
Abstract
The purpose of this study was to assess the rate of post-traumatic stress symptoms (PTSS) experienced by individuals in response to COVID-19; to identify which coping strategies individuals employed in response to the pandemic; and to understand the relationship between COVID-19 stress and PTSS over time. Adult participants were assessed at three timepoints over the course of approximately 8 months. Between 13% and 15% of participants endorsed high levels of PTSS at Time 1, indicative of likely PTSD. Participants endorsed using a variety of coping strategies with moderate frequency at Time 1, including self-distraction, active coping, positive reframing, planning, acceptance, and religion. Longitudinally, Time 1 COVID-19 stress was found to predict the development of Time 3 PTSS. This relationship was partially mediated by Time 2 behavioral disengagement. Additionally, acceptance was identified as a moderator of the relationship between Time 1 COVID-19 stress and Time 3 PTSS, in an unexpected direction.
Plain Language Summary
The purpose of this study was to assess the rate of post-traumatic stress symptoms (PTSS) experienced by individuals in response to COVID-19; to identify which coping strategies individuals employed in response to the pandemic; and to understand the relationship between COVID-19 stress and PTSS over time. Adult participants were assessed at three timepoints over the course of approximately 8 months. Between 13% and 15% of participants endorsed high levels of PTSS at Time 1, indicative of likely PTSD. Participants endorsed using a variety of coping strategies with moderate frequency at Time 1, including self-distraction, active coping, positive reframing, planning, acceptance, and religion. Longitudinally, Time 1 COVID-19 stress was found to predict the development of Time 3 PTSS. This relationship was partially mediated by Time 2 behavioral disengagement. Additionally, acceptance was identified as a moderator of the relationship between Time 1 COVID-19 stress and Time 3 PTSS, in an unexpected direction.
Introduction
SARS-CoV-2, commonly referred to as COVID-19, has impacted individuals of all ages worldwide. Mental health conditions were exacerbated by government imposed lockdowns, which limited social interaction and required social distancing practices (Beck et al., 2021; Umucu & Lee, 2020). These protective practices were efficacious in slowing the rate of infection (World Health Organization, 2020), but may have precipitated adverse psychological implications. Studies have shown similar disease outbreaks resulted in increased risk for various mental health conditions including depression, anxiety, post-traumatic stress disorders (PTSD), and sleep disorders (Bendau et al., 2021; World Health Organization, 2020). More so, research suggests that strict social distancing practices may have contributed to psychological distress due to isolation and inadequate social support (Beck et al., 2021; Bendau et al., 2021).
Previous research studies examining stress and coping responses to health emergencies, such as the 2003 severe acute respiratory syndrome-CoV (SARS-CoV), 2009 influenza A (H1N1), and 2013 Ebola Virus Disease outbreaks, noted high rates of anxiety, depression, and post-traumatic stress symptoms (PTSS) in respondents(Cheng & Cheung, 2005; Hawryluck et al., 2004; Sim et al., 2010). Similarly, early international work reported high rates of psychological disorders in response to COVID-19 (Li, 2020, Mazza et al., 2020; Sønderskov et al., 2020; Wang, Pan, Wan, Tan, Xu, Ho, & Ho, 2020; Wang, Pan, Wan, Tan, Xu, McIntyre, et al., 2020). Li reported that 42.7% of 1109 respondents surveyed in China endorsed clinically significant symptoms of psychological distress, as measured by the General Health Questionnaire–28 (Li, 2020). Additionally, Wang and colleagues found 53.8% of 1210 persons surveyed in China reported moderate to severe psychological stress on the Impact of Events Scale–Revised; 28.8% reported moderate/severe anxiety, and 16.5% reported moderate/severe depressive symptoms on the Depression, Anxiety, and Stress Scale (Wang, Pan, Wan, Tan, Xu, Ho, & Ho, 2020). When participants were re-assessed 4 weeks later, no significant differences were identified in overall rates of anxiety or depression, suggesting that psychological stress symptoms can persist over an extended period (Wang, Pan, Wan, Tan, Xu, McIntyre, et al., 2020).
Current studies suggest the presence of potential trauma responses in individuals affected by COVID-19. Reported prevalence rates of COVID-19 associated PTSS and PTSD vary widely, based on timeframe of assessment in relation to the outbreak, measure used, and cut-off score employed. Specifically, rates of likely PTSD range from 7% (Liu et al., 2020) (PTSD Checklist for DSM-5; cutoff score of 33+) to 10.8% (Tan et al., 2020) (Impact of Events Scale–Revised; cutoff score of 24+) to 67.1% (Li, 2020) (Impact of Events Scale – Revised; cutoff score of 20+). Critically, these studies were conducted at a single time point with Chinese samples, and information regarding rates of PTSD within the United States either at a single time point or longitudinally has, to our knowledge, not yet been reported.
Additionally, despite the significant potential for psychological distress, research has minimally investigated the coping skills individuals implemented in response to COVID-19. Coping is defined by cognitive and behavioral efforts to manage an experience in response to stressors, and it is tied to psychological wellbeing and emotional outcomes (Li, 2020, Lazarus, 1966). Coping skills include both individual strategies as well as strategies that exist within the family unit and community as a whole (Li, 2020, Carver, 1998; Folkman, 2013; Roesch et al., 2002). Of importance, COVID-19 restrictions on activities may have undercut individuals’ abilities to utilize otherwise effective coping strategies. In particular, the limiting of social connectedness due to closure of schools, restaurants/bars, gyms, restricted access to healthcare, changes in business practices (i.e., transitioning to working from home), and restrictions on social gatherings may have negatively impacted an individual’s ability to engage in healthy, positive coping behaviors, and/or may have potentially compounded pre-existing mental health symptoms.
Presently, few studies have examined the coping strategies utilized by individuals in response to COVID-19 (Park et al., 2020). In a study of Iranian individuals, problem-focused coping strategies were used most often, followed by emotion-focused, and avoidant coping, as determined by the Coping Inventory for Stress Situations–Short Form (Mohammadzadeh et al., 2020). In a cross-sectional study conducted by Umucu and Lee in the US, COVID-19 related stress was positively associated with the use of various coping strategies, as measured by the Brief-COPE (Umucu & Lee, 2020). These strategies included self-distraction, denial, substance use, behavioral disengagement, venting, planning, religion, and self-blame (Umucu & Lee, 2020). One study examined these constructs in individuals living in China (Li, 2020). These results suggest that individuals tended to use emotion-focused coping or a mix of emotion and problem-focused coping, relative to problem-focused coping alone, in response to COVID-19 (as measured by the Brief-COPE) (Li, 2020). Furthermore, those individuals who reported use of both emotion and problem-focus coping reported fewer psychological symptoms, relative to those who used emotion-focused coping only; those who reported using problem-focused coping only were at higher risk for experiencing PTSD, compared to those who reported using emotion-focused coping only (Liu et al., 2020). This suggests that the flexible use of a mix of emotion and problem-focused coping skills may have been necessary to manage the chronic, yet shifting, stress associated with COVID-19, though this area clearly warrants further investigation. Specifically, longitudinal assessment must occur to understand how the use of particular coping strategies may impact individuals’ psychological functioning over time.
Given the nascency of the medical field’s understanding of the impact of COVID-19 on psychological health, the purpose of the present study was to provide longitudinal data on the stress and coping behaviors of individuals in response to COVID-19 in the United States. Specifically, this study assessed the exposure level of adults living primarily in the Southern United States to COVID-19 associated stress, their PTSS responses, and their use of various coping strategies. Further, this study assessed the relationship between COVID-19 stress, coping, and PTSS over three time points spanning 8 months. Considering the novel and exploratory nature of this study, no a priori hypotheses were made.
Method
Measures
This study was IRB approved. A formal waiver of consent was applied to all participants, which included a complete explanation of the purpose of the study, the potential benefits and risks, as well as the voluntary nature of participation. Additionally, contact information for the primary investigator was provided to all participants prior to survey initiation. The survey first included a detailed demographic questionnaire. Demographic items included: age, size of household, age of children (if applicable), gender, race, ethnicity, marital status, education level, income, zip code, employment status, and employment risk. Participants were also asked about their primary news source (television, online news websites, social media, print news, or radio) and quantity of time spent consuming COVID-19 related information.
Second, participants were given four psychological measures: COVID-19 Stressor Questionnaire; PTSD Checklist for DSM-5 (PCL-5); Brief-COPE Inventory; and COVID-19 Experience Qualitative Section (Blevins et al., 2015; Carver, 1997; Errett, 2020a, 2020b).
The COVID-19 Stressor Questionnaire includes 11-items relating to level of concern for various COVID-19 stressors. Participants rated their level of concern (i.e., 0 = not concerned, 1 = somewhat concerned, 2 = very concerned) for items such as “getting sick myself” and “not being able to work.” Scores range from 0 to 22 with higher scores indicating greater level of COVID-19 stress (Errett, 2020b).
The PCL-5 is a 20-item self-report measure assessing symptoms experienced in the past month based on DSM-5 PTSD diagnostic criteria. Item responses range from 0 (Not at all) to 4 (Extremely). A total symptom severity score is computed, and a cut-off score is utilized to identify participants likely to meet criteria for PTSD (Weathers et al., 2013). Previous literature has varied regarding appropriate cut-off score selection; therefore, results will be reported utilizing cut-off scores of 31 and 33, respectively (US Department of Veterans Affairs, N.D; Weathers et al., 2013). This measure is psychometrically sound, with strong internal consistency (α = .94), test-retest reliability (r =.82), and convergent validity (rs =.74–.85) (Blevins et al., 2015).
The Brief-COPE Inventory is a 28-item self-report questionnaire used to assess coping responses. Subscales, composed of two items each, include: self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame. Responses range from 1 (“I haven’t been doing this at all”) to 4 (“I’ve been doing this a lot”). The Brief-COPE is noted to have adequate internal consistency of subscales (α = .50–.90) (Carver, 1997).
Finally, the COVID-19 Experience Qualitative Section is an open-ended question for participants to describe their personal experience of the COVID-19 pandemic (Errett, 2020a). The questions include: (1) how has the disease itself impacted you, your family, or your community? (2) how have recommendations and actions taken by public health officials impacted you, your family, or your community? (3) how are you, your family, or your community adapting to these impacts? (4) how are you, your family, or your community coping with these impacts? (5) what are your concerns in the short-and long-term? and (6) what has been helpful in making this experience less challenging in the short- and long-term? All responses were coded and analyzed using NVivo to identify themes.
Procedures
This longitudinal survey was designed to assess current and former hospital patients (age 18 and older), patient families, employees and volunteers of the hospital and other local hospitals, as well as community members of the larger Dallas/Fort Worth metro area and beyond. The survey was administered across three time points (referred to here as Time 1, Time 2, and Time 3).
Time 1 data collection occurred between May and August 2020, which was the initial peak of the COVID-19 pandemic in the Southwestern United States. Participants were largely recruited using the hospital electronic medical record to identify patients with an active status and phone number and/or email address since October 2016. Email or text message communication was sent to active patients (age 18+)/patient families with listed information inviting them to participate in this voluntary study.
Hospital employees and volunteers were recruited using internal email messages, clinic flyers, and word of mouth. Community participants were recruited through hospital social media platforms, the hospital website, recruitment flyers at community locations, and word of mouth.
Participants completed the study via the secure online portal Research Electronic Data Capture (Harris et al., 2009, 2019). Data was collected anonymously and stored on a secure server via a password protected website. Once participants completed the survey, they were automatically provided with links to COVID-19 coping resources. Participants were given the option to be re-contacted for follow-up at two additional time points. Time 2 data collection occurred between September and December of 2020, and Time 3 data collection occurred between January and April 2021.
Data Sharing Statement
Individual de-identified participant data (including data dictionary) are shared in the form of an excel spreadsheet. Additional related documents include syntax file for SAS 9.4, explanatory memo e, and outputs with results of the analysis completed.
Results
Descriptive Information
At Time 1, 2243 participants completed the survey. All participants were included in data analysis, even in the presence of skipped items and associated missing data. Eight participants were excluded due to being outside of the required age range. Participants ranged in age from 18 to 86 (M = 42.56 years, SD = 10.75 years). Participants identified primarily as English-speaking (96.2%), non-Hispanic White (66.2%), and cis-gender female (78.8%). Most participants had a bachelor’s degree or higher (65.8%) with a household income of $75,000+ (62.9%). Concerning employment, 56.6% of participants were employed, 12.8% were unemployed, 4.1% were retired, 2.2% were students, and 9.0% identified as Other or preferred not to say.
Ninety-five participants completed the survey at Time 2 (M = 42.63 years, SD = 10.56 years). Participants at Time 2 identified primarily as cis-gender female (80.0%) and non-Hispanic White (75.7%). Nearly all participants had a bachelor’s degree or higher (82.1%), and 64.2% reported a household income of $75,000 or higher. Two-hundred and thirty-four participants completed the survey at Time 3 (M = 42.58, SD = 10.58 years). Time 3 participant characteristics were similar to that of Time 2 with 81.6% of participants identifying as cis-gender female, 77.3% non-Hispanic White, 79% reported a bachelor’s degree or higher, and 68.8% reported a household income of $75,000 or higher.
In total, 58 participants completed the survey at all three time points (M = 42.63 years, SD = 10.56 years). The majority of participants identified as cis-gender female (86.2%) and non-Hispanic White (79.3%). The vast majority reported earning a bachelor’s degree or higher (87.9%), and 67.2% reported a household income of $75,000 or higher. See Table 1 for additional demographic data.
Time 1 Demographics.

Cross-Sectional Assessment at Time 1
COVID-19 Stressors
Regarding COVID-19 associated stressors at Time 1, 72.7% of participants reported feeling somewhat or very concerned about becoming sick with COVID-19; 87.8% reported feeling somewhat or very concerned about a family member becoming sick. Several participants expressed concerns for elderly family members, those with pre-existing conditions, and those working as essential workers. Sample qualitative responses include:
“My mom is 97 so I worry for her. She has a caregiver two days a week, but I worry if we should just cancel but then we won’t have any help and the caregiver supports two teenage daughters. My other concern at home is my husband who has a severe aortic valve leak.” (Participant 638)
“I am concerned about my spouse, who works in an environment where they are in close proximity to COVID patients and work very long hours, so I am often home alone during this time.” (Participant 371)
With respect to healthcare, 43.2% of participants reported being somewhat or very concerned about the inaccessibility of COVID-19 treatment, 46.1% reported being somewhat or very concerned about the inaccessibility of treatment for other chronic conditions, and 50.6% reported being somewhat or very concerned about the inaccessibility of treatment for other emergent conditions.
Considering employment, 58.4% of participants reported feeling somewhat or very concerned about not being able to work due to COVID-19, and 55.4% reported feeling somewhat or very concerned about not being able to pay their bills. Retirement was a lesser concern, as 36.0% of participants reported feeling somewhat or very concerned about not being able to retire as scheduled.
Interpersonally, 56.5% of participants endorsed being somewhat or very concerned about experiencing social isolation. Participants were even more concerned for their family members, and 75.8% endorsed being somewhat or very concerned about family members experiencing social isolation with concerns surrounding psychological distress, and developmental delays in children. Sample qualitative responses include:
“I’m worried about my son with autism regressing in social skills and living in his own world more.” (Participant 2578)
“My grandmother is on strict lockdown, and she is going crazy…like truly. Her mind isn’t the same. She’s depressed.” (Participant 1116)
Post-Traumatic Stress Symptoms
PCL-5 Total scores were relatively low at Time one, M = 15.25, SD = 14.163 (range 0–80). When identifying participants who were likely to meet criteria for PTSD, 15.4% met criteria with a cut-off score of 31, and 13.3% met criteria when the cut-off score was increased to 33.
Coping Skills
On the Brief-COPE, participants reported using self-distraction (M = 5.29, SD = 1.70, range 1–8), active coping (M = 5.15, SD = 1.75, range 1–8), positive reframing (M = 5.24, SD = 1.84, range 1–8), planning (M = 5.20, SD = 1.79, range 1–8), acceptance (M = 6.38, SD = 1.64, range 1–8), and religion (M = 4.97, SD = 2.38, range 0–8) with moderate frequency at Time 1. Participants reported using denial (M = 2.60, SD = 1.11, range 1–8), substance use (M = 2.72, SD = 1.31, range 1–8), emotional support (M = 4.57, SD = 1.81, range 1–8), instrumental support (M = 4.06, SD = 1.67, range 1–8), behavioral disengagement (M = 2.75, SD = 1.24, range 1–8), venting (M = 3.95, SD = 1.51, range 1–8), humor (M = 3.96, SD = 1.78, range 1–8), and self-blame (M = 2.78, SD = 1.34, range 0–8) less frequently.
Active coping, religion, and substance use were the main coping themes that emerged from the qualitative data. Some participants chose to learn new hobbies, others engaged in outdoor activities, and a few turned to various substances to relieve the pain and immense psychological distress of the pandemic. Participant responses included:
Active Coping
“I have been attempting to take each day one at a time and keep in contact with family members and close friends and busy myself with hobbies.” (Participant 3714)
“When dad comes home from work we play outside, go for bike ride, swim in the pool, or take a hike at the lake.” (Participant 2619)
Religion
“My saving grace is the fact that I know God is in control of the situation and his word says that he will never leave us or forsake us. After the initial shock of this situation, I have learned to put more faith in God.” (Participant 784)
“We rely on our faith and continue to pray together each day.” (Participant 831)
Substance Use
“My sister (who I live with) is SO obsessive about all of it and spent probably 8 hours a day researching stuff. She was grumpy and irritable and all we did was drink and slack off.” (Participant 1116)
“The loss of my son’s senior year in high school was devastating and he is still grieving. He has begun using illegal drugs to cope with the pain, anxiety and isolation, and it’s extremely stressful as his parent.” (Participant 1797)
Correlations
Participants’ PCL-5 Total scores at Time 1 were concurrently, positively associated with each COVID-19 stressor (r = .27–.43, p’s < .01), suggesting that greater COVID-19 stress was associated with higher PTSS (Table 2). Participants’ PCL-5 Total scores at Time 1 were also concurrently, positively associated with the following coping skills : self-distraction (r = .27, p < .01), denial (r = .24, p < .01), substance use (r = .25, p < .01), emotional support (r = .17, p < .01), instrumental support (r = .20, p < .01), behavioral disengagement (r = .43, p < .01), venting (r = .32, p < .01), planning (r = .24, p < .01), humor (r = .07, p = .01), and self-blame (r = .59, p < .01). PCL-5 Total scores were not significantly related with the following coping skills: positive reframing (r = −.02, p = .37), religion (r = −.003, p = .90) and acceptance (r = −.02, p = .56).
Correlations Between PCL-5 Total Score and COVID-19 Stressor Questionnaire Subscales at Time 1.
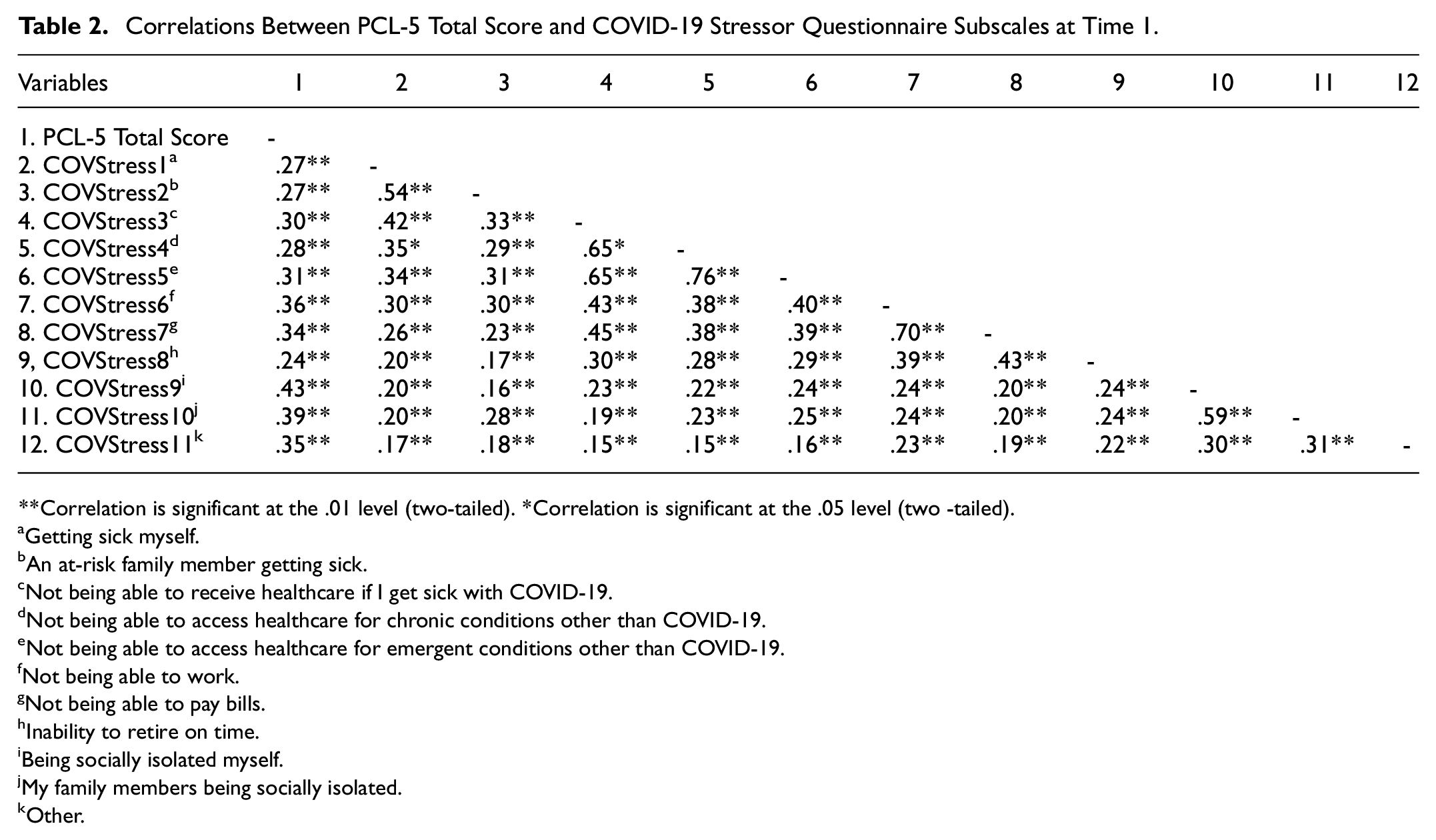
Correlation is significant at the .01 level (two-tailed). *Correlation is significant at the .05 level (two -tailed).
Getting sick myself.
An at-risk family member getting sick.
Not being able to receive healthcare if I get sick with COVID-19.
Not being able to access healthcare for chronic conditions other than COVID-19.
Not being able to access healthcare for emergent conditions other than COVID-19.
Not being able to work.
Not being able to pay bills.
Inability to retire on time.
Being socially isolated myself.
My family members being socially isolated.
Other.
Longitudinal Assessment Across Times 1, 2, and 3
To evaluate the longitudinal relationship between Time 1 COVID-19 stress and Time 3 PCL-5 Total scores, two mediation models and two moderation models were assessed. Behavioral disengagement was selected as a potential mediator, due to its moderate concurrent correlation with PTSS. Substance abuse was also selected as a potential mediator, due to its prevalence in participants’ qualitative responses and public health relevance. Additionally, acceptance and religion were selected as potential moderators, due to their reported high frequency of use at Time 1, and the negative concurrent correlation between religion and PTSS.
Mediation Models
Behavioral disengagement was first considered as a possible mediator of the relationship between COVID-19 stress and PTSS controlling for age, gender, ethnicity, income, and essential employee status (see Table 3). Time 1 COVID-19 stress significantly predicted Time 3 PCL-5 Total scores (R2 = .29, F (9, 171) = 7.84, p < .0001), suggesting that increased stress at Time 1 predicted higher PTSS scores at Time 3. Time 1 COVID-19 stress also trended toward predicting Time 2 behavioral disengagement (R2 = .21, F (9, 66) = 1.90, p = .07), suggesting that higher levels of stress at Time 1 led to greater Time 2 disengagement. Of note, the specific predictive value of Time 1 stress was significant (p = .02). Time 2 behavioral disengagement additionally predicted Time 3 PCL-5 Total scores (R2 = .33, F (1, 48) = 24.06, p < .0001), indicating that greater disengagement at Time 2 led to higher PTSS at Time 3. When both Time 1 COVID-19 stress (p = .0029) and Time 2 behavioral disengagement (p = .0009) were considered simultaneously, both remained significant predictors of Time 3 PCL-5 Total scores, indicative of partial mediation (R2 = .63, F (10, 35) = 5.90, p < .0001).
Regression Analysis: Time 2 Behavioral Disengagement as a Mediator of the Relationship Between Time 1 COVID-19 Stress and Time 3 PTSS.
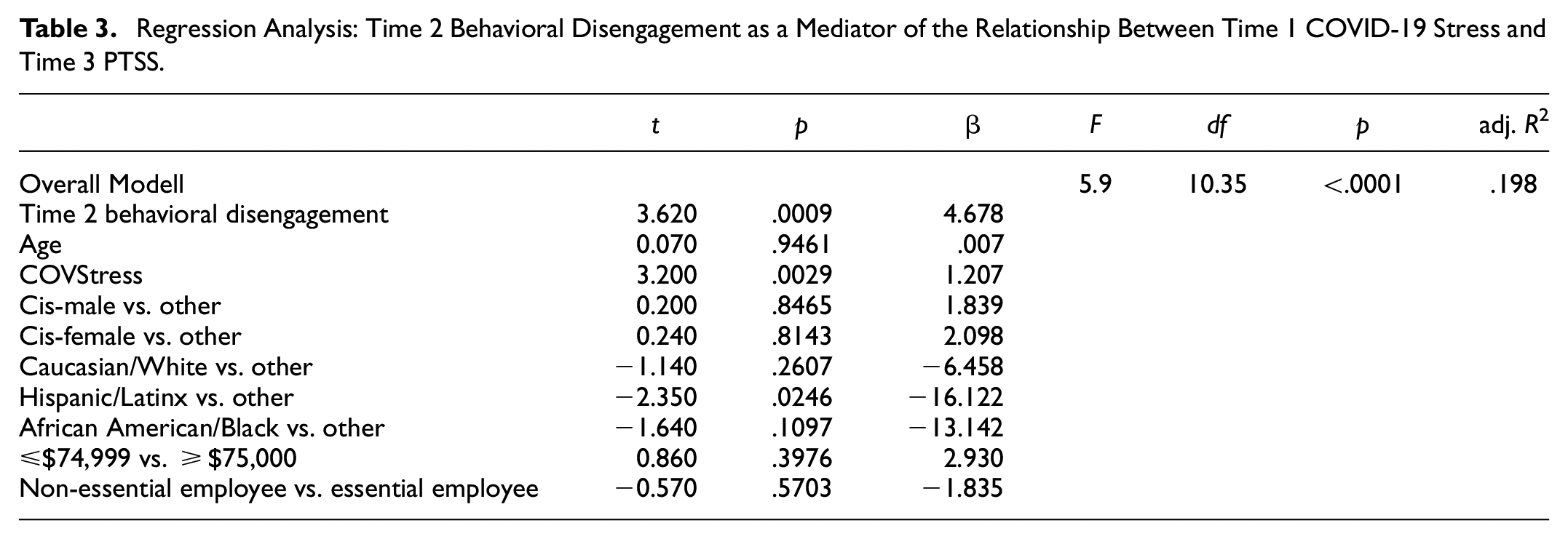
Substance abuse was also considered as a possible mediator. However, Time 1 COVID-19 stress did not significantly predict Time 2 substance abuse (R2 = .08, F (9, 65) = 0.62, p = .78). Similarly, Time 2 substance abuse did not predict Time 3 PCL-5 Total Scores (R2 = .03, F (1, 48) = 1.33, p = .25). As such, Time 2 substance abuse was not identified as a mediating factor in relationship between Time 1 COVID stress and Time 3 PTSS.
Moderation Models
Acceptance was first considered as a possible moderator of the relationship between Time 1 COVID-19 stress and Time 3 PCL-5 Total scores controlling for age, gender, ethnicity, income, and essential employee status (R2 = .32, F (11, 168) = 7.03, p < .0001; see Table 4). The interaction variable of Time 1 COVID-19 Stress and Time 1 acceptance was a significant predictor of Time 3 PTSS (p = .0125). Post-hoc analyses revealed that, at higher levels of Time 1 stress, greater use of acceptance (p < .001) predicted higher levels of Time 3 PTSS.
Regression Analysis for Acceptance as a Moderator Between COVID-19 Stress and PTSS.

Religion was also considered as a possible moderator of the relationship between Time 1 COVID-19 stress and Time 3 PCL-5 Total scores (R2 = .30, F (11, 169) = 6.43, p < .0001). The interaction variable of Time 1 COVID-19 Stress and Time 1 religion was not a significant predictor of Time 3 PTSS (p = .3943), and therefore not a significant moderation effect.
Discussion
Researchers are beginning to report on the emotional and psychopathological responses to the COVID-19 pandemic. This study sought to further elucidate individuals’ long-term stress and coping reactions. Overall, this study identifies the multifactorial stressors individuals experienced in social, career, and medical functioning, and highlights that a portion of the population is reporting significant PTSS. Additionally, it identifies the coping strategies used to manage COVID-19 stress and how certain strategies may increase the likelihood of developing PTSS over time.
Regarding pandemic stress, most of the sample reported concerns about getting sick themselves, while an overwhelming majority were concerned with family members becoming ill. This finding is consistent with Wang and colleagues, who noted that a large majority of their sample expressed concern with family members contracting the disease (Wang, Pan, Wan, Tan, Xu, Ho, & Ho, 2020). Additionally, the current sample identified the accessibility of healthcare as a stressor; this was true both for COVID-19 and unrelated medical needs. Over half of the sample reported concerns about employment and/or their current financial situation. Respondents also noted significant concern with social isolation, for both themselves and others, which has been linked to numerous emotional symptoms (Pietrabissa & Simpson, 2020).
Despite participants’ extensive report of stressors, our sample showed relatively low rates of PTSS, and 13.3%–15.4% met likely criteria for PTSD at Time 1. This is consistent with extant research utilizing the same stringent PTSD assessment tool, the PCL-5 (Liu et al., 2020). Our estimates of likely PTSD are notably lower than some studies, however, which utilized broader assessment tools (Li, 2020; Tan et al., 2020). This suggests that although individuals are experiencing very high rates of stress in response to the pandemic, a much smaller portion of the population may be exhibiting clinically impairing levels of PTSS (Ahmed et al., 2020).
Importantly, COVID-19 stress was positively correlated with PTSS at Time 1, suggesting that those with increased COVID-related stress may be more likely to exhibit concurrent PTSS. Concerning the use of coping strategies at Time 1, participants reported frequently utilizing a variety of positive coping strategies (e.g., active coping, positive reframing, acceptance, religion). Negative strategies (e.g., denial, substance abuse, self-blame) tended to be employed less often, and nearly all coping strategies were correlated with participants’ Time 1 PCL-5 Total scores.
Considering the strength and direction of these relationships, behavioral disengagement and self-blame at Time 1 were moderately, concurrently, positively associated with participants’ PCL-5 Total scores, suggesting that individuals who display symptoms of avoidance, hopelessness/helplessness, and/or self-blame are likely to report higher PTSS. This was confirmed via longitudinal assessment, such that behavioral disengagement at Time 2 was found to partially mediate the relationship between Time 1 COVID-19 stress and Time 3 PTSS. This is consistent with research that has identified behavioral disengagement and avoidant coping, generally, as a risk factor for the development of PTSS/PTSD in both clinical and non-clinical samples (Badour et al., 2012; Batchelder et al., 2021; Viana Machado et al., 2020). Understanding the role of disengagement is particularly important within the context of this global health emergency and highlights the need for coordinated community efforts to keep members connected, within necessary safety constraints.
Time 1 self-distraction, denial, substance use, venting, and planning were weakly, positively associated with participants’ concurrent PCL-5 Total scores. Assessment of substance use as a mediator of the relationship between Time 1 COVID-19 stress and Time 3 PTSS was not significant, however. Future research should consider alternative roles that substance use may have played within the setting of the pandemic. For example, instead of functioning as a mediator, increased substance use may be a potential outcome for individuals experiencing PTSD.
Alternatively, Time 1 use of positive reframing, religion, and acceptance were not correlated with concurrent PCL-5 Total scores. Further, despite previous findings that reliance upon religion may reduce fear and social isolation, religion was not found to function as a significant moderator of the relationship between Time 1 COVID-19 stress and Time 3 PTSS in this study (Lucchetti et al., 2021). This suggests that the relationship between COVID-19 stress and the subsequent development of PTSS was similar for individuals, regardless of the extent to which they relied upon religion as a coping strategy.
Finally, acceptance was identified as a moderator of the relationship between Time 1 COVID-19 and Time 3 PTSS in an unexpected direction. Specifically, at higher levels of Time 1 stress, greater use of acceptance predicted higher levels of Time 3 PTSS. This finding was counterintuitive, given the typically positive benefits of utilizing acceptance as a coping strategy (Umucu & Lee, 2020). Within the context of the pandemic, however, acceptance of the current state—particularly prior to the introduction of vaccines—may have translated to feelings of helplessness and lack of control, both of which are hallmarks of traumatic experiences and predictors of PTSD (Le et al., 2018; Salcioglu et al., 2017). This is consistent with emerging literature that there may be two subsets of acceptance coping: active acceptance and resigning acceptance (Nakamura & Orth, 2005), whereby resigning acceptance may be linked to poorer psychological outcomes.
Several study limitations merit comment. First, this study relied on survey data from a community sample. Our sample was composed of predominantly upper-middle class White, non-Hispanic females, and thus, it is unclear how these results may generalize to more diverse groups.
Second, although our Time 1 sample was large, the number of participants who provided data at all three timepoints was substantially smaller. The participants who completed all three time points may have been particularly motivated to participate for a variety of reasons (e.g., especially strong coping; particularly high distress), which may have resulted in a self-selection bias. Future studies would benefit from additional consideration regarding how to reduce participant attrition within the context of substantial stressors.
Third, missing data may account for underreporting of PTSS and coping strategy use. This may be particularly true on the Brief-COPE, as many participants did not complete all items to inform the subscales.
Concerning the application of study findings, community-wide education regarding common stress symptoms is critical. Information should be disseminated regarding which types of symptoms are clinically concerning, as well as ways to connect with mental health providers. Suggestions regarding beneficial coping strategies, such as focusing on health behaviors, positive reframing, and targeted community efforts to support safe, socially-distanced community engagement will also be necessary. Alternatively, education on the potential risk of engaging in avoidant coping, such as behavioral disengagement, will be equally important.
Considering future directions, the current investigation included open-ended free response prompts for qualitative data collection. The research team plans to report on this data in a future publication, as it may provide further detail regarding the multitude of stressors, emotional responses, and coping strategies employed by respondents.
Research Data
sj-docx-1-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-docx-1-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-docx-2-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-docx-2-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-pdf-3-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-pdf-3-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-pdf-4-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-pdf-4-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-pdf-5-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-pdf-5-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-pdf-6-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-pdf-6-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-pdf-8-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-pdf-8-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Research Data
sj-pdf-9-sgo-10.1177_21582440231221323 – Supplemental material for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment
sj-pdf-9-sgo-10.1177_21582440231221323 for Post-Traumatic Stress Symptoms and Coping in the Time of COVID-19: A Longitudinal Assessment by Whitney M. Herge, Emily B. Gale, Emily J. Stapleton, Ashley Ofori, Kiley F. Poppino, Shelby P. Cerza and Daniel J. Sucato in SAGE Open
Footnotes
Acknowledgements
There are no other parties or third parties to acknowledge for this study.
Author Contribution
Kiley Poppino and Shelby Cerza assisted with study design, data collection, and manuscript preparation. Drs. Whitney Herge, Emily Gale, and Emily Stapleton assisted with study design, statistical analysis, and manuscript preparation. Ashley Ofori assisted with manuscript preparation. Dr. Daniel Sucato assisted with manuscript preparation and oversight.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the University of Texas Southwestern Medical Center Institutional Review Board. The committee approval number is STU-2020-0320.
Pre-registration
This study is not pre-registered. It is not an experimental study.
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
The current article is accompanied by the relevant raw data generated during and/or analyzed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.