
Abstract
The epidemiology of suicide could provide interesting data for societies that are undergoing significant demographic transformations. The main purpose of this study was to analyze the scale of and trends in suicide in Italy during the period 1979 to 2016. The secondary aim was to compare rates and methods of suicide in the elderly with those in other age groups. This was a population-based study on suicide for the period 1979 to 2016. Data on suicide regarding gender and age from the Italian Institute of Statistics and the World Health Organization were examined with linear regression and ANOVA test. The data on the elderly were compared with those for other age groups. Linear regression revealed a significant decline in the overall suicide rate (F = 180.6; p < .0001). The 45 to 54 age group accounted for the highest suicide rate in recent years (2003–2016). The second highest incidence was among the elderly, with the “young” elderly (65–75 years old) having the highest suicide rate in this group. The male-to-female suicide ratio increased proportionally with age. Hanging was the suicide method most frequently employed independently from age groups. Universal and selective preventive strategies could be developed on the basis of the results of this study. The sensitization of health professionals, families, and friends to specific circumstances could contribute to the decline in the incidence of suicide in specific circumstances of time and place. Further studies are needed in order to better understand social and clinical risk factors related to the risk of suicide in specific age groups.
Introduction
Suicide is a serious world health issue that affects individuals from early adolescence to old age (World Health Organization [WHO], 2021). In Italy, approximately 4,000 people die by suicide each year (Italian Institute of Statistics [ISTAT], 2019). Considering the manner of death, as classified by death investigation, suicide is the third cause of death in Italy, coming after natural and accidental, and before homicide (ISTAT, 2019). Suicide is relevant as not only a health issue but also a medicolegal issue. It is considered a differential diagnosis from homicide (fewer than 400 homicides were reported in Italy in 2017) and may be related to professional liability (Terranova & Sartore, 2013) in the cases of deaths acknowledged as preventable.
The highest suicide rates have been observed in the elderly (Terranova et al., 2012), with a preponderance of men with regard to the more lethal methods (Terranova et al., 2012). This phenomenon has been observed in most countries (Conejero et al., 2018) even though the pattern can vary (Conwell et al., 2011). For example, a peak in the suicide rate in Canada and, in recent years, the United States of America, has been seen in individuals at midlife (Conwell et al., 2011). Countries with an existing or emergent high mean age and low birth rate could face a potentially preventable important health issue in the near future. Italy, which has the fifth highest (of 226 countries) median age and one of the lowest birth rates, must consider the potential negative effects of suicide on health and the society in general.
Suicide is a multi-determined phenomenon, and the reasons for its occurrence become more complex in older adults (Van Orden & Conwell, 2016). With the stress–diathesis model of suicidal behavior, a negative stressful life event, particularly among individuals with distal risk factors, is recognized as a trigger for such behavior (van Heeringen, 2012). Epidemiology could contribute to the identification of the distal risk factors and, thus, suicide prevention. The knowledge of gender rates, methods, and risk or protective factors (e.g., the presence of disease) could be the starting point for the development of preventive strategies. Such information could also be significant in the contexts in which suicidal ideation and conduct have been frequently reported (Kennedy et al., 2014; Lohman et al., 2016). Preventive strategies in homes can include physical barriers in instances of recurring demonstrations of suicide methods (e.g., jump from height; Beautrais, 2001). The improvement or development of clinical preventive procedures and psychological care for patients who epidemiologically are at a higher risk (e.g., male, low education levels) can also play an important role (Terranova et al., 2012). The epidemiology of suicide could offer interesting insights into those societies, such as Italy, that are characterized by significant demographic transformations. In Italy, the proportion of people aged 65+ has increased from 12.8% in 1979 to 22.8% in 2019 (ISTAT, 2019).
Elder suicide is not a homogenous phenomenon (Koo et al., 2017); thus, the analysis was focused on not only the general category “elderly” (individuals aged 65+) but also on the subcategories. Differences in gender, methods, and risk factors could exist for the young-old (65–74), middle-old (75–84), and oldest old (85+ years), as highlighted by Koo et al. (2017). The choice of method is likely influenced by age, with late-life suicidal behaviors characterized by an increase in lethality (Van Orden & Conwell, 2016). The choice of a method might depend on its availability (Yeum et al., 2018). It might also be influenced by other factors, such as acceptability of the method, knowledge of the likely lethality, and seriousness of intent (Brown Henriques et al., 2004; Yeum et al., 2018). The lethality of a method is related to the inherent deadliness, ease of use, and possibility for aborted attempts.
According to the assumptions made above and with the aim of providing novel insights into understanding of the epidemiology of suicide, the main purpose of this study was to analyze the scale and trends of suicide in Italy from 1979 to 2016. The secondary aim was to compare methods and suicide rates in the elderly with those in other age groups. The results could contribute to the development of prevention strategies.
Methods
This was a population-based study of deaths by suicide in Italy during the period 1979 to 2016. The data were obtained from the World Health Organization (WHO, 2019) and the Italian Institute of Statistics (ISTAT, 2019). ISTAT, a public research organization and main producer of official statistics for use by citizens and policy makers, provides the data, which are published and elaborated by the WHO. The source of the data is the form completed by physicians regarding “deaths and causes of death” (Terranova et al., 2012). Death certificates are filled out by the general practitioner or specialist physician in cases of natural death, and sometimes in cases of death by suicide; alternatively, they are filled out by the coroner in cases of violent death (homicide and suicide). The data employed met the criteria of the WHO and the European Community, including those regarding quality. Suicide was classified according to the 10th revision of the International Classification of Diseases and Related Health Problems (ICD-10; WHO, 2004). The data are provided free of charge to users. They are available on the WHO and ISTAT websites as interactive worksheets that can be extracted as Excel spreadsheets (Terranova et al., 2017).The suicide phenomenon was analyzed with regard to age, gender, and method. The aggregate numbers of suicide by gender, age-group, and method, but not individual level data, were available On the basis of the available data, the variables were studied for the following periods:
✓ 1979 to 2016: Gender and age-group data were extracted from the WHO database. The following age groups were considered: 5 to 14, 15 to 24, 25 to 34, 35 to 54, 55 to 74, and 75+. Notably, for 2003 to 2016, the data were also provided for 10-year age intervals (e.g., 45–54, 55–64, 65–74, 75–84, and 85+).
✓ 1993 to 2015: The suicide methods used in this period were extracted from the WHO and ISTAT databases. The age groups relating to suicide statistics were 0 to 24, 25 to 44, 45 to 64, and 65+. Data for specific methods of suicide were only available for this period for the age groups combined. However, for the years 2011 to 2016, and for age groups 15 to 34, 35 to 64, and over 65, data relating the methods of suicide to age groups were available.
Direct standardization for all the age groups was performed in accordance with the European Standard Population 2013 (Eurostat, 2013). The data were analyzed by linear regression, with the standardized suicide rate (grouped by variables such as age and gender) as the dependent variable and time as the independent variable. The t-test and the analysis of variance (ANOVA) with the Bonferroni correction were used for the comparisons of the mean suicide rates for the gender and age groups (Otzen et al., 2015) and for the different methods of suicide . Effect sizes were calculated using r square for linear regression and the ƞ square for ANOVA. All of the analyses were performed with IBM SPSS Statistics 25.0 for Windows, Version 25.0 (Armonk, NY; IBM Corp, 2012) and GraphPad Prism 8.0.0 for Windows (GraphPad Software, San Diego, CA; www.graphpad.com).
Results
From 1979 to 2016, individuals aged 75+ were 7.6% of the Italian population; however, they represented 17.8% of the total number of suicides (28,726 of 160,943 cases) with an annual mean and standard deviation (SD) of 755.94 ± 89.57 cases. After direct standardization, the mean ± SD suicide rate for individuals aged 75+ was 1.65 ± 0.41 per 100,000. The results of the linear regression revealed a significant decline in the overall suicide rate (F = 180.6, r2 = .833; p < .0001). A significant decline was observed in the 75+ age group (F = 138.9; p < .0001), 25 to 34 (F = 12.38, r2 = .794; p = .0012), 35 to 54 (F = 18.38, r2 = .339, p = .0001), and 55 to 74 (F = 235.4, r2 = .867; p = .0001). In contrast, the suicide rates for individuals aged 5 to 14 and 15 to 24 were stable during the study period (r2 = .054 and .017, respectively). Figure 1 shows the suicide trends per 100,000 according to the age groups.

Trends of suicide per 100,000: 1979 to 2016.
The male and female suicide trends for 1979 to 2016 are presented in Figures 2 and 3. In the 37 years observation period deaths due to suicide were more frequently observed in individuals aged 35 to 54 and 55 to 74, followed by subjects aged 75 and over (η2 = .911, p < .0001). By ANOVA male died by suicide more frequently than female, irrespective of age group (p < .0001).

Suicide trends per 100,000: 1979 to 2016 according to gender: (a) suicide trends per 100,000 in males and (b) suicide trends per 100,000 in females.

Male and female suicide trends per 100,000 in groups 55 to 74 and 75 and over from 1979 to 2016.
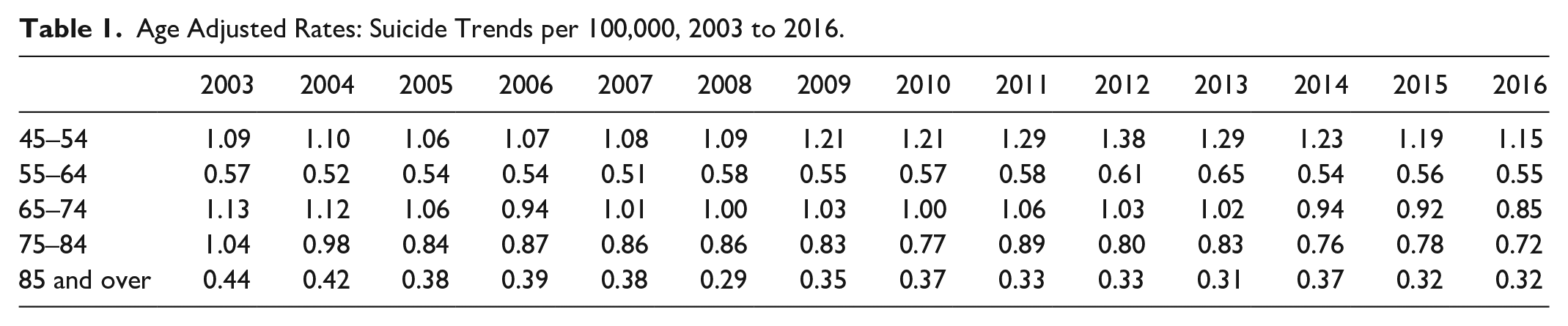
To highlight the influence of age on the observed trends and to provide a deeper explanation of the phenomenon, the adjusted rates for the 45 to 54, 55 to 64, 65 to 74, 75 to 84, and 85+ age groups during 2003 to 2016 were analyzed (see Table 1 and Figure 4 for the results). The comparisons of the males and females in the 45 to 54 and 65 to 74 age groups (see Figure 5) revealed an increase in the suicide rate for males aged 45 to 54. The mean male-to-female suicide ratio tended to increase with age: 3.33, 3.47, 5.37, and 8.33 for the 45 to 54, 65 to 74, 75 to 84, and 85+ age groups, respectively.
Age Adjusted Rates: Suicide Trends per 100,000, 2003 to 2016.

Suicide trends per 100,000: 2003 to 2016.
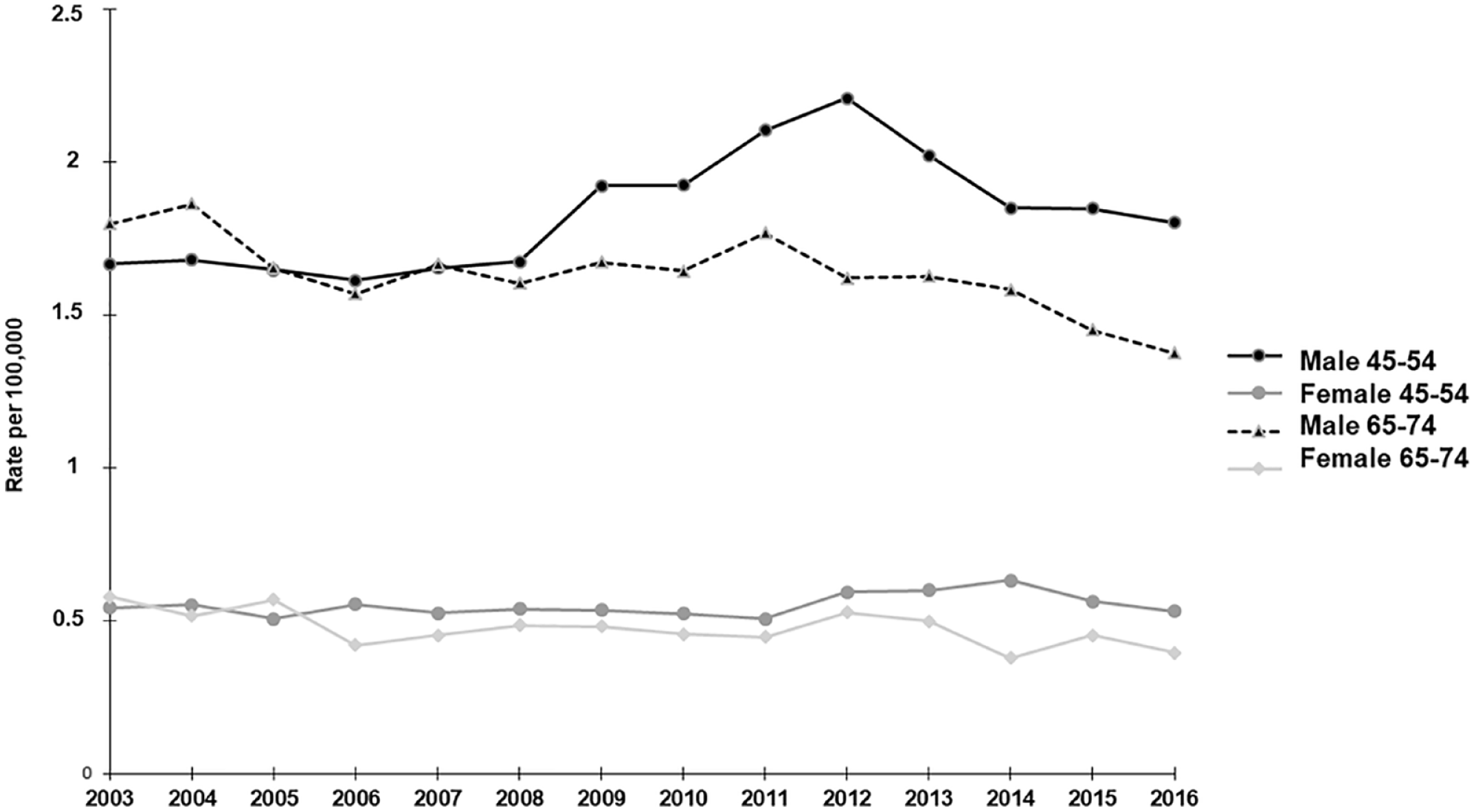
Suicide trends per 100,000, male versus female: 2003 to 2016.
The mean crude rates per 100,000 for hanging, jump from height, use of firearms, poisoning, drowning, motor vehicle crash, and use of sharp objects were 3.18, 1.52, 0.94, 0.62, 0.36, 0.21, and 0.13, respectively, with an overall crude suicide rate of 7.20. A decline was observed for almost all of the methods (F = 29.71, r2 = .585; p < .0001) except hanging (F = 0.080, r2 = .003; p = .77) and the use of sharp objects (F = 2.84, r2 = .119; p = .10; see Figure 6).

Methods of suicide, crude rate per 100,000: 1993 to 2016.
The crude rates showed that among males the three most used suicide methods were hanging (5.48), firearms (1.86), and fall from height (1.83). For females, they were fall from height (1.23), hanging (1.02), and poisoning (0.36). Regarding gender, the trends observed for the suicide methods used by males were the same as those for the total sample (r2 = .426, p = .0007). For females, there was a significant decrease in hanging (F = 15.35, r2 = .422; p = .008) but stability in the incidence of motor vehicle crashes and the use of sharp objects (r2 = .057 and .001, respectively). When analyzing the method of suicide in the different age groups by ANOVA, after direct standardization in 2011 to 2015, we confirmed that hanging was the most frequent method of suicide in all age groups (15–34 years: p < .001, η2 = .988; 35–64 years: p < .001, η2 = .996; 65 and over: p < .001, η2 = .989). In the analysis by age groups and gender, hanging was the first methods of suicide in female aged 15 to 34 and 35 to 64 (p < .001, η2 = .955; p < .001, η2 = .975), and jump from heigh in those aged 65 and over (p < .001, η2 = .974). In the analysis of trend of suicide over time according to the method used and the period analyzed, we observed a decrease in suicide rate in elderly (p = .006, F = 26.33, r2 = .868).
Discussion
Suicide is a complex phenomenon caused by the interaction of biological, psychosocial, cultural, and environmental factors (Aguglia et al., 2019). Although the role of the multiple factors involved in suicide are not fully understood, the results of epidemiological studies can highlight the risk factors at the local and national levels. The present study contributes to the analysis of the phenomenon of suicide in Italy over a relatively long-time span. The focus on the elderly, defined as individuals over 65 years old (Terranova et al., 2017), is important because of the demographic characteristics of the Italian population and the incidence of the phenomenon in this specific group as demonstrated in previous studies (De Leo et al., 2020). Together with an analysis of suicide by gender and age group, the study of the main methods of suicide identified in this work could be used to develop preventive strategies.
The overall suicide rates declined between 1979 and 2016. This was consistent with worldwide trends (Bremberg, 2017; WHO, 2019) with the exception of data from the region of the Americas. The global data could be related to higher attention being paid to mental health through the development of suicide prevention programs (Fond et al., 2016). According to WHO (2014), interventions for suicide prevention, based on risk factors, could be subdivided into universal (targeting the entire population), selective (for specific vulnerable groups), and indicated (targeting vulnerable individuals). In Italy, the decline in the phenomenon of suicide could be related to important changes in mental health policy that began in 1978 with the reform of the mental health system. According to some authors (Ronchetti et al., 2020), in the early years, the reform was associated with an increase in suicide rate. However, it drastically changed the mental health system by shifting the care of mental illness onto the community and by trying to modify the image of the psychiatric patient. The concept of the patient as being dangerous to himself and to others was eliminated, and it became well established that, for the psychiatric patient, as for all patients, health treatment has to be based on the person’s rights as well as on respect for human rights (Volpe et al., 2014).
The decline in the elderly male and female suicide rates paralleled the overall positive trend. The stability of the suicide rates for young individuals (15–24) should be interpreted with caution because suicide is the second leading cause of death in this age group (WHO, 2021).
In the latest years (2003–2016), the highest suicide rate was observed in the 45 to 54 age group. These results are consistent with those of previous studies (Mattei et al., 2014; Pompili et al., 2014) and with the data of other countries (WHO, 2021). The increase in the incidence of suicide in males aged 45 to 54 in 2008 to 2014 could explain the highest rate observed in this age group. . This period was characterized by an economic crisis during which many countries, including Italy, experienced a decrease in the gross domestic product and an increase in the unemployment rate (Mattei et al., 2014). Gross domestic product at market prices (Eurostat, 2021) fell in 2009, and by 2014 the value was still below that of 2008. The unemployment rate (ISTAT, 2019) increased from 6.1% in 2007 to 12.7% in 2014. Alongside the aforementioned factor, social and family changes as well as specific clinical conditions should be carefully analyzed to provide possible reasons of the suicide.
Age differences were found in the elderly suicide rates (Koo et al., 2017). The incidence of suicide among the young-old (65–74 years; Koo et al., 2017) was higher than that in the 75+ group after direct standardization in contrast with a crude rate higher in subjects older than 75 compared to the other groups. The different suicide rate observed for those over 75 might be related to the prevalence of potential risk factors that are specific to the various elderly groups (Koo et al., 2017). Another possible explanation might be the influence of the differences in the mean ages of the females and the males (females, 84.3; males, 79.1 in 2010). This has implications for the composition of the population and, thus, the suicide rates.
The analysis confirmed that male-to-female suicide ratio increased proportionally with age. In elderly the highest ratio was observed for the 85+ age group (male-to-female suicide ratio superior to 8). These data confirm the results of previous studies (Didier et al., 2012; Martini et al., 2019). They are also consistent with the world risk ratio of 3.2 for sex, with higher rates for older men (Martini et al., 2019; WHO, 2014). Gender-related differences could result from poor ability to diagnose depressive symptoms in men (Streb et al., 2021). This hypothesis arises from the evidence that suicide can be associated with depressive symptoms, and that women, who are diagnosed as suffering from depression more frequently than men, die less from suicide than men. Therefore, an earlier diagnosis of depression, using appropriate tools, could be a useful preventive measure (Möller-Leimkühler & Mühleck, 2020).
As has been suggested by other studies (Crestani et al., 2019; De Leo et al., 2020), the results in elderly might also reflect women’s ability to maintain their roles in the family and society after retirement. In contrast, men might experience feelings of uselessness (Martini et al., 2019).
Studies show consistently that hanging is the suicide method most frequently employed (Koo et al., 2019; WHO, 2014). This is followed by falling from a height and the use of firearms. The frequency reflected in these data might be attributed to the simplicity, availability, and speed of hanging, which is compatible with impulsive behaviors. The relative socio-cultural acceptability of this method of suicide could play an additional role, as has been suggested by other authors (Gunnell et al., 2005). The fact that rates for suicide by hanging, which has been the preferred method for men and the second most preferred method for women, have been relatively stable, is deeply concerning and suggests that there has been a failure to tackle this phenomenon. The stability of the data could be explained by a comparison with other methods of suicide that have been hindered by preventive strategies (Gunnell et al., 2005). It is more feasible to implement the prevention of suicide by other methods than it is to restrict all means of hanging (WHO, 2014). For example, structural interventions restricting access to bridges or high buildings can be effective in preventing suicide by jumping, as can the lack of access to poisonous gases (WHO, 2014). Hanging, apart from cases that take place in controlled environments, such as hospitals and prisons, is seldom avoidable through restricting access to the means of this method. Hanging is thus rarely preventable immediately prior to the fatal event (Kosky & Dundas, 2000), and the strategies to be adopted should be based on universal interventions focusing on raising awareness about mental health, improving mental health policies, and probably, responsible media reporting (WHO, 2014). Preventive strategies through a selective intervention could be directed to specific populations at risk on account of individual, familial, and social risk factors.
The decline in the use of other suicide methods was a positive fact that was consistent with the decline in the overall suicide rates. In some cases (e.g., intoxication), the data could reflect increased caution around the use of psychotropic drugs. In other cases (e.g., jump from height), the decline could be a consequence of the construction of physical barriers in dangerous locations to address the problem (Stenbacka et al., 2018). The reduction in the number of gunshot suicides appears to be a consequence of the overall reduction in the number of suicides observed rather than the consequence of prevention strategies targeting this method of suicide. In fact, Italian legislation has not changed over the years in the period considered, although undoubtedly, a case of homicide-suicide by firearm, in which the physician who authorized the possession of the gun by the murderer was found guilty of manslaughter, sparked a debate at the judicial level and probably among clinicians releasing licenses to possess a firearm (Terranova & Rocca, 2016).
The results of the present study can be useful for revealing the epidemiologically related risk factors for suicide considering the age groups, gender, and methods of suicide.
Trends observed in various age groups, especially for the age group 45 to 54, merit additional study from the perspective of prevention and trying to deepen an understanding of the social and clinical variables that are linked to suicide risk. As previously reported, preventive interventions should consider hanging, as it is the primary method of suicide in this particular age group, requiring both universal and selective interventions. In Italy, as in other countries, there is little evidence of suicide prevention programs targeting hanging.
Another age group at risk for suicide is represented by the elderly. The predominant suicide methods in the elderly confirmed the overall Italian data (hanging followed by jump from height and use of a firearm). Even if difficulties in preventing hanging are the same as for other age groups, preventive strategies for this group could be carried out with greater efficacy because the elderly are usually in greater contact with the healthcare system. Health workers, such as general practitioners or those who care specifically for the elderly (geriatricians, nurses, general practitioners, and other health professionals working in geriatric units or senior citizens’ homes) (Frénisy & Plassard, 2017; Raue, 2019) should be aware of the groups that are considered to be at risk for suicide (e.g., males aged 65 and above) and the methods most frequently used (jump from height in females, hanging in males). In this group of subjects, interventions can be indicated following the evaluation of an individual (e.g., for mental disorders, substance use disorders, and previous suicide attempts) and relational (e.g., social isolation and lack of a familial support) risk factors. In residential communities and nursing homes, the use of jump from height, the method more frequently employed by women, could be forestalled by the construction of physical barriers (Stenbacka et al., 2018). The development of procedures or protocols for retirement homes could be an approach to prevention.
The possession and availability of firearms, indipendently from the age group should be investigated and evaluated, given the presence of other risk factors. Restrictive firearms legislation could be an important part of a country’s suicide prevention program (König et al., 2018), and these choices could be reflected in the elderly population and in male mid-life subjects.
Strengths and Limitations of the Study
The analysis of the phenomenon of suicide in Italy over a relatively long-time span is a point of strength of the study, as is the analysis of the method of suicide. The results of the analysis suggest the importance of epidemiological studies for monitoring the phenomenon and in the development of preventive strategies.
The limitations of the study relate to the source of its data. The study is based on death certificates filled out by physicians. The identification of the manner of death by suicide and thus, the number of cases to be considered in the study, is not always easy to assess. These difficulties may be experienced by the medical examiner and more frequently by the general practitioner. Thus, the real number of suicide decedents is not identifiable and is likely to be underestimated. Moreover, the data concerning the methods of suicide are not comparable to those for the period 1979 to 2016 in which different age groupings were given.
In conclusion, the highest suicide rate in recent years was observed for individuals in the 45 to 54 age group. The elderly had the second highest suicide rate overall, with the young elderly (65–75 years old) having the highest rate, after direct standardization, within this group. The male-to-female suicide ratio increased proportionally with age, reaching a value of approximately eight after 75 years. The suicide rate, including that for the elderly, started to decline in 1980 . Hanging was the method most frequently used by the elderly, followed by fall from height. The fact that rates for suicide by hanging have been relatively stable, is deeply concerning, and suggests that there has been a failure to tackle this phenomenon.
Universal and selective appropriate preventive strategies could be developed on the basis of the findings from this study. Specifically, an increase in the awareness of health professionals (in particular, general practitioners), families, and friends could make a positive contribution to the decline in the phenomenon in subjects living in specific context. Further studies are needed in order to better understand social and clinical risk factors related to the risk of suicide in specific age groups.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No grant was provided by funding agencies in the public, commercial, or non-profit sectors for this study.