
Abstract
Technology use for personal health management should not only be assessed in terms of the rate of adoption but also examined in the form of sustained use to ensure the long-term benefit. This study addressed the issue of the continued use of wearable devices by ensuring value co-creation among a user, the wearable device, and other users within a service system. This study was a scenario-based experiment to examine interaction design, including interactivity level and game dynamics, which act as a combination of value co-creation mechanisms to elicit a user’s intentions to continuously use wearables. The study also examined user perception factors, such as self and social perceptions, as moderators. This study contributes to existing literature by using the value co-creation and service system perspective to examine continued use behavior. The findings of the research also offer practical insights into designing the features of wearable fitness trackers to promote long-term value for their users.
Keywords
Introduction
Technological advances and service delivery are considered potential topics for future service research in healthcare (Danaher & Gallan, 2016). Leveraging technology to enhance service using wearable devices has been gaining significant academic attention, particularly in healthcare service. It has been a kind of anomaly that people massively adopt and use wearable fitness trackers but abandon them within several months. Recently, designers have attempted to introduce new features, such as dozens of exercise modes, glucometers, and spirometers to retain their users. However, this long list of features represents a shift to technical abundance and short-term marketing gimmick rather than well-executed value propositions (Canhoto, 2017). Therefore, continued use is a key concern in ensuring the long-term value of service by compelling value propositions.
With technological advances, value co-creation becomes more relevant in observing resource exchange processes enabled by the device (Lee, 2019). Value co-creation has emerged as a promising perspective to examine the dynamics of healthcare services (Hau et al., 2017; Nguyen Hau & Thuy, 2016) due to the nature of the involvement of actors in health service systems. For example, patients who are search for information online, engage with community support groups, and actively participate in a treatment plan designed by the doctors, are proven to generate more positive outcomes (Walker et al., 2017). Another example is the use of games to increase engagement and promote socialization. However, it seems unclear of the specific mechanics that directly impact the continued fitness wearable use intentions.
This study took an alternative approach to investigate users’ continued use intentions from the service system view. Studies on continued use intentions of technology have mainly examined users’ acceptance and experience, focusing only on individuals’ perceptions (Beldad & Hegner, 2018; Cho, 2016; Dhir et al., 2020). Different from the long-established view of continued use intention as an individual post-adoption behavior (Dhir et al., 2020; Talwar et al., 2020), by taking the service system perspective, this research emphasizes the importance of promoting value co-creation mechanisms and self and social perceptions. Furthermore, research on health IT adoptions urges the focus to meet sociotechnical complexity rather than focusing on individual acceptance (Shachak et al., 2019).
This research used the sociotechnical system design to operationalize value co-creation mechanisms. Sociotechnical system design considers human, social, and technical factors (Baxter & Sommerville, 2011), which become the pillars of a service system (Barile & Polese, 2010). In the experiments, the study translated this concept as to how a user, with his/her self and social perception (human factors), interacts with other users (social factors) to engage with game dynamics or add-on services from third parties offered by the device (technical factors).
This research explored the features and mechanisms that can challenge both individual and social factors; the features offered by the device act as value propositions. Wearable devices enable their users to integrate resources with the service provider (user-device interactions), as well as with other customers during service encounters (user-user interactions) (Windasari et al., 2021). Therefore, this study chose factors enabling these interactions.
To enable user-device interaction, an interactive system is required. As a service system, fitness wearables work with sensors, cloud services, third-party apps, and a user’s mobile device to record and process information obtained from a user’s biometric data. Interactivity enables the interactive information flow between a user and the device to simultaneously enhance the value provided to the user. While to enable user-user interactions, there need to be gamification mechanisms. Game dynamics enable a user to interact with other users in their social networks to gain mutual reinforcement. The wearable producer and a user may coproduce value during the use of wearable. Moreover, the influence of the user’s health extends beyond the firm-user relationship that involves cognitive and emotional resources to include resources from friends, family, and other actors (McColl-Kennedy et al., 2012). For example, a user may obtain additional motivation through collective actions and peer encouragement.
Further, from a system view, an actor’s behavior will systematically affect other actors. This research also proposes two moderators, namely self and social perception, showing that the value perceived from the device does not exist in isolation. The value proposed by the device is not only an information but also follow-up effects on how a user perceives and then his/her intention for prolonged use. A user is an actor whose cognition process is influenced by the link between his/her self and social perceptions (Lieberman & Pfeifer, 2005), moving beyond persuasive design. This research also aims to determine under which circumstances an individual’s self and social perceptions might strengthen his/her intentions to continue using a wearable fitness tracker over time.
Literature Review and Hypothesis Development
Continued use intentions can be defined as a user’s intention to continue using a system or repeated performance of an activity. For personal health management, long-term use is much more valuable and has a greater impact on individuals’ health outcomes. The success of wearable technologies should rely on users’ continued usage, rather than an initial status, such as adoption and acceptance (Ledger & McCaffrey, 2014).
This study uses the alternative perspective based on service-dominant logic (S-DL) to explain the continued use intentions of a health device. In most information technology research, continued use is perceived as a result of user satisfaction (Storbacka et al., 2016). Meanwhile, the nature of health services always involves a set of interactions between individuals (i.e., patients, healthcare providers, physicians, etc.), practices, and recently, with technology (Kumar et al., 2020). S-DL accommodates this trend adequately because it requires the service system view to see the dynamic configuration of resources, including individuals, information, and technology, connected by value propositions (Vargo et al., 2008). This perspective fits with how fitness wearables work by connecting users with other actors as value propositions that affect users’ continuance intention (Windasari et al., 2021).
This study examined the literature on the sustained use of consumer health information technology (HIT), specifically wearables and mobile health applications, in the recent 5 years (2016–2021) to seek new factors contributing to prolonged use. The search criteria focused more on the factors that were considered part of the integrative value of wearables within a service system rather than specific demographic or device quality factors. A number of studies were found that examined sustained use of wearable devices, as listed in Table 1.
Prior Studies on Sustained Use of Wearable and Fitness Apps (2016–2021).

In this literature review, a limited number of studies took an integrative view that regards a wearable device as an inseparable part of a service system. There is a growing demand on investigating continued use of wearables from partial into integrative view of technical and behavioral factors (Asimakopoulos et al., 2017; Hassan et al., 2019; Huang & Ren, 2020). However, how the integrative view was operationalized was less explained, not to mention how the technical and behavioral factors enable value co-creation.
Value co-creation is defined as resource integration and service exchange (Vargo & Lusch, 2017). The degree of engagement through human-to-human interactions can promote value co-creation. Furthermore, value co-creation can also occur between user and technical device interactions that engender positive users’ experiences (Lee, 2019).
In this study, we fill the gap by operationalizing sociotechnical system design that incorporates both technical and behavioral factors into value co-creation mechanisms. In this study, we explore two antecedents of wearables’ interaction features, interactivity, and gamification, as the proxy of value co-creation mechanisms, which might affect users’ behaviors. The interaction design of a wearable device with features to motivate users’ health behaviors will improve the value co-creation between its users’ and the device; for example, to suggest the next exercise plan when a user reviews his/her daily performance information, or to allow a user to get motivated from his/her peers and social networks. In health promotion, goal reinforcement via gaming rules can make users feel interested in using wearable devices, which may lead to sustained engagement (Ledger & McCaffrey, 2014).
Besides considering wearable’s, we also examined self and social perceptions as two moderators that affect the continued use of wearable devices for personal healthcare management. The research model is drawn as shown in Figure 1. Those proposed factors and hypotheses are described in the following subsections.

Research model.
Interactivity
In the context of using a wearable device, a user is mainly concerned with information feedback via the interface between him/herself and the wearable device with associated applications. Interactivity is found to play an important role in building a positive relationship between the device and its users, which can make a device with a higher interactivity level more attractive to users (Sutcliffe & Hart, 2017). In the context of personal health record services, interaction plays a significant role in influencing adoption-related behaviors (Hietala et al., 2009).
Interactivity, in this scenario, is operationalized as the integration of back- and front-end data. Data integration is the process in which data obtained from the device and its user (front-end) are used for connecting the service from third parties such as health experts and health insurance providers (back-end) via the user interface.
A wearable device collects information about a user’s activities and movements. Based on the collected information, the feedback should be meaningful and valuable for users. Rather than presenting raw information collected from a sensors, the wearable device, together with the back-end system, may provide a summary of the collected information. Furthermore, this system can also provide suggestions to enhance user activity aligned with the pre-determined goals during the use of wearable devices. For example, based on the collected information, the wearable device should be intelligent enough to detect irregularities in a user’s bodily functions and suggest appropriate actions for users to control them. In this regard, the back-end systems of wearable devices may enhance the overall function of wearable devices in a way that will ultimately influence users’ intention to continuously use them.
This study designated two levels of interactivity, namely high and low. A high-interactivity wearable device presents information by integrating front-end user biometric data and back-end data from other sources of information, such as anonymous users’ data and personalized healthcare service provisions. A low-interactivity device only shows the data collected from the user of the device. Different levels of information provision through the wearable imply different values proposed to the user. This study proposes that a fitness wearable providing more integrated information creates different degrees of durability for a user to continuously wear it. Therefore, hypothesis H1 is as follows:
H1. Higher interactivity provided by a wearable will lead to higher continued use intention.
Gamification
Gamification has attracted the attention of academics, practitioners, and business professionals in diverse domains, including health. Though the term has been employed in diverse ways bearing a lack of adherence to the emerging standard definition, it is largely suggested as an approach to design instead of describing a gamified system (Seaborn & Fels, 2015).
Gamification is the use of game design elements in non-game contexts to influence user behavior (Petkov et al., 2011); it is a process of enhancing a service with motivational affordances as gaming experiences to support a user’s overall value creation. In the context of the applicability of gaming elements, challenge, clarity in the goal, curiosity, and interactive feedback may lead to the generation of engagement and enjoyment (Malone, 1982). Similar to interactivity, gamification has also been found to impact user engagement (Flatla et al., 2011). Game mechanics help stimulate users’ willingness to continue using gamified applications or serious games (Sardi et al., 2017). This conceptualization is rooted in S-DL, which suggests that a customer acts as a value co-creator and determiner simultaneously. Therefore, when a customer is engaged in gaming experiences, s/he will subsequently enhance the perceived value of the service (Hamari, 2013; Huotari & Hamari, 2012).
A wearable health device incorporating gamification offers rewards to its users when they achieve specified goals regarding health behaviors. In the context of wearable devices for healthcare, an individual’s extrinsic motivation to perform health promotion activities may be boosted and reinforced through goal setting and an achievement process. Effective gamification design should initially understand the game personalities of learners, social engagement styles, and intrinsically and extrinsically motivated user styles to then evaluate and select appropriate game mechanics and dynamics to create ideal gamification (Tu et al., 2015).
Blohm and Leimeister (2013) developed a framework composed of game-design elements, namely game mechanics and dynamics, and related them to specific motives. Game mechanics cover diverse building blocks for gamifying a core offer, such as scoring systems or badges. This research controls the game mechanics as the default of each scenario by providing challenges and goals in all manipulated scenarios, as shown on the visual interface. Game dynamics, however, describe the effects of specific mechanics overtime on its user experience corresponding to a user’s motives (Huotari & Hamari, 2012). To operationalize the gamification mechanism, this study used three different types of game dynamics, namely self-goal attainment, peer competition, and peer collaboration, to stimulate assigned subjects to experience different treatments of the value-creation process of individual users, user-to-user, or user-to-many users encountered in the experiment.
Goals in health promotion activities may be designed for the user to compete with the prior self or with peer groups. This system was pursued (Liu et al., 2013) by designing a game dynamic that used social interdependence theory as a framework to classify games into individualistic (individual actions have no effects on others), competitive (individual actions obstruct the actions of others), and collaborative (individual actions promote the goals coherent with others).
Self-goal achievement is placed in an autonomous cluster in which the user is in a low degree of relatedness and competence (Liu et al., 2013). Therefore, a user does not depend on the actions of others. However, due to group dynamics created in peer settings, a user may pay greater attention to the fluctuation of group records to react to the updated status in the other two settings of competition and collaboration. Therefore, a higher extent of game dynamics in gamification may create a higher degree of permeability when using wearable devices:
H2. A higher extent of game dynamics in the gamification of a wearable device leads to higher continued use intentions.
The Effect of Self-Perception
Self-perception theory explains how a person determines his/her attitude and preferences by observing his/her behavior (Bem, 1972). This study proposes two factors underlying self-perception, namely perceived self-health risk and health self-efficacy (HSE). Self-perception of one’s own health reflects a capability to act in a definite social and organizational situation, which is regarded as a prognostic indicator of the prevalence of various chronic diseases. A person with low self-perceived health may use medical services more frequently.
In alignment with self-perception theory, the Health Belief Model (HBM) proposes that a person’s health-related behavior depends on the person’s perception. The prominent health behavior theories are HBM and self-efficacy. The expanded HBM, which incorporates self-efficacy, was expected to provide more explanatory power in health-related behavior (Rosenstock et al., 1988). According to the HBM, a person is most likely to practice healthy behavior when s/he perceives that the consequence of having a disease is severe (Maddux & Rogers, 1983). With additional self-efficacy, it is rational to incorporate the need to feel competent before achieving long-term progress (Champion & Skinner, 2008). Therefore, self-perception is included in the model with health risk perceptions and health self-efficacy as two variables.
Risk perception (i.e., beliefs about potential harm) is the construct of most theories regarding health behavior. Stigma represents an increasingly significant factor affecting the individual perception of health, influencing the acceptance of smart wearable health (Li et al., 2019). The wellness of a person may contribute to predicting user behavior in the context of wearable devices. The generated value and utility perceived by healthy users might be different from those facing health issues. Healthy users may initially adopt wearable devices for social status, whereas a person obtaining monitored bio-data provided by a wearable device may be motivated to maintain his/her health (Salah et al., 2014). However, healthy users may not sustain the use of wearable devices because the benefit that they perceive is lower than expected and diminishes over time.
In contrast, wearable devices may be optimum tools that help users with health concerns to more effectively manage their health in a paperless format on a day-to-day basis (Salah et al., 2014). For example, chronic diseases require proper care and treatment from users themselves and family members. Therefore, the efficient design and implementation of wearable devices (e.g., frequent feedback, goal reinforcement, relevant suggestions, etc.) that are capable of providing good health management may generate value for users suffering from chronic disease. This system can influence users to continue using wearable devices. Thus, hypothesis H3a is as follows:
H3a. The effect of interactivity on users’ intention of continuously using wearables is moderated by users’ health risk perception. That is, high interactivity of wearables will enhance users’ continued use intention when their health risk perception is high.
Studies on the adoption of health practices have measured self-efficacy in assessing its potential influence on initiating and more substantial long-term behavioral change (Rosenstock et al., 1988). A rule of thumb is to use the following semantic structure: “I am certain that I can do xx, even if yy (barrier)” (Luszczynska & Schwarzer, 2005). Self-efficacy operates independently of contextual factors (Stretcher et al., 1986). Whereas general self-efficacy measures refer to an ability to deal with stressful situations, this research measures health self-efficacy as a belief of a person’s own ability to perform specific health behaviors.
Providing feedback has a positive effect on enhancing user self-awareness and a sense of self-efficacy. Interactivity features may be a trigger for users to increase concerns about their own health based on the feedback generated by the device. Once a user is aware of his/her own health condition and feels competent to perform healthier behavior, s/he may be motivated to manage personal health, including his/her high intention to continue using fitness wearables. Thus, hypotheses H3b is as follows:
H3b. The effect of interactivity on users’ intention of continuously using wearables is moderated by their health self-efficacy. That is, high interactivity of wearables will enhance users’ continued use intention when their health self-efficacy is high.
The Effect of Social Perception
Social perception has been explained by social psychologists (Ferguson & Bargh, 2004) as having determined how human behavior can be unknowingly influenced. This variable explains how users that adopt wearable devices perceive themselves in relation to others. Incidental social perception also activates goal knowledge that may automatically influence actual goal-pursuit; that is, a person’s behavior directed toward an objective persists over time that resumes after interruptions (Bargh et al., 2001). In the context of health change behavior, long-term behavior is needed rather than just initial adoption or use. Therefore, this research predicts that social perception can act as a moderator to sustain a user’s intention to continue using the wearable fitness tracker.
Prior research has found that wearable activity trackers have been adopted by individuals seeking to enhance their personal fitness through increased self-monitoring and social connections with other users (Chiauzzi et al., 2015). Game dynamics can be classified from self-elements (to focus on competing with themselves and recognizing self-achievement) to social elements (interactive competition or cooperation). Keeping other factors constant, social elements may motivate users in a community environment (Huang & Soman, 2013).
Game dynamics enable a user to interact with other users in his/her social networks to obtain mutual reinforcement. The wearable producer and the user may coproduce value during the use of wearable. Moreover, the influence of the user’s health extends well beyond the firm-user dyad relationship to involve his/her own cognitive and emotional resources to include resources from friends, family, and other actors (McColl-Kennedy et al., 2012). There exist two popular types of social comparison strategies that emphasize either peer competitive or cooperative aspects. In these cases, on one hand, participants report that they enjoy the awareness and competing against their peer groups in achieving a higher physical activity level. On the other hand, cooperative mechanisms are based on social psychology theories that suggest that, when individuals develop a strong identity within a group, they are more committed to the group goal and its success; as a result, users tend to care more about collective outcomes and contribute more (Ufkes et al., 2016). These factors may lead users to have more stickiness and increase their user intentions.
Individuals within a peer game setting in a public social context observe others’ activities and adapt to their interactions. While in the self-goal achievement setting, which is anonymous and non-public, a user’s decision is based on individual preferences rather than peer game settings. Since the public context is associated with the use of peer game settings, social influences can affect group settings in driving users’ continued use intentions than individual game settings.
H4. The effect of gamification on users’ intention of continuously using wearables is moderated by their social perception. That is, high extent of game dynamic enabled by wearables will enhance users’ continued use intention when their social perception is high.
Methods and Study Design
Experimental Procedure
This study proposes that, based on the service-dominant logic (S-DL), continued use intention of wearables can be affected by users’ acceptance of value propositions and the congruence of perceived value. Value, as proposed by Helkkula et al. (2012), may be based on an imaginary event or thought, and the interaction between actors does not always need to be practically lived and may incorporate imaginary experiences without any contact with the service provider (Helkkula, 2011).
To support the paper’s assertions, scenario-based experimentation was conducted by manipulating wearable device features and guiding subjects to immerse themselves into the proposed value propositions describe by the scenarios. Subjects then filled out the questionnaires to test the hypotheses derived from the model of continued use intentions for wearable devices. An online scenario-based experimentation was chosen to answer the research questions with several advantages. Firstly the experimentation would allow for the control and manipulation of variables to achieve internal validity and offer considerable external validity (Bendapudi & Leone, 2003). Existing research has found that having participants imagine themselves in a situation can serve to elicit the same reactions that they would have had in real life (Montes & Zweig, 2009), particularly when assessing imaginary future value in experience (Helkkula et al., 2012). This advantage is essential in overcoming challenges in the research questions because it is hard and costly to manipulate the actual features of a wearable. Using this method, the atmosphere of a real situation can be created for the respondent to also generate a large number of responses. It is also less costly compared to laboratory experiments required for this type of research. The most significant challenge associated with this method involves creating scenarios that reflect the real features of wearables. This limitation was overcome by performing pre-tests before data collection and using manipulation and realism checks for data analysis.
This study used two antecedents as independent variables and two interactivity levels (low, front-end data only vs. high, interactive feedback) × three-game dynamics (self-goal attainment, peer competition, and peer collaboration) between-subjects factorial design. In total, six scenarios were generated, as shown in Figure 2. The questionnaire was then designed containing question items generated from the following constructs: (1) health status; (2) self-perception; (3) social perception; and (4) continued use intentions. The measurement items were adopted from existing literature in a seven-point Likert scale with minor wording adjustments for a wearable device study.

Scenario manipulation for interactivity and gamification.
In the scenario, interactivity was manipulated into high and low levels of interactivity. The high interactivity of a wearable device described in the scenario involved a third-party service (health experts and health insurance companies) integrated through feedback from a user’s activity. A low-interactivity scenario does not employ third-party integration and provides feedback only from data gathered during activities. The gamification scenarios are divided into three categories of game dynamics, namely self-goal achievement, peer competition, and peer collaboration. Self-goal achievement setting is a purely individual effort, whereas competition and collaboration are extended to group settings. In these settings, “lose scenarios” were designed, in which the user did not achieve the goal to motivate longer user engagement in the goal achievement process. Examples of the lose scenarios include “did not hit the target,” “lost the challenge,” and “contributed least among participants.”
Data Collection
To recruit the participants, a research panel company based in Taiwan was used. The eligibility criteria included Taiwanese citizens to ensure the commonality of the national healthcare service system. Taiwanese national healthcare covers the entire population and has been known to promote greater health awareness that in turn leads to a gradual increase in Taiwan’s life expectancy (Ministry of Health and Welfare, 2017). Other criteria were not set to ensure that the proposed scenario could be accepted as generic value propositions. The survey was back-translated into Traditional Chinese to ease participants in filling out the online survey.
Before formally distributing a scenario-based survey, a pilot test was conducted to revise the composed scenarios with question items. Survey data were collected for the main experiment over approximately 3 months and enhanced the accuracy of the collected data by ensuring that the participants read the scenario clearly and by enhancing the manipulation check. There were 306 valid respondents that passed the manipulation check. Table 2 presents the profiles of the participants.
Participant Profile of Experiment Survey.
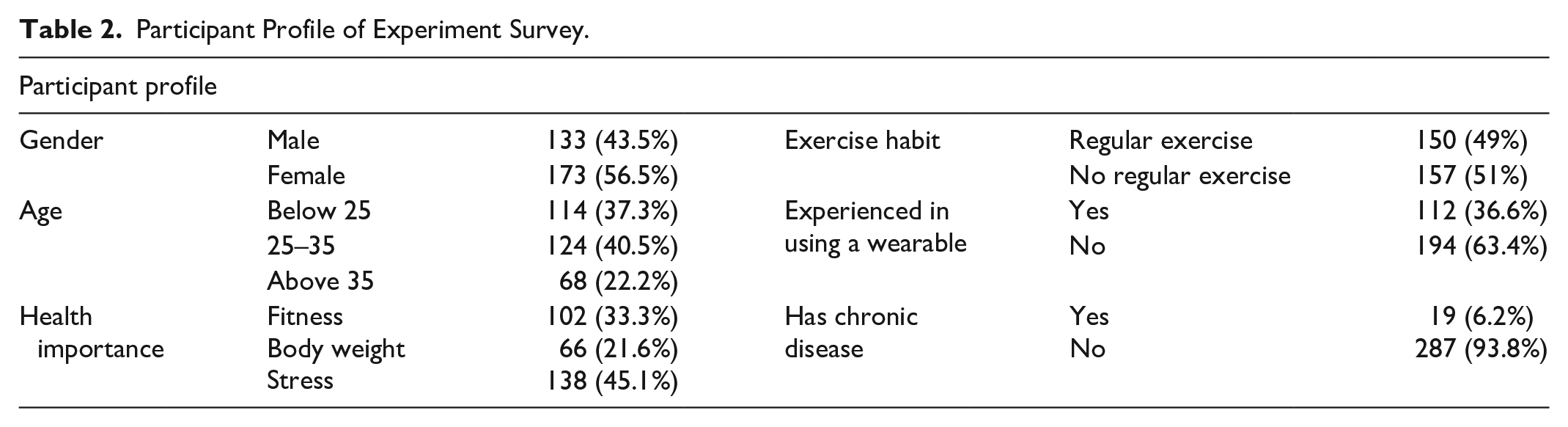
The survey consisted of three stages and began with an informed consent form to ensure that participation was voluntary, ensuring that participants knew that they could leave the experiment at any time. The first stage explored participants’ profiles, such as gender, age, health priority, exercise habits, and prior experience of wearables.
In the second stage, participants received an introduction to the experiment. Six manipulated scenarios and one control scenario were randomly assigned to participants as shown on Table 3. One participant was only exposed to one scenario. Participants were asked to read the scenarios assigned to them and view a rendering of a device interface (see Appendix 1-3). Participants were then instructed to answer the two manipulation check questions to ensure that they had read the scenario carefully. In the final stage, participants filled out the questionnaire on self and social perceptions, as well as their intention for continued use.
Sample Size of Seven Group Experiments.

Results
Reliability and Validity Analysis
This study examines the role of interaction design in wearable fitness trackers and users’ perceptions of continued use intentions. The measurement of continued use intentions was adopted using a seven-item scale developed by Bhattacherjee (2001). Under self-health perception, two factors were used alongside previously used measurement items with minor modifications, namely self-health risk perception (Witte et al., 1996) and self-health efficacy (Schwarzer & Renner, 2000), whereas under social perception, social influence and subjective norms were employed (Wang et al., 2020).
A confirmatory factor analysis (CFA) was performed on all of the constructs. Based on the analysis, items with loadings >0.50 were retained for further analysis. One item on health risk perception (HRISK 2) was abandoned due to its low factor loading. Furthermore, social influence and subjective norm items were considered a single factor in the factor analysis. Discriminant validity was assessed with average variance extracted (AVE). Higher AVE indicates greater reliability and convergent validity of a latent construct. The value of AVE should be greater than 0.5 (Ab Hamid et al., 2017). All of the variables proposed in the model were considered valid.
In terms of reliability, internal consistency was measured using composite reliability (CR), the results of which demonstrate that all measurement items used were well above the cut point of CR above 0.6 (Ab Hamid et al., 2017), as reported in Table 4. The value indicates that the reliability of measurement items is satisfactory. The results confirm the dimensionality of the solution and suggest discriminant validity (average variance extracted > 0.50 for all) and composite reliability (values > 0.70) for all of the variables.
Reliability and Validity Test.

To test the effectiveness of the manipulation, the six scenarios were also tested with a control scenario using a one-way analysis of variance (ANOVA). The results demonstrate that the six scenarios were significantly different from the control settings (there were no gamification and interactivity features in the control case, F(6, 299) = 4.15, p < .001). This finding suggests that the six manipulation scenarios were successful.
Hypothesis Testing
To test hypotheses H1 and H2 on the main effect, a 2 × 3 between-subject factorial ANOVA was performed to test the six scenarios (n = 260). To confirm the assumption of equal variances, Levene’s test was employed to determine the homogeneity of the variance. This result was significant at p > .05, indicating that the assumption was correct.
In the factorial ANOVA, continued use intention was the dependent measurement, with gamification and interactivity serving as predictors. This analysis revealed significant main effects for both factors. Specifically, greater gamification indicated higher intentions of continued use (F(2, 254) = 5.13, p < .01). Participants exposed to a high level of interactivity (vs. low) also indicated higher continued use intention (F(1, 254) = 5.39 p < .05). No other effects were observed for the variables with the interaction plot, as seen in Figure 3.

Graph plot on main effects of gamification and interactivity.
To test the robustness of the results, the effect of covariates on demographics was estimated, namely health status, exercise habits, and prior experience. Results of the analysis of covariance shown in Table 5 suggest that all covariates had no significant effect (p > .05) on the relationship between interaction design and continued use intention. For the purpose of parsimony, the following section only reports results based on the model without covariates included.
ANCOVA Results on Continued Use Intention.
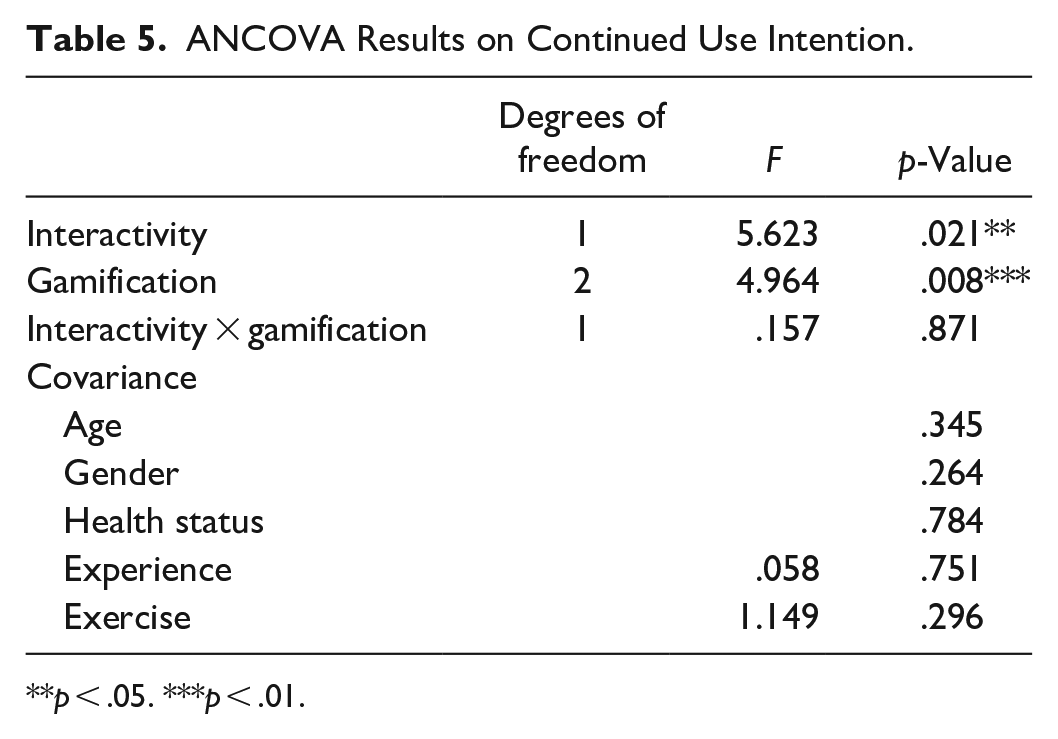
p < .05. ***p < .01.
For both levels of interactivity, continued use intention was low in self-achievement settings and increased in peer settings. On collaboration settings, the variable reached its peak; again, this trend was roughly the same for both interactivity settings. The fact that the line of low interactivity is lower than that of high interactivity reflects the main effect of interactivity. This finding is consistent with the theory that a higher level of interactivity will lead to higher continued use. These results suggest that users exposed to more interactive features have greater intention to continue using wearables (Mhi_int = 4.96 vs. Mlo_int = 4.64). Therefore, Hypothesis 1 is supported.
A Bonferroni post-hoc test found significant differences in the gamification scenario between self-goal achievement and peer collaboration (p < .01), while there were no significant differences in competition settings. Given that peer collaboration has a higher extent of gamification, participants exposed to peer collaboration settings showed higher continued use intentions (Mself = 4.58 vs. Mcomp = 4.75 vs. Mcoll = 5.07). A Helmert contrast analysis also provided similar findings, suggesting that the mean of self-setting is different than that of group settings (competition and collaboration), as shown by a Contrast Estimate and Difference of −.337 (p = .018). Thus, Hypothesis H2 was also supported.
In further analysis, the investigation was extended to determine whether self and social perception moderated the effect of interaction design on continued use intentions in prior findings. As a moderating effect was proposed, the interaction between gamification and interactivity was tested with self and social perceptions. The proposed moderators were continuous variables, thus, and the spotlight and floodlight (Johnson-Neyman, JN) technique (Spiller et al., 2013) was used. Floodlight analysis is derived from spotlight; this method was chosen over mean/median splits due to its robustness in seeking turning points for where exactly, in the absolute value of the moderator, the effect of the predictor changes from non-significance to significance (Krishna, 2016).
Firstly, the moderating effect of self-perception was used. Using the PROCESS macro with 5,000 bootstrapped samples, the results reveal a significant interaction between interactivity and self-health risk perception (b = −.36, t = −3.00, p < .01), indicating that health risk perception moderates the difference between low and high levels of interactivity.
The data suggest a crossover point. To more accurately understand this interaction, a spotlight analysis was conducted by subtracting either the value of one standard deviation below the mean or the value of one standard deviation above the mean from the self-health risk perception score, respectively (Spiller et al., 2013). In terms of the conditional effect, when health risk perception is low (i.e., one standard deviation below the mean, −1 SD), continued use intention with high interactivity is higher than that in low interactivity settings (Mhi = 4.98 vs. Mlo = 4.32; b = 0.657, t = 3.55, p < .001). The direction is in contrast to what was hypothesized.
To determine the directional predictions of hypothesis H3a, the guidelines provided by Spiller et al. (2013) and the JN technique were used. To decompose this interaction, a floodlight analysis was used to identify the region of self-health risk perception where the simple effect of the differences in interactivity was significant. The JN technique showed self-health risk perception; at a value of 4.72, the turning point was from significant to non-significant in the effect of interactivity (high vs. low) on continued use intention. In other words, when self-health risk perception is below 4.72, a user exposed to high interactivity has significantly more intent to continue use, as shown in Figure 4, compared to low-interactivity settings (confidence intervals, CI, between 0.29 and 1.02). For users with health risk perception above 4.72, differences between the two extents of interactivity are non-significant (p > .47) in predicting continued use intentions. Thus, hypothesis H3a is partially accepted.

Interaction Plot of Self-perception ((a) Health risk perception; (b) Self-health efficacy) and Interactivity.
The procedure was repeated to examine the effect of health self-efficacy in the relationship between interactivity and continued use intentions. The direction and propensity of results were similar to those on health risk perception; when health self-efficacy is lower, continued use intention in high interactivity is higher compared to a low-interactivity setting, and vice versa. However, the statistical test found that the moderating effect does not generate significant results (b = −0.17, t = −1.64, p = .10). Thus, hypothesis H3b is rejected.
Further, the moderating effect of social perception in the relationship between gamification and continued use intention was examined. The multi-categorical PROCESS macro (Hayes & Montoya, 2017) was employed since gamification is not a dichotomous but a categorical variable. Helmert coding was used for coding the three gamification scenarios to use a pairwise test to further examine differences among the three group settings.
Because it was not possible to use the JN technique in multi-categorical testing, the interaction was probed by estimating the effect of social perception using spotlight analysis. To perform this analysis, low social perception (a standard deviation below the mean, −1 SD), moderate social perception (using the mean, SD), and high social perception (+1 SD) were operationalized. The interaction test results indicate only small change in R2, ∆R2 = .013, F(2, 254) = 2.73, p > .066, showing no significant interaction effect. Therefore, Hypothesis 4 is rejected.
Upon further examination, it became apparent that the difference was significant between individual (self-achievement) types of gamification versus group (competition, collaboration) settings: (D1 × social), t = 2.3, p < .05. On the other hand, there was no significant evidence to suggest a difference between competition and collaboration settings: (D2 × social), t = 1.38, p > .16. For users with low social perception, the individual (self-achievement) scenario leads to higher continued use intention than the group scenario (competition, collaboration), whereas for users with high social perception, the group scenario leads to higher continued use intention than the individual scenario. Due to inadequate statistical significance, the direction of what was predicted is still supported.
Discussion
The findings of this study demonstrate how interaction design through gamification and interactivity should be well-integrated with users’ self and social perceptions to create a seamless value co-creation process. The analysis suggests that wearables with higher interactivity (integration of both back- and front-end services) and gamification (group dynamic settings) are more likely to influence users to continue using a wearable device. This finding is in line with flow theory; when a user is experiencing total involvement through an engagement mechanism, there will be a holistic sensation, which will trigger continued use intention (Kim et al., 2013). This finding also supports the value conceptualization of S-DL, in that once value increases from the integration of resources and the connection between people and technology, customers will be more likely to sustain prolonged engagement (Vargo & Akaka, 2012).
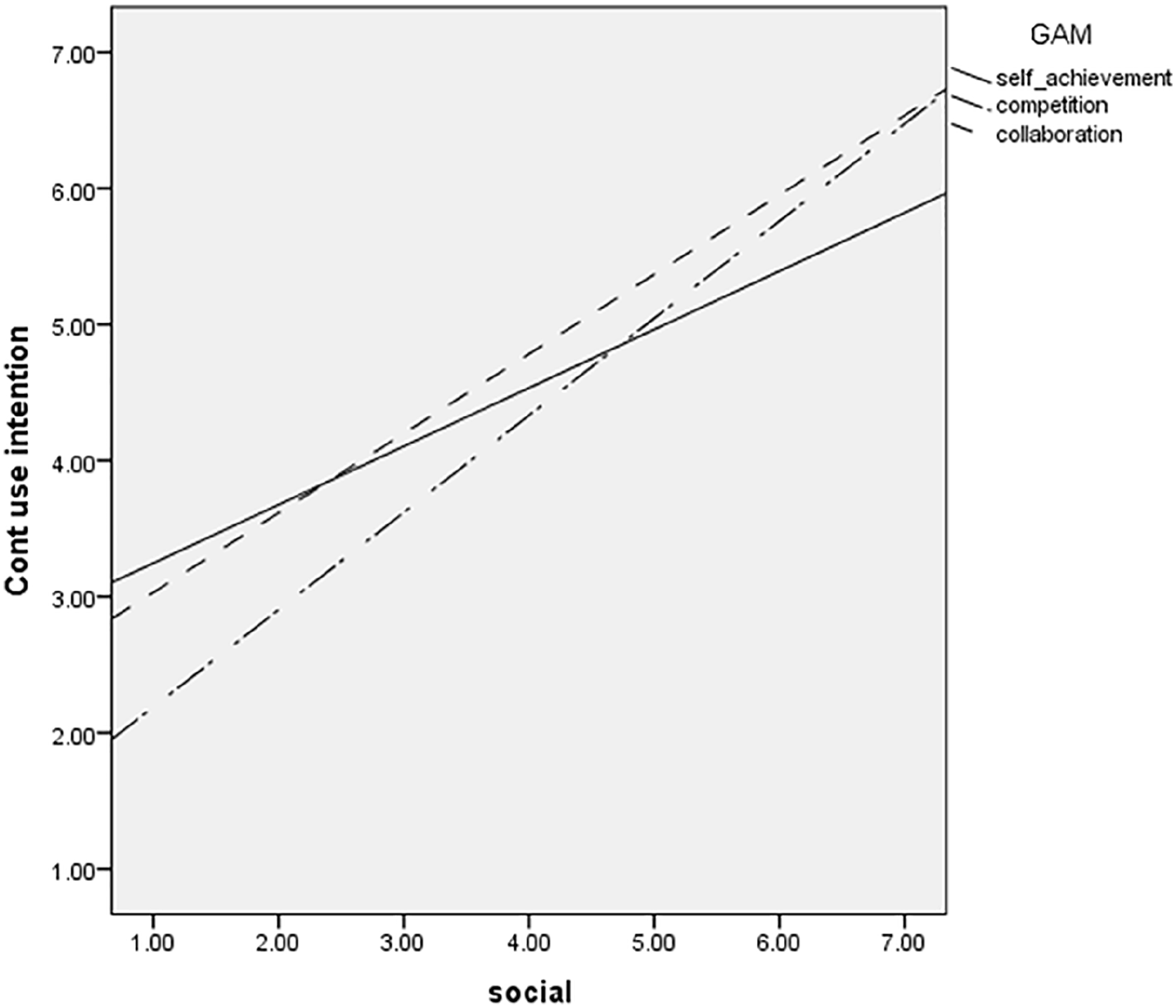
The effect of social perception on different extent of gamification to continued use intention.
What interactivity offers from flow theory is closely tied to user involvement. Interactivity was found to have several potential benefits, including offering users a sense of fun, satisfaction, and engagement (Teo et al., 2003). Through an interactive device, the user will feel a dyadic interaction as they communicate with personal healthcare assistants and service providers, whereas gamification may provide users with a positive flow experience and feelings of acceptance in social networks. Therefore, this involvement has a positive effect on sustaining use intention. However, there is no evidence of interactions between interactivity and gamification that affect users’ intention of continuously using wearables, suggesting that interactivity and gamification are mutually exclusive. This finding implies that the two mechanisms can be applied individually.
The results show that a higher level of interactivity leads to a higher intention to continuously use wearables. Intention is even higher when the resource becomes richer (Jaakkola & Alexander, 2014). Therefore, once front- and back-end systems are integrated, greater value is provided to the user. Furthermore, when it is integrated with third-party services, the feedback from a user’s exercise history and the comparison of performance with other users, the system provides additional exchanged resources that can be taken advantage of by the user. This finding also supports the conceptualization of value in S-DL, in which value is created through user-device interactions over an extended period (Beirão et al., 2017).
A large number of group dynamics (compared to individual game challenges) also positively influences a user’s continued use, a finding that demonstrates the effectiveness of collective behavior in health behavior changes. In terms of the impact of gamification itself, challenge and reward-based game mechanics positively influence users’ positive behavior (Whittakee et al., 2021). When a wearable is designed that can offer a gaming experience (both group and game mechanics in the form of challenges and goals), it will subsequently enhance customers’ overall value creation (Huotari & Hamari, 2012).
As we investigated further, it was found that individuals’ perceptions of their health play an important role in the use of wearables. It is surprising that the findings of this research suggest that people with low self-health efficacy are more likely to perceive value from interactivity and exhibit greater intentions to continue using wearables. The HBM explains that individuals’ behavior in certain health activities depends on weighing the effectiveness of reducing a health threat against possible negative outcomes associated with that action. People with lower health risk perceptions rely more on wearables to provide additional information. Users feel helpful by additional features and feedback provided by wearables through interactivity.
In terms of the effect of self-efficacy, one of the most significant predictors in healthcare decision making is conscientiousness, which is positively related to beneficial health behaviors such as physical fitness. Conscientious individuals tend to be autonomous in enhancing their health and prefer more active participation in healthcare decision making (Flynn & Smith, 2007). It may be inferred that individuals with self-discipline can manage themselves and do not rely much on wearables. The desire to avoid becoming ill is a value, and the belief that a specific health behavior can prevent illness is an expectation. However, these individuals are likely to manage their health activities and use wearables as a reminder or tracker. For these users, interactivity features do not have a significant effect on their health decision making. Therefore, a different extent of interactivity may not be significant.
In terms of social perception, there is no evidence from the findings of this study to support the interactions between gamification and social perception. It was found that people with low social influence preferred the individual setting, whereas people with high social influence prefer a peer setting for the purpose of higher intention. However, it is unclear as to whether the intention is affected by group dynamics since there are no significant differences in competition and collaboration settings. Therefore, collective behavior has a positive effect, but the true motives behind this effect are unclear. This finding may suggest that most people still think that maintaining health (through wearables) is self-domain decision making. Further investigation is required to support this assertion.
Based on the findings of this study, it is apparent that a technology-assisted healthcare system should actively respect individuals’ perspectives. This finding is in line with growing concern for a proactive role in healthcare research (Smith et al., 2009). Relationships among actors in health management activities are inevitable. However, rather than bringing an inside-out perspective that requires that users reveal more about their health information, the value co-creation process should use the outside-in concept by providing customized service that respects users’ health profiles and motives.
Conclusion
This research found that a higher level of gamification and interactivity embedded in wearables lead to higher continued use intentions. Furthermore, only self-health risk perception moderates the relationship between interactivity and continued use intention, whereas social perception is not entirely proven as a moderator between gamification and continued use intentions. Theoretical and practical implications, as well as limitations, are provided in the following sections.
Theoretical Implications
Theoretically, this research adopted a systemic view of wearables as an actor to trigger users to co-create value with not only the wearable itself but also other actors within the ecosystem. Existing research on wearable fitness trackers has focused too much on the individual adoption or an isolated view of users’ behaviors and/or device-specific features. In contrast to prior research, this study crossed dyadic boundaries of user-device relationships into multi-actor interactions from the service system perspective.
This study provides an alternative view on examining continued use intentions using value co-creation perspective. By using this perspective, this paper suggests that continued use intentions can be driven by the value propositions that promote users’ active value co-creation behavior rather than merely relying on prior adoption.
Practical Implications
From a practical perspective, this research offers implications for marketers and wearable device producers in designing a device that offers long-term value. Value propositions become important determinants, and producers should always promote novel interactive features that encourage users’ active engagement to sustain rather than measuring satisfaction to predict continued use.
Wearables producers may design interactive features and cooperate with related service providers to tailor service offerings to meet users’ needs. However, wearable producers should be careful when determining users’ profiles while providing these features and taking their health risk perceptions into account. Customization and profiling before a user start to experience the service would be an ideal beginning point for the device to learn about users’ patterns. As suggested in the findings of this study, higher interactivity by integrating with third-party services (i.e., data analytics, dietitian/health experts, and insurance) should be presented to users concerned with their health and low efficacy to maintain their own health.
Wearable producers are also advised to adopt gamification features on their devices. Game mechanics should promote a sense of challenge and goal attainment to make goals always relevant to users. The results of this study emphasize the importance of group dynamics (such as through peer-competitions and collaborations) to be embedded in a wearable device, particularly in embracing “the new normal” due to the COVID-19 pandemic, which limits social interactions, this feature can help to fight a sense of loneliness and self-isolation (Laato et al., 2020). There will be a higher need to socialize in a safe way so that group activity in virtual settings can be a solution.
However, the findings of this study suggest that there should be options to choose gamified settings in either group or individual modes because we also find that the impact of gamification is highly moderated by social influence. For example, producers can promote group competition and collaborations to younger or impressionable users who are driven by peers or social networks.
Limitations and Directions for Future Research
This research has a number of areas for potential improvement. The respondents were skewed in terms of health status. The research only asked about self-reported health risk perception; though there was not sufficient data to consider more objective measurements, such as healthy participants or those with serious health concerns. Health-related behavior may also be influenced by healthcare systems. Further research should examine factors affecting health risk perception such as users’ reliance on healthcare protection, the responsibility that they bear, and the values that they believe are related to the risk of becoming sick.
It may be interesting to consider wearable features in a specific scenario. This study only examined basic functions such as activity tracking and calories. Further research may distinguish basic activity trackers versus health-dedicated features to profile respondents differently. Users of these two wearables may possess different motives and orientations for long-term usage behavior. The different value propositions proposed by wearable producers might also signal usage. Thus, use motivations and variations in health risk perception among groups of users can be overcome. The other limitation is on scenario design. In designing gamification and interactivity, research can further examine cultural embeddedness, such as the role of individualism or collectivism in game dynamics settings and interactivity features in relation to users’ trust in information and interactivity type regarding willingness to obtain and share health information. Cultural factors, such as risk avoidance profile and a long-term orientation, could be the determinants.
Finally, value co-creation perspective has the potential to explain continued use, particularly in terms of technological services that require multi-actor interactions (e.g., health services). Technological devices serve as platforms for resource exchange. The impact of interaction and resource exchanges might also depend on who are the actors involved and what kind of resources are being exchanged. Therefore, future research may benefit from exploring the potential of value co-creation perspective in examining continued use in other sectors that have intense, rich interactions between actors, such as tourism or education.
Footnotes
Appendix
Questionnaire Items.

| Items | |
|---|---|
| Continued use intention | |
| CIT1 | I intend to continue use of the wearable fitness tracker for the purpose of maintaining my personal health |
| CIT2 | I would like to recommend my friends and family to use a wearable fitness tracker |
| CIT3 | In general, I intend to continue using the wearable fitness tracker |
| Self-health risk perception | |
| HRISK1 | In general, I would say that I am in a good health |
| HRISK2 a | My current body weight is a threat to my health (dropped) |
| HRISK3 | Compared to people of the same age, how do you rate your own health condition? |
| HRISK4 b | I am at higher risk of suffering illness than others |
| Self-health efficacy | |
| EFFIC1 | I can manage to carry out my exercise intentions even when I feel depressed |
| EFFIC2 | I can manage to carry out my exercise intentions when I feel tired |
| EFFIC3 | I can manage to carry out my exercise intentions even when I feel busy |
| Social influence | |
| INFL1 | It is important to keep in touch/share events (community) with my friends and family |
| INFL2 | It is important to be connected and meet other people with similar interests in health |
| INFL3 | It is important to tell my friends and family about my experiences of using the wearable fitness tracker |
| INFL4 | People who influence my health behavior (doctors, physician, personal trainer) think that I should use the wearable fitness tracker |
| INFL5 | People who are important to me (e.g., my parents, spouse, children, close friend) think that I should use the wearable fitness tracker |
Dropped due to low factor loading.
Reversed item.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the project MoST 105-2410-H-007-037-MY2 from the Ministry of Science and Technology – Taiwan.