
Abstract
Literature suggests that laughter interventions can positively influence psychological well-being and quality of life (QoL) in various populations, yet their efficacy among cancer patients remains underexplored. This mini systematic review aims to examine the cross-sectional associations between laughter/humor interventions and psychological wellbeing/Quality of life and synthesize the latest quantitative evidence regarding the effects of laughter interventions on the psychological wellbeing/Quality of life of cancer patients as well as the longitudinal relationships between interventions and outcome. A comprehensive search was conducted across electronic databases to identify relevant studies published from 2011 until 2022. Eligible studies were those examining the impact of laughter interventions on psychological well-being and Quality of Life in cancer patients. Five studies met the inclusion criteria and were included in the review. The findings indicate significant improvements in various psychological parameters following laughter interventions among cancer patients, including stress, depression, anxiety, overall Health Related Quality of Life (HRQoL), emotional well-being, Global Health Status & QoL, mental well-being, and positive mood. Moreover, the review highlights the synergistic effects of laughter when combined with other therapeutic elements. However, it was noted that laughter therapy did not demonstrate significant efficacy for moderate to severe depression among cancer patients. Longitudinal effects of laughter interventions on psychological well-being and QoL remain inconclusive. This systematic review underscores the beneficial effects of laughter interventions on the psychological well-being and QoL of cancer patients. It suggests the potential for multidisciplinary approaches, led by Health Psychology Practitioners, to develop and implement tailored laughter therapy programs for this population. Further research is warranted to elucidate the longitudinal effects and optimal delivery methods of laughter interventions in the context of cancer care.
Plain Language Summary
Literature suggests that laughter interventions can positively influence psychological well-being and quality of life (QoL) in various populations, yet their efficacy among cancer patients remains underexplored. This mini systematic review aims to examine the cross-sectional associations between laughter/humor interventions and psychological wellbeing/Quality of life and synthesize the latest quantitative evidence regarding the effects of laughter interventions on the psychological wellbeing/Quality of life of cancer patients as well as the longitudinal relationships between interventions and outcome.
Keywords
Introduction
Plato, Aristotle, Kant, Descartes and Darwin are among the philosophers who spoke about the significant role of laughter in our lives (Paddington, 1963). In 400 AD, Miletus explained that the Greek word for laugher is “gelos” and its root is “hele” which means “health.” Diverse theories have approached laughter from different angles aiming to explain the mechanisms behind its effect on human behavior. The psychoanalytic theory on humor (Freud, 1928) suggested that laughter is a factor with a positive effect on the negative emotional behaviors. Positive Psychology aims to shift the focus from repairing the pathological ill health toward working for a better life while or after illness by inheriting a positive attitude (M. E. P. Seligman, 2002; M. E. Seligman et al., 2005). Hence, positive feelings may improve the physical, psychological and emotional well-being among patients with long-term conditions (LTCs). The behavioral imitation of simple and intentional positive activities practiced on a regular basis such as simulated laughter and counting blessings is a common technique applied in positive psychology interventions (Cohn & Fredrickson, 2010; Lyubomirsky & Layous, 2013).
Laughter can be spontaneous, simulated, stimulated, induced or pathological (Yim, 2016). Simulated laughter is self-induced while stimulated is induced by external humorous stimuli. Literature is rich in simulated and stimulated laughter interventions among both healthy individuals (Bennett et al., 2003; Bennett & Lengacher, 2006) as well as among patients with dementia (Takeda et al., 2010), depression (Ko & Youn, 2011) and diabetes (Bains et al., 2015). Improvement in quality of life (Cha & Hong, 2015; Ko & Youn, 2011) and stress levels is also evidenced. Research evidence suggests that laughter interventions had a significant beneficiary effect on patients’ mood and stress (Choi et al., 2010) QoL (Cho & Oh, 2011), anxiety (Han et al., 2011; You & Choi, 2012) among adults with cancer.
Laughter research is limited in cancer patients (Joshua et al., 2005) and most evidence comes from quantitative studies using self-reported measure outcomes. Thus, existing reviews have assessed latest studies from within the last decade among diverse population groups (Gonot-Schoupinsky & Garip, 2018; van der Wal & Kok, 2019). No laughter interventions reviews among cancer patients were found; a research gap that could be attributed to the limited existing literature on this population group.
This review gap in existing literature along with a personal painful experience following the loss of a close family member from lung cancer guided the reviewer`s interest on cancer patients. The reviewer suggests that there is a potential for health psychologists to design and implement simple laughter interventions that will be safe, low-cost and convenient (Hatzipapas et al., 2017; Zhao et al., 2019).
The impact of laughter may be of utmost significance for patients, services and the community while it may contribute to the patient-practitioner relationship (World Health Organization [WHO], 2021; Zhao et al., 2019). Existing literature reports no argument or controversy on the significance of laughter effect either on individuals. The need for improving and maintaining a positive psychological well-being and QoL is a common issue especially for patients with cancer; one of the most lethal health conditions in our modern world. This work summarized the latest quantitative laughter interventions and their effect on the psychological well-being/QoL in cancer patients. Due to limited resources (time restrictions) the author considered the mini review format compared to a more extended work. Thus, this paper is characterized by a limited time frame research and scope (Griffiths, 2002).
The findings of this mini systematic review will set the basis for formulating the intervention research question of a forthcoming laughter intervention that will be conducted by the reviewer. “What is the effect of laughter intervention on psychological wellbeing/QoL in patients with cancer?” is the research question. The main objective was to examine the cross-sectional associations between laughter/humor interventions and psychological wellbeing/QoL. The secondary objective was to examine the longitudinal relationships between interventions and outcome. The hypothesis was that the laughter interventions will be associated with greater psychological wellbeing and QoL in cancer patients.
Methods
A review protocol was developed to serve as a guide throughout the review process. The reviewer abided on this protocol which along with the inclusion/exclusion criteria allowed for the elimination of bias. A detailed briefing of all the included elements of the review protocol is presented in Table 1.
Review Protocol.

The research question was formed following the PICO frame (Higgins & Green, 2008) which was developed aiming to facilitate the formulation of highly feasible and answerable clinical research questions based on the Problem/Population, Intervention, Comparison and Outcome (Huang et al., 2006). The search strategy involved an electronic advanced search EBSCO PsychINFO and PsychArticles databases aiming to identify all quantitative laughter interventions delivered in any setting (hospital, institution, privately) and delivery mode (online, in-person) among adults with no upper age limit worldwide with any type and at any stage of cancer. All peer-reviewed, full texts in English published between 2011 and 2021 were considered for inclusion aiming to evaluate studies applying the latest quantitative methods (Table 2).
Detailed search criteria and keywords to be applied*.

All quantitative studies examining the effect of laughter on the psychological well-being/QoL in cancer patients were included and assessed for eligibility. Studies among adult populations with no upper age limit were considered as eligible aiming to capture a wider lifetime period of cancer patients. Qualitative studies and systematic reviews were excluded aiming to evaluate studies applying objective methodology. Anecdotal and case-studies were also excluded in order to focus on those with higher generalizability. The Inclusion/Exclusion Criteria are presented in detail in Table 3.
Inclusion/Exclusion Criteria.

The data extraction process involved four consecutive phases: identification, screening, eligibility and inclusion aiming for the extraction of 5 eligible studies to be included in this mini systematic review. The search results were to be reported in a PRISMA flowchart (Moher et al., 2009) and a customized data extraction sheet was generated to record the main characteristics of each included paper aiming to facilitate the direct comparison of different elements between the studies. The Newly Updated CASP Randomized Controlled Trials Checklist (Critical Appraisal Skills Program [CASP], 2020) was chosen to be applied as a Quality Assessment tool and a narrative synthesis would serve as a data synthesis outcome measure on the existing evidence from the 5 identified as eligible studies. The Template for Intervention Description and Replication (TIDIeR) would assess the reporting quality of the selected interventions for their replicability and description accuracy in the Inclusion Phase (Hoffmann et al., 2014). A meta-analysis was not possible due the limited number of studies to be included in this review.
Results
A detailed schematic presentation of the search process and Outcomes is presented in the PRISMA flow chart (Figure 1). The search was conducted on 15/03/2021. The advanced search in EBSCO PsychINFO and PsychArticles electronic libraries identified 29 papers (Figure 1).

PRISMA flow chart of search result.
A total of 14 papers were screened following the duplicates removal; non quantitative (n = 3), anecdotal (n = 1), non-English (n = 1) and not available in full text (n = 2) were excluded narrowing down the list in a total of 7 studies which passed for assessment to the Eligibility phase. One study examining the effect of laughter on a non-psychological factor (n = 1) and one that was published before 2011 were considered as non-eligible for inclusion. A 10-year research limit was considered by the author as a rule of thumb for this work due to limited resources while allowed her to include the most recent papers and make the review manageable (Griffiths, 2002). Citations of the retrieved studies that rejected in each Assessment phase is presented in Supplemental Appendix A. Five studies were identified as eligible to be included in the review (Table 4).
Citations of Eligible Data to be Included in the Review (n = 5).

Quality Assessment Outcomes
The Quality Appraisal assessment results showed that all five studies were sufficiently good in terms of their methodological quality and risk of bias. However, certain factors within all four sections affected the chosen papers to be evaluated as Satisfactory rather than as Key Papers. All studies were designed properly as RCTs although exclusions and withdrawals of participants were reported after randomization; a limitation that encompasses a low risk of bias or distortion of the final results. All studies were evaluated as methodologically sound although blinding was not applicable. The nature, design and methods used in designing a laughter intervention eliminate masking potentiality during implementation; neither single nor double-blinding. An intervention that requires for the experimental group to participate in a simulated laughter session discloses the identity of group allocation to the participants. All papers reported their results at a satisfactory level although only one paper reported the confidence intervals (CI; Morishima et al., 2019). Whether the benefits of each intervention outweigh the harms and costs could not be clearly stated as it is not addressed by the researchers and no information on any cost-effectiveness analysis is reported. Still, the positive effect of laughter on the psychological well-being and QoL that was reported in all studies may suggest that the benefits potentially outweigh the harms and costs. In any case, more studies need to be conducted including a cost-effectiveness analysis before any decisions to be made.
The reviewer finds no similarity between the participants of the studies (cancer patients) and the population of the forthcoming laughter intervention (healthy participants) although the outcomes could potentially be equally beneficial to a healthy cohort. Whether the five experimental interventions provide greater value to the people in reviewer’s care than any of the existing interventions remains unanswered. The Quality Assessment CASP Reports are presented for each study in Supplemental Appendix C. A summary of the CASP Checklists is presented in Table 5. An overview of the Quality Assessment outcomes is presented in Tables 6 and 7. The Template for Intervention Description and Replication (TIDIeR) reporting showed adequate reporting quality, replicability and description accuracy of all the selected interventions (Hoffmann et al., 2014) allowing for replication (see Supplemental Appendix D).
Quality Assessment Overview of Included Studies Using the CASP Randomized Controlled Trial Standard Checklist (see Supplemental Appendix C).
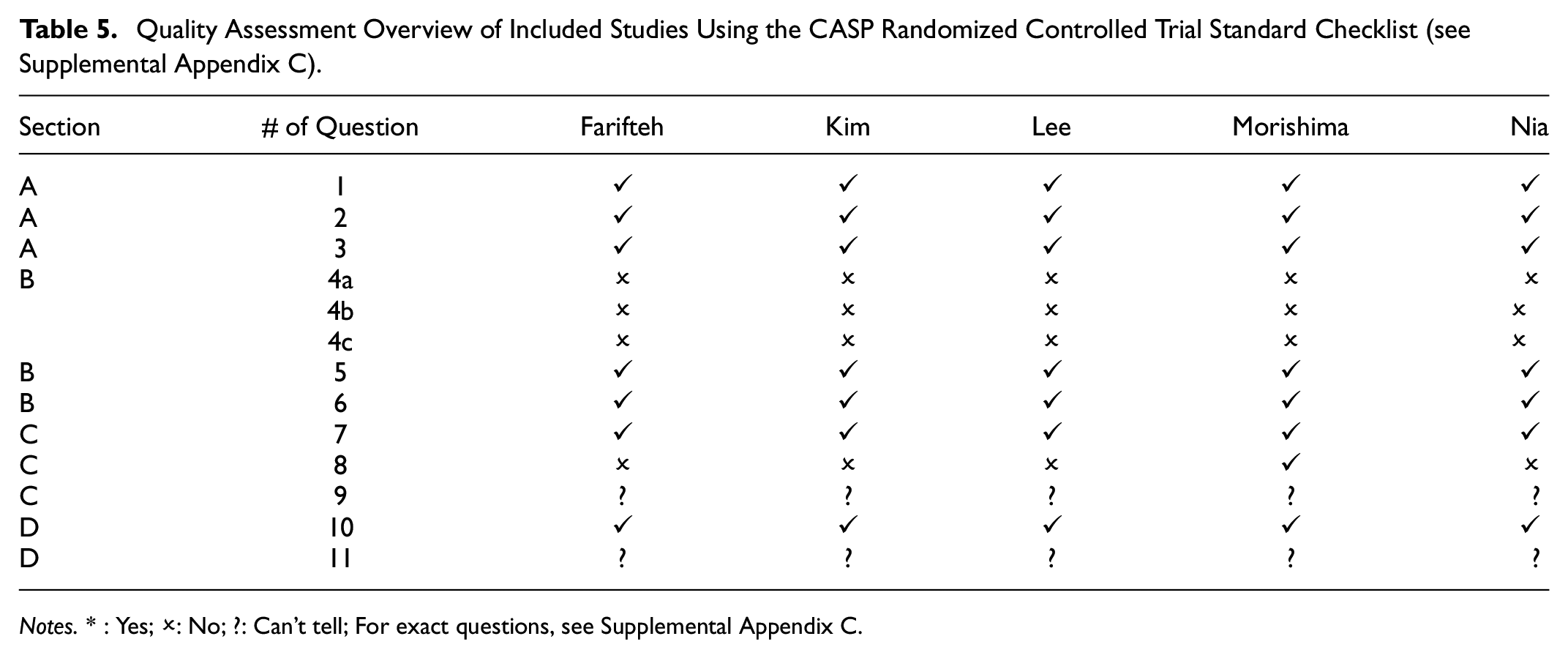
Notes. * : Yes; ✗: No; ?: Can’t tell; For exact questions, see Supplemental Appendix C.
Overview of the Quality Assessment outcomes.
Note. * Satisfactory: A satisfactory paper for inclusion in the mini systematic review.
Positive Therapy With Laughter: Some “Happiness or Well-Being Exercises” of Practical Application in Medicine, Adapted from Mora Ripoll and Quintana Casado (2010).

Study Characteristics Outcomes
All studies share similar study designs, populations, intervention settings, delivery modes and outcome measures. Self-administered quantitative data were collected before and after the interventions and the comparison was achieved with control groups (n = 5). Most of the randomized controlled trials (RCTs) reported primary outcomes (n = 3); Morishima et al. (2019) assessed QoL as a secondary outcome in iOSACA trial (Y. J. Lee et al. (2020) was a pilot secondary analysis from a primary RCT study reporting secondary outcomes. Most of the studies have recruited both male and female cancer patients (n = 3).
The effect of laughter was examined either alone (n = 2) or combined with another variable (n = 3). Methods included either humorous (n = 1) or non-humorous (n = 4) laughter stimuli. The study populations included only adult cancer patients. A detailed overview of the study characteristics is presented in Supplemental Appendix B.
Psychological Well-Being/QoL Outcomes
Results reported significant improvements in stress (n = 3), depression (n = 2), anxiety (n = 1), overall Health Related QoL (HRQoL; n = 1), emotional well-being (n = 1), Global Health Status & QoL (n = 1), mental well-being & positive mood (n = 1). Longitudinal relationships between interventions and outcome were not reported.
Farifteh et al. (2014) examined the effect of simulated laughter yoga on the perceived stress before chemotherapy. The researchers considered the effect of the intervention on certain covariant including among other psych-physical complaints and fear. The intervention was conducted and completed in a single 30-min session. The findings showed that yoga laughter may have a beneficial effect on psych-physical complaints, fear and reduce significantly overall stress in cancer patients. The researchers suggested a replication of their work using objective outcome measures including heart rhythm and pulse recordings along with self-administered questionnaires in order to diminish any potential effect of participants on the outcomes.
Similar results were reported another paper (Kim et al., 2015) examining the immediate effect of simulated laughter on stress, anxiety and depression among patients with breast cancer undergoing postoperative radiotherapy. This intervention was conducted twice weekly including four 1h duration sessions and the results showed significant reductions in all the three psychological health factors in the intervention group shortly after the first session compared with the control group. As the study population was consisted only by female patients, the authors acknowledged a potential enhancing effect of homogeneity on the results and further research was suggested to assess the longitudinal effect of the outcomes.
A homogenous population is also seen in the quasi-experiment by Y. J. Lee et al. (2020) who examined the effect of simulated laughter with entrainment music on stress, depression and Health-Related QoL (HRQoL) in gynecological cancer patients. The intervention was completed in eight 1h duration sessions and reported significant improvements in all three assessed factors after intervention; stress, mild depression, overall HRQoL and emotional. Interestingly, the laughter intervention was not significantly effective for moderate/severe depression and further assessment of any determinants that may increase the effect in moderate/severe depression in cancer patients was suggested. The researchers suggested that the single-center design might limit the outcomes generalizability. However, such a drawback has a dual effect. As soon as one might argue that the outcomes cannot be taken into account due to the chosen study design, the criticism that a laughter intervention is effective only in mild cases diminishes suggesting the need for further research with a different study design that would allow for generalizability. The researchers acknowledged also a potential effect on the outcomes due to the combination of laughter with the entrainment music; as was proven difficult to conclude on the size effect of each variable separately suggesting further examination of laughter effect alone.
Morishima et al. (2019) added the humorous linguistic element in an open-label RCT to examine the effect of simulated laughter yoga along with verbal comedy on QoL among cancer patients. The intervention was completed in two phases; an initial and a cross-over phase consisting of four 60-min sessions per phase. A significant improvement in Global Health Status was found in the intervention group although the results were reported only for a short time eliminating any longitudinal effect. The researchers acknowledged a potential social desirability effect due to the open-label study design as well as a potential recall bias attributed to a response shift in the survey due to the cross-over part in the study design. QoL was assessed as a secondary endpoint of iOSACA trial (Akazawa et al., 2018) and the authors concluded that further research is needed to verify the outcomes.
One study examined the effect of simulated laughter yoga on mental well-being among cancer patients undergoing chemotherapy (Nia et al., 2019). The mental well-being and the positive mood were significantly increased (6%) while the positive energy and relationships were also improved at a significant extend. The intervention was consisted of 4 sessions conduced before chemotherapy with a duration of 20 to 30 min. The researchers suggested further research with prolonged duration laughter yoga sessions to assess the accuracy of the outcomes.
Discussion
All the reviewed studies reported significant outcomes suggesting some robustness. This review revealed the beneficial health outcomes of laughter on diverse psychological well-being factors on cancer patients. Similar research has shown a decrease on depression, stress and anxiety among diverse populations such as elderly (Ghodsbin et al., 2015; K. I. Lee & Eun, 2011) or patients undergoing hemodialysis (Heo et al., 2016; Shin et al., 2010).
The beneficial effects of laughter when combined with other elements among cancer patients were also shown and they are in accordance with previous research suggesting the positive effect of laughter yoga on QoL or mood among cancer patients under chemotherapy (Dhruva et al., 2012; Dolgoff-Kaspar et al., 2012), humor therapy effect on QoL among breast cancer patients under radiotherapy (Rad et al., 2016), laughter with breathing exercises on QoL and mood (Heo et al., 2016), laughter therapy with music and exercise (Kuru & Kublay, 2017) laughter therapy with clowns on stress (Bacqué, 2010), laughter and stand-up comedy on psychological function (Yoshikawa et al., 2019) among different populations.
Two of the reviewed studies (Kim et al., 2015; Y. J. Lee et al., 2020) focused only on female patients with breast cancer and contributed with their positive findings showing both that laughter therapy may improve stress, anxiety and depression. Interestingly, research has shown that gynecological cancer patients might have an increased tendency to laugh (Ellis, 2006) resulting into a greater response tendency toward a laughter therapy program compared to men (Weisenberg et al., 1998); findings that suggest further research on homogeneity impact on outcomes.
Diverse cross-sectional associations between the interventions and the psychological wellbeing/QoL were identified but the longitudinal effect of these behavioral change outcomes and health benefits remains unclear. This can be attributed to the short duration sessions or the low number of sessions that was a common limitation between the reviewed studies. As the optimal duration and number of sessions is yet to be specified (Yoshikawa et al., 2019) further research with extended duration and multiple sessions is needed to assess and establish the accuracy of the effect and its exact mechanism.
A major finding showed that laughter therapy was not significantly effective for moderate/severe depression (Y. J. Lee et al., 2020). It could be argued that a simulated laughter therapy might be effective only in mild cases; an evaluation that constitutes a laughter program as a secondary or supplementary treatment suggesting that different management might be considered that is, primarily a pharmacological approach for achieving higher effect on more severe cases. Critically, it can be challenging to differentiate between placebo and actual pharmacological effects on cancer patients (Ostuzzi et al., 2018) suggesting a potential utilization of a laughter program either as a first-line complementary treatment or as a supplementary element to main cancer management treatment schemes (van der Wal & Kok, 2019) against depression and stress).
Among the common limitation the studies share is the lack of any theoretical underpinning, follow-ups, cost-effectiveness analysis and objective outcome measures. Noteworthy, none was designed and/or implemented by a health psychologist while no information of a multi-disciplinary research environment is reported. Considering the literature gap in assessing laughter effect on the psychological well-being/QoL in cancer patients and acknowledging that the design and implementation of health behavior interventions is the main research tool in Health Psychology, the significance and necessity of the knowledge, skills and overall contribution of Health Psychology Practitioners becomes more evident.
Conclusions/Recommendations
This mini systematic review showed the beneficial effects of laughter although its longitudinal effect remains unclear. The contribution of HP healthcare is major and health psychologists have the expertise to work with patients suffering from diverse long-term conditions and help them improve their psychological well-being and QoL.
Laughter therapy, also known as laughter yoga or laughter meditation, is a practice that harnesses the physical and psychological benefits of laughter for overall well-being. Some techniques commonly used in laughter therapy are (Bahari & Lorica, 2019;
The exercises for well-being that may be provided in positive therapy with laughing, both individually and in groups, are displayed in the table below. These exercises can be readily included into regular clinical practice as an alternative or supplemental treatment. Creating an emotional environment that encourages savoring and flow, encouraging change through the collaborative creation of new perspectives, languages, and discourse, the simultaneous presence of multiple communication channels and relation formats (laughter, humor, verbal and nonverbal language, art, music, dance, pairs, groups, etc.), and having an optimistic outlook on the future, which gives one the drive to act, interact, communicate, and dream in new ways are some of the factors that may contribute to its success (Mora Ripoll & Quintana Casado, 2010). Some of these techniques are:
Future implications include the setup of multidisciplinary work teams led by Health Psychology Practitioners to design and implement successful laughter therapy programs/interventions for cancer patients.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241300561 – Supplemental material for Laughter Interventions to Improve Psychological Well-Being/QoL in Cancer Patients: A Mini Systematic Review
Supplemental material, sj-docx-1-sgo-10.1177_21582440241300561 for Laughter Interventions to Improve Psychological Well-Being/QoL in Cancer Patients: A Mini Systematic Review by Anastasia Olympiou and Sana Ahmed in SAGE Open
Footnotes
Acknowledgements
I would like to thank Sana Ahmed for proof reading the article; and most importantly, my beloved husband, Dinos Kokkinos, for the inspiration and his support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Statement
Research data are available at References and in-text.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.