
Abstract
This study examined whether the Health Belief Model and the heuristic of multilevel institutional trust would help explain U.S. residents’ support for travel bans on foreigners during the COVID-19 pandemic. Analysis of data collected from two nationwide online surveys conducted in 2020 (n = 511 fielded between March 19 and March 27; n = 472 fielded between April 30 and May 13) suggested that support for this policy was associated with individual differences in risk and benefit perceptions, the presence of interpersonal cues, and trust in domestic and foreign institutions. Efforts to promote or resist international travel restrictions during a pandemic may benefit from accounting for these differences.
Plain Language Summary
There is limited research on the psychological motivators of support for disease control measures that do not require personal action. Focusing on the travel restrictions imposed on foreigners by the U.S. government during the early phases of the COVID-19 pandemic, the current study explored whether the Health Belief Model and the heuristic of multilevel institutional trust would help explain U.S. residents’ support for these restrictions. Analysis of data collected from two nationwide online surveys conducted in 2020 (n = 511 fielded between March 19 and March 27; n = 472 fielded between April 30 and May 13) suggested that support for this policy was associated with individual differences in risk and benefit perceptions, the presence of interpersonal cues, and trust in domestic and foreign institutions. These findings can help national and international institutions in their endeavors to shore up support for their cross-border disease control policies during future outbreaks.
Keywords
During the early stages of the COVID-19 pandemic, there was almost universal imposition of international travel restrictions by governments to control the importation and transmission of SARS-CoV-2 and its variants (Connor, 2020; K. Lee et al., 2021; Salcedo et al., 2020). Considerable research has been conducted on the effectiveness of these restrictions in limiting the spread of COVID-19 and other infectious diseases (Mateus et al., 2014; Russell et al., 2021; Ryu et al., 2020). However, review studies suggest that more research is needed to understand the psychosocial motivators of individual support for such policies (Aiello et al., 2010). The current study sought to contribute to this line of inquiry by exploring psychological factors associated with U.S. residents’ support for the travel restrictions imposed on foreigners during the COVID-19 pandemic. The U.S. travel bans, as explained below, illuminate some of the competing interests between national and international institutions as they react to global outbreaks. Using data collected at two points in time, the current study offered some preliminary evidence on how shifting political interests and epidemic situations domestically and internationally could reshape public trust in different institutions and inform support for cross-border disease control measures.
An array of international travel restrictions has been implemented by different countries during the COVID-19 pandemic, ranging from granting entry to travelers who tested negative for COVID-19 prior to departure only, to denying entry to all non-nationals (K. Lee et al., 2021). Among the different types of restrictions, blanket entry bans on visitors from certain countries, such as the ones implemented by the United States in 2020, are one of the most controversial. Some global health and human rights experts suggest that such bans can help protect the right to health within a country (Chia & Oyeniran, 2020; Sekalala et al., 2020), whereas others perceive these bans as a contravention of the principles set out in the International Health Regulations (IHR), the legal framework adopted by the WHO and revised in 2005 to guide international collaboration in responding to health threats.
Given the premises of the IHR, WHO (2020, 2021c) recommended against the imposition of international travel restrictions during the early phases of the COVID-19 pandemic, citing concerns about these restrictions’ undue consequences on civil liberties, national economies, and international collaboration. However, it is unclear whether these consequences are factored into individuals’ support for entry restrictions on foreigners, and what additional considerations might be associated with support for such policy. There is a need to fill this knowledge gap, as the WHO and national governments begin to face internal and external reviews of their COVID-19 response and the legal frameworks undergirding such response (WHO, 2022). Revisions to these frameworks would benefit from a deeper understanding of psychological factors associated with individual support for cross-border restrictions during global outbreaks. Such understanding would not only help national and international institutions address public concerns in their revised approaches to managing cross-border disease transmission, but also enable these institutions to better communicate the rationale behind their policies to the public.
One prominent theory that illuminates how psychological factors motivate support for public health measures is the Health Belief Model (HBM). In addition to personal compliance with public health recommendations, research conducted during the COVID-19 pandemic suggests that the HBM can help explain support for restrictive policies that may not have an immediate impact on individuals, such as vaccination requirements for air travel (Suess et al., 2022). However, travel bans on foreigners do not require local residents to modify their behavior in any way, either in the present or in the future. Given this distinction, the current study sought to investigate whether the HBM can be applied to understanding support for entry restrictions on foreigners.
Furthermore, the present study explored the role of multilevel institutional trust as a judgment-making heuristic in shaping support for cross-border disease control strategies. The HBM follows a value-expectancy approach and considers health decisions as a result of a systematic evaluation of beliefs relevant to the outcome of a health behavior (Conner & Norman, 2015). Beyond systematic evaluation, research has demonstrated that trust in domestic authorities is a mental shortcut frequently used by individuals when deciding whether they would support public health measures implemented to control infectious diseases (Bish & Michie, 2010; Holroyd et al., 2021). Therefore, it is of interest to assess the relationship between trust in domestic authorities and support for COVID-19 travel bans among U.S. residents. Given the global scope of the COVID-19 pandemic and the cross-border impact of entry restrictions, it is plausible that trust in institutions beyond national borders could also influence support for this policy. However, extant literature rarely looks into if and how trust in foreign or intergovernmental institutions shapes individual response to international public health crises (Bayram & Shields, 2021). The current study thus sought to investigate this topic.
A number of institutions at different levels of governance (e.g., domestic, intergovernmental, foreign) have been implicated in the U.S. entry restrictions implemented to control COVID-19. The current investigation focused on former U.S. President Donald Trump, the WHO, and the Chinese government as three highly relevant sources of institutional trust that might sway individual judgments. However, before assessing whether trust in each of these authorities was associated with policy support, it was critical to establish whether trust in these institutions represented distinctive constructs. This was necessitated by the observation that most Americans have limited knowledge of foreign affairs and institutions (Bayram & Shields, 2021). It is thus possible that individuals’ trust in external institutions is merely a reflection of either their trust in domestic authorities, or their underlying tendency to be more or less trusting in all institutions (Muñoz et al., 2011). Therefore, it was important to clarify the relationship among multilevel institutional trust before conducting further analyses.
Through statistical analysis, the current study found that trust in the U.S. President, WHO, and Chinese government were indeed distinctive constructs. Further analysis was therefore conducted to explore how the relationship among trust in these authorities evolved during the COVID-19 pandemic amid rising tension among these institutions. Utilizing data collected at two points in time during the early phases of the pandemic, this study provided insights into the dynamic nature of multilevel institutional trust and its potential consequences on individual support for cross-border disease control measures.
The U.S. Travel Bans: A Subject of Scientific and Political Uncertainty
International travel restrictions alone have limited effects on keeping pathogens from border-crossing (Mateus et al., 2014). However, early and stringent border regulations, especially when complemented with proactive domestic public health efforts (Chinazzi et al., 2020), can mitigate the impact of global outbreaks on a country (Leonhardt, 2021). Therefore, some global health and human rights experts consider cross-border restrictions a way to protect the right to health within a country, as they help slow down disease importation and transmission domestically (Chia & Oyeniran, 2020; Sekalala et al., 2020). However, others argue that border control measures implemented by national governments often contravene the principles set out in the International Health Regulations (IHR) and violate fundamental human rights.
The IHR stipulates that governments should implement disease control measures with full respect for human rights (e.g., rights to movement and economic activity) and without being unnecessarily restrictive (WHO, 2016). In reviewing international travel restrictions implemented during recent global outbreaks, researchers contend that these IHR stipulations were often breached (Gostin et al., 2020). In addition, experts warn that cross-border restrictions tend to impose disproportionate socioeconomic burdens on marginalized peoples (Forman & Kohler, 2020; WHO, 2020). There is also concern that governments may conceal or underreport future outbreaks within their jurisdiction, in contradiction to their obligation under the IHR, due to worries about economic harm associated with border restrictions (Worsnop, 2017).
In light of these considerations, the WHO, the leading agency for coordinating global health issues within the United Nations (UN) system, has typically advised against the application of international travel restrictions by national governments during international outbreaks (Gostin et al., 2020; Grépin et al., 2021). In the early phases of the COVID-19 pandemic, the WHO also issued an opposition to any type of international travel restriction (WHO, 2020). Even though the organization has since updated its international travel recommendations in response to the emergence of various SARS-CoV-2 variants (WHO, 2021b), it has continued to advise against the imposition of blanket travel bans on visitors from particular countries (WHO, 2021c).
Against the WHO’s advice, former U.S. President Donald Trump issued five proclamations between January 31 and May 24, 2020, to suspend the entry of foreigners who have visited China, Iran, European countries in the Schengen Area, the United Kingdom, Ireland, or Brazil during the previous 14 days. As the first target of the U.S. travel bans, the Chinese government was critical of this policy and its civil rights implications (Maxouris, 2020). However, beyond the official exchange of critical words, U.S.-China relations remained amicable in the initial weeks following the bans. President Trump was reported to have several phone conversations with the Chinese President Xi in February 2020, and Trump also publicly praised Xi for effectively managing the COVID-19 situation in China at that time (Viala-Gaudefroy & Lindaman, 2020).
The rift between the U.S. and Chinese governments began to widen following the WHO’s pandemic declaration on March 11, 2020. The United States soon became a global epicenter of COVID-19. As domestic cases surged, Trump became increasingly vocal in his criticism of the Chinese government and its lack of transparency when COVID-19 first emerged (Mangan, 2020). By April, Trump was also publicly dissatisfied with the WHO, criticizing its slow initial response to the pandemic and its close ties to China. The U.S. President went as far as withdrawing the country’s membership from the WHO due to these concerns (Moncus & Connaughton, 2020). While President Trump halted funding for the WHO for a while, his plan to withdraw U.S. membership from the WHO did not ultimately come to pass, as this decision was retracted by President Biden on his first day in office on January 20, 2021 (Morales, 2021). It was under this context of scientific uncertainty and political controversy that the current study took place.
In laying out the context for the current investigation, it becomes clear that the interests of governmental and intergovernmental institutions could clash in different ways during an international outbreak. The reality and rhetoric of cross-border restrictions are not merely informed by the tension between the need to protect the right to health within a country, and the need to guard human rights worldwide. These policy decisions and announcements can also be used by national authorities to direct the public’s gaze outward and away from domestic troubles, while simultaneously providing reassurance that strong and sovereign action is being taken to protect the population from disease (K. Lee et al., 2021; Worsnop, 2017). The current study sought to provide some preliminary evidence on whether these strategies could reshape public opinions on external institutions and motivate receptiveness toward border control measures during a pandemic.
Health Belief Model and Support for Entry Restrictions
Research on individual support for outbreak control strategies typically focuses on public health measures that require individuals to take action, such as immunization, enhanced personal hygiene, and social distancing (Bish & Michie, 2010). Such inquiry is often informed by expectancy-value theory, according to which a person is assumed to perform an elaborate cost-benefit analysis before choosing a behavioral option with the highest expected utility among different courses of action (Conner & Norman, 2015). For example, the Health Belief Model (HBM), one of the most widely applied health behavior change models since the 1950s, postulates that motivation is key to the adoption of new behaviors (Janz & Becker, 1984). Moving beyond the traditional focus on sociodemographic determinants of behavior, the HBM identifies a set of psychological factors that motivate action. People are motivated to the extent that they perceive a health problem as serious (i.e., perceived severity), feel themselves to be at risk (i.e., perceived susceptibility), believe that the recommended behavior is beneficial (i.e., perceived benefits), and regard the costs associated with the recommendation as reasonable (i.e., perceived barriers).
All of the abovementioned HBM constructs seem relevant to understanding support for entry restrictions on foreigners during a pandemic. It is plausible that individuals who consider themselves more susceptible to the pandemic disease, and who connect the disease to more serious consequences, would be more supportive of cross-border restrictions to control the pandemic. Individuals are also more likely to support these restrictions when they perceive the policy as an effective means to control the spread of disease. On the other hand, the “barriers” to implementing cross-border restrictions might be less obvious and personal to most individuals. Unlike personal behavioral modifications, which constitute the focus of HBM research, travel restrictions on foreigners do not incur direct costs to most local residents. Instead, the “barriers” to this mitigation strategy are typically discussed in more abstract terms (e.g., the associated costs to domestic and global economies, negative consequences on human rights, and impact on international collaboration) (Forman & Kohler, 2020; Gostin et al., 2020; Human Rights Watch, 2020; WHO, 2020; Worsnop, 2017). This is in contrast to how perceived barriers are typically operationalized in personal and concrete terms in HBM research (e.g., the financial, psychological, and physical costs to an individual). It is therefore of interest to investigate if these more abstract and impersonal costs are associated with individuals’ support for travel restrictions on foreigners.
Over the years, the HBM has been expanded to include two more constructs to enhance its predictive power—“self-efficacy” and “cues to action” (Rosenstock et al., 1988). Self-efficacy refers to individuals’ belief in their own capability to overcome obstacles in performing a behavior. This construct has little relevance for understanding individual support for public health measures that do not call for personal action, such as travel restrictions on foreigners. Therefore, self-efficacy was not examined in the present study. The other construct, cues to action, is defined as anything that prompts individuals to undertake a health behavior, such as public service announcements in the media or reminders from one’s doctor. In the context of COVID-19 travel restrictions, mediated and interpersonal cues can conceivably encourage policy support or objection. The present study thus focused on interpersonal cues and investigated whether knowing someone who has been affected by the travel bans was associated with support for this policy.
The HBM has informed many studies on preventive action and intention during international disease outbreaks in recent history, such as the 2002 to 2003 Severe Acute Respiratory Syndrome (SARS) pandemic, and the 2009 to 2010 H1N1 swine flu pandemic (Bish & Michie, 2010; Coe et al., 2012). This line of research indicates that while the HBM as a whole serves as a useful framework for understanding receptivity toward disease control measures, the predictive power of each HBM construct varies by disease, intervention, and country (Bish & Michie, 2010; Coe et al., 2012). Research on COVID-19 has similarly demonstrated the general utility of the HBM as an explanatory framework for personal preventive behaviors, as well as variations in individual constructs’ predictive power across behaviors and countries (Chu & Liu, 2021; Kim & Kim, 2020; Tong et al., 2020).
When it comes to understanding the psychological motivators of support for disease control measures that do not require personal action, there is a scarcity of empirical investigations overall, let alone research that is informed by the HBM. In one recent study by Suess et al. (2022), perceived susceptibility to COVID-19, perceived severity of COVID-19, and perceived protection benefits of COVID-19 vaccination were found to predict receptivity toward vaccination mandates for air travel, which might or might not have a direct impact on an individual. These findings suggest that the HBM can be a promising framework for understanding individual support for travel restrictions on foreigners. However, given past evidence on the varying predictive power of individual HBM constructs across disease control measures and countries, and in light of the more abstract way in which barriers to travel restrictions were operationalized in the present study, it is important to empirically investigate the following research question (RQ):
RQ1: Is support for entry restrictions on foreigners during the COVID-19 pandemic associated with (a) perceived susceptibility to the disease, (b) perceived severity of the resulting illness, (c) perceived benefits of such restrictions, (d) perceived costs of such measures, and (e) interpersonal cues?
Measuring Multilevel Institutional Trust and Its Impact
One major critique of the HBM pertains to its insufficient attention to the role of heuristics in shaping health decisions (Chen, 2015). Heuristics are mental shortcuts used by individuals in judgment making when they lack the time, interest, ability, or other resources to thoroughly evaluate all information relevant to a decision (Siegrist et al., 2000). A heuristic that has gained traction in research on individual response to public health crises is institutional trust (Giddens, 1990). Also known as system-oriented social trust (Frewer & Salter, 2007), it refers to trust directed at public institutions created to act on individuals’ behalf in managing a multitude of risks in modern society. Various models, such as the Trust Determination Model (Quinn et al., 2009) and the Trust, Confidence and Cooperation Model (Earle et al., 2007), have been developed to shed light on the centrality of institutional trust in influencing judgments in the face of health hazards. This construct is thus integrated into the HBM to provide the theoretical framework for the present study.
Researchers in different countries have consistently found that trust in domestic institutions—at the local, state, or federal level—motivates preventive action and intention during a pandemic. For example, trust in local authorities was positively related to personal protective behaviors, such as frequent sanitizing and mask-wearing, in Hong Kong during the SARS pandemic in 2003 (Tang & Wong, 2005). During the 2009 to 2010 H1N1 flu pandemic, higher levels of trust in one’s government were associated with greater intention to vaccinate against H1N1 influenza in the United States (Freimuth et al., 2014; Quinn et al., 2009), Netherlands (van der Weerd et al., 2011), and Italy (Prati et al., 2011). Trust in domestic authorities was also positively associated with personal sanitizing and social distancing practices in Italy (Prati et al., 2011) and the United Kingdom (Rubin et al., 2009) during the 2009 H1N1 flu pandemic.
Similarly, during the COVID-19 pandemic, trust in one’s government was found to predict preventive intention and action. For example, research conducted across 23 countries found that greater trust in one’s government was associated with greater likelihood of engaging with personal protective behaviors, such as frequent handwashing, avoiding crowded spaces, and self-quarantine (Han et al., 2021). Trust in domestic authorities was also positively associated with intention to vaccinate against COVID-19 in the United Kingdom, United States, Australia, and Germany (Grüner & Krüger, 2021; Trent et al., 2022). Compared to the wealth of research on the role of trust in one’s government in shaping personal compliance with preventive recommendations, there is little investigation on disease control measures that do not require personal action. Blair et al. (2017) conducted one of the few studies on this topic during the 2014 to 2015 Ebola epidemic in Liberia. They found that trust in domestic authorities was positively associated with support for disease control policies that might or might not require personal action, such as safe burial practices and domestic travel restrictions. Building upon this nascent research, the present study explored if trust in domestic institutions is associated with U.S. residents’ support for travel restrictions on foreigners during the COVID-19 pandemic.
It is worth noting that in extant studies, such as the ones reviewed, trust in domestic institutions is typically measured in relation to an all-encompassing concept, such as “the government” (Blair et al., 2017; Quinn et al., 2009; van der Weerd et al., 2011) or “the authorities” (Prati et al., 2011; Rubin et al., 2009). However, in light of the divergent responses from different government agencies in the United States during the COVID-19 pandemic, it is important to measure institutional trust in relation to a well-defined authority rather than using an all-inclusive term. The current study focused on trust in Trump as a predictor of support for travel bans, as he was the authority who directly issued these bans through presidential proclamations:
RQ2: Is support for entry restrictions on foreigners during the COVID-19 pandemic associated with trust in President Trump?
There is an emerging recognition that trust in institutions other than domestic authorities can also shape public response to international outbreaks, but the small number of studies on this topic have generated inconsistent results. For example, Blair et al. (2017) found no association between preventive behaviors and trust in international nongovernmental organizations (e.g., the American Red Cross, Médecins Sans Frontières) active in providing care and health education in Liberia during the 2014 to 2015 Ebola epidemic. In contrast, Bayram and Shields (2021) found that trust in the WHO was positively related to U.S. residents’ compliance with public health recommendations during the COVID-19 pandemic. To contribute to this expanding knowledge, the present study explored:
RQ3: Is support for U.S. entry bans associated with (a) trust in the WHO, and (b) trust in the Chinese government?
The Chinese government is the foreign government impacted by the first-ever U.S. travel ban in response to COVID-19, and the WHO is the principal UN agency responsible for issuing advice related to global travel, trade, and other exchanges during large-scale outbreaks. Therefore, U.S. residents’ trust in these two institutions may carry special weight in influencing their support for international travel restrictions.
Prior to assessing the association between multilevel institutional trust and policy support, one remaining question is the relationship among trust in different institutions. Research suggests that most Americans have limited knowledge of foreign organizations and their scope of work (Bayram & Shields, 2021). Consequently, an individual’s assessment of these institutions can be shaped by their level of general institutional trust (i.e., a trait to be more or less trusting of all institutions) as well as their trust in domestic authorities (i.e., trust in domestic authorities can spill over onto foreign authorities with aligned missions) (Muñoz et al., 2011). In other words, trust in the U.S. President, trust in the WHO, and trust in the Chinese government are likely to be related to one another. However, it is unclear whether they remain three distinctive constructs, or they represent one underlying construct only. Therefore, the present study investigated:
RQ4: Do trust in the U.S. President, trust in the WHO, and trust in the Chinese government represent three distinctive constructs during the early phases of the COVID-19 pandemic?
If trust in these institutions constituted distinctive constructs, it is then of interest to explore whether the relationship among them changes when a domestic authority becomes increasingly vocal in calling external institutions untrustworthy, as in the case of Trump’s escalating disapproval of the WHO and Chinese government during the COVID-19 pandemic.
RQ5: Does the relationship among trust in the U.S. President, trust in the WHO, and trust in the Chinese government change as the U.S. President becomes increasingly critical of the other two institutions?
Method
Participants and Procedure
Two cross-sectional online surveys were conducted in 2020 (between March 19 and March 27, and between April 30 and May 13) to understand U.S. residents’ responses to the evolving COVID-19 pandemic. March 19 marked the beginning of the U.S. “lockdown,” with California announcing the country’s first statewide stay-at-home mandate to decelerate disease spread (A. Lee, 2020). At this point, there were nearly 20,000 confirmed cases of COVID-19 and almost 200 officially recorded deaths nationwide (The COVID Tracking Project, 2020). By May 13, when data collection for the second survey was completed, there were almost 1,400,000 cases and over 79,000 deaths nationally.
Survey participants were recruited through Qualtrics Online Panels. A target of 500 participants was set for each survey, as power analysis using G*Power version 3.1.9.7 (Faul et al., 2009) suggested that a minimum sample size of 277 would be required to detect an effect size of 0.15 at the level of 0.05 with 95% statistical power. Qualtrics invited respondents from all 50 states and the District of Columbia to partake in the study, and quotas were set based on 2010 U.S. Census data to ensure sufficient representation of ethnic minorities and of both sexes in the samples. The two surveys started with the screening question “Do you currently live in the United States?” All respondents answered yes to this question and were eligible to continue with the study (n = 511 and n = 522 for the first and second surveys, respectively). The second survey also included an item to identify those who were diagnosed with COVID-19 (25 cases) or believed they might have it but did not get tested (25 cases). These 50 cases were removed from subsequent analyses given HBM’s focus on future expectancy, resulting in a final sample of 472 for the second survey. Individuals in the samples were older and more highly educated than the general population (see Table 1 for sociodemographic characteristics of the samples).
Sample Sociodemographic Characteristics in Comparison to the 2010 Census.

Measures
The outcome variable “support for entry restrictions on foreign visitors” was measured on a 10 point-scale (1 = not at all supportive, 10 = extremely supportive). The HBM constructs were measured by items adapted from Chen (2015). Perceived susceptibility was measured by asking participants how likely they were to catch COVID-19 on a 10-point scale (1 = not at all likely, 10 = extremely likely), and perceived severity was assessed as the extent to which respondents felt that their usual activities would be disrupted if they became ill with COVID-19 (1 = not at all disrupted, 10 = extremely disrupted). Perceived benefits were measured by asking respondents how effective they considered the travel restrictions to be in preventing widespread transmission of COVID-19 in the United States (1 = not at all effective, 10 = extremely effective). Perceived barriers were operationalized by asking how much participants agreed that suspending the entry of foreigners into the United States (a) is an unwarranted infringement on personal liberties and (b) will have negative political or economic impacts on the United States (1 = strongly disagree, 5 = strongly agree). Interpersonal cues were measured by asking participants if they knew anyone who had been affected by the entry bans. Individuals with an affirmative response were coded as “1,” and the rest was coded as “0.”
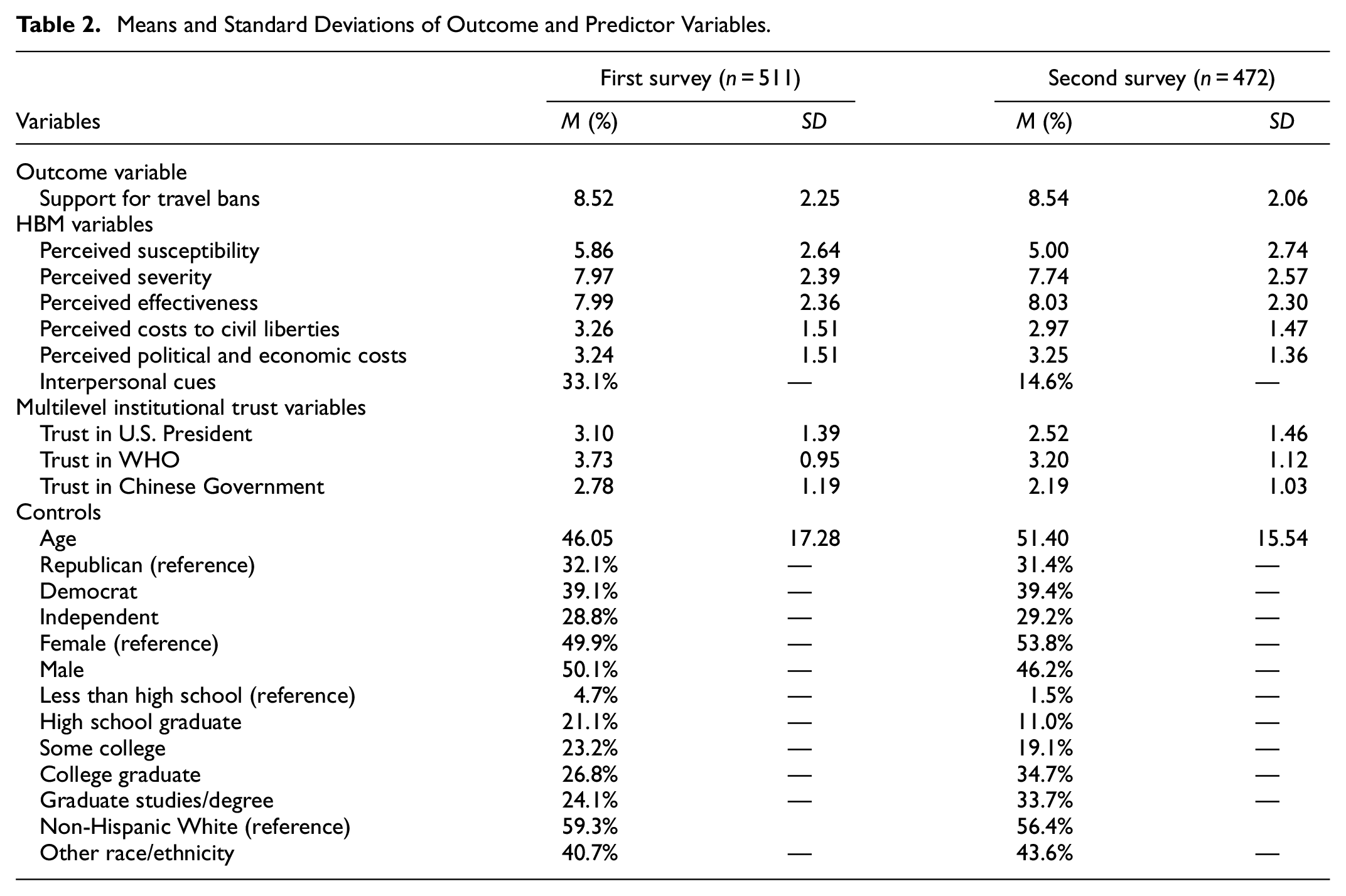
Three items adapted from Chen (2015) were used to measure institutional trust in the U.S. President, the WHO, and the Chinese government, respectively). Survey respondents indicated their level of agreement with three statements on how each institution was responding to COVID-19 on a 5-point scale (1 = strongly disagree, 5 = strongly agree): (a) [the U.S. President/ WHO/ Chinese government] can be trusted to do what is right during the COVID-19 outbreak, (b) [the U.S. President/ WHO/ Chinese government] is open and honest in communicating information during the COVID-19 outbreak, and (c) [the U.S. President/ WHO/ Chinese government] is well prepared to respond to the COVID-19 outbreak). Finally, age, sex, race/ethnicity, education level, and political affiliation were included as control variables. In subsequent analyses, age was entered as a numerical variable, whereas female, non-Hispanic White, less than high school education, and Republican served as the reference categories (see Table 2 for descriptive statistics for all measures).
Means and Standard Deviations of Outcome and Predictor Variables.
Analysis
To investigate the number of construct(s) underlying the nine items used to measure multilevel institutional trust in each survey (RQ4), exploratory factor analyses were conducted using SPSS 28. Principal component analysis with promax oblique rotation was performed, as any components identified were assumed to be correlated. The eigenvalue for extraction was set at 1, and the factor loading cutoff was set at <0.7 (Holroyd et al., 2021). Cronbach’s α coefficient was calculated to evaluate the internal consistency of each set of survey items identified to measure the same construct.
To test the significance, strength, and direction of the relationship among the latent variables identified (RQ5) as well as between the latent variables and their indicators, confirmatory factor analyses using structural equation modeling were conducted in AMOS 28. To assess the fit of each measurement model, the chi-square statistic was used. Given the sensitivity of the χ2 statistic to sample size, a χ2 to degrees-of-freedom ratio of 5 or smaller was considered a satisfactory fit. The GFI and RMSEA were also examined, with GFI values >0.90 and RMSEA values ≤0.08, representing a good fit. Finally, the significance of individual parameters was assessed, with the significance level set at p < .05. To answer RQ1, RQ2, and RQ3, linear regression analysis was performed in SPSS using data from the first and second surveys, respectively, with the significance level for all statistical tests set at p < .05. The adjusted R2 statistics were inspected to ascertain the extent of variance in the outcome variables explained by the regression.
Results
The exploratory factor analysis identified three factors underlying the survey items measuring multilevel institutional trust in each survey, with their respective eigenvalues being 3.89, 2.27, and 1.51 for the first survey, and 3.67, 3.01, and 1.08 for the second. The three factors explained a substantial proportion of the variability in the items (85% for the first survey and 86% for the second). In both surveys, the three factors reflected the constructs of trust in the U.S. President, trust in the WHO, and trust in the Chinese government. The factor loadings for all survey items were above 0.80 (see Table 3 for factor loadings).
Factor Loadings for Multilevel Institutional Trust Measurement Models.

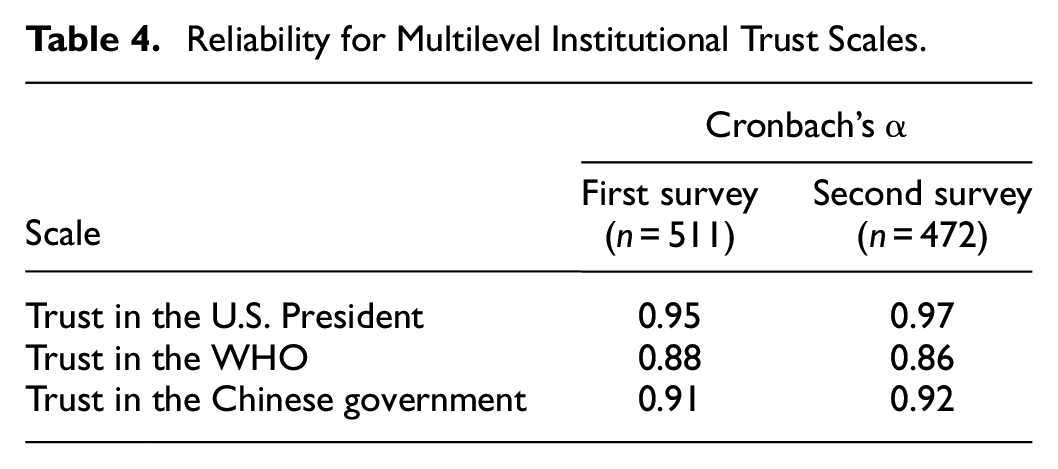
The Cronbach’s α for the items measuring trust in the U.S. President, the WHO, and the Chinese government, respectively, were also computed for both surveys, with reliability values ranging between .86 and .97 (see Table 4 for Cronbach’s α). These results suggest that multilevel trust consistently represented three distinctive constructs rather than a single underlying construct (RQ4).
Reliability for Multilevel Institutional Trust Scales.
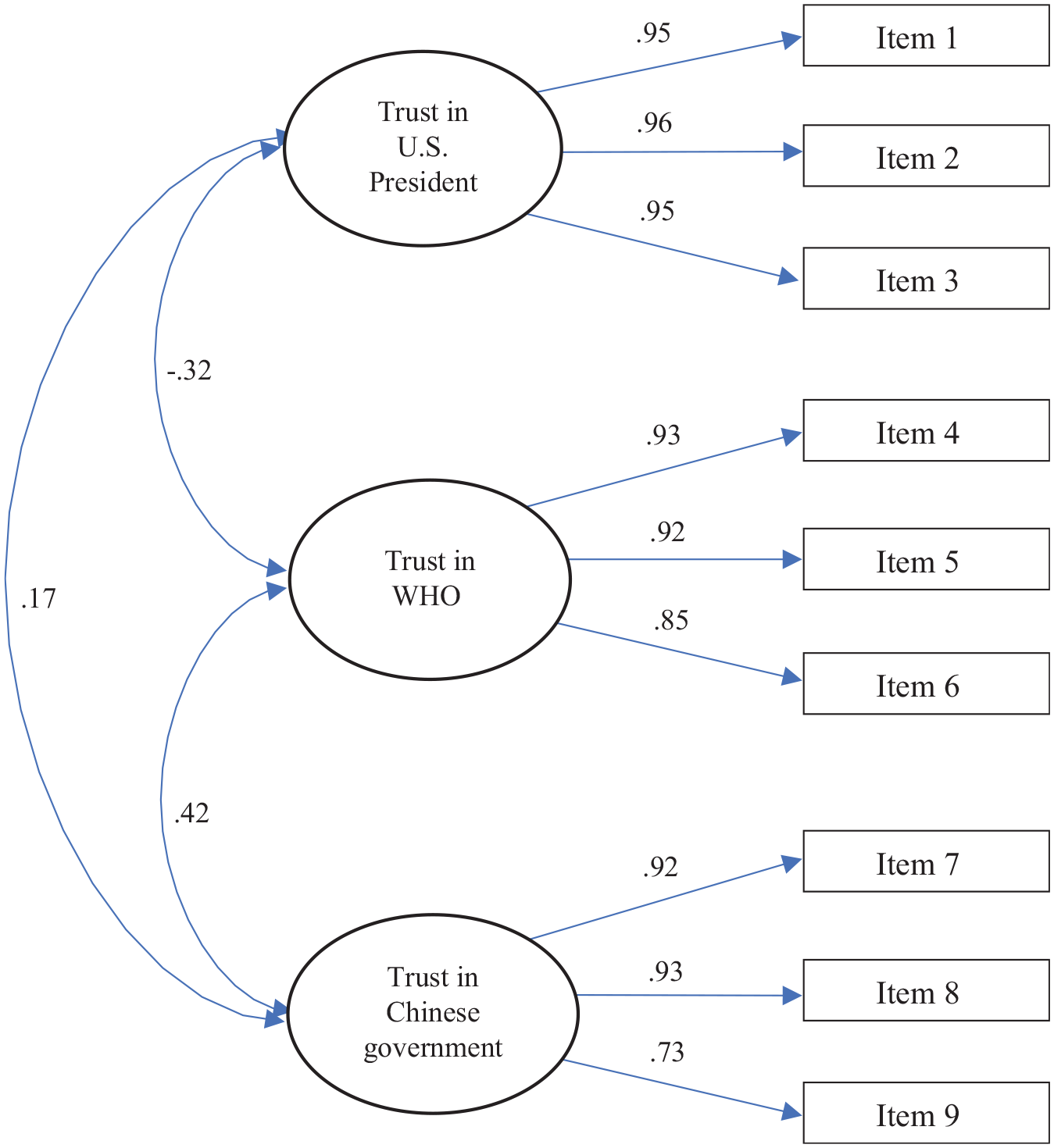
Next, confirmatory factor analyses indicated a satisfactory fit of the three-factor measurement model to the data (χ2/df = 3.56, GFI = 0.96, RMSEA = 0.07 for the first survey; χ2/df = 3.96, GFI = 0.95, RMSEA = 0.08 for the second survey). All correlations between the latent variables and their indicators, as well as all correlations among the latent variables, were statistically significant (see Figures 1 and 2 for correlations among the variables). For the first survey, trust in the U.S. President had a slight positive correlation with trust in the WHO (r = .13) and a low positive correlation with trust in the Chinese government (r = .29). A moderate positive association was found between trust in the Chinese government and trust in the WHO (r = .40).

Standardized estimates from confirmatory factor analysis for the multilevel institutional trust measurement Model from the first survey.
Standardized estimates from confirmatory factor analysis for the multilevel institutional trust measurement model from the second survey.
For the second survey, trust in the U.S. President continued to have a slight positive correlation with trust in the Chinese government (r = .17); however, its correlation with trust in the WHO was now negative (r = −.32). There remained a moderate positive association between trust in the Chinese government and trust in the WHO (r = .42). These results suggest that while trust in multilevel institutions was consistently correlated, the direction and strength of these relationships were not static (RQ5).
To investigate which multilevel institutional trust variables and HBM components were associated with support for the entry bans, regression analyses were performed on data from the first and second surveys, respectively (see Table 5 for both the unstandardized and standardized coefficients from the regression analyses).
Predictors of Support for Entry Restrictions on Foreigners.

p < .05, **p < .01, and ***p < .001 (two-tailed tests).
For the first survey, the model accounted for 47% of the variance in the outcome variable, and the following HBM variables were significantly associated with policy support (RQ1): perceived effectiveness of travel restrictions (β = .53, p < .001), perceived severity of COVID-19 (β = .13, p < .001), perceived susceptibility to COVID-19 (β = .08, p = .03), and interpersonal cues (β = −.13, p < .001). Among the multilevel institutional trust variables, trust in the U.S. President (β = .03, p = .43) did not contribute significantly to policy support, thus addressing RQ2. Regarding the role of trust in intergovernmental and foreign institutions (RQ3), policy approval was significantly and negatively associated with trust in the Chinese government (β = −.10, p = .02) but unrelated to trust in the WHO (β = .07, p = .06).
For the second survey, the model accounted for 43% of the variance in the outcome variable, and the following HBM variables were significantly associated with policy support (RQ1): perceived effectiveness (β = .53, p < .001), perceived severity (β = .20, p < .001), and interpersonal cues (β = −.09, p = .02). Among the multilevel institutional trust variables, trust in the Chinese government (β = −.11, p = .01) and trust in the U.S. President (β = .09, p = .047) were both significantly associated with policy support, whereas trust in the WHO did not contribute to the outcome variable (β = −.02, p = .65). These findings helped answer RQ2 and RQ3.
Discussion
In this era of globalization, it is vital to understand what motivates individual support for disease control measures that impact cross-border exchanges and fundamental human rights, such as international travel restrictions. There is limited research in this area, as extant literature tends to focus on preventive measures that require personal action. The present study is one of the first to explore psychological factors associated with support for travel bans on foreigners, a policy that does not require local residents to modify their behavior in any way. By analyzing data collected at two points during the early phases of the COVID-19 pandemic, this study found that U.S. residents’ support for the travel bans was associated with individual differences in risk and benefit perceptions, the presence of interpersonal cues, and trust in certain domestic and foreign institutions. Individuals who believed that contracting COVID-19 would seriously disrupt their lives (i.e., perceived severity) and considered the entry bans effective in controlling disease spread (i.e., perceived benefits) were consistently more supportive of this policy. On the other hand, respondents were less supportive if they knew someone—family, friend, or acquaintance—who was affected by the entry bans (i.e., interpersonal cues).
Furthermore, individuals reporting greater susceptibility to COVID-19 were more approving of entry restrictions during the first survey, but not the second survey. Between the first and second surveys, the United States moved from being largely free of confirmed cases to the global epicenter of the pandemic. It is plausible that as the U.S. public moved away from perceiving COVID-19 as an exotic and foreign disease to considering it common and domestic, individuals with varying levels of perceived susceptibility to COVID-19 no longer differed on their support for the travel bans on foreigners.
Perceived barriers constituted the only HBM construct not associated with policy support in both surveys. As the costs of the entry bans were operationalized in terms of their civil liberty, political, and economic ramifications for the United States, it is plausible that when the costs of a public health measure are more abstract and less personal, they no longer serve as a primary consideration in judgment making. However, it is not necessary for people to personally experience the negative impact of a public health strategy to object to it. This study found that individuals were less supportive of travel restrictions if they knew someone affected by such policies. In other words, even when individuals are not directly inconvenienced by a health measure, they may consider it unfavorable when cues that concretize or humanize its costs are available.
Beyond the systematic cost-benefit analysis posited by the HBM, this study investigated the role of multilevel institutional trust as a heuristic in shaping policy support and explored the relationship among trust in different institutions. Data analyses indicated that individuals’ trust in the U.S. President, the WHO, and the Chinese government constituted three distinctive concepts with evolving relationships during the COVID-19 pandemic. To elaborate, data collected in March 2020 suggested that U.S. residents with greater trust in President Trump were also more trusting of the WHO and the Chinese government. However, as Trump became increasingly critical of these external institutions, individuals with higher trust in the U.S. President were found to be less trusting of the WHO by May 2020. Interestingly, people with greater faith in Trump continued to report higher trust in the Chinese government. One possible explanation is that the Chinese government has been a fixture in the media and political discourse in the United States (Jones et al., 2013; Pew Research Center, 2022). Therefore, people’s attitudes toward Chinese authorities are more entrenched and less subject to influence from recent political rhetoric. On the other hand, the WHO typically does not receive much public attention in the United States. Without a strong preexisting attitude, people’s trust in this organization is more malleable to influence from recent political discussions and events. Consequently, the WHO and similar intergovernmental organizations might benefit from strategies that help enhance their visibility and advance their relationships with a global audience during “peacetime,” if they are to maintain credibility in times of crisis, especially when they became a target of criticism.
Furthermore, the results of this research suggest that trust in the WHO does not hold sway over U.S. residents’ support for international travel restrictions. For both surveys, trust in the WHO was not associated with policy support. One plausible explanation is that many individuals were unaware of the WHO’s opposition to international travel restrictions and thus did not apply trust in the organization as a judgment-making heuristic. Given the WHO’s charge to serve as the premier intergovernmental agency for coordinating global health policy within the UN framework, it is imperative to make its advice and decision-making rationale more widely known during international outbreaks. This is especially important because the inherent tension between the WHO’s priorities and national interests is bound to manifest in some policy differences (e.g., when it comes to disagreement over global travel restrictions, or the distribution of COVID-19 booster shots in wealthy nations when other countries have yet to acquire enough initial doses to immunize their populations; Rackimuthu et al., 2022; WHO, 2021a). The WHO may benefit from securing and committing more resources toward communication with national governments and members of the global public. This communication should aim to promote mutual understanding between the organization and its constituencies, and to identify ways in which compromises can be reached to advance their shared goals.
On the other hand, greater trust in the Chinese government was linked to lower support for entry restrictions in both surveys. For the second survey, participants more trusting in President Trump were also more approving of the entry bans. These findings underscore the importance for national governments to develop trust with not only their own citizens but also with foreign audiences, as distrust in foreign governments can make citizens more supportive of policies that constrain cross-border exchanges. A wealth of literature already exists to inform government efforts in trust building with domestic constituencies in order to facilitate effective pandemic response (Siegrist & Zingg, 2014). National authorities can also look to emerging discussions on how they can use mediated and more direct policy diplomacy strategies to strengthen their credibility overseas during a pandemic (S. T. Lee, 2021; S. T. Lee & Kim, 2021).
In conclusion, this study suggests that the HBM, together with multilevel institutional trust, provides a useful theoretical framework for understanding support for international travel restrictions during the COVID-19 pandemic. In terms of practice, policymakers and advocacy groups can consider the influence of perceived benefits, perceived severity, and interpersonal cues on policy support. That is, by publicizing the benefits of international travel restrictions and the severity of the disease they help prevent, proponents may shore up public support for this policy. On the other hand, oppositional messages may become more effective when the focus is shifted from the less tangible costs of international travel restrictions (e.g., impacts on national economies, civil rights violations) to the questionable effectiveness of such restrictions when not complemented by appropriate domestic public health measures. Furthermore, because people are less likely to support travel bans if they knew someone affected by them, publicizing personal stories that humanize the negative consequences of entry restrictions (e.g., prolonged family separation) may help promote empathy and motivate people to reconsider their stance.
One limitation of this study is that institutional trust was measured in relation to a particular U.S. president vis-à-vis two impersonal foreign establishments (i.e., the WHO and Chinese government). While recognizing the merits of measuring trust in a domestic equivalent (e.g., the U.S. government) to these external institutions, the drawbacks of this approach would outweigh its merits due to the divergent and sometimes conflicting responses to COVID-19 within the U.S. government during the early phases of the COVID-19 pandemic. This lack of coordinated responses created problems for measuring trust in an all-inclusive “U.S. government.” A decision was therefore made to measure trust in the Trump administration instead to provide cognitive clarity to research participants. One question stemming from this methodological approach is whether U.S. residents’ trust in the leadership of a foreign institution (e.g., the Director-General of the WHO or President Xi of China) would also differ from their trust in the institution that the leader oversees. It is plausible that given the research findings on U.S. residents’ limited knowledge on foreign institutions (Bayram & Shields, 2021), individuals’ trust in the leadership of a foreign organization would not diverge significantly from their trust in the institution itself, unless there is widely publicized internal conflict within the organization. However, this hypothesis remains to be tested empirically in future research.
Another limitation of the current study is that the data were collected from two nationwide cross-sectional surveys conducted in the United States using quota sampling. While it is encouraging to find most HBM variables and trust in the Chinese government consistently associated with individual support for travel restrictions, these findings need to be validated through future studies with nationally representative samples and a panel design. Future investigations should also seek samples from other countries to assess the generalizability of this study’s results, given that each national government has a different relationship with the WHO and with other nation-states, and in light of the varying disease burdens of COVID-19 across countries. Inevitably, individuals’ reactions to public health crises are shaped by their social, political, and economic contexts. As more contextualized studies become available, researchers may start developing a framework that explicates the role of health beliefs and multilevel institutional trust in influencing individual support for cross-border disease control measures under different macro-level conditions.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Minigrant from the Center for Integrative Studies at California State University Channel Islands and the CSUCI Provost’s Direct Costs Grants for Research and Creative Activities.
Ethical Approval
All procedures performed in this study involving human participants received prior approval from the Institutional Review Board at California State University Channel Islands (approval number #IO5525), and the study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants. They were provided with an electronic information sheet prior to completing the online survey and were required to electronically consent to participation.
Data Availability Statement
Data from this study may be shared upon request to the author.