
Abstract
Paranoid thought is one of the most common symptoms in psychiatric disorders. The Paranoia Checklist is a brief screening and diagnostic tool for clinical and subclinical paranoia. It has been used in research, clinical, and non-clinical settings. The Paranoia Checklist has not had its validity examined in university settings in Iran. A cross-sectional study was conducted to investigate the validation of the Farsi version of Paranoia Checklist in a randomized cluster sample of 365 Iranian volunteer college students selected from the Payame Noor University of Mashhad in Iran. They completed the Paranoia Checklist, the General Paranoia Scale, and the Symptom Checklist 90 Revised (SCL-90-R). The mean score of the Paranoia Checklist was 35.50 (SD = 7.21). The Cronbach’s α for the Paranoia Checklist was .87, indicating high internal consistency. The Paranoia Checklist correlated .42 with the General Paranoia Scale, .38 with the SCL-90-R subscales of Anxiety (ANX), Hostility (HOS), and Paranoia Ideation (PAR), and .37 with the Interpersonal Sensitivity (INTS), denoting moderate construct and criterion-related validity. The results of the factor analysis of the Paranoia Checklist identified three factors associated with the paranoid thoughts. The Paranoia Checklist has a multidimensional structure, and adequate validity and reliability. It can be used in the non-clinical, clinical, and research settings to measure paranoia in Iran.
Introduction
Paranoia is a continuum of clinical and subclinical experiences, and is one of the main symptoms of psychosis. Paranoid thoughts, as one of the personality characteristics, can have a significant impact on the mental and physical health. Paranoid thoughts cause severe psychological stress that can cause mental disorders. There are paranoid thoughts in the most of mental disorders such as obsessive compulsive, depression, schizophrenia, and mania disorder (Brown, 2010; Freeman, 2007; Freeman & Garety, 2004; Freeman, Garety, Bebbington, Slater, et al., 2005; Freeman et al., 2004; Freeman, Garety, Kuipers, Fowler, & Bebbington, 2002; Freeman et al., 2003). There are some risk factors for paranoid symptoms (Hartmann, Sundag, & Lincoln, 2014). Paranoid thoughts can be reduced through targeting negative emotions and self-esteem (Lincoln, Hohenhaus, & Hartmann, 2013). State anxiety increases paranoid ideation (Lincoln, Lange, Burau, Exner, & Moritz, 2010).
There are relationships between paranoia and positive schizotypy; between paranoia, negative affect, self-consciousness, and negative social perceptions in daily life (Brown, 2010); and also between paranoid symptoms, social phobia, and social anxiety cognitions (Linscott & van, 2013; Schutters et al., 2012). Brown, Barrantes-Vidal, Silvia, and Kwapil (2014) indicated that paranoia strongly correlated with positive schizotypy, moderately correlated with social anxiety, and weakly correlated with negative schizotypy. On the Green et al. Paranoid Thought Scales (GPTS), Ghadiri Sourman, Abdolmohammadi, Babapour Kheyradi, and Asl Rahimi (2016) showed a significant positive relationship between paranoid thoughts and somatization disorder in Iranian college students. Hosaini and Ariapooran (2012) found that a significant correlation between Cluster A personality disorders include paranoid personality disorder and suicidal ideation; and also between Cluster A, positive and negative emotion among Iranian college students. One of the newest systematic review study in Iran reported that having psychiatric disorders such as depression and paranoia can lead to suicidal thoughts and attempts in Iranian college students (Bakhtar & Rezaeian, 2017).
There are paranoia thoughts in the normal population (Barreto Carvalho et al., 2018; Barreto Carvalho et al., 2017; Yamauchi, Sudo, & Tanno, 2009b). Subclinical paranoia is estimated to occur in around 10% of the general population (Brown, 2010). Studies have reported that between 10% and 15% of the normal people experience paranoia thoughts (Freeman, 2006; Freeman, 2016; Freeman, Gittins, et al., 2008; Freeman, Pugh, et al., 2008; Freeman et al., 2007). Paranoid disorder is a cultural and dimensional phenomenon (Abdolmohammadi, Mohammadzadeh, Ahmadi, & Ghadiri Sourman, 2016; Ibáñez-Casas et al., 2015). Some studies have reported the prevalence of paranoid thoughts in Iranian clinical and non-clinical samples. For example, on the SCL-90 R, Ghobari Banab and Hadadi Kohsar (2010) found that paranoid thoughts were lower in Iranian females than in males students; Atef Vahid, Bolhari, Ehsanmanesh, and Karimi (2011) reported that Paranoia subscale had higher score than other subscales in general population; Habibzadeh (2014) showed that prevalence of paranoid thoughts was 46.11% among Iranian high school female students; Heidari Pahlavian, Mahjub, and Rahimi (2011) found that Iranian drug dependency obtained higher scores in Depression, Paranoid Thoughts, and Interpersonal Sensitivity subscales than non-drug dependent persons; and Fakour et al. (2016) reported that the paranoia symptoms were the most prevalent disorders in patients with pemphigus (45% in female and 60% in male). On the Millon Clinical Multiaxial Inventory III (MCMI-III), Dadfar and Lester (2017) reported that one of the most common of severe syndromes was Thought Disorder (SS) (1.8%) in Iranian psychiatric outpatients, and the women patients had higher scores than men (t = 4.71, p > .000).
There are different questionnaires for investigating the paranoid thoughts, for example, the General Paranoia Scale (Fenigstein & Vanable, 1992), the Paranoia Checklist (Freeman, Garety, Bebbington, Smith, et al., 2005), and the GPTS (Green et al., 2008). The Paranoia Checklist is a self-report test and provides a multidimensional assessment of paranoid ideation. The Paranoia Checklist assesses the frequencies, conviction, and distress associated with the paranoid/suspicious thoughts of a clinical nature (Freeman, Garety, Bebbington, Smith, et al., 2005). The items assess ideas of persecution and reference. There are different versions of the state Paranoia Checklist: the three-, five-, and 13-items versions (Schlier, Moritz, & Lincoln, 2016). The Paranoia Checklist was translated to German (Lincoln, Peter, Schafer, & Moritz, 2010; Lincoln, Ziegler, Lüllmann, Müller, & Rief, 2010) and Japanese (Yamauchi, Sudo, & Tanno, 2007, 2009a) languages.
There are some psychological approaches for paranoid and suspicious thoughts (Freeman & Garety, 2006). Lincoln, Peter, et al. (2010) suggested a combined meta-cognitive training directed at reasoning biases and promoting emotion regulation skills. The study of Amirpour, Tabatabaee, Modares-Gharavi, and Hasanabadi (2010) showed that cognitive behavioral therapy reduced paranoid ideations, persecutory delusions, and anxiety associated with them in Iranian paranoid schizophrenic patients. Due to lack of reliable and valid measures, appropriate efforts to diagnosis and treatment of paranoia disorder have not been done in Iran. The Paranoia Checklist has not been translated for use in Iran. This is an important study which validates a scale for paranoid thoughts in Iran. The present article examines the psychometric and screening properties for paranoia thoughts of the Paranoia Checklist in a sample of Iranian college students.
Method
Among a population of 17,871 people, a randomized cluster sample of 365 Iranian volunteer college students was selected from the Payame Noor University of Mashhad in Iran. The students provided written consent. The study protocol was approved by an institutional review board. They completed the Farsi versions of the Paranoia Checklist, the General Paranoia Scale, and the Symptom Checklist 90 Revised (SCL-90-R). For matching the Paranoia Checklist items in two original and Farsi versions, there were no any necessary modifications of the Paranoia Checklist needed as per the cultural context in Iran.
Measures
Paranoia Checklist
The Paranoia Checklist was developed by Freeman, Garety, Bebbington, Smith, et al. (2005) in England. It has 18 items, each rated rarely, once a month, once a week, several times a week, and once a day on a 5-point scale (1-5), with a score ranging from 18 to 90, for frequency, degree of conviction, and distress. The higher scores show greater frequency of paranoid ideation, stronger conviction, and greater associated distress. The Cronbach’s α for each of the three dimensions of the Paranoia Checklist was reported .90 or above. It has shown a low positive correlation with a total score for frequency, conviction, and distress The General Paranoia Scale correlated .71 with the Paranoia Checklist frequency, .62 with the conviction, and .58 with the distress scores (Freeman, Garety, Bebbington, Smith, et al., 2005). The Cronbach’s α for the German Paranoia Checklist version was .90 or above for some items (Lincoln, Ziegler et al., 2010) and .96 for three-dimension Portuguese Paranoia Checklist version (Barreto Carvalho et al., 2018). A typical item is “I need to be on my guard against others.”
General Paranoia Scale
The General Paranoia Scale was developed by Fenigstein and Vanable (1992) to measure paranoia in college students. It is used for dimensional measure of paranoia. The scale has some items that are not clearly persecutory, and also does not assess the frequencies, conviction, and distress associated with the paranoid thoughts. It has 20 items, each rated (1) not at all applicable and (5) extremely applicable on a 5-point scale. Scores can range from 20 to 100, with the higher scores indicating greater paranoid ideation (Freeman, Garety, Bebbington, Smith, et al., 2005). The study of Fenigstein and Vanable (1992) showed one-dimensional model, and Barreto Carvalho et al. (2014, 2017) found three dimensions of mistrust thoughts, persecutory ideas, and self-deprecation for the scale. A typical item is “I am sure I have been talked about behind my back.”
SCL-90-R
The initial frame of Symptom Checklist 90 (SCL-90) was designed by Derogatis, Lipman, and Covi (1973) to assess various psychological aspects of physical and mental illnesses. The SCL-90-R was developed in 1984 (Derogatis, 1992). The SCL-90-R has 90 items and nine subscales including Somatization (SOM; 12 items), Obsessive-Compulsive (O-C; 10 items), Interpersonal Sensitivity (INTS; nine items), Depression (DEP; nine items), Anxiety (ANX; 10 items), Hostility (HOS; six items), Phobic Anxiety (PHOB; seven items), Paranoid Ideation (PAR; six items), and Psychoticism (PSY; 10 items), and additional items such as the Global Severity Index (GSI), the Positive Symptoms Distress Index (PSDI), and the Positive Symptoms Total (PST). The each item of SCL-90-R rated (0) not at all, (1) little, (2) some, (3) very, and (4) severe on a 4-point scale. The GSI of the SCL-90-R is calculated by dividing the total score on the derived 90 items, and ranged from 0 to 4. The higher scores than 2 indicate psychopathology (Sereda & Dembitskyi, 2016). The SCL-90-R has been validated in Iran (Anisi, Akbari, Majdian, Atashkar, & Ghorbani, 2011; Ardakani et al., 2016). The Cronbach’s α was from .70 to .97, and test–retest reliability was from .78 to .90 (Zakiei, Rajabi Gilan, Reshadat, & Ghasemi, 2015). Fasahati and Kalantarkousheh (2014) found Cronbach’s α .80 for PAR subscale. A typical item is “The idea that someone else can control my thoughts.”
Results
The mean age of the students was 28.50 years (SD = 6.33); 68.3% were female; 34.6% were single; 65.4% were married; and the majority 76.6% had completed BA, and 23.4% had a MSc degree. The mean score on the Paranoia Checklist was 35.50 (SD = 7.21). The lowest mean score was 1.28 (SD = 0.78) for Item 16, and the highest mean score was 3.93 (SD = 2.08) for Item 1 (see Table 1).
Mean and Standard Deviation of the Paranoia Checklist Items and Total Score.

Note. The minimum and maximum values were all from 1 to 5.
Reliability of the Paranoia Checklist
The Cronbach’s α coefficient for the Paranoia Checklist was .87, indicating high internal consistency (see Table 2). The Paranoia Checklist Cronbach’s α coefficients after item deleted were from .86 to .89.
Descriptives of All Questionnaires.
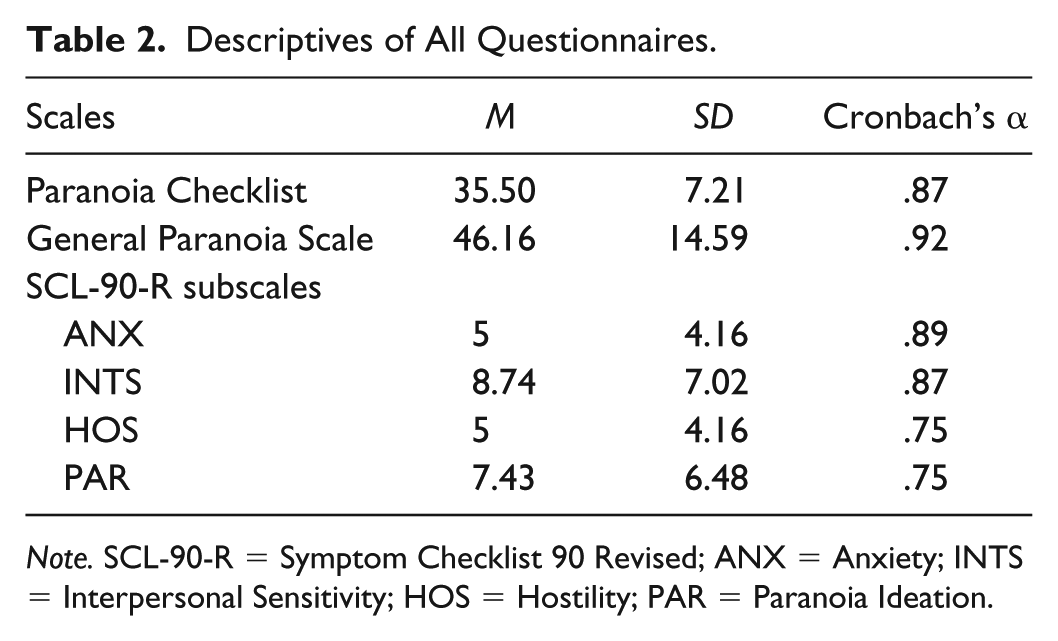
Note. SCL-90-R = Symptom Checklist 90 Revised; ANX = Anxiety; INTS = Interpersonal Sensitivity; HOS = Hostility; PAR = Paranoia Ideation.
Correlations of the Paranoia Checklist With Other Scales
The Paranoia Checklist score correlated .42 with the General Paranoia Scale, .38 with the SCL-90-R subscales of ANX, HOS, and PAR, and .37 with the INTS, indicating moderate concurrent validity (see Table 3).
Pearson’s Correlations (r) Between the Scales.

Note. SCL-90-R = Symptom Checklist 90 Revised; ANX = Anxiety; INTS = Interpersonal Sensitivity; HOS = Hostility; PAR = Paranoia Ideation.
Correlation is significant at the .01 level (two-tailed).
Factor Analysis of the Paranoia Checklist
The criteria for the factor analysis were evaluated using the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy and the Bartlett Test of Sphericity. The KMO was 0.919, indicating the adequacy of the sample of university students, and the Bartlett’s Test of Sphericity was 2273.615 (df = 153, p < .001) indicating that the factor analysis was justified. The exploratory factor analysis (EFA) was used to check the latent structure.
The results of the factor analysis of the Paranoia Checklist identified three factors (40.22% of total variance). Factor 1 (Items 3, 5, 8, 10, 11, 12, 13, 14, and 16) explained 33.71% of the variance and was labeled Frequency. Factor 2 (Items 5, 6, 8, 9, and 16) explained 3.70% of the variance and was labeled Conviction. Factor 3 (Items 1, 2, 3, 4, and 5) explained 2.79% of the variance and was labeled Distress (see Table 4). Item 3 loaded on Factors 1 and 3; Item 5 loaded on three factors; Items 8 and 16 loaded on Factors 1 and 2.
Factor Loadings (>0.5) of the Farsi Version of the Paranoia Checklist With Iranian Students (N = 365).

Note. Factor 1 (Items 3, 5, 8, 10, 11, 12, 13, 14, and 16): Frequency. Factor 2 (Items 5, 6, 8, 9, and 16): Conviction. Factor 3 (Items 1, 2, 3, 4, and 5): Distress.
Conclusion
The aim of the study was to examine the psychometric and screening properties for paranoia with the Paranoia Checklist in a sample of Iranian college students. On the Paranoia Checklist, 37% of the sample showed frequency, degree of conviction, and distress paranoid thoughts (M = 35.50, SD = 7.21). The Cronbach’s α for the Paranoia Checklist was .87, indicating good reliability, consistent with research in other countries (e.g., Brown, 2010; Barreto Carvalho et al., 2018; Freeman, Garety, Bebbington, Smith, et al., 2005; Hirao, 2016; Yamauchi et al., 2007, 2009a; Yamauchi, Sudo, & Tanno, 2009c; Lincoln, Ziegler, et al., 2010).
In the present sample, the Paranoia Checklist score correlated with the General Paranoia Scale and the SCL-90-R subscales of ANX, INTS, HOS, and PAR scores, all statistically significant, indicating good construct validity. The results are consistent with other studies, for example, Yamauchi et al. (2007) indicated that the Japanese-version Paranoia Checklist (JPC) scores positively correlated with the Paranoia Scale and the Peters et al. Delusions Inventory (PDI). In two studies, Yamauchi et al. (2009a) found that the Paranoia Checklist correlated with the Spielberger Trait Anger Expression Inventory in undergraduate students, and Yamauchi et al. (2009c) showed that the JPC positively correlated with trait anxiety, social anxiety, and anger, and negatively correlated with social support. Lincoln, Ziegler, et al. (2010) reported that the Paranoia Checklist correlated .52 with the Positive and Negative Syndrome Scale (PNSS). Hirao (2016) found that the JPC Distress subscale correlated with the Flow Experience Checklist (FEC). On the modified version of the Paranoia Checklist, Lamster, Nittel, Rief, Mehl, and Lincoln (2017) found that loneliness correlated with paranoid beliefs in a non-clinical sample.
Three factors labeled were identified, indicating good homogeneity in the items. Our findings were consistent with results of Brown, 2010; Freeman, Garety, Bebbington, Smith, et al., 2005; Lincoln, Mehl, et al., 2010; and Barreto Carvalho et al., 2018. But Yamauchi et al. (2007) identified one-factor structure for the JPC. Moritz, Van Quaquebeke, and Lincoln (2012) yielded two factors (explained 64% of the total variance) labeled as “Unspecific Suspiciousness” (37% of the variance) and “Psychotic Paranoia” (27% of the variance) for the German version Paranoia Checklist in the general population. These results are not consistent with our findings. They used the varimax rotation with factor loadings above 0.6 in their study (Oblimin rotation with factor loadings above 0.5 in our study) that can justify this inconsistency.
The study has some limitations. There were only some demographic data of the participants such as age, sex, marital status, and educational level, but there were no data about their medical and psychiatric history. From obtained mean and standard deviation in the sample, it is hard to state that none of participants had psychiatric illness. The General Paranoia Scale has not been validated in Iranian population. An epidemiologically representative sample and a clinical sample were not selected. The group included college students who may have higher rates of suspiciousness. Examination of cross-sectional correlations between paranoia, coping strategies, and social cognitive processes is recommended.
We conclude that the Farsi Paranoia Checklist has a multidimensional structure, has good validity and reliability, and may be useful for non-clinical, clinical, and research settings to measure paranoia in Iran.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.