
Abstract
Recognizing the importance of prevention during a highly transmissible disease like COVID-19, this study analyzed the effect of health psychological capital and health appraisals (benefits, barriers, contextual threat, seriousness and susceptibility) on voluntary adoption of preventive behavior. The theoretical framework was based on health belief model. The study also proposed the mediating role of health appraisals between health psychological capital and preventive behavior. Participants from Pakistan (N = 321) and Malaysia (N = 343) completed an online survey. Samples from both countries were compared for measurement model invariance and variance in path coefficient. Partial least squares approach to SEM using SMART-PLS3 software was adopted to analyze the measurement model, structural model, importance-performance analysis, and mediation testing. Our finding showed that the model explained a higher variance in preventive behavior for Pakistani samples compared to Malaysian samples. Countries were found to moderate some of the proposed relationships. Benefits and threats are the two most important predictors of preventive behaviors in both countries. Psychological capital is more predictive of coping and threat appraisals and is, directly and indirectly, related to preventive behavior via benefits, barriers, and threats in Pakistani sample, and only indirectly related to preventive behavior via benefits and threats in the Malaysian sample. Perceived threat also mediates the relationship of susceptibility and seriousness with preventive behavior. Public health messages should focus on enhancing health psychological capital, highlight the potential benefit and emphasize the perils of not adopting the precautionary approach.
Keywords
A new type of coronavirus, named SARS-COV-2, first appeared in Wuhan, China causing a pneumonia type respiratory ailment termed as COVID-19 (Holshue et al., 2020). Within few months, the virus had spread globally and as the disease is still ongoing, it has already caused most deaths by any pandemic in the 21st century (Roy et al., 2020). COVID-19 is highly transmissible disease as it can quickly spreads human-to-human when a healthy person comes within 6 ft of contact with an infected person either through nasal droplets or direct body contact (Lai et al., 2020). Whenever a threat of Pandemic lingers in the air, an individual faces two types of health challenges, (1) treatment and (2) prevention. Our research is more focused on the second type of health challenge, which is, how to minimize the chances of being getting infected in the first place using certain health protection behaviors. Previous pandemics which involve a highly communicable virus such as MERS (Middle East Respiratory Syndrome), SARS (Severe Acute Respiratory Syndrome), Swine Flu, H1N1 and now COVID-19 have taught us the importance of preventive measures observed by general public to reduce the spread of contagion and flatten the curve (Lin et al., 2020). Since its inception, the best available non-pharmacological tool to prevent the spread of COVID-19 contagion is for the individuals to follow the recommended infection control preventive measures. For COVID-19 the World Health Organization’s (WHO) recommended precautions are generally derived from previous experience of managing MERS and SARS infections (Lai et al., 2020). Some of the recommended behaviors to observe are; maintaining social distancing, hygiene etiquettes such as washing hands frequently, covering nose and mouth while sneezing, avoid touching mouth, nose, and eyes unnecessarily if hands are not washed and wearing a face mask when going out in the public. It is also suggested that infected individuals maintain social isolation so that they do not transfer the disease to others.
Adopting these preventive measures always require a large scale co-operation from the public and their voluntary participation in the prevention process (Seale et al., 2009). Ever since COVID-19 disease converted into an outbreak in Wuhan, China, there are continuous and rigorous media campaigns backed by the political authority for the awareness and course of recommended actions for the public. However, the masses often did not understand the gravity of the situation and showed a casual attitude in adopting social isolation and other preventive measures (Roy et al., 2020). For example, while community spread was in early stages in Malaysia and most of the cases were of foreign origin, a religious gathering that occurred at the end of February and attended by 16,000 people (including foreigners) in Kuala Lumpur. This gathering played a major role in the pandemic outbreak as more than half of confirmed cases, and most of the community spread cases trace to the event. Subsequently, Malaysia became the country with the highest number of cases in South East Asia early on (Ho & Mokhtar, 2020). The government was, after that, compelled to take an extreme measure by “imposing” the necessary lockdown, thereby halting the economic, social, and academic activities. Similarly, several instances have been reported in Pakistan when infected people avoided mandatory checks from the airport, or some foreign travelers managed to escape from quarantine facilities in Pakistan, causing an outbreak in their local community (Butt, 2020).
Our research probe into the notion that why do some people are more willing to follow recommended preventions while others are not? We seek to answer this question by adopting the Health Belief Model (HBM) as the conceptual framework. We expand the HBM by exploring the relationship between psychological capital, various health and prevention from COVID-19 related perceptions and preventive behavior. Although several studies have explored the HBM model in the context of a pandemic regarding preventive behavior and vaccination willingness (Brewer et al., 2007; Green et al., 2010; Murray et al., 2013; Rubin et al., 2009; Scherr et al., 2016), research on the impact of positive and developable personality characteristics on health appraisals and preventive behaviors remains limited. Scherr et al. (2016) explored a two-dimensional model of dispositional pandemic worry as a predictor of vaccination intention of the H1N1 pandemic. They found that worry frequency was positively related to vaccination intention with mediating role of threat, benefits, and barriers. Similarly, they discovered that worry severity was also related to vaccination intention with mediating role of threat and barriers. Our study, however, took a more positive approach and contributed to the existing literature by examining the health-related implications of psychological capital with the focus on preventive behaviors for COVID-19 with parallel mediating roles of health perceptions.
We have conducted this study in, Pakistan and Malaysia, to explore cross cultural differences in proposed relationships. Understanding cross-cultural differences in the adoption of preventive measures is crucial to tailor effective strategies that consider cultural norms, beliefs, and behaviors for better public health outcomes. The insight into how positive personality resource of psychological capital influence health appraisals and preventive behavior is important for the success and adoption of precautionary measures against the spread of COVID-19. Findings of our study can help public health decision makers to enhance the efficacy of risk communication messages and design wide-scale psychological intervention strategies to enhance the voluntary adoption of preventive behavior.
Related Literature and Framework Development
Health Belief Model
Health belief model is a widely employed health psychology framework that is used to explain the determinants of preventive health behavior among the people (Rosenstock, 1974). Many studies have adopted HBM to investigate a range of behavior during flu pandemics, including pre-emptive screening, getting vaccinated, compliance with recommended precautions, and response to disease symptoms (Bish & Michie, 2010). According to the classic HBM, any stimulus which concerns an individual health may influence two types of appraisals or beliefs in a person; risk appraisal, and coping appraisal. The risk appraisal is a more reactive appraisal in which the person will not strive to prevent a negative health outcome until they feel endangered such as fear of getting ill due to current health condition or threat of getting infected by a pandemic (Seale et al., 2009; Zak-Place & Stern, 2004).
Generally, the level of perceived risk for any health-related danger is assessed by two dimensions, perceived susceptibility (susceptibility) and perceived seriousness (seriousness). According to Kirscht et al. (1966), if people believe that they are vulnerable to get sick or they appraise that the disease have serious repercussions of their health, they are likely to adopt health-seeking behavior. A meta-analytic study of HBM literature found that people’s perception of likelihood, seriousness, and susceptibility was strongly related to their decision to get a vaccination against infectious disease (Brewer et al., 2007). In prior studies on willingness to adopt protective behaviors to reduce the risk of getting infected with SARS, the seriousness of perceiving the Pandemic as risk and likelihood of contracting disease were central determinants (Cava et al., 2005; Leung et al., 2005). Therefore, we expect that individual’s perception of how serious COVID-19 is, and appraisal of susceptibility to get infected by the virus is positively related to adoption of preventive behavior.
Classical HBM do not include perceived threat as a separate construct. Rather a combination of seriousness (or severity) and susceptibility is often collectively termed as threat appraisal (Champion & Skinner, 2008), because both these represents a threat to one’s health. However, there are many studies which have investigated perceived contextual threat of disease as a conceptually distinct constructs and found that people who feel threatened by spread of pandemic are cautious and tend to avoid potential disease spreading elements (Green et al., 2010; Murray et al., 2013; Scherr et al., 2016). McKellar and Sillence (2020) mentioned perceived threat as one of the mediators in HBM model, yet there is scant empirical research which has included seriousness, susceptibility and threat of pandemic within a single HBM framework. Considering the theoretical overlap between these constructs, it is expected that people’s appraisal of how “serious” COVID-19 pandemic is and the extent to which they are “susceptible” to get infected further transforms into threat appraisal which positively influences their tendency to adopt preventive behaviors (Champion & Skinner, 2008). Therefore, we also propose that perceived threat is positively related to preventive behavior and mediates relationship between risk perceptions (seriousness and susceptibility) and preventive behavior.
People can also develop two types of coping appraisals; perceived benefits (benefits) and perceived barriers (barriers) of preventive behavior. Previous research on women’s likelihood to screen for breast cancer revealed that if they believed that mammograms are unlikely to detect cancer, they would prefer not to schedule an appointment (Hyman et al., 1994). A study carried out in the UK post swine flu pandemic found that people who felt that preventive behavior is beneficial for them were more likely to report handwashing, wearing masks, and other precautionary behavior (Rubin et al., 2009). Another study concluded that some women did not opt for mammograms test even they believed it would deduct cancer because of the related pain with the procedure (Hyman et al., 1994). A barrier to adopt preventive behavior during COVID-19 can be because of the social, professional or economical sacrifices that needs to be made to observe the required behavior. Therefore, we propose that higher perceived benefit and lower perceived barriers of COVID-19 precautions is associated with higher performance of preventive behavior.
Health Psychological Capital
F. Luthans and Youssef (2004) proposed psychological capital (PsyCap) as a higher-order personality type composed of four personality types of self-efficacy, hope, resilience, and optimism. The reason these four personality types were chosen because they are firmly established in existing literature, have established measures, are malleable in nature and have strong relationship with multiple attitudes and behaviors. An optimistic person considers that positive events in life happen due to personal, permanents and pervasive factors and negative events are attributed to external, temporary and contextual factors (M. E. Seligman, 2000). Self-efficacy is one’s believe about capacity and capabilities to organize and execute a specific course of action to perform a task (Bandura, 1997). Hope is defined as a positive motivational state which determine pathways that leads to desired goals and agentic forces which utilizes the pathways efficiently to achieve a goal (Snyder et al., 2002). Finally, resilience is defined as a reactive psychological capacity to overcome the failures, setbacks, and adversities in life; and having the ability to bounce back by striving to reacquire what is lost (F. Luthans & Church, 2002). What makes PsyCap a unique personality type is the state-like and malleable nature of its constituents which means an individual’s PsyCap can be developed by interventions to achieve the desired behavior (F. Luthans & Youssef-Morgan, 2017).
PsyCap was primarily proposed to serve as an organizational based personality type under the umbrella of positive organizational behavior (F. Luthans, 2002). Later it was extended to other domains such as academic, relationship, and health (B. C. Luthans et al., 2014; F. Luthans et al., 2013). It is argued that domain specific PsyCap (e.g., health PsyCap) relates to satisfaction in that domain (e.g., health satisfaction) which in turn enhances overall wellbeing leading to even higher levels of positive personality resource of overall PsyCap in life. Drawing from the positive cognitive resources of four underlying personality types, people high in health PsyCap would have a positive appraisal of health-threatening situations and a higher tendency to show motivated effort and perseverance to achieve success in health outcomes (F. Luthans et al., 2013).
There are number of pathways through which PsyCap can influence preventive behavior. First, it is directly related to individual’s adoption of preventive measures for COVID-19. Previous studies exploring the effect of positive psychological states on mental and physical health suggests that people with greater optimism and efficacy are more likely to devote efforts on health-promoting behavior and prevention strategies (Taylor et al., 2000). It is found that health PsyCap is a negative predictor of a person’s cholesterol levels and body mass index and a positive predictor of satisfaction with one’s health (F. Luthans et al., 2013). Previous literature has also shown a close association between individual constituents of PsyCap and health-related outcomes. Self-efficacy is consistently found to predict the initiation and perseverance of complex health maintaining behaviors (Holden, 1992). Self-efficacy was also added as a determinant in later models of HBM as an expectation from one-self to execute the preventive behavior successfully. Evidence also exists that people with higher hope (Scioli et al., 1997) and optimism (Peterson & Bossio, 1991) act more healthfully. Although resilience is not directly related to traditional health constructs, more resilient people have shown to better tendencies to receive treatments, take a more protective health approach, and have better coping with health threats (Holaday & McPhearson, 1997; Sandau-Beckler & Devall, 2002). Acting in synchrony, the four underlying personality characteristics of the health PsyCap would activate a self-directed health management mechanism within the individual, which according to B. C. Luthans et al. (2014) would be greater than each component alone. Therefore, we propose a direct relationship between health PsyCap and preventive behavior.
Second, we also believe that health PsyCap would be indirectly related to preventive behavior via the mediating mechanisms of five health belief perceptions of barriers, benefits, seriousness, susceptibility and threat. Theoretically, health PsyCap would act as a key resource within the proposed HBM model. A key resource is that influential psychological characteristic which controls, collect, and modify other resources as well as play a crucial role in managing and coping with various stressors (Thoits, 1994). People who are high in key psychological resources when face external stressor do not panic and have lower stress because their belief system makes them take a positive outlook of the situation. Although previous research has not explored relationship of PsyCap with five health appraisals constructs, studies have shown that people high in PsyCap develop those appraisals which makes them feel more resourceful and helps to develop effective coping strategy to handle the external stressful situations thus enabling them to attain well-being and other positive outcomes (Dorsch et al., 2017; Grover et al., 2018). For instance, Grover et al. (2018) tested PsyCap as a personality resource within Job Demands Resources model. They found that PsyCap positively influenced employee’s perception of job resources and diminished the perception of demanding job characteristics. Furthermore, job demands and job resources also mediated the link between PsyCap and subjective well-being and between PsyCap and job engagement.
In the same manner we expect that individual who possess higher PsyCap would be more engaged in preventive behavior because they feel more prepared and resourceful to overcome the obstacles, they may face in adopting those preventions that may protect them from COVID-19. Therefore, we propose that PsyCap indirectly relates to preventive behavior by diminishing perceived barriers. People with positive personality resources have stronger sense of self-worth (Taylor et al., 2000) and are more cautious of their health (Krasikova et al., 2015), they are expected to develop appraisal that adopting preventive behavior is beneficial for them because it is can save them from the disease. So, we propose that perceived benefits mediate the PsyCap-Preventive behavior relationship. Since it is established that COVID-19 is extremely contagious, spreading at unprecedented rates and everyone is vulnerable to this disease (Holshue et al., 2020), people high in health PsyCap would take this disease as a serious concern, feel susceptible to fall ill and are thus threatened by the spread of contagion. Therefore, it is proposed that susceptibility, seriousness and threat would mediate the relationship between PsyCap and preventive behavior. Figure 1 depicts the schematic diagram of the proposed relationships.

Schematic diagram of proposed relationships.
Methods
Participants and Data Collection
This is a cross-sectional study, and primary data was collected from Pakistan and Malaysia using a self-administered online survey. The survey was designed using a GOOGLE survey, and participants were selected through the snowballing technique. A weblink was circulated through WhatsApp to the diverse contacts of the authors in their respective countries. They were also requested to circulate the survey link to their contacts within the country. Since COVID-19 pose equal threat to everyone due to its highly contagious nature, we did not confine our study to any specific segment. All personals above 18 years of age, able to understand English and residents of the respective countries (Pakistan and Malaysia) were eligible respondents. We used snowball sampling to maximize data collection since we had allocated only 2 days for this process. The reason to allocate a limited time for data collection was an attempt to keep the environmental context homogenous. We believed that the rapid escalation of the Pandemic in both countries as well as globally would have had a confounding effect on the research model. On average, the survey took 15 min to complete.
The survey started with an introduction to the research and an informed consent statement. We guaranteed our participants anonymity and privacy of their response and utilization of data as aggregate. They were advices to skip a question or leave the survey incomplete if they feel uncomfortable. To ensure freedom of responses, we did not impose any software-based compulsions on questions. The study was ethically reviewed and approved by the Ethical Review Board of Faculty of Education, Allama Iqbal Open University (AIOU) Islamabad, Pakistan. The questionnaire was administered in English as it is the lingua franca of academic circles in both countries.
In Pakistan, we conducted surveys from 26th March 2020 to 28th March 2020. By the cut off time, we had received 348 responses. In Pakistan, the first case of the COVID-19 was reported on February 27. The government took various prompt actions such as the closure of educational institutes, banning congregational based activities, restricting flights, and launching a national wide media awareness campaign. On 26th March, there were1,197 cases in Pakistan with a death toll of 9. In the next 2 days, the cases increased to1,526, with 13 deaths. During our data collection period, a mandatory lockdown was imposed throughout the country. As of 24th April, 2020 the total number of cases in Pakistan are 11,155 with a death toll of 237.
Data collection in Malaysia started on the morning of 28th March 2020, and by the cutoff date after 2 days (30th March 2020) we had received 349 responses. the first case was identified almost a month earlier on 25th January. However, there was a sudden spike in cases by early March linked to a religious event held in the last month of February at Kuala Lumpur. On 28th March, there were2,320 active COVID-19 diagnosed cases with 27 deaths. By 30th March, these cases had reached2,626, with 10 more deaths in the next 2 days. During the data collection time, a Movement Control Order was in place around the entire country, which restricted the unnecessary movements of people. The total number of cases in Malaysia on 24th of April, 2020 were5,603 with a death toll of 71.
Demographic Profile
We screened the data for missing responses (greater than 10% of total items), inconsistent responses, and participants who were not in the scope of the research (e.g., less than 18 years). The final sample size for Pakistan and Malaysia was 321 and 343, respectively. Data in Table 1. depicts the demographic profiles and descriptive of both countries.
Demographic Profiles and Descriptive Statistics of Sample From Both Countries.

Instruments
There were five determinants and one focal outcome in the study. Responses for five constructs, other than health PsyCap, were registered on a 4-point scale (1 = very little, 2 = somewhat, 3 = moderately, 4 = a lot). Items related to health PsyCap were registered on a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). The composite reliability values of the scales are mentioned in the measurement model analysis section.
Health PsyCap
We adopted the PCQ12 scale to assess the respondent’s health PsyCap. The PCQ-12 is a short form of PsyCap questionnaire which has three questions from the self-efficacy scale, four questions from the hope scale, three questions from the resilience scale and two questions from the optimism scale of. Although the original scale refers to work-place related PsyCap, we slightly rephrased them to refer to the health domain. For instance, a work hope item, “I can think of many ways to reach my work goals,” we replaced the phrase word “work” with “health-related.” The PCQ12 is available free from the author’s website www.mindgarden.com on special permission.
HBM Appraisals
We adopted and modified the items for susceptibility, seriousness, benefit, and barriers, from earlier scales developed by Champion and colleagues (Champion, 1984, 1999).
We measured perceived susceptibility with three items, which measures their likelihood of getting infected with a COVID-19 in general, if they have flu and pneumonia symptoms and according to their current health status. A sample item is, “How likely it is that you could become infected with COVID-19?”
We measured the perceived seriousness of COVID-19 with three items. A sample item is, “To what extent do you believe that COVID-19 is a hopeless disease with no treatment.” Other dimensions are; “not just a media hype,”“long-lasting impact.”
The benefit was measured with four items. We asked respondents about the potential benefit and usefulness of preventive actions. A sample item is “To what extent you think recommended preventive action for COVID-19 is useful”? other dimensions included; “reduction in the spread,”“reduce problem-related to disease,” and “keep safe from future health issues.”
We measured perceived barriers to adopt preventive behaviors with three items. We asked the respondent whether these preventive behaviors are practical, disrupts the social and professional life, and demands sacrifices. A sample item is: “To what extent you think preventive behavior for COVID-19 is practical?”.
To measure threat appraisal, we adopted a contextual threat questionnaire from Green et al. (2010) study on swine flu and modified it to COVID-19. There were four questions that asked respondents how much they are worried about the COVID-19, think about it, discuss with others, and pay attention to the information in media. A sample item is: “To what extent are you worried about COVID-19 pandemic?”.
Preventive Behavior
To measure preventive behavior, we followed the pattern of questions as used by Oh et al. (2021) in their study related to the SARS outbreak. Our scale for preventive behavior was based upon WHO recommended guidelines to keep safe from the COVID-19. These questions gauged individual frequency of behaviors such as social isolation, handwashing, avoiding public, wearing a mask in public, canceling travel plans, and compliance with government guidelines and policies. A sample item is: “To what extent has the threat of COVID-19 influenced your decisions to go out in public?”.
Data Analysis
We used IBM SPSS 25® for descriptive statistics and analysis of common method bias. A theoretical model was tested using partial least square structural equation modeling (PLS-SEM) in SMART-PLS 3® (Ringle et al., 2015) and WarpPLS Software (Kock, 2017). PLS-SEM offers a various advantage over more traditional co-variance-based SEM. First, it does not restrict data normality. Second, it can handle constructs with a low number of items. Third, it is more capable of handling complex models. Fourth, it does not suffer from the issue of factor indeterminacy. Moreover, various previous studies has shown that results from PLS-SEM and CB-SEM are comparable over various data sets (Hair, Matthews et al., 2017; Rigdon et al., 2017).
We tested two separate models for both countries. The testing was based on a two-step approach for testing an SEM model (Anderson & Gerbing, 1988). In the first step, the adequacy of the measurement model is analyzed for reliability (Composite reliability, >0.7), convergent validity (Average Variance Extracted; AVE, >0.5) and discriminant validity (Fornell-Larcker Criteria, square root of AVE of a construct > correlation with all other constructs). All the constructs in our model were modeled as reflective. We also conducted MICOM (measurement invariance of composite models) to check for measurement invariance between samples of both countries (Henseler et al., 2016).
In the second step, the structural model was analyzed for collinearity statistics, standardized regression coefficients (β), coefficient of determination (R2), and predictive relevance (Q2). Significance testing was done by bootstrapping (3,000 resample), which generated t-statistics for hypothesis testing. The existence of mediation was determined by bias-corrected and accelerated bootstrapping (BCa-CI) in which zero between lower confidence interval and upper confidence interval depicts non-significance (Hair, Hult et al., 2017). We also conducted multi-group analysis (PLS-MGA) to test for the moderating effect of countries on the results of path coefficients. All the above analyzes for measurement model and structural model along with MICOM was conducted using SMART-PLS 3. Finally, we calculated Tenenhause goodness of fit (GoF) index and Average Path Coefficient (APC) as indication of model fit using WarpPLS.
Results
Common Method Bias
Presence of common method bias was assessed using Harman’s single factor technique (Podsakoff et al., 2003). Principal axis factoring revealed that when all the items were loaded on a single factor, the variance explained was less than 50% (15.19% for Pakistan and 18.66% for Malaysia). We also checked for common method bias in SMART PLS using the approach suggested by Kock (2015). In this method the variance inflation factor (VIF values) of each latent construct is tested by making it dependent variable and loading all other latent factors on it. Our results depicted that VIF values in all cases were less than the cut off value of 3.3. Hence common method bias is not a problem in the study.
PsyCap as a Higher-Order Construct
We modeled Health PsyCap as a second-order reflective construct and followed a two-step approach of hierarchical linear modeling (Hair, Hult et al., 2017). In the first step, which is a repeated indicator approach, all items were assigned to the sub-dimension and main construct in a repeated manner. The four dimensions, self-efficacy, hope, resilience, and optimism, were linked to higher-order PsyCap in reflectively. As shown in the Figure 2, all the respective items had loadings of greater than 0.70 on their respective sub-dimension, which in turn had a strong loading (Path coefficients >0.70) on the second-order dimension. Besides, the R2 of each dimension was greater than the recommended value of .50. The sub-dimension also had adequate reliability (minimum composite reliability = 0.84), convergent validity (minimum AVE = 0.64) and discriminant validity. We saved the latent values of four dimensions for both countries’ samples to be utilized in the second step.

Loadings of PsyCap as higher order construct for both countries.
Measurement Model Analysis
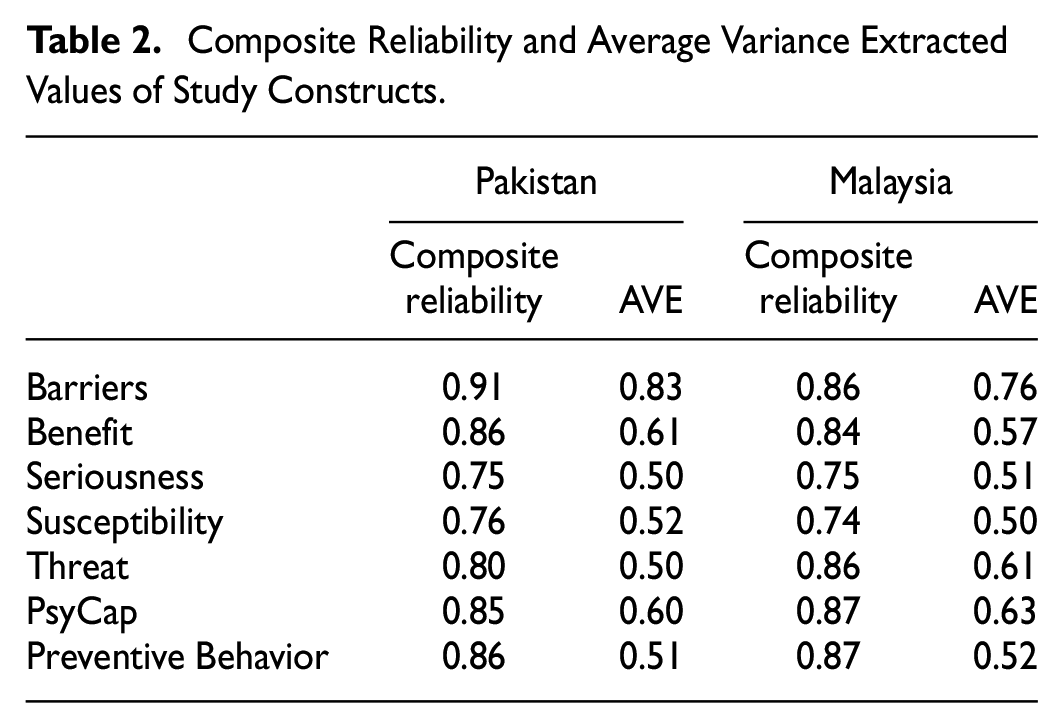
The latent scores saved for four dimensions of PsyCap were loaded as items. All other items were loaded on their respective construct and related to each other as per the theoretical model. First, we analyzed the factor loading of each item on its respective construct. We had to eliminate one item from the barrier scale of the Malaysian sample since the AVE value was less than the recommended value of 0.50. The same item was also removed from the Pakistani sample to maintain comparability. Table 2 shows that the loading of all the indicators on their respective construct is above 0.40, the minimum recommended value in social sciences (Hair, Hult et al., 2017). Similarly, the composite reliability of all the constructs in Pakistani and Malaysian sample was above the criterion value of 0.70. As seen in the Table 2, all the AVEs for a sample of both countries were greater than or equal to 0.5, the threshold level (Henseler et al., 2009).
Composite Reliability and Average Variance Extracted Values of Study Constructs.
Data in the Table 3 depicts the inter constructs correlations (Pakistan below diagonal and Malaysia above diagonal) and square roots of AVE (bold: Pakistan | Malaysia) of a construct. As we can see that in all of the cases, the square root of AVE is higher than the correlations. Hence Fornell-Larcker criterion (Fornell & Larcker, 1981) for discriminant validity in both samples was also met.
Hetero-trait Mono Trait Values Depicting Discriminant Validity of Study Constructs.

Note. Below the diagonal inter-construct correlation for the Pakistani sample, above the diagonal inter-construct correlation Malaysian Sample.
The square root of AVE in the diagonal = Pakistani|Malaysian, Suscept = susceptibility.
Assessment of Measurement Invariance
We conducted MICOM procedure to test for measurement model invariance among constructs of both samples to analyze that if there is no significant difference due to the content and meaning attributed by respondents in both countries. Step 1 of MICOM, configural invariance was established by administering the same questionnaire in both countries, following identical patterns of data treatment such as descriptive, PLS algorithm settings, and a number of bootstraps, etc. The second and third steps of MICOM were carried out by a permutation procedure with 10,000 permutations (Henseler et al., 2016). As shown in Table 4, for all the constructs’ original correlations are higher than 5% quartile of the empirical distribution of cu, which confirms that both samples have compositional invariance. In the last step of MICOM, equality of the composite means and variance depicted insignificance since 95% confidence interval of mean and variance differences of samples of both countries included zero. Hence, we can surmise that estimates of models for both countries are not different in terms of contents and meanings of the constructs. The results of path coefficients can be compared, and data can be pooled as well.
Measurement Model Invariance.

Note. CI = confidence interval; Pak = Pakistan; Mal = Malaysia; Cu = correlation.
The Structural Model
First, we analyzed the structural model as depicted in Figure 1 by adding control variables of Age, Gender, Marital Status, and Level of Education as independent variable linked to preventive behavior. None of the control variables had a significant relationship with the focal outcome (preventive behavior); therefore we omit them from further analysis for the sake of parsimony as suggested by Becker et al. (2016).
To validate the fit of the PLS model, we calculated global goodness of fit (GoF) index (Tenenhaus et al., 2005). GoF reflects the predictive power of the model and is the product of square root of average AVE and average R values. The benchmark for GoF is small ≥0.1, medium ≥0.25, and large ≥0.36. The GoF for both Pakistani and Malaysian samples were 0.25 which depicts that both sample has predictive power greater than the baseline model. Another criteria we employed for model fit was APC. A significant value of APC indicates an adequate model fit (Kock & Lynn, 2012). The APC value for Pakistan was 0.18, p < .01 and for Malaysia was 0.18, p < .01.
The coefficient of determination (R2) and predictive relevance (Q2) shown in Table 5 are reported from the direct effect Model 1. For the Pakistani sample, all the exogenous variables explained 45.6% variance in preventive behavior, which was slightly low in the Malaysian sample at 39.2%. The Q2 value (Geisser, 1975; Stone, 1974) for preventive behavior for each sample was also greater than zero. Hence it can be concluded that there are sufficient in-sample and out-of-sample predictions for an endogenous variable in both Pakistani and Malaysian samples (Sarstedt et al., 2014).
Path Coefficients, Multi-group Analysis, R Square and Q Square Values.
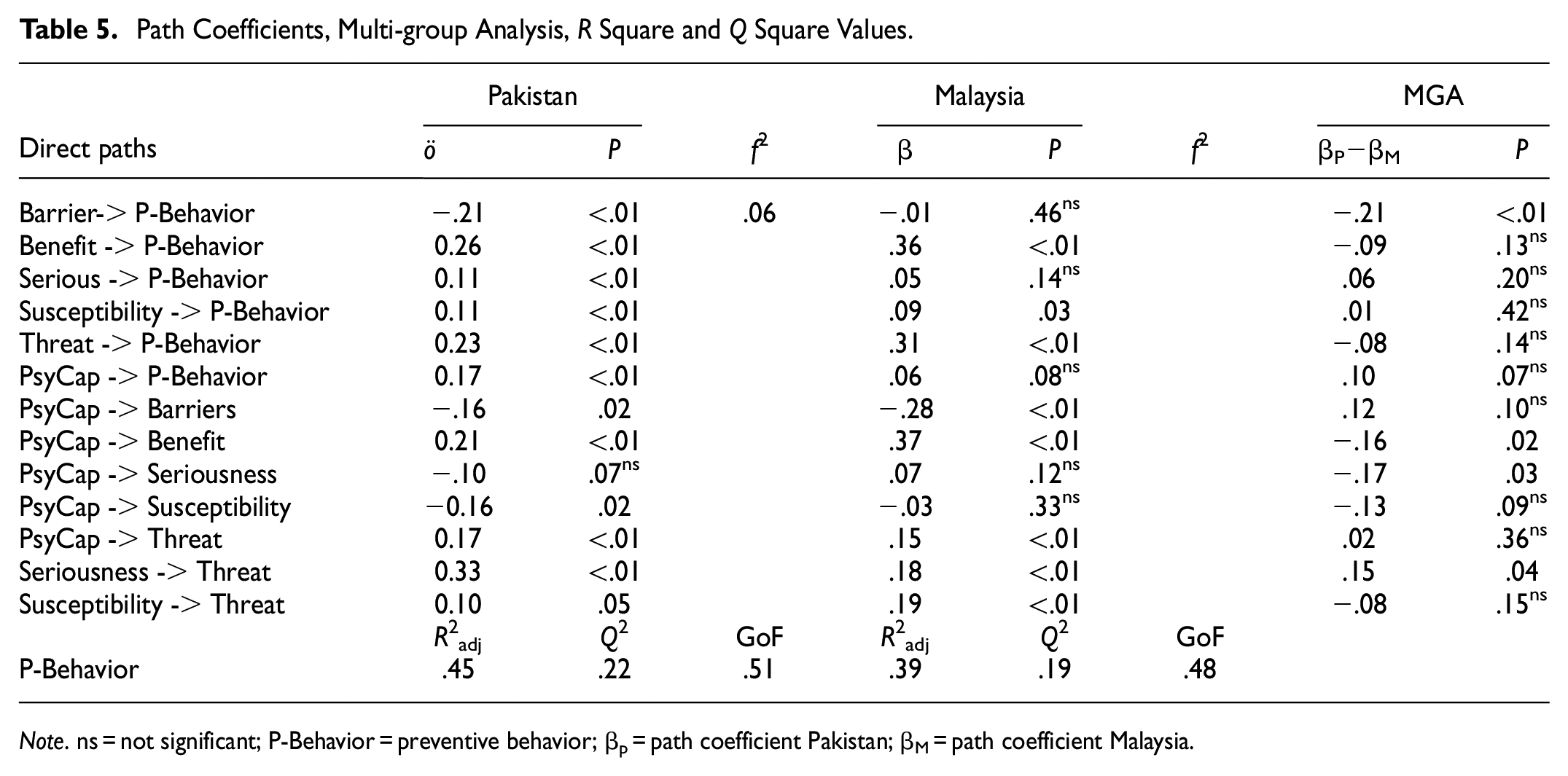
Note. ns = not significant; P-Behavior = preventive behavior; βp = path coefficient Pakistan; βM = path coefficient Malaysia.
As shown in Table 5 and Figure 3, bootstrapping results of the structure model with Pakistani sample revealed significant direct relationship of all of the determinants with preventive behavior. Barriers were negative, β = −.21, p < .01 while benefit, β = .26, p < .01, susceptibility, β = .11, p = .02, seriousness, β = .11, p = .02, threat, β = .23, p < .01, and Psycap, β = .17, p < .01, were positively and significantly related to preventative behaviors. For the Malaysian sample, barrier, β = −.01, p = .36, seriousness, β = .05, p = .14, and PsyCap, β = .06, p < .08, were not significant predictors while benefit, β = .36, p < .01, threat, β = .31, p < .01, and susceptibility, β = .10, p = .03, were significantly related to preventive behavior.

Results of direct effect coefficients and significant values for both countries.
We also tested for the relationship between PsyCap and five predictors of HBM. In Pakistani sample, PsyCap was significantly and negatively related to barriers β = −.16, p < .01, and susceptibility, β = −.17, p = .02 and positively related to perceived benefit, β = .20, p = .02. In the Malaysian sample, PsyCap had a significant negative relationship with perceived barrier, β = −.28, p < .01 and significant positive relationship with perceived benefits, β = .37, p = .03 and perceived threat, β = .15, p < .01. In the Pakistani sample, seriousness, β = .32, p < .01, and susceptibility, β = .10, p = .05 were significant and positive predictor of perceived threat. Similarly, in the Malaysian sample, seriousness, β = .19, p < .01, and susceptibility, β = .17, p < .01, were positively related to preventive behavior.
Our results of MGA analysis (Table 5) indicated that majority of the path coefficients were invariant across both countries. The difference in the direct effect from barrier to preventive behavior, βP−βM = −.23, p < .01, from health PsyCap to perceived benefit, βP−βM = −.16, p = .02, from PsyCap to seriousness, βP−βM = −.17, p = .03 and from seriousness to threat, βP−βM = .15, p = .04, were significant. This indicates that in the aforementioned relationships, country moderates the difference in the path-coefficients. However, in three of the relationships (serious → preventive behavior, PsyCap → preventive behavior, PsyCap → Susceptibility) we found that even-though path coefficients were invariant across both countries, the relationship was significant in one of the groups and insignificant in other, which depicts that country does not moderate these relationships.
Mediation Analysis
First, we tested parallel mediation of barriers, benefits, seriousness, susceptibility, and threat between PsyCap and preventive behavior (Table 6). Our bootstrapping result of bias-corrected and accelerated confidence interval (BCa-CI) yielded that perceived benefit β = .06, 95% BCa-CI [0.02, 0.09], perceived barriers β = .03, 95% BCa-CI [0.01, 0.06] and perceived threat, β = .04, 95% BCa-CI [0.02, 0.07], were significant mediators in Pakistani sample. Perceived benefit, β = .13, 95% BCa-CI [0.09, 0.18], and perceived threat, β = .05, 95% BCa-CI [0.02, 0.08], were significant mediators in Malaysian sample. Second, we tested perceived threat as mediator between perceived seriousness and preventive behavior and between perceived susceptibility and preventive behavior. The mediation analysis revealed that perceived threat mediated relationship between perceived seriousness, and preventive behaviors in both Pakistani and Malaysian sample, β (Pakistan) = .15, 95% BCa-CI [0.09, 0.21], β (Malaysia) = .10, 95% BCa-CI [0.04, 0.15], but only significantly mediated relationship between perceived susceptibility and preventive behavior in Malaysian sample, β (Pakistan) = .09, 95% BCa-CI [0.03, 0.13].
Testing for the Mediation Effects of Health Perceptions.

Note. P-Behavior = preventive behavior; BCa-CI = bias corrected and accelerated – confidence interval.
Significant mediation.
Importance-Performance Analysis
To further explore the relative importance of each variable in explaining our focal variable of preventive behavior and to analyze the current levels of each predictor variable in the sample, we conducted importance-performance analysis (IPA). IPA calculates the total effect of each predictor variable on the outcome variable, including direct and indirect effects. It extends the PLS-SEM results by also indicating the performance levels of the construct on a scale of 100. The results on both dimensions can help public health practitioners and authorities in both samples to focus on those constructs, which shows large importance but are relatively low in performance. Since one of the requirements of IPA is that all the predictors have the same directional relationship with the predictor, we inverted the values of barrier (neg_barrier) to fulfill this condition. Therefore, a higher value of neg_barrier represents the low perception of a barrier to preventive behavior.
The results of the IPA (Table 7) revealed some useful insight into similarities and differences between the sample of two countries. Perceived benefits (Pakistan = 0.26, Malaysia = 0.33), followed by a perceived threat (Pakistan = 0.24, Malaysia = 0.29), were the most important predictor in both countries. The performance values of both these constructs were higher in the Malaysian sample. Inv_Barrier was a relatively important predictor of preventive behavior in Pakistan (0.19) and had a lower performance (61.09, which means higher perception of barrier) but it depicts no importance toward preventive behavior in Malaysian sample (0.01) although the performance levels were on the higher side (69.98, almost nine point lower perception of barrier than Pakistan) Similarly, Pakistani were low on seriousness and perceived susceptibility of the disease, yet seriousness was relatively more important for perceived behavior as compared to the Malaysian sample. The performance level and importance of PsyCap was slightly higher for the Pakistani sample (Importance = 0.18, Performance = 77.80) as compared to Malaysian Sample (Importance = 0.15, performance = 74.46).
Importance-Performance Analysis.
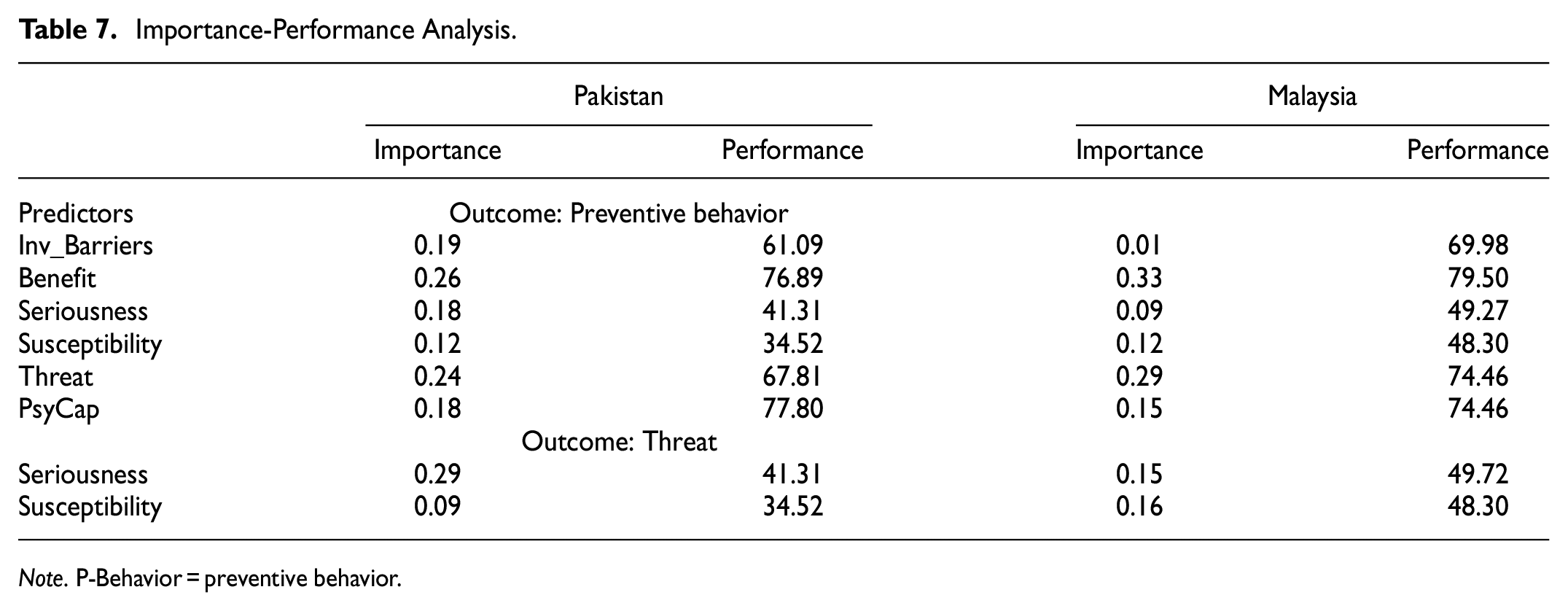
Note. P-Behavior = preventive behavior.
We also tested for importance of seriousness and susceptibility as predictors of threat of COVID-19 contagion. Our results reveal that seriousness (0.29) was a very important predictor of threat as compared to susceptibility (0.09) in Pakistani sample. On the other hand, both seriousness (0.15) and susceptibility (0.16) had moderate and almost similar importance for threat in Malaysian sample.
Discussion
We extended the HMB to include a positive personality resource as a predictor of individuals’ adoption of prevention toward COVID-19. Our study explored the role of health psychological capital in shaping the health-based coping and threat appraisal leading to preventive behavior. The importance-performance analysis presents a useful comparison on the relative effect of PsyCap and five health appraisals on preventive behavior as well as the current performance level of each construct in both counties. Up to the best of our knowledge, this is the first study to examine the health-related implications of PsyCap in the context of COVID-19. We have contributed to the literature by extending HBM backwards by incorporating health PsyCap as predictor of health-based appraisals and preventive behaviors. In addition, we have also incorporated threat as one of the health appraisals along with risk appraisals of susceptibility and seriousness. This allowed us to test the proposition that seriousness and susceptibility transform into threat appraisals and then influence the health-based behavior (Champion & Skinner, 2008).
One of the strengths of our study is that we conducted surveys in two countries, Pakistan and Malaysia, which represents South/South-east Asia region in cross-cultural studies. Both countries do share similarities as well as have many socio-economic differences. For instead when compared on Hofstede’s culture index, dimensions such as masculinity (both: 50), individualism (Pakistan: 14, Malaysia: 26) and long-term orientation (Pakistan: 50, Malaysia: 43) are quite similar. On the other hand, Malaysia score very high on power distance (Malaysia: 100, Pakistan:55) and indulgence (Malaysia 57, Pakistan, 0) as compared to Pakistanis. On the contrary Pakistan (70) high in uncertainty avoidance compared to Malaysians (36). Therefore, our data not only enhances the cross-cultural generalization of the study, it has also allowed us to compared the cross-cultural similarities and differences in how PsyCap and health beliefs influence preventive behavior. Our analysis depicts that country do act as a moderator in few of the relationships.
First, we tested for the direct effect of five health beliefs; perceived benefit, barriers, seriousness, susceptibility, and threat on the preventive behavior. Bootstrapping results revealed that perceived benefit of adopting prevention was significantly related to preventive behavior in both countries. IPA revealed that benefit was the most important predictor of focal outcome in both Pakistan and Malaysia. These results are in concordance to results of a meta-analysis of longitudinal studies on effectiveness of health belief model variables on predicting behavior, which found perceived benefit to be the strongest and most consistent predictor (Carpenter, 2010). The meta-analysis also indicated that benefit was a better predictor of behavior when the motive is to prevent potential disease and disorder rather than treatment after an illness. This is aligned with the Rosenstock’s (1974) original HBM philosophy, whose focus in advocating this model was to study how individuals respond to preventive behavior when they face a disease threat. Scherr et al. (2016) also found that people who are worried about flu, get vaccinated because they find health benefit in it. These findings reveal that health behavior promotion messages should focus on beneficial outcomes for people. Multi-group analysis revealed no significant difference in path-coefficient in both countries. Performance values suggested that Malaysians are slightly more convinced of the benefit of adopting the preventive approach to avoid getting infected from COVID-19.
Unlike the influence of benefit, perceived barriers to observe prevention against COVID-19 was negatively related with preventive behavior in Pakistani sample, but not for the Malaysian sample. MGA revealed that the difference in path coefficients was significant. The moderating effect of the country in this relationship can be explained by the socio-economic differences in both countries. Pakistan is a lower-middle-income country (GDP/capita = $1,500), while Malaysia is an upper-middle-income country (GDP/capita = $11,000) (Prydz & Wadhwa, 2019). Pakistanis seems to perceive higher barriers toward preventive measures because they are already facing a myriad of issues such as inflation, law and order, energy crisis, corruption, crumpled health facilities, mismanaged governance, and so on. The adoption of preventive measures is rather impractical for Pakistanis as it is related to the disruption of social and professional life. This finding suggests that authorities in Pakistan need to understand and find solutions for the difficulties people face during a lockdown, which may discourage them from adopting preventive behavior. An interesting finding from IPA is that our respondents in both countries had a similar appraisal of barriers but its relationship with preventive behavior was significantly different in both countries.
Our results suggested that risk perception of susceptibility and severity are weaker predictors of preventive behavior compared to the coping appraisals of benefit and barriers in both countries. In this regard, our results slightly deviate from previous literature which consistently found that perception of susceptibility and severity (seriousness) of the disease was strongly related to preventive approach (Brewer et al., 2007; Leung et al., 2003, 2005). We conducted this study at a time, when COVID-19 had globally spread but was still in the initial phase of spread in both the countries. So, there is a possibility that people in both countries have accepted it as a threat but did not fully invest their mental energies in trying to understand the epidemiological aspects of COVID-19 and relate it to their vulnerability based upon personal health status. Similarly, survey was conducted at a time when patient count and deaths in both countries were very low. On the other hand, the pandemic had already proven to have a catastrophic effect on some of the most developed countries of the world. So our respondents tendency to misread the seriousness of the situation might have come from an inherent judgmental bias heuristic (Tversky & Kahneman, 1973) and optimistic bias such that they underestimate the seriousness of the pandemic at this point (Bottemanne et al., 2020). These biases in judgment may be a reason that both types of risk perceptions (seriousness and susceptibility) had a lower contribution in preventive behavior as compared to coping appraisal. The IPA of seriousness and severity and comparison across countries reveals that Pakistani sample is relatively less serious and feel less susceptible to the disease when compared to the Malaysia sample. However, MGA revealed no significant difference in path coefficients of seriousness/susceptibility and preventive behavior relationships.
Unlike susceptibility and seriousness, contextual threat appraisal seems to be a strong contributor in adoption of preventive behavior, as a direct predictor as well as a mediator of effect of seriousness in Pakistani sample and mediator of effect of both seriousness and susceptibility in Malaysian Sample. Scherr et al. (2016) also reported a strong relationship of the threat of flu with people’s intentions to get vaccinated. People who are high in health related psychological capital make more realistic appraisals of disease as their tendency to be over-optimistic about a prevailing situation is often counteracted by the hope component which provides a more balanced picture of the health situation and the steps needed to control it (F. Luthans et al., 2013). Considering that data was collected when pandemic had spread globally but still in early phases of spread in both countries, it is plausible that people high in health related PsyCap keep themselves abreast of COVID-19 updates and realistically consider it a situational threat. Threat gives rise to an emotional response of fear, which is a human’s defense system against situational dangers and has played an important role in the survival of the human race. We also found statistical support for our proposition that seriousness of pandemic and susceptibility of getting sick relates to perceived contextual threat in both countries. MGA revealed that seriousness was a stronger predictor of threat for Pakistani sample as compared to Malaysia. In addition, mediation analysis found that threat mediates the relationship between seriousness and preventive behavior in both countries but mediates the relationship between susceptibility and preventive behavior only in Malaysia. The performance level of perceived threat was almost five units higher in the Malaysian sample.
Finally, one of the most unique theoretical contributions of our study is to expand the health belief model to include personality resource of health psychological capital as a predictor of preventive behavior. First, we tested how psychological capital directly influence preventive behavior and relates to five types of health beliefs. Second, we analyzed possible parallel mediation of five health beliefs between PsyCap and preventive behavior. From our direct effect analysis, we found that psychological capital was a direct predictor of preventive behavior in Pakistani sample but not in Malaysian sample. Similarly, we found that PsyCap was negatively related to perceived barriers and positively related to benefits and threat in both countries. Multi-group analysis reveals a stronger relationship between benefit and preventive behavior in Malaysian sample as compared to Pakistani respondents. However, it was a negative predictor of susceptibility in Pakistani sample but not in Malaysian sample, yet country was not a moderator in this relationship as MGA did not reveal a significant difference. A strong sense of self-worth and devotion toward health (Krasikova et al., 2015) also explains why PsyCap was negatively related to susceptibility of COVID-19 among the Pakistani sample. No relationship existed between PsyCap and seriousness in both countries. It seems that terms like “no treatment,”“media hype,” or “long lasting impact” which were used to measure the respondent’s seriousness about pandemic and represent a pessimistic and defeatist belief, do not agree with cognitive capacities of confidence, optimism, hope and resilience ingrained within high PsyCap individuals.
We found barriers, benefits and threat to be partial mediator between PsyCap and preventive behavior in Pakistani sample and benefits and threat to fully mediate the relationship between PsyCap and preventive behavior in Malaysian sample. Overall, our results indicated a more profound relationship of PsyCap with coping appraisals (positive with benefit and negative with barriers) which also act as mediating mechanisms in the PsyCap-preventive behavior link (except for barriers in Malaysian sample which is not a significant predictor of preventive behavior). The agentic positive approach ingrained within health PsyCap and its four components acting in synchrony to maintain and improve overall health triggers an individual to proactively involve in health-management behavior (Krasikova et al., 2015). It seems people who are more optimistic, hopeful, confident and resilient regarding their health are more focus on the positive, beneficial aspect of preventive behavior and are motivated to overcome the possible barriers between their health and efforts.
On the other hand the trivial role of risk perceptions (susceptibility and seriousness) in relating PsyCap with prevention can be explained by the positive outlook of the situation ingrained within the personality itself (F. Luthans & Youssef-Morgan, 2017). Research has shown that negative and unfavorable perceptions about ones health or higher health anxiety may lead to mental health issues in future (Kaplan et al., 1987; Williams, 2004). Considering that people high in health PsyCap are more directed toward identifying strengths rather than weaknesses while striving for good health, it is plausible that more negatively toned health risk perceptions do not act as mediating mechanisms in PsyCap-preventive behavior relationship. Since it is established that the prevailing situation is detrimental to health in general, appraising COVID-19 as a threat and being worried about its spread seems to be a realistic belief for a person who is health conscious. This explains why threat appraisal acts as a mediator between PsyCap and preventive behavior. The different relationships of PsyCap with risk perceptions and with threat appraisal also helps to reinforce our stance that both types of appraisals are convergent yet discriminant concepts. The performance analysis of PsyCap indicated that respondents from both countries were high in health PsyCap, which can be an indication of the public’s positivity and motivation to keep themselves healthy.
Implications
The current global trend indicates that it is not easy to get people to adopt strict preventive measures such as restriction on mobility, maintaining social distance and health hygiene. Authorities worldwide have taken extreme steps to curb out the spread of contagion such as lock-downs, closure of borders, putting a halt to the majority of economic and social activity to keep people safe and healthy to mitigate the spread of disease. Besides, based on their respective financial capacity, governments have also announced bailout packages for the public. However, all these efforts to curb the spread of disease by halting trade and travels come at a huge toll to the economy as well as the deterioration of mental health to the people forced to be socially isolated under lockdowns (Wilder-Smith et al., 2020). As countries started to ease the lockdowns, a surge in infections or the second wave of COVID-19 has emerged (Cacciapaglia et al., 2020). Both Pakistan and Malaysia started experiencing their second wave around end of October,2020 with Malaysia getting a steeper slope and multifold more cases as compared to its first wave. Although discovery of vaccination at the end of 2020 and its limited distribution in some countries is a promising step, no one can undermine the importance of prevention, especially when the dangers of ongoing and possibility of another pandemic lingers in air.
To control the spread of COVID-19 while allowing for economic and social activities, people need to adjust preventive behaviors within their social and professional lives. First of all, our study reiterated the unique contribution of various health beliefs, especially perceived benefit and perceived barriers in individual’s adoption of preventive behaviors. The governments need to mobilize all possible communication means (social media, electronic media, political appeals, celebrity endorsements, etc.) to change the schemas of their citizens for a voluntary adoption of preventive measures. In accordance to our results, the messages should make them believe that adopting this lifestyle has a direct benefit to their well-being as well as of those they are concerned for. Importance of threat perception indicates, that public awareness campaigns, in part, should also draw a grim picture of the future if the spread of COVID-19 continues. However, authorities should understand that there is a thin line between the threat message which informs the public about the seriousness of the disease and a sensational message that creates fear and panic. To maintain this delicate balance, stakeholders like political leaders and popular media need to work as one voice.
Over and above what is already known, this study adds health communication literature with the perspective of positive psychology. After a long haul of focus on the disease model in existing psychology, the role of positive psychology in promoting health and well-being as well as enhancing human capacity to face the adverse situations such as pandemics cannot be ignored (Kulandaiammal, 2020; M. E. P. Seligman & Csikszentmihalyi, 2000). Our research has highlighted that health domain psychological capacity can be instrumental in shaping various health perceptions which leads to higher adoption of preventive behavior. Previous research has shown that individuals high in health PsyCap have better psychological health, low on stress (Avey et al., 2011) and realistically evaluate the steps needed to protect their health (F. Luthans et al., 2013). As a positive psychological resource, people high in PsyCap are more satisfied with their health, and strive to keep the indicators representing health condition inflated (Manzano-García & Ayala, 2017). Therefore training and development interventions aimed at improving PsyCap (Avey et al., 2010; F. Luthans et al., 2008) are likely to have more profound and far reaching health benefits.
Previous studies have also shown that PsyCap is moderately stable personality state which means that a positive psychological interventions tools and techniques to promote health PsyCap can be a slightly long-term alternative to risk communication messages which aim to directly influence coping and risk appraisals. However, to improve public’s health PsyCap of a wider public, health authorities need to redesign interventions currently targeted for a smaller group. Previous research has shown that PsyCap can be enhanced though leader-member exchange (Avey et al., 2011), political leadership can also play a very important role enhancing health-related psychological tendencies, beliefs and behaviors among the public. In addition, the current risk communication and public health campaign messages for COVID 19 or any future pandemic can also incorporate messages to enhance health-related positive outlook of now and future (optimism), confidence on one’s ability (self-efficacy), goals and pathways and ability to bounce back in case a health issue arise (resilience).
In contemporary times, media plays a central (and sometimes disturbing) role in spreading the information, which is often spice up the real information to make it more sensational. This information plays an essential role in creating an anticipatory threat of the disease in the public’s mind. However, some researchers have also shown concern regarding threat messaging. Excessive fear can convert threat into distress, thus creating more psychological harm, then the actual disease would (Ren et al., 2020; Taha et al., 2014). Enhancing preventive behavior through PsyCap intervention can mitigate this issue. Our research has shown that people high in PsyCap are more adoptive of preventive behavior because they had developed more practical (coping appraisals) and realistic approach (COVID-19 as a contextual threat) rather than getting afraid of getting sick or cognitively overburdening themselves by considering COVID-19 as a desolate situation.
Limitations
There are several limitations that ought to be considered while interpreting the results. First of all, the study collected data online using snowball sampling. Although this technique was quite successful as we had a sample of more than 300 respondents in each country only within the span of 2 days, the sample may not be a true representative of the population in each country. There was an oversampling of people with master/PhD degree (40.8% Pakistan, 30.9% Malaysia). This probably because the authors being academicians, has majority of personal contact belonging to academics. However, the study was conducted at time when both countries were undergoing a mandatory lockdown and online data collection through social media was the only plausible solution. However, a preliminary analysis of demographics as control variable when regressed with dependent variable did not reveal significant path values. Since our respondent were present on internet, we believe they would have a greater awareness and knowledge of COVID-19 and are more akin to the scope of current study whose purpose was to test a theory. Literature has recommended that in an exploratory study, when the aim is to test a theory, results from non-probability sampling can be generalized when a study is testing an established model, measures of constructs are established and the results are not too much deviant from existing research (Calder et al., 1982; Lucas, 2003). Nevertheless, the findings of this study should be generalized with a caution. In addition, we have analyzed data from early stages of COVID-19 when pandemic had not severely impacted both Pakistan and Malaysia. This can be the reason that effect sizes were relatively small. Both countries have seen a different pattern of first wave and a second wave of pandemic subsequently. Therefore we recommend further research to explore the relationships at later stage of pandemic.
Although we used a priori model to depict causal relationship, it should be underscored that the study was pure correlation and we cannot justify any causal or direction relationship from methodology of the research. There is ample possibility for reverse relationship such that perceived threat influence the seriousness and susceptibility of the disease. Similarly considering that PsyCap is a malleable personality resource, which shapes perception, both threat and risk perceptions and coping appraisals can also influence one’s positive psychological capacity overtime. Longitudinal research can be more pertinent to explore this proposition. Regarding PsyCap in our model, we feel that the effect sizes were lower than expected. Perhaps when it comes to preventive approach, resilience as a more reactive personality style may not have played an important role influencing this behavior. Therefore, we recommend future researchers to analyze the relationship of four components separately with preventive behavior.
Conclusion
In conclusion, this study highlights the importance of health psychological capital and health appraisals in influencing the voluntary adoption of preventive behavior during COVID-19, based on the health belief model. The findings show that perceived benefits and threats are significant predictors of preventive behavior in both Pakistan and Malaysia. Psychological capital plays a key role in shaping health appraisals, which in turn affect preventive behavior. Country-specific differences were observed, with a higher explained variance in preventive behavior for Pakistan compared to Malaysia. These findings have practical implications for health communication and intervention development, emphasizing the importance of promoting positive psychological resources, addressing barriers, and highlighting benefits and threats associated with preventive behaviors. Overall, this study contributes to understanding the factors influencing preventive behavior during a pandemic and provides insights for designing targeted interventions to promote health-related positive personality resources and encourage the adoption of preventive behaviors, ultimately contributing to efforts to combat the spread of highly transmissible diseases like COVID-19.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.