environments: trust in the health professionals of the social and health system, in science, and in the socio-political context (Verger & Dubé, 2020) or, in more concrete terms, the healthcare system, science and the Government (Dye et al., 2021), which led to an investigation of the trust in these three environments. In addition, confidence (or trust) is one part of the 3C model (complacency, convenience and confidence)—one of the most widely used models in studies on vaccine hesitancy.
Hypotheses
On the basis of the theory of planned behaviour, the health belief model and the above-mentioned factors, the following hypotheses have been extracted.
Given the characteristics of the disease and of our population, our first hypothesis (H1) was that the constructs of the HBM would not be good indicators of vaccination intention, given that for this group of people, the disease tended not to be terribly severe.
Considering the importance of trust in the analysis of vaccine hesitancy, we explored whom our group has trust in, and to what extent that trust influences their vaccination intention. Our second hypothesis (H2) was that the higher the level of trust, the greater should the vaccination intention be.
The constructs of the TPB, attitude, self-control and subjective norms (H3) have a positive correlation with vaccination intention.
Objective knowledge (or knowledge of technical matters) (H4) has little or no impact on vaccination intention.
Subjective knowledge, or one’s belief that one is well informed (H5), has a positive impact on vaccination intention.
Methodology
Study Participants
The information used comes from an anonymous questionnaire put to students at the University of Salamanca, the data from which were compiled between 4 and 22 December 2020. Participants were recruited by self-selection: the questionnaire was distributed by sending a hyperlink to all groups within the university, by their university e-mail, following authorisation from the institution’s Ethics Committee. All respondents gave their consent before filling in the questionnaire.
Only data submitted by students were retained for the study, as they are the target research group. The total population of students comprised 29,023 potential respondents in that cohort—the number of enrolled students during the 2020 to 2021 academic year. More than 12.2% of them responded to the survey, giving a final sample made up of 3,542 valid questionnaires in total. Assuming randomness in the responses received, for a confidence interval of 95.5% (2σ) and P = Q, this gives a sampling error of 1.57% for the university, and 1.68% if the sample is considered representative of all university students (or young people) in the country.
Only two demographic characteristics were included in the questionnaire: gender, woman (71.1%) or man (28.9%), and age, with five groups: (a) <25 (82%), (b) 25 to 34 (12.4%), (c) 35 to 44 (3.2%), (d) 45 to 54 (1.8%), and (e) >55 (0.6%). The over-representation of women, while real, is not as high as it may seem, given that, in the academic cohort to which the questionnaire was distributed, women represented 60.2% of enrolled students. But age was not used in this research because most of the respondents belonged to the first group.
Instruments and Measurements
To contrast the hypotheses, a number of questions from the contents of the questionnaire were used. In certain cases, it was necessary to construct indicators which furnished the necessary measurement (as a proxy variable).
Dependent Variable: COVID-19 Vaccination Intention
Vaccination intention (VACINT) was measured by means of the following question: “If, tomorrow, there were a vaccine available to prevent COVID-19, would you take it?” Response options were on a scale of 1 (absolutely not) to 7 (with total confidence). This echoes the scale to measure vaccination intention put forward by Zampetakis and Melas (2021), but differs from the approaches employed by Chu and Liu (2021), Dye et al. (2021), Shmueli (2021), and Zheng et al. (2021).
Predictive Variables
To measure the variables in the HBM, two questions were used. Perceived susceptibility (PSUSC) was assessed using the question: “In relation to yourself, what would you say is the likelihood of contracting the novel coronavirus?,” with options ranging from 1 (highly unlikely) to 7 (highly likely). Perceived severity (PSEVER) was assessed using the question: “How severe do you think it would be for you to become infected the novel coronavirus?,” with options ranging from 1 (not serious at all) to 7 (extremely serious). Both these questions have been widely used, in healthcare studies in general (Comodari, 2017), and specifically in relation to COVID-19 (Hilverda &Vollmann, 2022; Rattay et al. 2021).
However, the methods used in this study to measure the various aspects of the Theory of Planned Behaviour are entirely new, having been developed by the authors specifically for this study. That is, they are not tried-and-tested metrics. Nevertheless, we believe that our metrics, as described below, are appropriate to approximate the factors of this model: the use of proxy variables yields lower bias than does the omission of explanatory variables (Wooldridge, 2009, p.310). To establish the value of attitude (ATTIT), an indicator was developed, with values ranging from 0 to 3. This value included the sum of the responses to two questions: (a) “Are vaccines effective in preventing disease?” (as opposed to other opinions about vaccines in general [1 point]), (b) Have the news stories about problems that have arisen in vaccine trials influenced your perception of vaccine safety? (0 if it led them to mistrust the vaccine, 1 if they felt that was a normal outcome, and 2 if it reinforced their confidence in the vaccine’s safety).
The subjective norm (NORM) was evaluated by means of a binary variable, based on the responses as to whether the vaccine should be compulsory (1 = Yes, 0 = No), as we believe it an adequate proxy to know the individuals’ beliefs about the hypothetical case of compulsory vaccination.
Self-control (SELFCON) was evaluated on the basis of the response to the question “When do you believe that the vaccine will be available for the whole population of Spain?,” with the following values: (4) It will take at least 3 months; (3) It will take at least 6 months; (2) It will take at least 9 months; (1) It will take at least 12 months.
To establish the level of subjective knowledge (SUBKNOW), a single question on the questionnaire was used: “To what extent do you feel yourself informed about the development of COVID-19 vaccines?,” with responses ranging from (1) Not well informed, to (7) Well informed. Then, to determine objective knowledge (OBJKNOW), an indicator was constructed on the basis of nine statements about vaccine development. To develop the items in this question, we used the information available from the Ministry of Health about vaccine development (Ministerio de Sanidad, 2020). Respondents were asked to determine whether each of the following statements was true or false: (a) The pre-clinical trial phase inevitably involves testing the vaccine on nonhuman primates. (b) All effective vaccines are safe. (c) The first step in vaccine trials is to demonstrate that the vaccine is safe and effective in animal organisms. (d) The WHO has determined that COVID-19 vaccines must be at least 80% effective. (e) The flu vaccine prevents COVID-19 infection. (f) Vaccines must pass at least seven stages of clinical trials. (g) All vaccines may have side effects. (h) There is an effective homeopathic vaccine against coronavirus. (i) The Oxford vaccine is in the final stage of clinical trials. Thus, the indicator’s value may be anywhere between 0—no correct responses—and 9—all responses correct. The value of the internal consistency of this indicator, calculated on the basis of the Kuder–Richardson coefficient KR20 (Kuder & Richardson, 1937), was 0.438. Though this is a low value, it was deemed to be an appropriate indicator, because of the similar level of education across the sample. This produces less variance in the total score which leads lower values of Cronbach’s alpha (Streiner, 2003), or, in this case, the KR20 coefficient.
To establish the respondents’ levels of trust in the different groups, the questionnaire included a question measuring the degree to which the respondents would take account of the opinion of various people in making their decision whether or not to get the COVID-19 vaccine. The participants answered on a scale of 1—little trust—to 7—a great deal of trust—in the person in question. Trust in the doctor (TRUSTDR) was measured by means of a single item on that question, which specifically referred to the physician. To measure trust in the Government (TRUSTGOV), the mean value of the following two items was used: “Trust in the Minister of Health” and “Trust in the Director of the Centro de Coordinación de Alertas y Emergencias Sanitarias” [Coordination Centre for Health Alerts and Emergencies], Fernando Simón, who was the spokesman for the Ministry during the fight against the COVID-19 pandemic (Cronbach’s α = .828). To establish the value of trust in experts (TRUSTEXP), a similar approach was applied, taking the mean of the items “Trust in a virologist from the Spanish National Research Council” and “Trust in the former director of the WHO’s Health Action in Relation to Crises and Disasters” (Cronbach’s α = .771).
The only control variable used was gender (WOMAN = 1).
Statistical Analyses
The software SPSS V.28 was used to assess the bivariate relationship between the explanatory variables and the dependent variable, and to perform multiple regression to find the degree to which vaccination intention depends on the factors indicated in our hypotheses.
To study these models, multiple linear regression (MLR) was applied, with the variables input in hierarchical order—that is, the variables were added sequentially. They were added in blocks, as the objective was to assess the effectiveness of the proposed theoretical model, rather than simply to find new models by exploration (Tabachnick & Fidell, 2007). In this way, it is possible to find each one’s contribution to the dependent variable being analysed. For this purpose, to begin with, the control variable was added: WOMAN—the only available demographic variable. Next the rest of analyzed dimensions. The macro PROCESS V.4.1 was used to identify any mediating effects between the explanatory variables.
Results
Influencing Factors on Acceptance of COVID-19 Vaccine
Table 1 describes the variables and their bivariate relation to the dependent variable. The two variables for the HBM were omitted from the overall model, given that, as Table 1 indicates, neither of them had a significant bivariate relation to vaccination intention and, for reasons of parsimony, it was inadvisable to include them.
Descriptive Statistics of the Variables Used.

p < .001.
Table 2 sets forth the values of the unstandardized coefficients of the different multiple-regression equations. It also includes the values of the coefficient R2 for each of these equations. In addition, it presents the values of F, to determine whether there is a significant change in the explicit variance of the dependent variable (VACINT) when the variables corresponding to the model are added. Finally, for the equation resulting for the complete model, with all the interest factors, the standardized regression coefficients and VIFs (Variance Inflation Factors) are stated. (See Supplemental Appendix to check other linear regression assumptions).
Hierarchical Multiple Regression Analysis. Coefficients of Predictors of COVID-19 Vaccination Intention (VACINT).
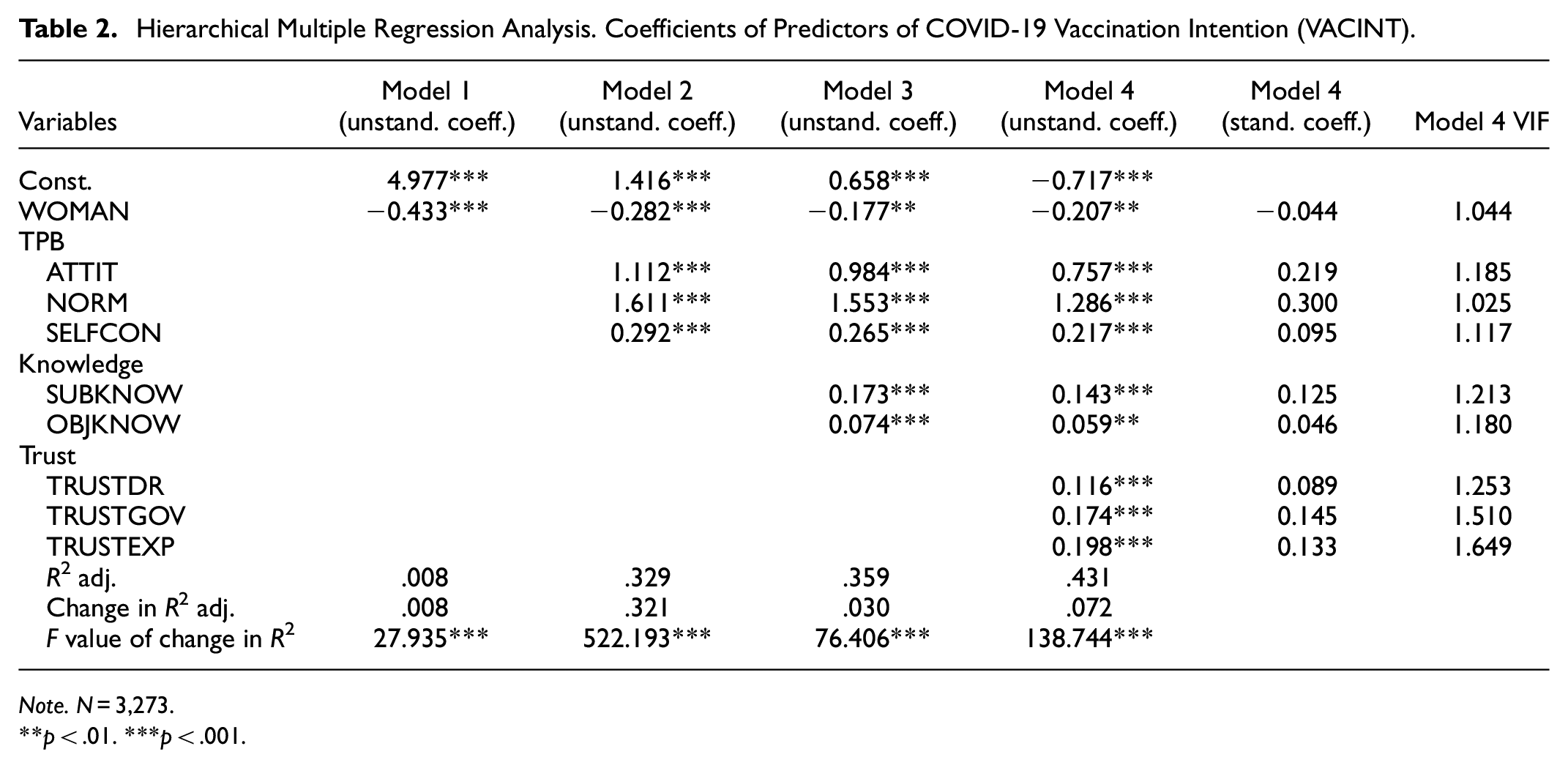
Note. N = 3,273.
p < .01. ***p < .001.
The fits of all the models are significant, as are the changes that occur in the adjusted R2. The contribution of the only available sociodemographic variable (WOMAN), though slight (0.8%), is significant. The component factors of the TPB are those which make the greatest contribution to the prediction of the dependent variable (32.1%). The two types of knowledge about the vaccine (objective and subjective) inject 3% variability which is not accounted for by the previous two models. Finally, the trust in the various groups (in the family doctor, in the Government and in the experts) makes up 7.2% of the remaining percentage of the total of the adjusted R2, finally reaching 43.1% with the full model (Model 4), and thus accounting for over 43% of variance in vaccination intention.
The women in the studied group have a lower vaccination intention than do the men, as a negative regression coefficient is seen. However, all the other factor making up the set of theories included in the proposed model have a positive impact on the dependent variable. Considering the values of the standardized coefficients, it can be seen that subjective norm and attitude have the greatest impact on vaccination intention. On the contrary, we can see that gender and objective knowledge have the least impact on the studied variable.
Mediating Effects
The collinearity tests reveal acceptable values, far from the levels considered to be evidence of collinearity (VIF > 5). Nevertheless, given that it is an imperfect measurement, which may not pick up the complex relations between the explanatory variables (Heiberger & Holland, 2015), we opted to analyse the possible mediating effects of the two independent variables with values over 1.5: trust in the Government and trust in the experts. In other words, we decided to study the possible mediating role of these two types of trust between the subjects’ knowledge (both objective and subjective) and their vaccination intention, given that according to the deficit model, greater knowledge should lead to greater trust. To study this, we used the macro PROCESS V4.1 for SPSS. Specifically, Model 4 was applied, with the aforementioned mediating variables in parallel, and a total of 10,000 bootstrapping samples (Hayes, 2018). By this method, it is possible to estimate the total effects, direct effects and indirect effects. Of these, the method enables us to estimate whether or not the effect is present, by providing, in addition to the effects, the standard errors and confidence intervals (CI) at 95% (Hayes, 2018). (See Supplemental Appendix)
Figures 1 and 2 show the unstandardized regression coefficients, also reflecting the direct effect (quoted in Table 2, Model 4) and the total effect, in brackets. Table 3 sets out the indirect effects occurring by the mediation of trust (in the experts and in the Government) between (objective and subjective) knowledge and vaccination intention.
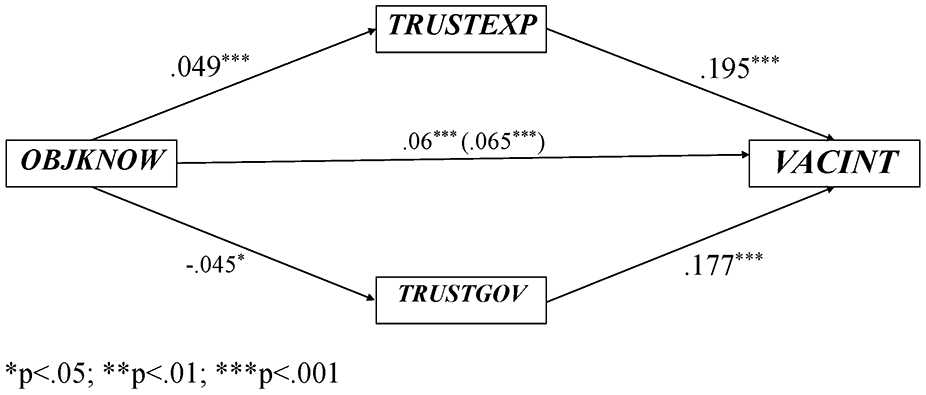
Unstandardized regression coefficient of the mediating effect of trust in expert and trust in government, between objective knowledge and vaccination intention.
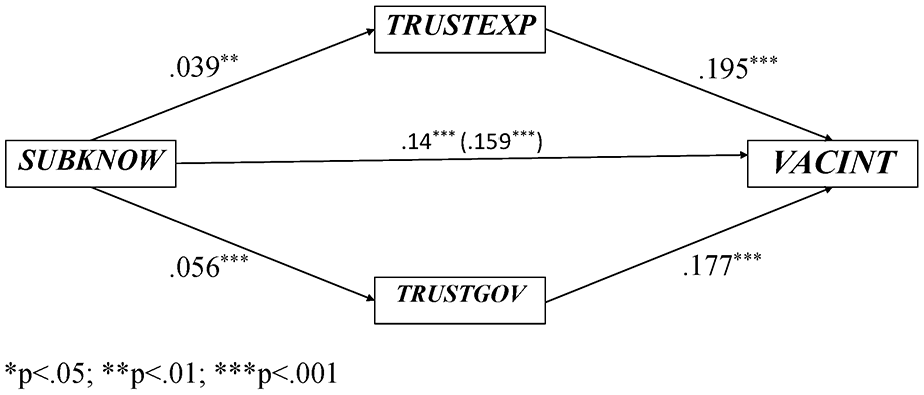
Unstandardized regression coefficient of the mediating effect of trust in expert and trust in government, between subjective knowledge and vaccination intention.
Indirect Effects of the Impact of Objective and Subjective Knowledge on Vaccination Intention.

In both these figures, it can be seen that all the coefficients are significant. The same thing happens with the indirect effects, as none of the CIs estimated by means of the bootstrapping samples contains zero, which would be indicative that the aforementioned effects are not significant. It is apparent that the effect of the objective knowledge, through trust in the experts, has a positive impact, reinforcing the effect on the dependent variable. On the other hand, this type of knowledge has a negative influence on trust in the Government and, thereby, reduces its effect on vaccination intention.
The mediating effects of subjective knowledge, both on trust in the Government and on trust in the experts, are positive. That is, this type of knowledge increases trust, reinforcing the influence of feeling oneself well informed on vaccination intention.
Discussion: Determining Factors Influencing Vaccination Intention
Our study focuses on a group of people who, due to their characteristics—high social mobility and only mild symptoms from COVID-19—have low incentives to get vaccinated; however, they contribute greatly to the spread of the virus, so they need to be a high priority for vaccination campaigns. In order to effectively design and target those campaigns, it is enormously important to understand the factors which positively impact on the vaccination intention of this sector of the population. Neither the perceived severity of the disease nor their own perceived vulnerability to it have been found to be reliable predictors; however, their trust in the Government and in science are. This, combined with the variables of the TPB model and those relating to knowledge, allowed us to construct a model which accounts for over 43% of the variance in vaccination intention.
Gender-based Differences in Attitude Toward Vaccination
In our study group, 25.5% of the women responded that they would get vaccinated without hesitancy, compared to 37.8% of the men (INTVAC = 7). Hence, being female may be said to have a negative effect on vaccination intention. This is in keeping with the findings of the majority of studies analysed by Wang et al. (2021), and with others such as Zampetakis and Melas (2021), Zheng et al. (2021), and Shmueli (2021). Our study also asked respondents about reasons why they would refuse a vaccine. The majority of women had doubts as to the vaccine’s safety, whereas the reasons given by men tended to be that they felt their risk of infection was low.
Effect of HBM
The HBM has produced disparate results in the various studies where it has been employed: Zampetakis and Melas (2021), Shmueli (2021), and Limbu et al. (2022). In our study, neither perceived severity nor perceived susceptibility are found to have an impact on vaccination intention, which confirms H1. We believe the reasons relate to the fact that the fundamental variable which the model analyses is perceived risk, and many studies point to differences in risk perception between young adults and the rest of the population (Kollmann et al., 2022; Scaletti et al., 2022).
Effect of TPB
The TPB performed better as a predictor of vaccination intention in this group than did the HBM, so H3 is confirmed. This is in line with Seddig et al. (2022), who found that attitude is a powerful predictor of vaccination intention. We believe the model’s yield is related to the fact that, as one of the explanatory factors, it takes account of the subjective norms—that is, the perception of what is felt to be proper behaviour by one’s own social group. Latkin et al. (2021) also found that individuals with a stronger perception of the social norms (defined as the subjective norms) of social distancing and mask-wearing had higher levels of trust in the COVID-19 vaccine. The subjective norms had a greater effect on vaccination intention than any other variable. In addition, it is surprising that so high a percentage of the group (55%) believed vaccination should be compulsory.
Effects of Objective and Subjective Knowledge
Knowledge is a typical variable in the explanation of the decision to accept a vaccine (WHO, 2014; Huynh et al. (2021)), but we must distinguish between the subjective—that is, the subject’s perception of their own knowledge—and the objective, measured on some kind of a scale. In our study, it is noteworthy that subjective knowledge carries the most weight—those individuals who feel themselves better informed are more likely to get vaccinated, which confirms H5. This contrasts with the results found by Lee et al. (2022), who report a positive correlation between the feeling of being well informed and vaccine hesitancy. The authors attribute this result to the so-called “infodemic,” where abundant information does not necessarily mean accurate information. Thus, it is possible that as vaccination campaigns continue, and fake news and conspiracy theories continue to spread, the feeling among the recipients of that misinformation that they are well informed could be negatively associated with vaccination intention. Therefore, in spite of the problems of the knowledge deficit model, it was helpful to have some measurement of objective knowledge. In our model, objective knowledge carries far less weight than do the rest of the explanatory factors in vaccination intention (standardized coefficient 0.046). This means that the level of a person’s knowledge about the vaccine has a certain amount of weight, but it is not—by a long chalk—the most important factor influencing the studied dependent variable. It could be argued that we did not select the right means of measuring knowledge, but that is among the criticisms often levelled at the deficit model. Whilst knowledge is a variable that impacts vaccination intention, it needs to be established which type of knowledge ought to be broadcast to the public. In general terms, our finding that knowledge does not greatly impact vaccination intention confirms our H4, and is consistent with the more contemporary view of PUS. According to that view, there is not a knowledge deficit which prevents the general public from supporting science, but rather, a deficit of trust in science, and specifically, in scientific experts (Clements, 2020).
Effect of Trust in the Health System, in the Government and in the Experts
The figure of the family doctor, and the trust with which they are invested, has always been of enormous importance in all vaccination strategies, so we include the doctor as a relevant figure in the decision to take a vaccine. Surprisingly, the value of the standardized coefficient (0.089) shows that, in the case of COVID-19, it is far less important than the trust in experts (0.133) or trust in the Government (0.145) in the decision to get vaccinated. In any case, trust in all three systems is positive, which confirms H2. This indicates that COVID-19 vaccination strategies need to be radically different to campaigns aimed at persuading parents to vaccinate their children, which tend to hinge on the importance of the doctor. Our group trusts in science to a large extent, as shown by the mean value of the respondents’ trust in experts and, to a lesser extent, in the Government (Table 1). However, it is their trust in the Government (or lack thereof) which is most important in shaping their vaccination intention (Table 2). This coincides with the results found by Van Oost et al. (2022), Lazarus et al. (2021), and Soares et al. (2021), highlighting the positive association between trust in the Government and vaccination intention. As to trust in experts, our results are in line with those obtained by Thaker (2021), for whom trust in scientific experts is one of the strongest correlates of COVID-19 vaccine intention. They are also in agreement with the work of Dye et al. (2021) and Seddig et al. (2022), who found that attitudes toward science were a strong predictor of vaccination intention. It appears that trust in the Government and trust in experts go hand in hand, so one way of fostering trust is through the advice of a scientific expert.
Mediating Effects of Trust Between Knowledge and Vaccination Intention
Another of the conclusions that can be drawn is that objective knowledge has an indirect effect on vaccination intention. Knowledge has a positive impact, as it creates trust in the experts; however, it negatively impacts the level of trust in the Government (Figure 1). That is to say, greater objective knowledge means greater trust in experts and less trust in the Government. It reduces trust in the Government, leading to a reduction in vaccination intention. On the other hand, such knowledge has an increased effect on that intention, as it increases trust in experts, and that has a positive impact on the likelihood that our group will get vaccinated against COVID-19. However, subjective knowledge positively affects both trust in the Government and trust in experts. Thus, part of the effect, on vaccination intention, of feeling oneself well informed acts by influencing the trust that our population has in the Government and in the experts. This leads us to believe that one way of building trust is through providing information which, in principle, is unlike the type of knowledge used in the governmental campaign, centring around objective knowledge, which was used for the construction of our indicator. Rather, it is a matter of transparent management, meaning that the populace perceive that they are receiving accurate information about the Government’s process in making this type of decision. Proof of this lies in the fact that 78.8% of respondents, in a question included on the questionnaire used for this study, pointed to the need for the general population to know the identity of the experts advising the Government.
Conclusions
Looking at our results, messages focusing on the risk of contracting the disease do not appear to be effective in incentivising this target group to accept a vaccine. The most decisive factor is trust in the Government. Therefore, information campaigns need to be transparent and rigorous. This does not mean that they need to go into great depth on a technical level; however, it is advisable that the information come from trustworthy scientific experts.
Limitations
There are certain limitations to our study. To begin with, in view of the characteristics of the questionnaire, no sociodemographic variable other than gender has been able to be taken into consideration, as the Ethics Committee insisted that age be recorded only in age groups, to safeguard the students’ anonymity, and not asked as an open question. Similarly, the questionnaire provided no information that would allow better proxy variables to be used to apply the TPB to our model. In addition, the population studied (university students) meant that education level could not be used as a control variable, This could also be a contributing factor to vaccination intention. Finally, there may be a certain amount of sampling bias, resulting from the fact that the respondents were recruited by self-selection, and it is likely that our sample is representative of young university students, rather than of that age group as a broader whole.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241267044 – Supplemental material for The Impact of Knowledge and Trust on COVID-19 Vaccination Intention: Analysis of a Population Group with Low Incentives to Vaccinate in Spain
Supplemental material, sj-docx-1-sgo-10.1177_21582440241267044 for The Impact of Knowledge and Trust on COVID-19 Vaccination Intention: Analysis of a Population Group with Low Incentives to Vaccinate in Spain by Obdulia Torres González and Libia Santos-Requejo in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been funded by Ministerio de Ciencia e Innovación, El papel de la experticia distribuida y dialógica en la solución de controversias científico-tecnológicas publicas: un análisis epistemológico, argumentativo y sociológico PID2019-105783GB-I00
Ethical Approval
This research has been evaluated favorably by the Research Ethics Committee of the University of Salamanca. Identification number of the application 00549.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.