
Abstract
Total laryngectomy (TL) is defined as a life-altering operation involving surgical removal of laryngeal structures. Quality of life levels of individuals with TL might be severely affected, therefore current study sought to examine these levels using validated tools in Turkish. The study design was comperative, correlational, and descriptive. Turkish versions of Self-Evaluation of Communication Experiences after Laryngectomy (TR-SECEL) and University of Washington Quality of Life Questionnaire (TR-UW-QOL) were administered online to 39 participants with TL (Meanage = 62.10, SD = 9.81). Participants were stratified into two or three groups according to age, education, alaryngeal communication method (ACM), and time after TL as scores of these groups were compared accordingly. Correlation between a number of variables and scores was examined. Regarding TR-SECEL, General domain scores were significantly higher in individuals with TL using tracheoesophageal speech (TES) compared to esophageal speech (ES), there was a positive and moderate relationship between age and General domain scores. Regarding TR-UW-QOL, Mood domain scores of individuals aged 60+ were significantly higher while Anxiety domain scores of individuals with nine or more years of education were significantly higher than the other groups. Appearance domain scores were higher in favor of individuals using TES as well as with a duration of 121 months and above following TL, while Shoulder domain scores were in favor of those with ES. As reported in previous studies, it does not seem plausible to state one specific ACM has priority over the other or it fulfills voice restoration in the long term without any complications.
Plain language summary
This study sought to examine the quality of life (QoL) levels of individuals with total laryngectomy (TL) by using two clinically validated tools that measure QoL: the Turkish versions of Self-Evaluation of Communication Experiences after Laryngectomy (TR-SECEL) and University of Washington Quality of Life Questionnaire (TR-UW-QOL). These tools were administered online to 39 participants with TL who were stratified into different groups according to the variables examined, such as age (40-59 & 60-82), education (one to eight years; nine years and above), alaryngeal communication methods (tracheoesophageal speech, TES; and esophageal speech, ES), and time after TL (eight-63, 64-120, 120 months and above). The findings related to TR-SECEL showed that there was no significant difference between age and education groups, the General domain scores were significantly higher among individuals with TL who used TES, the scores did not differ between three groups in terms of time after TL, there was a positive and moderate relationship between age and General domain scores. Regarding TR-UW-QOL,the Mood domain scores among individuals with TL aged 60 and over were significantly higher than other group, and those of Anxiety domain among participants with nine years of education or more were significantly higher than the other group, the mean scores of the Appearance and Shoulder domains were higher in favor of participants who used TES and ES, respectively. The Appearance domain scores among participants with a duration of 121 months and above after TL were significantly higher than the scores of the individuals in the range of eight-63 months following TL. As observed and reported in previous studies, it does not seem plausible to state that one specific alaryngeal communication method has priority over the other or it fulfills voice restoration in the long term without any complications.
Introduction
Laryngeal cancer is one of the most common types of head and neck cancer. In recent years, it is reported to be the only cancer that has shown a decrease in survival rates in the US (Siegel et al., 2016). In Türkiye, it ranks ninth within the most common cancer types especially among males with a prevalence rate of 1.7% (Kara & Keskinkılıç, 2021). Despite a recent shift toward laryngeal-preserving therapies in advanced laryngeal cancer (Wulff et al., 2021), total laryngectomy is still carried out in clinical practice.
Total laryngectomy (TL) is defined as a life-altering operation that involves the surgical removal of all laryngeal structures and part of the upper trachea. This surgery leads to the disconnection of the airway and a permanent breathing hole (tracheostoma/stoma) in the neck (Chotipanich, 2021). Following this operation, a number of problems including the loss of nasal function, weakening of coughing ability, difficulty in swallowing, and restriction in tongue movements may be observed as well as those related to the individual’s voice (Kazi et al., 2010; Wulff et al., 2021). The voice restoration methods offered following TL include esophageal speech, electrolarynx, and tracheoesophageal speech. The final decision on which method to be used depends entirely on the individual with TL. Esophageal speech (ES) refers to the alternating vibration sounds produced by the release of air into the esophagus. Electrolarynx is defined as a medical device that mechanically generates sound signals transmitted from the lower jaw or cheek to the oral cavity. Tracheoesophageal speech (TES) is achieved by placing a prosthesis with a one-way valve function into an artificial fistula formed between the trachea and esophagus on the posterior wall of the trachea (Doi et al., 2011). A recent meta-analysis (Maniaci et al., 2024) suggested that both TES and ES were effective methods for voice rehabilitation after TL. It also reported higher levels of voice-related quality of life for individuals using TES despite a significant heterogeneity and moderate inconsistency within the studies included in the meta-analysis. Although each method has its own advantages and disadvantages (Maniaci et al., 2024; Tang et al., 2023), it is crucial that the method is delivered quickly and effectively, which might in turn affect the quality of life of the individual.
Quality of life (QoL) is defined as a multidimensional construct which is rooted in the behavioral sciences, particularly in social psychology and sociology (Relic et al., 2001). The QoL is unique to the individual, and includes positive and/or negative self-reports about the individual’s life. It is reported to affect the physical and economic conditions as well as the psychological state of the individual (Koller et al., 1996). In the case of individuals with laryngeal cancer and TL, the physiological functions might be affected and altered, including breathing, deglutition, and speaking. However, as reported by Relic et al. (2001), coming to terms with TL is mostly a social phenomenon. This means the effect of TL extends far beyond the physiological consequences, encapsulating a number of repercussions on the emotional, social, and professional environment of the individual with TL. To exemplify, the individuals with TL need time to adapt to their “new” voice. Regardless of the alaryngeal communication method in use, individuals with TL report difficulty in identifying with their voice, getting their message across to their communication partners, speaking in noisy environments, and being spontaneous during communication (Tang et al., 2023). To fully comprehend these problems, Babin and Grandazzi (2014) emphasize that the knowledge related to these individuals’ social environment is essential as the individuals live in a familial, social, and economic context. These authors call for a multidisciplinary approach toward patient care to address the psychosocial dimensions, suggesting the need of collaboration between medical sociologists and physicians in transforming patient care (Babin & Grandazzi, 2014).
All of these reports necessitate examining the QoL levels of individuals with TL through psychometrically validated measurement tools, which is the widely accepted way to document the psychosocial adaptation of individuals with TL (Souza et al., 2020; Wulff et al., 2022). These tools include Self-Evaluation of Communication Experiences after Laryngectomy (SECEL; Blood, 1993), The University of Washington Quality of Life Questionnaire (UW-QOL; Hassan & Weymuller, 1993), Functional Assessment of Cancer Therapy Head-Neck (FACT-H&N; List et al., 1996), European Organization for the Research and Treatment of Cancer, Quality of Life Scale (EORTC QLQ H&N35; Fayers et al., 2001), Short Form-36 (Ware & Sherbourne, 1992), and Voice-Related Quality of Life (V-RQOL; Hogikyan & Sethuraman, 1999). Despite the fact that these tools have their own strengths and weaknesses, they are psychometrically validated, easy to fill in, and suitable for use in the clinical and research contexts. On the other hand, SECEL stands out with its communication-specific items as it was formed to evaluate communication experiences following laryngectomy and adaptation to the new voice in daily life (Blood, 1993). In addition, the UW-QOL is considered to be advantageous in terms of being comprehensive and including 12 different domains that assess the QoL specific to head and neck cancer (Hassan & Weymuller, 1993).
Previous studies using SECEL and UW-QOL examined the QoL levels according to age, education, alaryngeal communication method (ACM), and time after TL to elaborate on the need for improving the QoL levels of these individuals by taking such variables into consideration. More specifically, these studies reported older individuals held better QoL levels (Eadie & Bowker, 2012; Kazi et al., 2007; Vilaseca et al., 2006) while other studies did not report any difference among age groups in relation to these levels (Souza et al., 2020; Uzuner, 2021; Williamson et al., 2011). Similarly, the education did not have any effect on these levels (Souza et al., 2020; Uzuner, 2021). As for the ACM, the individuals using ES reported more problems related to communication experiences in certain environments or situations than those with TES (Rodrigues et al., 2023; Uzuner, 2021) while this difference was not reported, independent of any ACMs in use including electrolarynx (Mesolella et al., 2023). Regarding time after TL, there was variability in the values of duration (e.g., two, five, less or more than ten years), but studies indicated higher QoL in the case of increasing duration (Souza et al., 2020; Vilaseca et al., 2006) or reported no such differences (Uzuner, 2021; Williamson et al., 2011).
These variables help researchers and clinicians identify the psychological, social, and functional outcomes related to QoL which plays a crucial role in the selection of primary intervention modality in laryngeal cancer as well as ensuring the overall well-being of individuals with TL (Maniaci et al., 2024; Rossi et al., 2014; Wulff et al., 2021). Aligned with this rationale, current study aims to examine the QoL levels of Turkish-speaking individuals with TL by using the Turkish versions of SECEL and UW-QOL (hereafter, TR-SECEL and TR-UW-QOL; Senkal et al., 2012; Uzuner, 2021). The nature of current study is exploratory in that there is a lack of previous studies that examine communication-related problems that challenge the QoL of these individuals in the Turkish context, except the Turkish adaptation study of SECEL (Uzuner, 2021). Moreover, the identification of QoL levels could influence the selection and maintenance of the ACM to be offered after TL. Taking all these statements into account, current study seeks to answer the following questions:
(1) Do TR-SECEL and TR-UW-QOL scores differ among individuals with TL stratified into groups according to age, education, ACM, and time after TL?
(2) Is there a relationship between the scores of TR-SECEL and TR-UW-QOL and variables including age, education, and time after TL?
Material and Methods
Participants
This study was designed as a comparative, correlational, and descriptive study. The dependent variables included the scores of the Turkish versions of Self-Evaluation of Communication Experiences after Laryngectomy (TR-SECEL; Uzuner, 2021) and the University of Washington Quality of Life Questionnaire (TR-UW-QOL; Senkal et al., 2012), while the independent ones included age, education, alaryngeal communication method (ACM), and time since total laryngectomy (TL). Before data collection, ethical approval was obtained from Ankara Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital.
A total of 39 individuals with TL participated in the study. The inclusion criteria were as follows: (i) having undergone TL surgery, (ii) actively using one of the ACMs including tracheoesophageal speech (TES), esophageal speech (ES) or electrolarynx following TL, (iii) using the ACM for at least 6 months at the time of administering the TR-SECEL and TR-UW-QOL, (iv) speaking Turkish as their native language, (v) having received at least one or more years of education.
Data were collected online by using Google Forms to minimize physical contact due to the COVID-19 pandemic between September 2022 and May 2023. The first author gathered the data from Ankara Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital that provided voice rehabilitation almost exclusively to individuals with TL. For this reason, the participants of the study were those who were or had been treated at Ankara Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital.
As the ethical permission was granted from the Hospital where these participants received intervention, the first author was given permission to contact potential participants. These participants were either patients receiving voice therapy from the first researcher or who had received voice intervention previously. Those who were considered to meet the inclusion criteria were contacted via telephone or teleconference application called Zoom™. Then, the researcher shared the Google Forms link of the study with these participants who agreed to participate in the study. In order to prevent any confusion that may occur during the participation, the researcher was available for the participants and responded to any questions they might have about the items in the tools during the Zoom meeting or telephone conversation with them. In the settings of Google Forms, single response from each participant was ensured by activating the feature of “Limit to 1 response.”
On the first page of the Google Forms link, the participants who met the inclusion criteria were given detailed information about the study. The participants gave informed consent by checking the box at the end of this page. Subsequently, they were asked to provide demographic information (age, gender, date of birth, education level, employment status, marital status) as well as pertinent information about the total laryngectomy (the ACM used, time after TL, and whether they received adjuvant intervention). The questions were in the following: (a) What is your age?, (b) What is your sex?, (c) What is your date of birth?, (d) What is your educational status?, (e) What is your employment status?, (f) What is your marital status?, (g) What is the alaryngeal communication method that you use?, (h) What is the duration after TL?, (i) Did you receive any adjuvant intervention such as chemotherapy and/or radiotherapy?, (j) (In case of receiving radiotherapy before) Did you receive radiotherapy prior to or after the TL? Most of these questions were the same as those asked at the first page of the TR-SECEL form (Uzuner, 2021), while the questions titled (h), (i), and (j) were added by the authors of the current study. As the participants filled in these questions, they moved on to filling in the items that belonged to TR-SECEL and TR-UW-QOL. Information regarding these two measurement tools was given in the following.
Instruments
TR-SECEL
It consists of 35 items divided into three domains: General, Environment and Attitude. It is a self-report scale, therefore the individual with TL is expected to rate the items mentioned in the scale according to the time of administration or in the last 30 days prior to the time. The first 34 items are rated on a scale of 0 to 3 (0 = never; 1 = sometimes; 2 = often; 3 = always). The total scores corresponding to the responses to each item range from 0 to 102. The higher the score on the TR-SECEL, the more difficulty the individual has with regards to adapting to the voice (or vice versa in the case of a lower score). During the scoring of three domains the following procedures are considered: (a) The first five items belong to the General domain where reverse scoring is carried out (i.e., 3 for 0, 2 for 1, 1 for 2, and 0 for 3). The higher the individual’s score in this domain, the more problems they have with the overall adaptation to their communication experiences. (b) The 14 items (numbered between 6 and 19) correspond to the Environment domain. The score that can be obtained from this domain ranges from 0 to 42 (14 × 3). Higher scores may signify more distress the individual with TL may experience within certain environments or situations. (c) The remaining 15 items (numbered between 20 and 34) correspond to the Attitude domain. The score that can be received from this domain is in the range of 0–45 (15 × 3). Higher scores may reflect the difficulties the individual with TL may experience with their social environment and its attitudes. A total score of 36 or less indicates that the individual shows adequate adaptation to the process after TL while a total score of 60 and above indicates the opposite. This demonstrates that the individual needs to receive additional support regarding how to cope with communication experiences following TL as documented by the items of TR-SECEL (Uzuner, 2021).
The validity and reliability analyses were conducted by Uzuner (2021). The validity analyses included content, criterion, and construct validity as well as correlation between domain and total scores; while the reliability analyses involved the examination of internal consistency and test-retest reliability. The findings of validity analyses showed that (a) the content validity index scores of all the items of TR-SECEL were above .80; (b) a statistically significant correlation was observed between TR-SECEL and Turkish version of Voice-Related Quality of Life (TR-VRQL; Tezcaner & Aksoy, 2017) as well as European Organization for the Research and Treatment of Cancer, Quality of Life (EORTC QLQ H&N35; Fayers et al., 2001); (c) a three-factor structure was explored in TR-SECEL in which a significant correlation was obtained between domain and total scores. Regarding reliability analyses, (a) the Cronbach’s alpha value of the TR-SECEL was .95, (b) a statistically significant correlation was observed between the scores of TR-SECEL as the scale was filled out by a number of participants for the second time after 1 week. As reported by Uzuner (2021), these findings show that TR-SECEL is a valid and reliable assessment tool both for clinical and research purposes.
TR-UW-QOL
It consists of 12 domains: Pain, appearance, activity, recreation, swallowing, chewing, speech, shoulder, taste, saliva, mood, and anxiety. These domains have three, four, or five response options. The most negative response is scored as 0, while the opposite is as 100: The domains with three response options are scored as 0–50–100, four options are as 0–33–67–100, five options are as 0–25–50–75–100. A composite score is calculated by considering all the scores derived from these domains. A higher score corresponds to a better level of quality of life (QoL). In addition, individuals respond to three global questions. The first one asks the individual to rate their health-related to QoL before cancer while the second asks the individual to rate their health-related QoL in the last 7 days at the time of administration. The last one asks the individual to rate their general QoL in the last 7 days at the time of administration. These three questions are not included in the calculation of the composite score but can be analyzed on their own. The composite score is not calculated when the individual does not respond to two or more domains (Senkal et al., 2012).
The validity and reliability analyses were conducted by Senkal et al. (2012). The validity analyses included content and construct validity; while the reliability analyses involved the examination of internal consistency and test-retest reliability. The findings of validity analyses showed that (a) content validity of TR-UW-QOL was ensured through the translation process in a qualitative way as well as the rigorous process of forward and backward translation; (b) significant correlation was obtained between the composite score of TR-UW-QOL and EORTC QLQ-C30 (Fayers et al., 2001) as well as global scores of TR-UW-QOL. As for reliability analyses, (a) the Cronbach’s alpha value of the TR-UW-QOL was .757, (b) the interclass correlation coefficient value was .941, which was obtained as a result of administering the tool for the second time following a 10-day interval. As reported by Senkal et al. (2012), these findings show that TR-UW-QOL is a valid and reliable assessment tool both for clinical and research purposes.
Data Analysis
The participants were stratified into two age (40–59 and 60–82) and education (1–8 years and 9 years and above) groups, and three groups according to the time after total laryngectomy (8–63, 64–120, and 121 months and above) which was in accordance with the methodological considerations of previous studies mentioned in the introduction section (i.e., Uzuner, 2021).
IBM SPSS 26 was used in data analysis. The independent sample t-test was used to identify whether there was a difference between the age, education and ACM groups. There was only one electrolarynx user that took part in the study, therefore the ACM group included those using TES and ES. Since there were three different groups for the time after TL (8–63 months; 64–120 months; 121 and more months), one-way analysis of variance test was used. Bonferroni was selected for the post-hoc because it did not require equal number of samples during group comparisons (Field, 2018). Pearson’s product-moment correlation coefficient was calculated to examine whether there was a correlation between the scores and variables including age, education, and time after TL. An alpha level of .05 for all the analyses was used with a confidence interval of 95%.
Results
In the process of data compilation; the data were collected through the Google Forms. A spreadsheet including the responses of the participants were formed. The responses were converted to numerical values in accordance with the scoring guidelines of the measurement tools reported in the previous section. The responses were complete, namely, there were no incomplete values in the dataset. Numerical values were also assigned to participants according to the groups of age, education, alaryngeal communication method (ACM), and time after total laryngectomy (TL). These values were transferred to IBM SPSS 26 to conduct statistical analyses including the normality distribution.
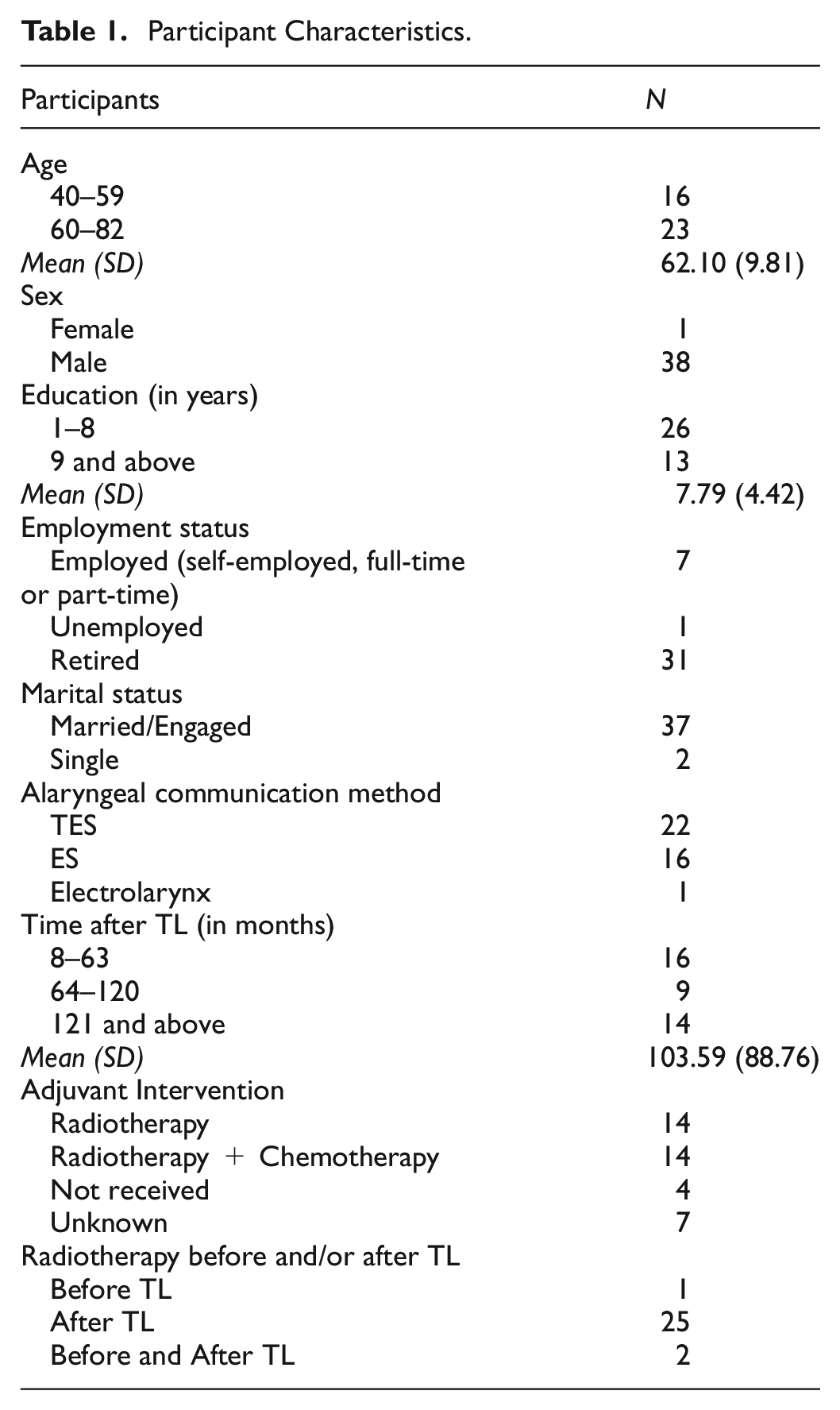
In the following, the skewness and kurtosis coefficients were analyzed to identify whether the data showed normal distribution. The skewness coefficient values of the total TR-SECEL and TR-UW-QOL scores were .939 and -.588, respectively. The kurtosis coefficient values of the total TR-SECEL and TR-UW-QOL scores were .861 and −.179, respectively. As these values were between −1 and +1, it was concluded that the data showed normal distribution. The participant characteristics were presented in Table 1.
Participant Characteristics.
The analyses showed the following: A significant difference was observed between age groups only in the mood domain of TR-UW-QOL. More specifically, the mood domain scores of individuals with TL who were 60 and above were significantly higher than those obtained from the younger group (Mood domain, t(37) = −3.018, p = .005). The remaining domain scores of TR-SECEL and TR-UW-QOL did not exhibit any statistical significance in terms of the age (p > .05; Table 2).
Descriptive Statistics and Independent Sample t-Test Results of TR-SECEL and TR-UW-QOL Scores According to Age Groups.

p < .01.
A significant difference was observed between the education groups only in the anxiety domain of the TR-UW-QOL. The group where individuals with TL received nine or more years of education scored significantly higher in this domain compared to one that received less years of education (Anxiety domain, t(37) = −2.065, p = .046). The remaining domain scores of TR-SECEL and TR-UW-QOL did not exhibit any statistical significance in terms of the education (p > .05; Table 3).
Descriptive Statistics and Independent Sample t-Test Results of TR-SECEL and TR-UW-QOL Scores According to Education Groups.

p < .05.
Considering the ACM and TR-SECEL, the general domain scores of individuals with tracheoesophageal speech (TES) scored significantly higher than those with esophageal speech (ES) (t(36) = 3.929, p < .001). Moreover, a significant difference was observed in the appearance and shoulder domain scores of TR-UW-QOL between the groups of individuals with TES and ES. In the appearance domain, the scores of individuals using TES were significantly higher than those using ES (t(36) = 3.467, p = .001). Conversely, in the shoulder domain, the scores of individuals using ES were significantly higher than those using TES (t(36) = −2.620, p = .013). The remaining domain scores of TR-SECEL and TR-UW-QOL did not exhibit any statistical significance in terms of the ACM (p > .05; Table 4).
Descriptive Statistics and Independent Sample t-Test Results of TR-SECEL and TR-UW-QOL Scores According to Groups Using TES and ES (Two ACMs).
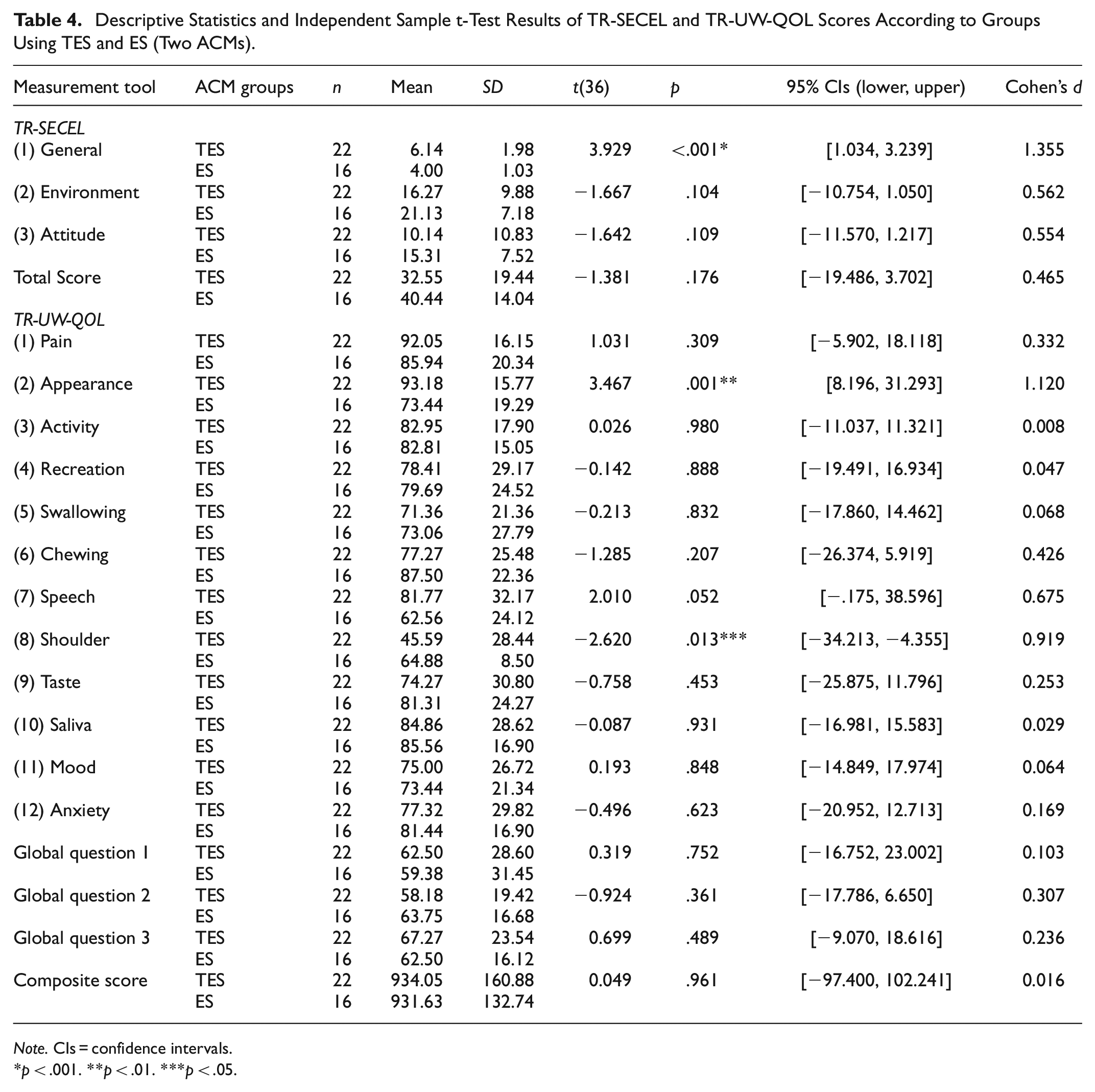
Note. CIs = confidence intervals.
p < .001. **p < .01. ***p < .05.
Considering the time after TL and post-hoc analysis, there was a significant difference in the appearance domain scores of two groups (one with a duration of 8–63 months, and the other with a duration of 121 months and above). More specifically, the scores of participants with a post-TL duration of 121 months and above were significantly higher than those of the other group (F(2-36) = 4.458, p = .019). The remaining domain scores of TR-SECEL and TR-UW-QOL did not exhibit any statistical significance in terms of the time after TL (p > .05; Table 5).
Descriptive Statistics and One-Way ANOVA Results of TR-SECEL and TR-UW-QOL Scores According to the Time After TL.

p < .05.
There was a positive and moderate correlation between the age and the general domain scores of TR-SECEL (r = .403, p = .011; Table 6).
Correlation Analysis of TR-SECEL and TR-UW-QOL Scores With Age, Education and Time After TL Variables.

p < .05.
Discussion
Current study contributed to previous literature by identifying the quality of life (QoL) levels of Turkish-speaking individuals with total laryngectomy (TL), using validated measurement tools and considering a number of variables reported to affect these QoL levels (i.e., age, education, alaryngeal communication method (ACM), and time after TL). The QoL is a multidimensional construct involving physical, psychological, financial, and social well-being. In the case of TL, the structures that are vital for speech and swallowing are affected, thus having a negative impact on the psychosocial adaptation of the individual with TL and consequently on their QoL levels (Saltürk et al., 2016; Tang et al., 2023).
Regarding age, current study only reported that those over 60 had a higher QoL levels in the mood domain of TR-UW-QOL compared to those below 60. Taking into account both of the measurement tools (except the mood domain), the findings are in line with those of Uzuner (2021), Souza et al. (2020), and Williamson et al. (2011). Unlike these studies; Eadie and Bowker (2012) reported a significant, albeit weak, relationship between age and composite UW-QOL scores, stating that older individuals had higher QoL levels. Similarly, Kazi et al. (2007) revealed that the mean composite score of UW-QOL among individuals whose age was above the median (66–84 years) was significantly higher than the score of those whose age was below the median. These authors stated that this significant difference was observed in the domains of shoulder, recreation, and speech (Kazi et al., 2007). Using UW-QOL, Vilaseca et al. (2006) reported that age was a predictor of the scores derived from the domains of appearance and anxiety, demonstrating that younger individuals with TL might have experienced more dissatisfaction related to these two domains. This might be the case for the younger participants of current study in terms of mood.
In the similar vein, there was no significant difference between the TR-SECEL and TR-UW-QOL scores of the two education groups (except the anxiety domain of the latter tool), which is in line with Uzuner (2021) and Souza et al. (2020). In the current study, the mean score of the individuals with nine or more years of education in the anxiety domain was significantly higher than that of the other group. Therefore, it can be concluded that those with nine or more years of education have a higher QoL in terms of the anxiety domain.
Considering the ACM, the scores of those using tracheoesophageal speech (TES) and esophageal speech (ES) were compared. The findings related to TR-SECEL revealed that the general domain scores of individuals with TES were significantly higher than those of the individuals with ES. On the other hand, the total TR-SECEL scores were higher among individuals using ES compared to TES despite being statistically non-significant. Similarly, the mean scores of environment and attitude domains did not show a significant difference among individuals using these two ACMs. This does not align with the finding of Uzuner (2021) in which they revealed that the mean scores of the environment and attitude domain scores of individuals with ES were higher than those of TES. However, it is important to note that Uzuner (2021) involved individuals undergoing partial laryngectomy (PL) as well as TL, and they reported that the total, environment and attitude domain scores of individuals with TL were significantly higher than those of the individuals undergoing other types of surgery (including PL, PL and unilateral neck dissection, and PL and bilateral neck dissection). Considering previous literature using other language versions of SECEL, Rodrigues et al. (2023) stated that the total score of individuals with ES was significantly higher than those of the individuals with other ACMs, also revealing that those with ES needed significantly more support as regards the environment domain. Also, Mesolella et al. (2023) revealed no statistically significant difference between the mean scores of individuals with different ACMs. On the other hand, Da Silva et al. (2015) showed that the environment and attitude domain scores were significantly higher among individuals who did not use any ACMs despite the fact that these scores were compared in terms of whether voice rehabilitation was received or not. Therefore, the SECEL scores pertaining to individuals with TES and ES were limited to descriptive statistics. Da Silva et al. (2015) stated that the use of ES did not require any use of prosthesis or device and therefore resulted in exemption from any economic and maintenance costs. For this reason, these authors argued that ES could be considered as a first option before TES or electrolarynx (Da Silva et al., 2015).
Considering ACM and TR-UW-QOL, the appearance domain scores of individuals using TES were significantly higher than those using ES; and the shoulder domain scores of individuals using ES were significantly higher than those using TES. In light of previous studies, Souza et al. (2020) showed that individuals with TES scored significantly higher in the speech domain compared to those using ES and electrolarynx. According to these authors, this finding indicated that TES provided more satisfaction related to speech than other ACMs. Indeed, in our study, the individuals with TES received higher scores in the speech domain than those with ES. However, the difference was not statistically significant. In relation to the appearance, Eadie and Bowker (2012) used additional measurement tools other than the UW-QOL, reporting that 42% of the individuals named the limitations in physical abilities, appearance and lifestyle due to cancer as the most stress-inducing experiences associated with TL. Furthermore, Vilaseca et al. (2006) observed no statistically significant difference in the speech domain regardless of whether the individual with TL used TES or not. This finding is in line with the one of the current study. However, these authors also reported that individuals with TES experienced less pain, adding that their scores were significantly higher in the shoulder and saliva domains. In the study by Vilaseca et al. (2006), 31 of the 49 participants used TES, nine used electrolarynx, and seven used ES. Ten individuals in the study were reported to regularly use more than one ACM (Vilaseca et al., 2006). Considering this point, in our study, it was seen that individuals using ES exhibited significantly higher scores in the shoulder domain. However, current study compared the scores of two ACM groups (TES and ES), which differed from the Vilaseca et al.’s (2006) study in this realm. In this context, it can be thought that individuals with ES may have more concerns about their appearance than those with TES.
There is still no clear framework as to which of the ACMs should be prioritized in the process of voice restoration following TL. The current study showed that there was no significant difference between the groups using TES and ES as far as many domain scores were concerned. The exceptions were that (a) individuals with TES needed more support related to the general domain of TR-SECEL, (b) individuals with ES had more difficulties related to the appearance domain but reported a higher QoL compared to those with TES in the shoulder domain of TR-UW-QOL. Indeed, previous literature favors the adoption of TES; however, it is criticized due to the potential long-term complications of TES (Tang et al., 2023). Also, Saltürk et al. (2016) reported the findings of Voice Handicap Index (VHI; Kiliç et al., 2008) and Perceived Stress Scale (PSS; Eskin et al., 2013) applied to Turkish-speaking individuals with TL using three ACMs (TES, ES, and electrolarynx). The findings showed that the mean scores of VHI and PSS among individuals with ES were significantly lower than those that pertained to the other two ACM groups. Based on these findings, Saltürk et al. (2016) associated lower scores of VHI among individuals with ES with a better level of QoL. In addition, with reference to PSS scores, these authors stated that individuals with ES may experience less stress and hold a better perception of their voice as these individuals did not need any prosthesis or device and was therefore exempt from its financial burden (Saltürk et al., 2016).
The final variable examined as part of the first research question was the time after TL. In light of the scores, a significant difference was observed only in the appearance domain of the TR-UW-QOL which was in favor of the individuals with a post-TL duration of 121 months or more. This finding aligns with Souza et al. (2020) and Vilaseca et al. (2006). The former study reported that participants undergoing TL for more than 2 years had significantly higher scores in the speech domain compared to those with a duration of less than 2 years, while the latter one indicated that individuals undergoing TL for more than 5 years had higher scores in the activity and anxiety domains. On the other hand, Williamson et al. (2011) reported no significant difference between the two groups who were divided according to the median value of 18.5 months following TL. Also, the finding related to TR-SECEL is not in line with the one by Rodrigues et al. (2023) who reported a significant and reverse correlation between the time following diagnosis and total score of SECEL. Also, an increase in time since diagnosis was associated with a higher perceived voice function. Similarly, an increase in time was associated with needing less support in the environment domain (Rodrigues et al., 2023). Considering previous literature, the strength of our study is that individuals with TL need to be informed of potential problems related to the appearance that could emerge in the first 5 years following the surgery, ideally during the pre-operative counseling to be offered prior to the operation.
Regarding the second research question, the findings showed that there was a positive and moderate correlation between the age and general domain scores of TR-SECEL. Eadie and Bowker (2012) reported a significant but weak relationship between age and composite scores of UW-QOL. On the other hand, Rodrigues et al. (2023) revealed no correlation between age at diagnosis and domain-total scores of SECEL as well as a lack of correlation between the age at which SECEL was filled and the domain-total scores of SECEL. The increase in the general domain score of TR-SECEL together with an increase in age may indicate that more support is needed in this domain along with aging, which needs to be considered by the health professionals including speech-language pathologists in the voice rehabilitation process.
Limitations and Recommendations
This study has some limitations: (a) The study consisted of 39 individuals with total laryngectomy (TL). A larger sample size may be needed to understand the effect of demographic variables and alaryngeal communication methods (ACM) on the quality of life (QoL) in the voice rehabilitation process of individuals with TL. (b) Since only one of the individuals used electrolarynx, a comparison was made between the scores of individuals using tracheoesophageal speech and esophageal speech (ES). (c) Similarly, only one of the participants was female, therefore no analysis was conducted in relation to the sex. (d) The responses were based on the self-reports of the individuals, and the measurement tools were administered online. (e) In addition, the analyses carried out did not allow more than two variables to be correlated as shown by the findings. Considering these limitations, future studies should include more number of participants as well as those who are female and use electrolarynx. Moreover, the adoption of qualitative methodology is suggested to examine in depth the views and communication experiences of individuals with TL related to QoL.
Tracheoesophageal speech (TES), ES, and electrolarynx are among the options for ACM. Tang et al. (2023) present both the advantages and disadvantages of each of these three ACMs, stating that the use of TES in particular is much more prominent in the literature and is presented as the “gold standard.” However, as observed and reported in previous studies, it does not seem plausible to state that one specific ACM has priority over the other or it fulfills voice restoration in the long term without any complications. In addition to voice restoration, adequate pulmonary and olfactory rehabilitation is also pivotal for individuals with TL. Biofilm formation on voice prostheses is still a major problem, which limits the durability of these prostheses. Therefore, it is necessary to promote the use of ES in conjunction with TES, and to provide pre-operative speech and language pathology counseling prior to TL. This counseling plays integral roles in the comprehensive care of individuals undergoing TL, helping individuals navigate the challenges of adapting to a new way of communication and coping with emotional responses (Longobardi et al., 2023).
Conclusions
The quality of life (QoL) of individuals undergoing total laryngectomy (TL) is a multifaceted construct influenced by various factors including age, educational level, alaryngeal communication method (ACM), and time after TL. Age may impact one’s adaptability to post-operative changes as evidenced in the general and mood domain scores of the TR-SECEL and TR-UW-QOL. Higher education levels could potentially affect the anxiety levels of the individuals as shown by TR-UW-QOL. The choice of the ACM plays a crucial role, as it might influence a number of domains (including appearance, shoulder, etc.) depending on the type of ACM. Regarding appearance, the self-reports of individuals undergoing TL for more than 10 years were more positive than those with a duration of 8 to 63 months. Consequently, the QoL levels of individuals with TL are dynamic and intricate, which highlights the importance of personalized interventions and support to optimize their well-being and adaptation to the changes caused by the surgery.
Footnotes
Acknowledgements
The authors thank the participants for their involvement in the study. The first author completed this study under the supervision of the second author as part of the MSc degree in Speech and Language Therapy at Istanbul Atlas University, Turkey. This study was presented as an oral presentation in the 13th National Laryngology Congress between 27 and 28 September 2024 in Samsun, Turkey.
Ethical Considerations
The approval for the study was granted by the Non-Interventional Clinical Research Ethics Committee of Ankara Dr. Abdurrahman Yurtaslan Ankara Oncology Training and Research Hospital (Date: 25.08.2022, No: 2022-08/84).
Author Contributions
Gülsün Adsiz (Conception and design of the study, acquisition of the data, drafting the manuscript, figure and tables), Şevket Özdemir (Conception and design of the study, analysis and interpretation of the data, revising it critically for important intellectual content, supervision), Bayram Barış Büyük (Drafting the manuscript, figure and tables, revising it critically for important intellectual content). All authors reviewed the manuscript and approved it for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data are available upon request.
Declaration of Generative AI and AI-Assisted Technologies
During the preparation of this work, the authors did not use any generative AI and AI-assisted technologies in the writing process.