
Abstract
The aim of this study is to determine the reliability and validity of the Adapted Turkish “Students’ Attitudes Towards Addressing Sexual Health” questionnaire (SA-SH-TR). This methodological study was conducted in two stages. In the first stage, the language was adapted to Turkish. Second, the reliability of the scale was evaluated. From January 2018 to March 2018, 292 nursing students volunteered to participate in the study. The content validity index of the Turkish version of the questionnaire ranged from 0.76 to 1.00 and was found to be high. Cronbach’s alpha coefficient was 0.89. Removal of Items 11, 12, 14, 16, 17, 18, 20, and 22 would have improved alpha to 0.91. It was observed that the item-total correlation values of the items changed between 0.24 and 0.75. Test–retest interclass correlation coefficient was 0.83. The study findings determined that the Turkish adaptation of the SA-SH-TR was valid and reliable and could be used in nursing research and practice.
Introduction
Sexuality is a significant yet complex aspect of human experience (Holland, 2019). Problems in sexuality and sexual health can negatively affect individuals’ lives (Ören et al., 2018). Health care professionals must identify sexual problems to provide relevant counseling to patients and their families or partners. However, evaluations, diagnoses, and nursing interventions for sexual health problems are often omitted from routine treatment and care (Sung et al., 2015). Therefore, detailed diagnoses are often excluded, and the subject of such problems may be avoided from the patients entirely. However, health care professionals play a key role in diagnosing and counseling for sexual health problems.
Individuals are often unable to discuss sexuality and sexual health problems clearly and comfortably (Holland, 2019). Initiating and continuing communication about sexual health is difficult for many people, especially in particular groups, such as nursing students (Ören et al., 2018; Soundy et al., 2013). Many nursing students are still in their adolescence. In addition, there are multibarriers for nursing students initiating communication about sexual health. These are lack of knowledge about sexual health, sexual health assessment is not nurses’ responsibility, nursing students feel uncomfortable with sexual health assessment, cultural or religious reasons, social restrains prevent talks about sexual topics, gender difference (male-female) between nursing students and patients (Atlı Özbaş et al., 2016; Bdair & Constantino, 2017). Therefore, their attitudes and behaviors toward sexual health result in difficulty communicating about the subject (Bal & Sahiner, 2015). Because nursing students are often adolescents, their sexual identities and development are not yet complete; however, students preparing for health care professions should be knowledgeable about sexuality and sexual health problems (Ören et al., 2018). Furthermore, maintaining professional boundaries is essential when addressing sexual health issues. Previous research regarding nursing students related to sexual health and sexuality shows the importance of competence in this field for health care workers and therefore is a need to explore students’ attitudes, knowledge, and view on working with sexual health in their future profession (Areskoug-Josefsson et al., 2019). Health care students should be equipped with sufficient knowledge to feel confident that they are upholding professional boundaries while working with sexual health issues—despite the sensitivity and hands-on practice that nursing often requires (Soundy et al., 2013). Many nursing students avoid communicating about sexual health with healthy or sick patients for a variety of reasons, such as embarrassment, confidentiality, and incompetence (Areskoug-Josefsson et al., 2016; Çuhadaroğlu, 2017; Holland, 2019; Khadivzadeh et al., 2016; Kong et al., 2009; Süt et al., 2015). A study on nursing students’ sexual health evaluation skills reported that structured education programs positively affect students’ attitudes about sexual health (Tugut & Golbasi, 2015).
Important nursing responsibilities include counseling patients to help treat sexual health problems and maintain their sexual health. Nurses can assess patients’ sexual health to identify existing problems and risk factors, and they can also counsel patients about necessary precautions for sexual developmental and reproductive health (Erenoğlu & Bayraktar, 2017). However, although nurses are aware of these potential nursing roles, many nurses do not consider such roles to be nurses’ professional responsibility (Nakopoulou et al., 2009). Haboubi and Lincoln (2003) reported that 90% of nurses do not consider sexual health part of health care and that 94% do not discuss sexual health–related issues with patients. In addition, many nurses lack adequate knowledge to discuss sexuality and cannot make sexual health diagnoses due to a lack of specific assessment guidelines or a fear of increasing patients’ anxiety (Jaarsma et al., 2010). A study by Saunamäki et al. (2010) reported that nurses did discuss sexuality with patients due to time limitations. At last decades, various studies on nurses’ attitudes toward sexuality and sexual health have been conducted in Turkey (Atlı Özbaş et al., 2016; Çuhadaroğlu, 2017; Erenoğlu & Bayraktar, 2017; Ören et al., 2018). These studies emphasized that nurses do not make sexual health diagnoses and do not communicate with patients about sexual health because they feel this topic should be confidential patients and their family and their physicians. Another nation-wide study in Turkey found that the number of individuals who seek treatment at health institutes for sexual health issues was very low (12%); moreover, 70% of men and 57% of women felt that health professionals should initiate questions about sexuality, rather than patients themselves (Turkey Family Health and Planning Foundation, 2011).
Culture and religion can also negatively affect sexual health communication (Bozdemir & Özcan, 2011). Indeed, Turkish nursing students consider sexuality a taboo and refrain from discussing this topic (Bal & Sahiner, 2015). Studies in Turkey have shown that traditional nursing education does not change students’ attitudes toward sexual health (Atlı Özbaş et al., 2016). Therefore, establishing new sexual health education programs within Turkish nursing education is imperative (Yanıkkerem & Üstgörül, 2020). Although there are a few measuring sexual attitude and studies conducted in different groups, psychometric studies have been found with these and similar scales in samples such as nursing, social worker, and physiotherapy regarding the evaluation of sexual health (Areskoug-Josefsson et al., 2019; Blanc et al., 2018; Fino et al., 2018; Fisher et al., 2013; Gerbild et al., 2017; Shah et al., 2020). However, the nursing education in Turkey part of this scale has been decided that the most appropriate scale for students. Adequate measurement tools are also needed to accurately analyze nursing students’ attitudes. However, the development of a new scale to properly assess attitudes presents a challenge. Such scales must use reliability and validity that are well identified in the literature and have been adapted to Turkish society (Erefe, 2002).
Method
Study Purpose
Adequate measurement tools are needed to accurately analyze nursing students’ attitudes about sexual health. This study aimed to determine the reliability and validity of the Turkish version of the “Students’ Attitudes Towards Addressing Sexual Health Questionnaire” (SA-SH-TR).
Study Design
The study’s participants comprised 1,213 students at a nursing facility in Istanbul during the 2017–2018 academic year.
In scale studies, participants’ sample size should be at least 10 times the number of items included in a study’s design (Child, 2006). Considering possible losses with a total of 292 nursing participants and a scale of 22 items at a 0.50, a power of 0.95, and an α of 0.05, the test–retest correlation assumption in the current study determined a required sample size of at least 42 participants (Faul et al., 2007). Students from all classes were included using a stratified sampling method. Participants who provided informed consent for interviews were included in this study.
Ethical Considerations
Permission was obtained from Areskoug-Josefsson to use the SA-SH questionnaire and to translate it into Turkish. Furthermore, written permission was acquired from the nursing faculty where the study data were collected. This study was approved by the Istanbul University Faculty of Dentistry Clinical Research Ethics Committee (Date: November 31, 2017, Number: 226/61).
Translation Procedures: Language Equivalence and SA-SH Content Validity
The SA-SH scale was translated from English to Turkish and from Turkish to English by two experts who were professional translators. The re-translation of the form back into English after translation into Turkish was done by two bilingual experts (Bolarinwa, 2015). Next, the adapted Turkish scale was examined by an academic member of the field and an expert in the Turkish language and Turkish literature, who provided suggestions for the final version. Finally, 13 academician academic members whose fields are in nursing were asked for their opinions on the Turkish version of the scale’s content validity. For information on these expert opinions, see the Content Validity Index (CVI).
Instruments: SA-SH–Based Student Assessment Form
The resulting form comprised 10 questions concerning students’ age, gender, class, marital status, income status, family type, parents’ educational backgrounds, working status, and place of residence.
The original SA-SH scale was published in Sweden in 2015 by Areskoug-Josefsson et al. under the title “Students’ Attitudes Towards Addressing Sexual Health (SA-SH).” The original scale’s questions were designed to measure both positive and negative attitudes toward sexual health. The questionnaire comprises 22 questions about attitudes, feelings, and thoughts regarding sexual health discussions with future patients.
The SA-SH uses a 5-point Likert-type scale ranging between 1 (disagree) and 5 (strongly agree). Respondents’ minimum number of points using the scale is 22, while the maximum is 110. A higher total correlates with positive attitudes toward sexual health behaviors. The scale’s reliability was evaluated through the test–retest method. Intrarater reliability was tested via Elisabeth Svensson’s test–retest method and attributed to factors found in the construct validity test (Özdamar, 2003; Özdemir, 2005). This method was selected to analyze the test-retest results. Significance was set at p < .05. Items numbered 9, 10, 11, 12, 13, 16, 17, and 18 were identified as negatively worded questions and scores of the items were reversed. A construct validity analysis was based on three main factors: present feelings of comfort, future working environment, and fear of a negative influence on future patient interactions. Construct validity was investigated through exploratory factor analysis (EFA) and principal component analysis. Internal consistency reliability was analyzed via Cronbach’s alpha with a coefficient of 0.71. Descriptive statistics were evaluated using SPSS 22 with Cronbach’s alpha and EFA (Areskoug-Josefsson et al., 2016).
Data Collection
In total, 292 students agreed to participate and were included in the present study. Written and verbal informed consent were obtained from these students. The data collection phase took place in students’ classroom at the end of their course. For test–retest evaluation, the same questionnaire was provided to 50 students in their classroom 3 weeks later, which concluded the data collection phase.
Analysis
IBM SPSS Statistics 22 and SPSS AMOS 22 (IBM SPSS, Turkey) were used for statistical analysis. The normality of distribution was evaluated using the Shapiro–Wilk test. Descriptive statistical methods—such as mean, standard deviation, and frequency—were used to evaluate the research data. To determine scale validity, EFA was applied. To determine the scale’s construct validity, confirmatory factor analysis (CFA) was used. To analyze reliability, Cronbach’s alpha interpretation was used to evaluate internal consistency. To determine item correlation, Pearson’s correlation analysis was used. To determine test–retest reliability, intraclass correlation (ICC) was administered, and p < .05 was assumed to be significant (Akgül & Çevik, 2005; Özdamar, 2003; Özdemir, 2005).
Results
Participants’ mean age was 20.46 ± 1.64 (ranging from 17 to 29) and 82.9% of participants were female. Of the participants, 28.4% were first-year students, 22.6% were second-year students, 23.6% were third-year students, and 25.3% were fourth-year students. Only 1% of participants were married. Educational statuses of participants’ parents were also recorded, and the highest level of education was primary school, for 68.5% of mothers and 63.7% of fathers (Table 1).
Students’ Descriptive Results (N = 292).

SA-SH Reliability-TR
Internal consistency
Table 2 presents analyses of the SA-SH-TR questionnaire. The internal consistency of the SA-SH-TR was calculated according to item-total correlation and Cronbach’s alpha methods for all the items and subitems in the scale. Items 9 to 13 and 16 to 18 were identified as negatively worded questions, and these items’ scores were reversed. The scale’s internal consistency coefficient (Cronbach’s alpha) was high, at 0.899. The scale’s anti-image correlation values ranged from 0.672 to 0.963, and the anti-image correlation value of all the scale’s items was found to exceed 0.500. Item-total correlation values ranged from 0.234 to 0.752. The item-total correlation values for Items 11, 12, 14, 16 to 18, 20, and 22 were low. Moreover, these items’ anti-image correlation values were lower than the other items’. When these items were omitted from the scale, the total internal consistency coefficient (Cronbach’s alpha) increased to 0.916. Considering this finding, Items 11, 12, 14, 16 to 18, 20, and 22 were omitted from the scale (Table 2).
The Analysis of Items in Students’ Attitudes Toward Addressing Sexual Health Questionnaire-Turkish (N = 292).

Subscale points for “present feelings of comfort” ranged from 8 to 40, with a mean of 24.97 ± 7.40 and an internal consistency coefficient of 0.956. Also, subscale points for “future working environments” ranged from 3 to 15, with a mean of 10.51 ± 2.78 and an internal consistency coefficient of 0.654. Furthermore, subscale points for “fear of negative influence on future patients” ranged from 3 to 15, with a mean of 9.13 ± 2.71 and an internal consistency coefficient of 0.677. Finally, the total points for students’ attitudes toward addressing the sexual health questionnaire ranged from 14 to 69, with a mean of 44.62 ± 10.78 and an internal consistency coefficient of 0.916 (Table 3).
Total Points of the Adapted Turkish Students’ Attitudes Toward Addressing Sexual Health Questionnaire and Internal Consistency (N = 292).

A significant positive correlation was found between the questionnaire’s total scores and the subscales for “present feelings of comfort,” “future working environment,” and “fear of a negative influence on future patients” at 50.8%, 47.5 %, and 93.7%, respectively (p = .001; p < .01). A significant positive correlation was also found between the questionnaire’s total scores and the subscales for “future working environment” and “fear of a negative influence on future patients” at 41.8% and 71.2%, respectively (p = .001; p < .01). Finally, a significant positive correlation was also found between the questionnaire’s total scores and the “fear of a negative influence on future patients” at 68.5% (p = .001; p < .01; Table 4).
Correlation of the Adapted Turkish Students’ Attitudes Toward Addressing Sexual Health Questionnaire Subscales and Total Scores (N = 292).

Pearson correlation analysis **p < .01.
Time-dependent invariance
For test–retest reliability, ICC was used. To examine the scale’s time-dependent invariance, the questionnaire was administered to 50 students at 3-week intervals, and the scale’s ICC was calculated. The ICC values for each subscale were as follows: 0.863 (ICC: 0.863, 95% confidence interval [CI]: 0.758–0.922) for “present feelings of comfort”; 0.639 (ICC: 0.639, 95% CI: 0.364–0.795) for “future working environment”; and 0.642 (ICC: 0.642, 95% CI: 0.368–0.797) for “fear of a negative influence on future patients.” The scale’s point total was 0.835 (ICC: 0.835, 95% CI: 0.710–0.907; Table 5).
Test–Retest Correlations of Subscale and Total Scores (N = 292).
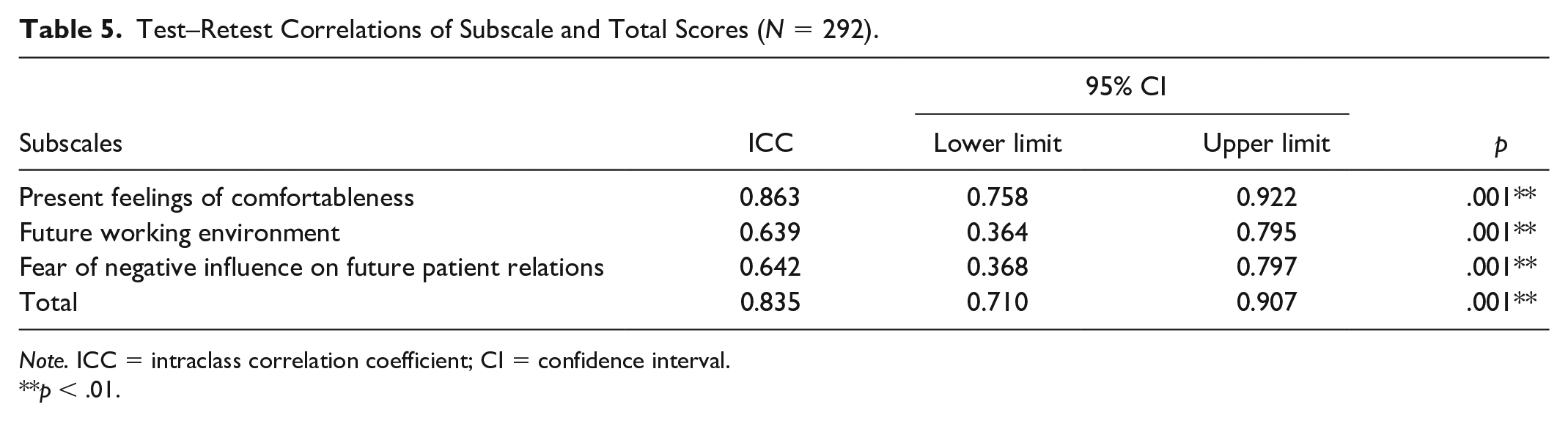
Note. ICC = intraclass correlation coefficient; CI = confidence interval.
p < .01.
SA-SH-TR Validity
To test the scale’s validity, EFA was used, while CFA was used to test the construct validity.
EFA
The scale’s Kaiser–Meyer–Olkin (KMO) sample sufficiency value was 0.931, which is sufficient for EFA. A Bartlett sphericity test verified this result as statistically significant (χ2 = 2.919, 758; df = 91; p = .001). Varimax rotation was used for EFA, and principal component analysis was used for extraction. Based on the factor analysis results, the questionnaire was assessed for three factors. The first factor accounted for 70.396% of the questionnaire’s total variance, two factors accounted for 56.32% of the questionnaire’s total variance, and three factors accounted for 70.396% of the questionnaire’s total variance (Table 6).
Factor Loads, Eigen Values, Exploratory Variance Percantages.
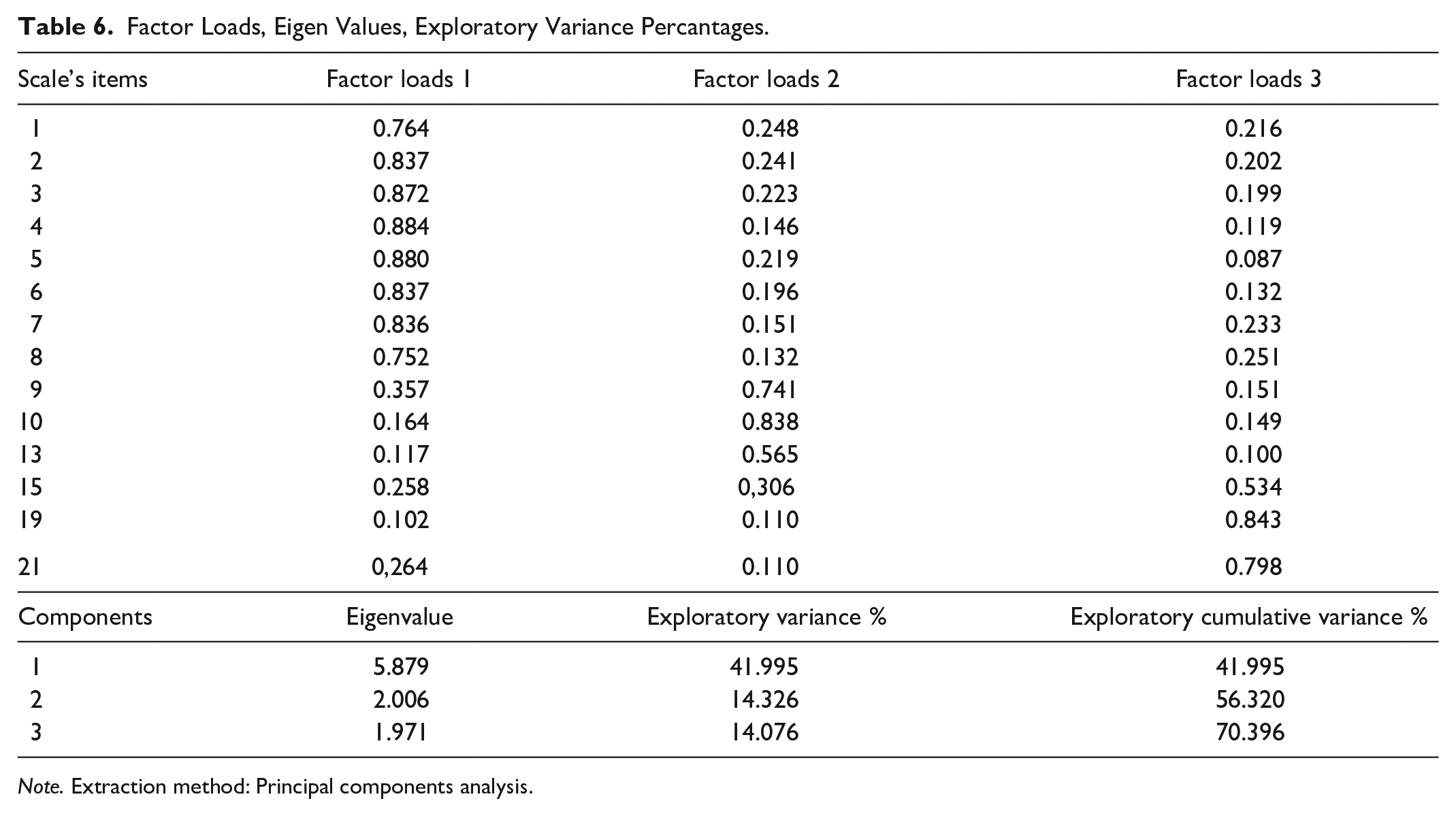
Note. Extraction method: Principal components analysis.
CFA
CFA values are provided in Table 6. The data’s chi-square goodness of fit was χ2(74) = 240.593, while the normalized chi-square (NC) was 3.251, the comparative fit index (CFI) was 0.942, the root mean square error of approximation (RMSEA) was 0.088, the normalized fit index (NFI) was 0.919, and the goodness of fit index (GFI) was 0.883 (Table 7). Based on these index values, the model’s fit was determined to be sufficient (Figure 1).
Evaluation of Goodness of Fit Index and Analysis Values.

Note. GFI = goodness of fit index; CFA = confirmatory factor analysis; NC = normed chi-square; RMSEA = root mean square error of approximation; CFI = comparative fit index; NFI = normed fit index.

Standardized solution of items.
Discussion
This study’s purpose was to translate and adapt the original English version of the SA-SH questionnaire into Turkish and, subsequently, to determine the reliability and validity of the questionnaire’s Turkish version. All of the nursing students in our sample reported that the scale, which comprised 22 items, was easy to understand and applicable.
Assessing testing tools’ internal consistency is a concept based on the understanding that a tool comprises independent units with distinct objectives that, as a whole, have visible and equal weights (Erefe, 2002; Gözüm & Aksayan, 2003). To determine whether a scale is internally consistent, all of its included subscales must test the same feature (Gözüm & Aksayan, 2003). In other words, internal consistency is also referred to as the “homogeneity of the tool” (Özdamar, 2003; Özdemir, 2005). Internal consistency reliability shows stability in tools with good-to-acceptable reliability, according to Cronbach’s alpha.
The present study identified a positive correlation between nursing students’ total SA-SH-TR points and item points. When Items 11, 12, 14, 16 to 18, 20, and 22 were omitted from the scale, the scale’s general internal consistency coefficient (Cronbach’s alpha) improved to 0.916. Areskoug-Josefsson et al. (2016) noted that the original scale’s Cronbach’s alpha value of was 0.71, while the scale items were originally between 0.65 and 0.71. The internal consistency reliability results for the complete questionnaire, measured with Cronbach’s alpha, are similar to the tests performed on the original version of the scale Areskoug-Josefsson et al. (2016) and in the Gerbild et al. (2017) study.
Factor analysis to determine whether other scale items could be analyzed under different subscales presented an additional measure to assess validity. In the present study, factor analysis was used to examine whether the original questionnaire was valid in Turkish culture.
For scale validity, factor item loading was expected at 0.30 or higher. The loading of the scale items was above 0.30. Gerbild et al. (2017) reported a good correlation, in the original SA-SH, between the items in each factor and the factors themselves, demonstrating factor analysis as a useful tool for determining the validity of the SA-SH. Therefore, the fit of our Turkish model was found to be good.
This type of reliability is determined by similar evaluation results when testing is conducted at different times in repeated evaluations (Erefe, 2002; Turan et al., 2017). Therefore, the test–retest method is often used (Gözüm & Aksayan, 2003). In the present study, the test–retest correlation coefficients of the SA-SH-TR demonstrated that the scale’s time-dependent invariance was satisfactory. According to Areskoug-Josefsson et al. (2016), test–retest correlation coefficients for the original scale varied from 0.74 to 0.90. In the present study, these values were significant. In the previous literature, the correlation values’ power was considered as follows: 0.00 to 0.25 is very weak, 0.26 to 0.49 is weak, 0.50 to 0.69 is mediocre, 0.70 to 0.89 is strong, and 0.90 to 1.00 is very strong (Akgül & Çevik, 2005; Kaya & Aştı, 2008). Therefore, for the items in the Turkish SA-SH, the item totals and subscale totals can be assumed not to have changed over time. Furthermore, the examination of the Turkish adaptation’s validity and reliability in terms of invariance according to time significantly contributes to the literature. Because the adapted scale was applied to a different society than the original scale, the adaptation increased the scale’s reliability and demonstrated its usage prevalence. The reliability of any scales tested in other cultures is, thus, expected to be high.
Validity is the second crucial component that helps assess whether a data collection tool is comprehensive or reflective of its measured theory, concept, or variables (Kaya & Aştı, 2008; Kaya & Turan, 2011; Turan et al., 2017). CFA, which is a criterion for validity, enables an assessment of whether scale items can be measured under different subscales. In the present study, CFA was used to examine whether the original questionnaire was valid in Turkish culture. This type of factor analysis expects item factor loadings to equal or exceed 0.30 (Özdamar, 2003; Özdemir, 2005). Fit indexes were investigated, and the model’s fit was found to be good. A study on the original scale stated that the model lacked a good fit, and consequently, modifications were implemented (Gerbild et al., 2017). These modifications led to the formation of a new model (Areskoug-Josefsson et al., 2016).
Construct validity shows a scale’s ability to test its related concept or entire conceptual structure. The simplest definition of construct validity is when test or scale items significantly relate to hypothetical factors and correlations among the factors suiting an applied theory (Gözüm & Aksayan, 2003). In the present study, a KMO test was used to determine the data’s applicability for factor analysis. A Bartlett sphericity test was administered to determine whether the correlations among the variables were significant for analysis. The KMO value indicated that the sample size was sufficient for factor analysis. Chi-square values were highly significant, indicating significant correlations between the variables. Therefore, the data were determined to be sufficient for factor analysis. In the previous literature, KMO values between 0.90 and 1.00 are considered excellent, and a Bartlett sphericity test value below 0.05 is considered significant (Akgül & Çevik, 2005; Karaahmetoğlu & Alpar, 2017). Therefore, based on KMO test values, the data applicability of the adapted Turkish SA-SH is excellent.
The present study’s Turkish SA-SH questionnaire was developed for use in planning and assessing nursing educational interventions in the field of sexual health. It will be useful for other health care professionals as well because of the lack of reliable questionnaires within the field of sexual health (Bal & Sahiner, 2015). The questionnaire may also be used to investigate attitudes toward sexual health among students in other health care professions.
Conclusion
The present study provides a basis for evaluating nursing students’ attitudes toward sexuality during their education. The adapted Turkish 22-item SA-SH-TR scale is a valid and reliable tool to measure nursing students’ attitudes about sexual health in Turkish society. This scale can be used as an objective tool to measure educational programs’ impact on attitudes and communication concerning sexual health among student nurses studying in various curriculum programs.
This scale also provides a basis for researchers and educators to develop educational methods that can improve students’ attitudes toward sexuality in nursing education. Moreover, it will allow for an assessment of nursing students and other university students’ attitudes. Therefore, the scale may be used to develop education programs that will positively affect sexual health attitudes.
Limitation
This study was conducted to introduce the SA-SH-TR scale for use in Turkey. Its limitation is that the adapted questionnaire was administered to a wider population, representing all nursing students. Therefore, the relationship between sexual attitudes and sociodemographic variables could not be determined.
Footnotes
Acknowledgements
We thank all the nursing students who participated in this research.
Authors’ Note
The research discussed in this article was originally presented at the 6th International Conference on Advance Nursing Practice, June 21–22, 2018, in Paris, France, an abstract of which was published in the Journal of Nursing and Health Studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.