
Abstract
This study examines the well-being of older Malaysians, using Control, Autonomy, Self-Realization, and Pleasure (CASP-19) score. Data for this study came from a cross-sectional survey on older adults living in a multiethnic metropolitan in Malaysia. The sample comprised Asia’s three major ethnic groups. Bivariate and multivariate analyses show significant ethnic differentials in quality of life (QoL). Results from multiple regression show that CASP-19 is strongly influenced by self-rated health and the ability to manage expenditure, and to a lesser extent by educational level and marital status, but not by age, gender, work status, co-residence with children, and housing tenure. After adjusting for sociodemographic variables, self-rated health was the only significant factor affecting the QoL of all ethnic groups. Ability to manage expenditure was also significant among the Chinese and Indians. Marital status matters for the Chinese, while education and housing tenure matter for the Indians. Differences in the effects of the various factors on the QoL of older adults require specific strategies and programs for different target groups.
Introduction
Population aging is a relatively new phenomenon in Malaysia. However, consequent upon the continuing fertility decline to below the replacement level since 2012, Malaysia will be an aging nation in 2035 when 15% of the population will be aged 60 and over (Department of Statistics, Malaysia, 2012). The increasing number of older people is straining the health care system, and the social protection system is inadequate to provide for the financial needs of older people. Moreover, the erosion of family care and support due to demographic and social changes has also affected the quality of life (QoL) of older Malaysians.
Malaysia is a multiethnic country. Of the 28.3 million population enumerated in the 2010 Population Census, approximately 92% were Malaysian citizens. Among the citizens, Malays made up 54.6%, Chinese 24.6%, Indians 7.3%, other indigenous groups 12.8%, and others 0.7%. Each ethnic community has maintained its sociocultural practices concerning religion, language, dress, food, and place of residence while developing an integrated national identity. Islam is the national religion. All Malays are Muslims, the majority of Malaysian Chinese are Buddhists, and most Indians are Hindus. However, a sizable proportion of Chinese (10%) and Indians (7%) are Christians. The Malay language (Bahasa Malaysia) is the official language, but English is widely used by all ethnic groups. The majority of Chinese and Indians send their children to vernacular schools. The Malays dominate the civil services and in agriculture, while the non-Malays are more actively involved in commerce and trade, and other urban occupations. Multiethnic Malaysia provides an excellent setting for studying the QoL of older adults.
With an urbanization level of about 77% in 2020, Malaysia is the most urbanized nation in Southeast Asia, after the city-state of Singapore and Brunei. The World Bank classifies Malaysia as an upper-middle-income country, and the United Nations categorizes it as a very high Human Development Index country.
Greater Kuala Lumpur includes the Federal Territory of Kuala Lumpur and four adjacent districts of Selangor state. It is the administrative, commercial, industrial, and educational hub of the country. The Malays make up about 47% of the population in Greater Kuala Lumpur, Chinese 31%, Indians 11%, non-citizens 8.4%, while others make up the remaining (Department of Statistics, Malaysia, 2013).
Issues related to older people have attracted increasing attention from policy-makers and researchers, as evidenced by the adoption of national policies for older people and proliferation in geriatric and gerontological research. In Malaysia, the National Policy for the Elderly, adopted in 1995, was revised as the National Policy for Older Persons and Plan of Action for Older Persons in 2011. The main objective of the Policy is to develop a caring society, enhance capacity building, advance health and well-being, and address the safety and social security of older adults (Department of Social Welfare, Malaysia, 2011).
Accurate and reliable measurement for the QoL is needed for the formulation of appropriate policies and strategies to improve well-being of older adults. The CASP-19 is one of the widely used QoL measures of older people (Hyde et al., 2003). This composite measure was derived from the social theory on human needs (Maslow, 1943), and its four domains cover human needs relevant in later life: control, autonomy, self-realization, and pleasure (Doyal & Gough, 1991). The scale is especially relevant for those in early old age or the Third Age when one can focus on self-development and self-realization (Laslett, 1996).
The differences in the QoL across different ethnic groups may be due to the sociocultural differentials in perception, expectation, and reporting. Better knowledge and understanding of the QoL of older adults from diverse sociocultural backgrounds is needed for policy interventions and program implementation. This study examines the differences in the QoL of older adults of Asia’s three major ethnic groups living in a metropolitan area in Malaysia. The present study also investigates the factors affecting the QoL of the different ethnic groups.
Literature Review
The CASP-19 and its technical properties and factor structure were described, evaluated, and interpreted by many researchers (Bowling, 2009; Bowling & Stenner, 2011; Higgs et al., 2003; Howel, 2012; Hyde et al., 2003; G. R. Kim et al., 2015; Layte et al., 2013; Lima et al., 2014; Sexton et al., 2013; Sim et al., 2011; Wiggins et al., 2008). These studies found CASP-19, with its excellent psychometric properties, a useful scale for measuring the QoL of older people. CASP can discriminate subgroups differing in health and socioeconomic status and across ethnicities and geographical regions (Grant & Bowling, 2011; Howel, 2012). A few studies have also been conducted to validate the CASP-19 instrument for use in the Asian culture (Heravi-Karimooi et al., 2018; Nalathamby et al., 2017; Wu et al., 2013).
CASP-19 was used to measure the QoL of older people in a few major surveys, such as the Survey of Health, Ageing and Retirement in Europe (SHARE) (Knesebeck et al., 2007), English Longitudinal Study of Ageing (ELSA) (Rafnsson et al., 2015), and the Irish Longitudinal Study on Ageing (TILDA) (McGee et al., 2011). Data from these surveys yielded a sizable literature on CASP (Bowling & Stenner, 2011; Chen & Chen, 2017; Grant & Bowling, 2011; Higgs et al., 2003; Khan & Tahir, 2014; Sexton et al., 2013; Sim et al., 2011; Wiggins et al., 2008; Wu et al., 2013). While most CASP studies were conducted in Europe, such studies have also been done in several Asian countries (Abdul Mutalip et al., 2020; Amit & Litwin, 2010; Damri & Litwin, 2016; Ganapathy et al., 2020; Heravi-Karimooi et al., 2018; Y.-J. Kim & Kang, 2020; Lane et al., 2020; Levin, 2013; Litwin et al., 2017; Nalathamby et al., 2017; Ramli et al., 2020; Wu et al., 2013, 2015).
Various authors have shown significant influence of socioeconomic factors on the well-being of older people (Bilotta et al., 2011; Blane et al., 2007; Knesebeck et al., 2007; Netuveli et al., 2006; Wiggins et al., 2004). It is common knowledge that health status and well-being are closely interrelated. Most of the studies were based on self-reported health status (Abdul Mutalip et al., 2020; Boyle et al., 2010; Collins et al., 2008; Gabriel & Bowling, 2004; Lane et al., 2020; McGee et al., 2011; Netuveli et al., 2006; Wiggins et al., 2004). Relatively few studies have examined the effects of objective measures of health on QoL, such as being inflicted with chronic diseases, disability, and depression, on QoL of older people (Abdul Mutalip et al., 2020; Blane et al., 2004, 2008; Chen & Chen, 2017; Lane et al., 2020; Ramli et al., 2020; Sexton et al., 2015; Wu et al., 2013).
Past studies have found a curvilinear relationship between age and QoL in old age, with a peak at early old age (60–74 years) (Layte et al., 2013). A study using ELSA found that age, aging in place, place, and the attachment to place interact in complex ways to affect the well-being of older people (Gilleard et al., 2007).
Education was found to be positively correlated with the QoL of older people (Knesebeck et al., 2007; Ma & McGhee, 2013). Niedzwiedz et al. (2014) found significant inequality in QoL by educational level for both men and women. The effects of employment on the QoL of older people are not always consistent across studies, with a positive correlation in some studies (Khan & Tahir, 2014) and negative correlation in others (Yahaya et al., 2010).
The few Malaysian studies on QoL dealt with specific groups such as diabetes patients and disabled youth. These studies found significant ethnic differentials in the QoL (Goh et al., 2015; Shamsul et al., 2013). However, a study conducted in neighboring Singapore found no significant ethnic differentials in QoL (Lane et al., 2020). Apart from socioeconomic variables and perceived health status, Abdul Mutalip et al. (2020) found that activities of daily living (ADL) and instrumental activities of daily living (IADL) are also significant predictors of the QoL of older adults in Malaysia.
Research Design
Data From MELoR Survey
This analysis used data from the baseline cross-sectional survey (first wave) of the Malaysian Elders Longitudinal Research (MELoR). MELoR is a multidisciplinary study of older adults living in a metropolitan area in Malaysia (Kuala Lumpur and its satellite town of Petaling Jaya). The survey aimed to interview a random sample of 500 respondents aged 55 and over from each of the three main ethnic groups (Malays, Chinese, and Indians) to achieve an overall sample of 1,500. The minimum sample size of 500 is required to limit the margin of error to about 4.5% at 95% confidence level. The sampling frame was the electoral roll at three parliamentary constituencies in Kuala Lumpur and the satellite town of Petaling Jaya. Out of the 8,769 invitations sent out to the three main ethnic groups (in about equal proportion), 5,815 participants with contactable addresses were identified. Of these, only 3,334 were eligible for the survey (criteria below). The inclusion criteria were age 55 years and above, willing to provide informed consent, and belonging to one of the three major ethnic groups of Malay, Chinese, or Indian. The survey excluded non-Malaysians, institutionalized older adults, and those with communication difficulties, including cognitive impairment, affecting their ability to provide valid responses.
A team of researchers comprising faculty members from various disciplines conducted the survey. The respondents were interviewed using the computer-assisted method. The fieldwork was carried out by trained enumerators between November 2013 and October 2015. A total of 1,565 respondents (519 Malays, 544 Chinese, and 502 Indians) were successfully interviewed. However, this analysis was confined to the 1,264 respondents aged 60 and over. Appropriate weight was applied to each ethnic group in the analysis to account for the disproportionate sampling. The weight for each ethnic group was calculated by dividing the population proportion with the sample proportion.
The questionnaire used was a compilation of validation tools and survey items and was pre-tested and back-translated in four languages: English, Bahasa Melayu, Mandarin, and Tamil (Romli et al., 2018). Based on the same data set as the present study, an earlier study using both the exploratory and confirmatory approaches has validated the CASP-19 measure for use in the Malaysian context (Nalathamby et al., 2017). A description of the research design of the MELoR cohort has been published previously (Alex et al., 2018; Lim et al., 2017; Mat et al., 2019; Romli et al., 2018).
The Variables
The dependent variable is CASP-19, a composite measure of the QoL. CASP-19 score consists of four questions on Control domain (ability to control their environments), and five questions each on Autonomy domain (self-determination and freedom from unwanted interference of others), Self-Realization and Pleasure domains (active and self-reflexive aspects of living that bring reward and happiness to people in later life). Each item was measured on a 4 point Likert-type scale: “never,” “not often,” “sometimes,” and “often,” with a range of 0 to 3. The 19 items were summed (with the reverse coding of negative responses for six items) to form CASP-19. The score ranges from 0 to 57, with a higher score indicating better QoL. Cronbach’s alpha reliability test was used to assess the internal consistency of the index. The independent variables include age, gender, ethnicity, marital status, educational level, current work status, self-rated health status, housing tenure, ability to manage monthly expenditure (score 1–10), and co-residence with adults children.
Internal Consistency and Correlation
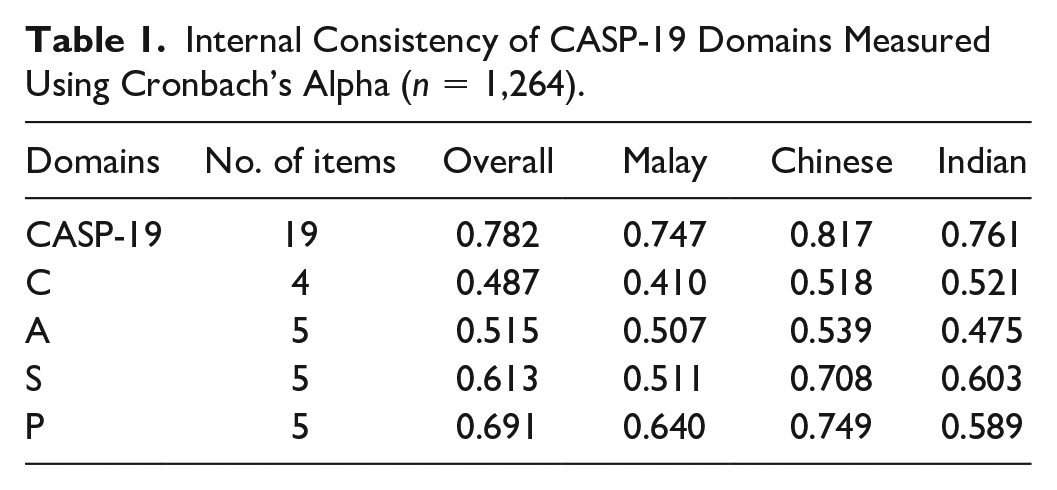
The internal consistency of CASP-19 and each domain was assessed using a reliability test. A Cronbach’s alpha value of 0.6 is considered acceptable and adequate for internal consistency, and a value of less than 0.6 is considered poor (Streiner & Norman, 2008). Table 1 shows adequate internal consistency of the items used for the computation of CASP-19 for all three ethnic groups. The Cronbach’s alpha values for Control and Autonomy for all the three ethnic groups (and for Self-Realization for the Malays and Pleasure for the Indians) are below the acceptable range for internal consistency. Hence, our analysis was confined to the composite measure of CASP-19.
Internal Consistency of CASP-19 Domains Measured Using Cronbach’s Alpha (n = 1,264).
Statistical Analysis
The analysis began with a description of the sample distribution, followed by bivariate analyses of CASP-19 for each ethnic group. Independent samples t tests/one-way analysis of variance tests were run to compare the mean scores of CASP-19 across the categories of the independent variables. Multiple regression analysis—a method commonly used to analyze CASP-19 (Abdul Mutalip et al., 2020; Bilotta et al., 2011; Howel, 2012; Netuveli et al., 2006; Okulicz-Kozaryn & Golden, 2018; Ramli et al., 2020; Wiggins et al., 2004), was used to assess the independent and combined effects of these variables on QoL, as measured by CASP-19. The sociodemographic variables were entered first in Model 1, followed by the economic variables (living in the self-owned house, and how well they can manage their monthly expenditure) in Model 2, self-rated health in Model 3, and all the study variables in Model 4—the full model. There is ample evidence that points to the predominant effect of health on happiness (Blane et al., 2008; Boyle et al., 2010; Liu et al., 2016; Sexton et al., 2015). Hence, self-rated health was entered as a QoL predictor, and used as a control variable for other sociodemographic factors, as done by Okulicz-Kozaryn and Golden (2018). The results were considered statistically significant if the p value is less than .05. Data analyses were carried out using SPSS for Windows version 25, released by IBM Corporation in 2017.
Results
Sample Description
The sample is rather evenly spread across the four age groups (60–64, 65–69, 70–74, and 75+) (Table 2). Male respondents made up about 46% of the sample. The Malays made up 57.1%, Chinese 29.2%, and Indians 13.7%. In this sample, 35% of the respondents had primary or no schooling, 43% had secondary education, and about 23% had tertiary education. Exactly three-quarters of the respondents were currently married. Only 18% of the respondents were currently working. Nearly two-thirds (66%) of the respondents lived with their children, and 55.4% stayed in their own house. About 43% of the respondents considered themselves to be good at managing their monthly expenditure (score 8–10), and only about 7% considered themselves as poor in managing their monthly expenditure (score 1–4). A little more than half of the respondents rated their health either as good (45.0%) or very good (10.5%), and only 6.0% perceived themselves to be in poor health, and the remaining 38.5% rated their health as fair. The percentage reporting having poor health increased from 4.7% among those aged 60–64 to 9.9% among those aged 75 and over.
Sample Characteristics of Respondents by Selected Variables (n = 1,264).

Missing values are excluded from the calculations. bThe weight for each ethnic group was calculated by dividing the population proportion with the sample proportion.
Bivariate Analysis of CASP-19
The average CASP-19 score for the whole sample was 45.04 (95% confidence interval [CI] [44.6, 45.5]), representing 79% of the total possible score of 57 (Table 3). The Malays had the highest score in CASP-19 of 46.36, followed by the Chinese (43.69) and the Indians (42.33). The standard error of mean CASP-19 was much higher among the Chinese (0.427) and the Indians (0.375) compared with the Malays (0.323). This finding suggests a lower reliability of the estimate for the minority groups.
Mean CASP Scores by Ethnicity, Socioeconomic Variables, and Perceived Health Status.
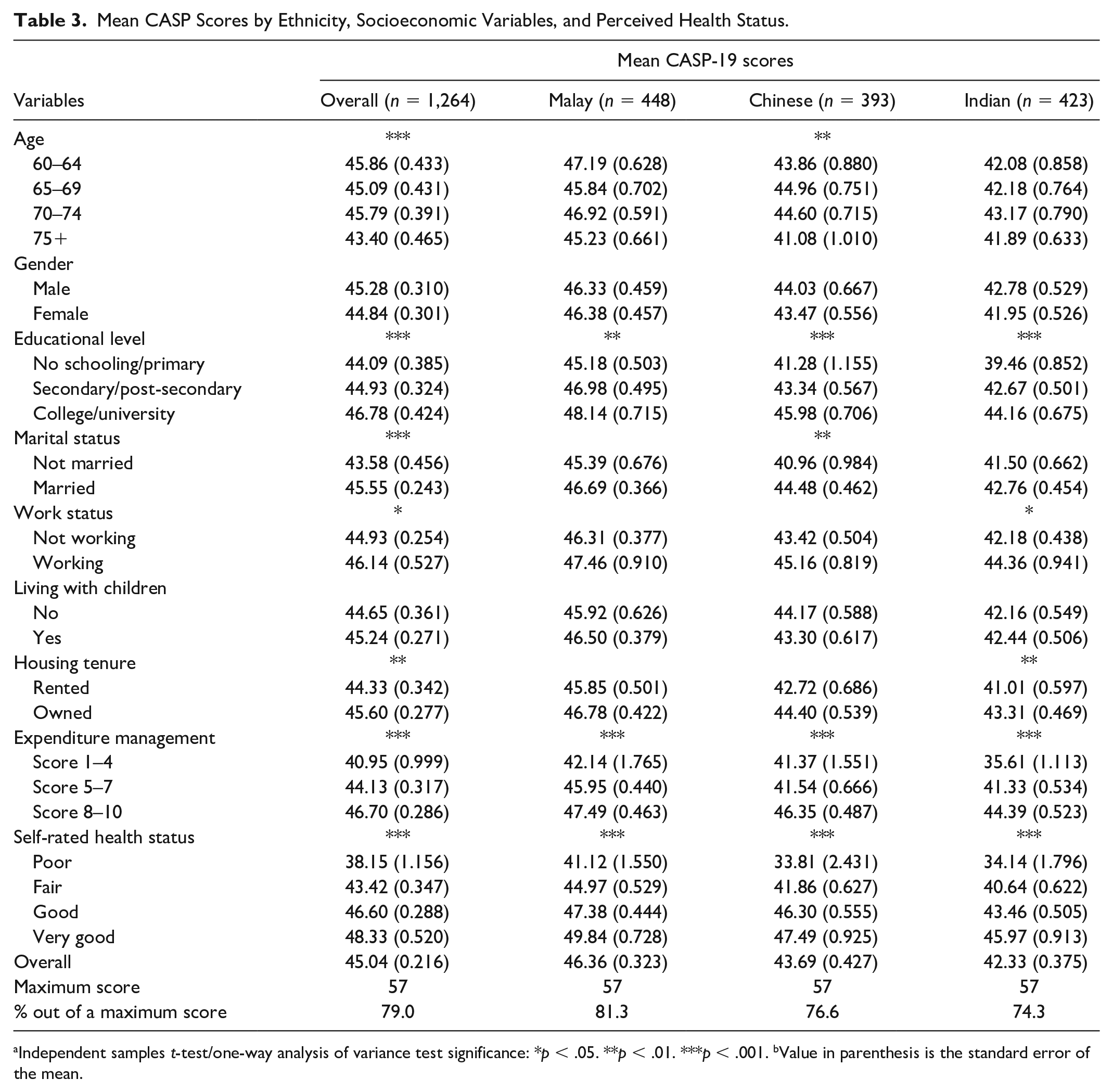
Independent samples t-test/one-way analysis of variance test significance: *p < .05. **p < .01. ***p < .001. bValue in parenthesis is the standard error of the mean.
No significant gender differential in QoL was found in this sample. The QoL differs significantly across age groups for the Chinese, but not for the Malays and Indians. Chinese aged 75 and over had a significantly lower QoL than the younger ones, but the CASP-19 scores were not significantly different across age groups below 75.
For all ethnic groups, QoL was positively correlated with educational level. The educational effect on QoL was most pronounced among the minority groups. Across all educational levels, the QoL was highest among the Malays and lowest among the Indians. These figures need to be interpreted with caution, given the higher standard errors for the estimates among the Indians and Chinese with primary education.
Married older persons tended to have higher QoL than unmarried persons among the Chinese. However, there was no significant difference in the QoL according to marital status among older Malays and Indians. Living with children did not have a significant effect on QoL. However, the Malays had higher QoL than the Chinese and Indians, whether they were co-residing with their children or not.
Current work status and housing tenure were positively related to QoL for the overall sample and the Indians. Nevertheless, these two variables did not have a significant effect on QoL for the Malays and Chinese.
Self-rated health and the ability to manage expenditure were the two most significant QoL predictors for all three ethnic groups. These findings underscore the importance of good health and financial adequacy in ensuring high QoL in old age. While the Malays tended to report a consistently higher QoL than the Chinese and Indians, the ethnic differentials in QoL were much more pronounced among those with poorer health and those who were unable to manage their expenditure.
Multivariate Analysis
The results from multiple regression show that the overall model is statistically significant and explains 19.5% of the variance in the overall CASP-19 or QoL of the older adults in this study (Table 4). The Malays had a significantly higher QoL than the Chinese and the Indians. Separate regression analysis by ethnicity (Tables 5–7) indicates that those who were currently married had higher QoL than those who were not currently married only among the Chinese. The education and housing tenure effect is significant only among the Indians. The ability to manage expenditure (in interval scale) had a significant effect on the QoL only for the Chinese and the Indians. Self-rated health was a significant predictor of QoL for all three ethnic groups. Exact age, gender, current work status, and co-residence with children had no significant association with perceived QoL for all the ethnic groups.
Results of Multiple Linear Regression Analyses for CASP-19 (Overall Sample, n = 1,264).

Note. SE = standard error.
t-test significance: *p < .05. **p < .01. ***p < .001.
Results of Multiple Linear Regression Analyses for CASP-19 (Malay Sample, n = 448).

Note. SE = standard error.
t-test significance: *p < .05. **p < .01. ***p < .001.
Results of Multiple Linear Regression Analyses for CASP-19 (Chinese Sample, n = 393).
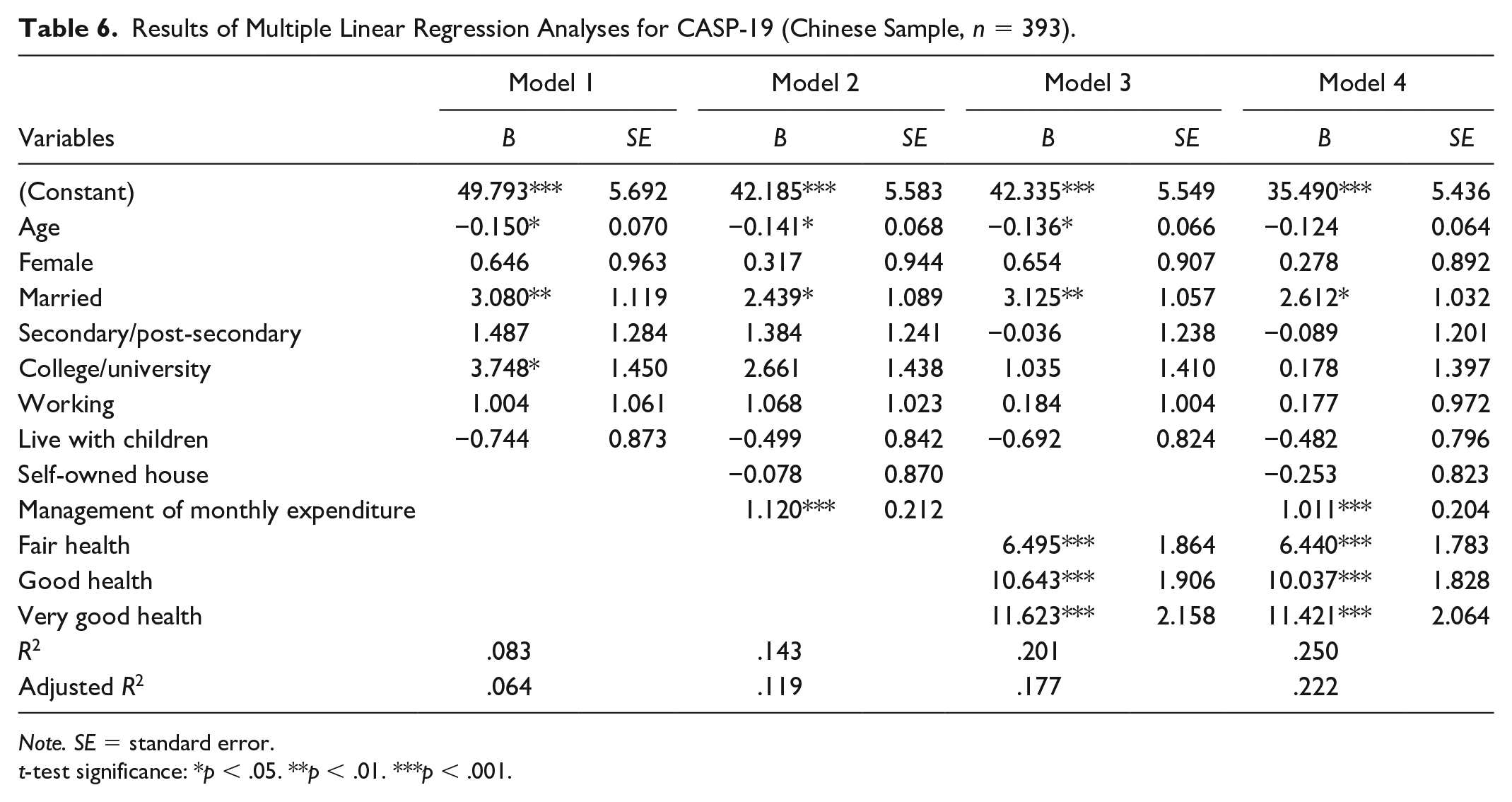
Note. SE = standard error.
t-test significance: *p < .05. **p < .01. ***p < .001.
Results of Multiple Linear Regression Analyses for CASP-19 (Indian Sample, n = 423).

Note. SE = standard error.
t-test significance: *p < .05. **p < .01. ***p < .001.
For the overall sample, Model 1 shows that the ethnic variable had the most substantial effect on QoL, with the Malays having significantly higher CASP than the non-Malays. After adjusting for the ability to manage monthly expenditure did not affect the ethnic differentials. However, controlling for self-rated health attenuated the Malay-Chinese differential somewhat.
Older adults in this sample who had tertiary education had the highest QoL, followed by those with secondary education, net of other sociodemographic variables. Adjusting for self-rated health reduces the educational differentials in QoL substantially, but the economic variable had a much smaller effect on the differential in QoL between the educational categories, especially between those with primary and secondary education. The QoL decreased with age and was slightly higher among the married adults than the singles, but age became insignificant with the inclusion of either the economic or health variable. The effect of marital status on QoL was slightly attenuated with the inclusion of the economic variables, but it remained almost unchanged after the inclusion of self-rated health. Gender, work status, and co-residence with children did not significantly affect the QoL of older adults in all the regression models for the total sample and each of the ethnic groups.
Education was the only socioeconomic variable affecting the QoL for all three ethnic groups. Separate regression for each ethnic group shows that the education effect became insignificant for the Chinese after including either the economic or health variable. The educational effect also became insignificant for the Malays after the inclusion of the health variable. However, it remained significant for the Indians even after controlling for the economic and health variables. Age had a significant effect on QoL only for the Chinese, but that became insignificant when both the economic and health variables were entered into the equation. Being currently married had a positive effect only among the Chinese, and it remained significant even after controlling for the economic and health variables.
Looking at Model 2, the ability to manage monthly expenditure had a positive effect on the overall sample and each of the ethnic groups, but it became insignificant for the Malays after the inclusion of self-rated health in Model 4. Staying in the self-owned house had a significant effect on the QoL of the Indians only. Self-rated health was positively correlated with higher QoL for all the ethnic groups, and its effects were stronger than those of the economic variables, as shown by the t-statistics (coefficients/standard errors) and the increments in the coefficients of determination (Model 2-Model 1 vs. Model 3-Model 1).
In the full model (Model 4), self-rated health and ethnicity were the two most important determinants of the QoL of the older people, followed by the ability to manage monthly expenditure, marital status, and education. For all the ethnic groups, self-rated health was the most dominant determinant of QoL, followed by the ability to manage monthly expenditure. Among older Malay adults, self-rated health was the only significant determinant of QoL after adjusting for all the other variables. Marital status was significant only for the QoL of the older Chinese, and education was significant only for the QoL of older Indians.
Discussion
This article aimed to study the difference in QoL in a multiethnic metropolitan in Malaysia using CASP-19. The QoL of older people varied widely among different subgroups of the population, and it was influenced by factors such as perceived health status, ability to manage expenditure, marital status, and education. The CASP-19 score of 45.04 (95% CI [44.6, 45.5]) in this study is lower than that estimated by Abdul Mutalip et al. (2020) for Malaysia as a whole, at 47.01 (95% CI [46.3, 47.7]), but it is higher than that found in Ireland in 2011, with a mean score of 43.8 (95% CI [43.6, 44.1]) (Layte et al., 2013), and in England, with a mean score of 42.5 (95% CI [42.3, 42.7]) (Netuveli et al., 2006).
QoL did not vary significantly across age for those below 75 years old, but it was significantly lower for those aged 75 and over than those who were younger. This finding corroborates with ELSA (Wave 1) which found no difference in the CASP-19 between those aged 50–64 (with a mean score of 43.0) and 65–74 (with a mean score of 42.9), but a significant drop to 40 among those aged 75 and over (Netuveli et al., 2006). After controlling for self-rated health, ability to manage monthly expenditure, and other variables in the model, there is no significant decrement of QoL, even at an advanced age, contrary to the popular belief that QoL declines with age. This finding reaffirms past findings that concluded that older people could maintain high-quality fulfilling lives (Higgs et al., 2003; Layte et al., 2013). Laslett (1996) proposed that the Third Age is a stage of life free of earlier responsibility of work and family, and when one is still healthy enough to pursue life-satisfaction before the onset of deteriorating health such as hearing loss, cataracts, osteoarthritis, diabetes, depression, and dementia (Higgs et al., 2003). Only a few studies have examined the gender differential in QoL, which found no significant gender differential in QoL. The insignificant gender differential in the bivariate and multivariate analyses across all the three ethnic groups in this analysis corroborates the findings by Rafnsson et al. (2015) and Wiggins et al. (2004).
There were similarities and differences in factors affecting the QoL of the three main ethnic groups in Malaysia. Self-rated health has a significant effect on QoL for all the three ethnic groups, and the ability to manage expenditure was significant only among the Chinese and the Indians at the multivariate level. Current employment and co-residence with children had no effects for all. Three of the study variables had a positive effect on only one ethnic group. The Chinese who were currently married had higher QoL than those who were not married. Education and housing tenure were positively related to the QoL among the Indians.
Appropriate programs should be directed to assist the target groups to enhance the overall well-being of all citizens. Much emphasis has been placed on the role of the family in taking care of their aging parents, and co-residence with children is often assumed to be associated with a higher QoL. However, it is somewhat surprising that co-residence with children was not a significant predictor of QoL of older adults in Greater Kuala Lumpur. Past studies have also found that co-residence with children may or may not enhance the well-being of the older people. A study in China found that co-residence with children did not result in better psychological well-being for the elderly who were married, but it was beneficial for the widowed (Wang et al., 2014). Intergenerational conflict and lack of privacy may lower the psychological well-being of the older adults (Yang & Chandler, 1992; Zhou & Qian, 2008). As the effect of co-residence on the QoL of older adults remains inconclusive, more detailed studies, including the use of a qualitative approach, are needed to ascertain ways to enhance the benefits of co-residence.
Adapting to the aging process was found to be easier for those who are healthy and those who could manage their finance (Steverink et al., 2001). Deteriorating health and the onset of disability prevent one from active social participation, an activity which was found to forestall the decline in QoL (Roberts & Adams, 2018; Xie, 2018). QoL in old age was influenced by current contextual factors and life course events (Blane et al., 2004). Promoting healthy aging requires more efforts to improve the current health care system and provide long-term health care services that cater to the need of the older population. Efforts should also be made to develop community services and support for the aging population and provide better quality aged-care services to cope with the rising number of older people.
Conclusion
This study found that the CASP-19 is a good measure of QoL with a high reliability level for all three ethnic groups in the metropolitan area in Malaysia. The significant findings of this study are the discernible ethnic differentials in QoL and the predominant effects of perceived health status and ability to manage expenditure (as a proxy of financial well-being) on QoL in old age. Another interesting and important finding is that older adults can look forward to a long period of good QoL if they take care of their health and finance. As the findings of this study generally corroborate with past studies, policy interventions to improve the QoL of older people in Europe, North America, and elsewhere may be adopted or adapted in Malaysia.
This study sought to fill the lacuna in the knowledge of QoL of older Malaysians living in the metropolitan areas which may apply to other developing countries. As Malaysia is implementing and evaluating programs to enhance the QoL of older people, we hope that this analysis will provide some inputs for the formulation of the action plans and strategies by the relevant agencies and stakeholders to improve the well-being of the older adults. Differences in the effects of the various factors on the QoL of older people call for specific strategies and programs for different target groups.
The main limitation of this study is that it covers only a metropolitan area in Malaysia, and the findings may not be generalized for the national population. The analysis was based on the cross-sectional data from the first wave of a longitudinal survey. An analysis of changes in QoL over time can only be carried out after the second wave of the survey is conducted. Although the original English version of CASP-19 was administered to the English-speaking respondents, the translated version was administered to the non-English-speaking respondents. Efforts were made to ensure the accuracy of the translation into Bahasa Melayu, Mandarin, and Tamil languages. Most Malaysians with secondary education would have at least an intermediate level of proficiency in the English language as it is a compulsory subject. Moreover, English is widely used in daily life. Hence, the CASP-19 instrument would not be unfamiliar to the respondents.
Footnotes
Acknowledgements
The authors thank the MELoR research team for providing the data for this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Population Studies Unit (PSU), Faculty of Economics and Administration, University of Malaya (IF002-2014).
Ethical Statement
This study was approved by the University of Malaya Medical Centre Medical Ethics Committee (Ref: 925.4) and complied with the Helsinki Declaration of 1975, revised in 1983. Written informed consent was obtained from all the respondents.