
Abstract
To move beyond the focus on individual types of support, we examined the overall reciprocity of support between older adults and their adult children. Drawing on the theory of esteem enhancement, we hypothesized that the under benefited older adults, defined as older adults whose support provided is larger than support received in intergenerational relationships, may have better health conditions than those with a more or less balanced exchange of support. To test the hypothesis, we examined the relationship between the reciprocity of intergenerational support and self-rated health (SRH) among older adults in China. We also investigated the moderating role of gender in this relationship. Using data collected from 832 older adults in Wuhan, China, we found that compared to those with a balanced level of reciprocal support in the intergenerational relationship, older adults who were under benefited from the intergenerational support had better SRH. This finding is in line with the esteem enhancement theory. We also found that gender moderated the association between the reciprocity of intergenerational support and SRH. Specifically, older women who under benefit from the support had better SRH than older women with a balanced level of reciprocal support. In contrast, older men who under benefit from the support had worse SRH than older men with a balanced level of reciprocal support. This finding highlights the necessity of constructing social psychological frameworks that are attuned to gender variations for a more comprehensive comprehension of health and health-related behaviors among older adults in China.
Plain language summary
We looked at how older adults and their adult children give and receive support from each other, instead of just focusing on one type of support. We thought that older adults who give more support than they receive might have better health. To test this, we asked 832 older adults in China about the support they gave and received, and how they rated their health. We found that older adults who gave more support than they received had better health than those with an equal exchange of support. Women who gave more support than they received also had better health, but men who gave more support than they received had worse health. This shows that we need to pay attention to differences between men and women when thinking about older adults’ health. We should also consider how older adults and their grown children support each other when we plan programs to promote health in older adults.
Keywords
Introduction
The number of Chinese aged 65 or above reached 190 million by the end of 2020 and represented 13.5% of the country’s population (National Health Commission of the PRC, 2020). Considering the high percentage of older adults in the population, it is important to examine the exchange of family support across generations as family remains the primary informal care unit for older adults in China (Y. Li & Guo, 2022; Lin, 2019). Previous studies found that intergenerational support can be beneficial for the general health status, life satisfaction, and psychological well-being of Chinese older adults (F. Huang & Fu, 2021; S. Liu et al., 2019; Shu et al., 2021). The health benefits may be in the form of psychosocial and economic resources that intergenerational support provides to older adults (F. Huang & Fu, 2021; S. Liu et al., 2019). However, some studies have also found that intergenerational support could negatively affect older adults’ general health and cognitive functioning (F. Huang & Fu, 2021; W. Mao et al., 2019; Wang & Gao, 2011). These studies suggest that receiving support in the intergenerational relationships may undermine the autonomy and self-esteem of older adults, thus deteriorate their health. With the inconclusive findings, there is a need to move beyond a focus on the individual effect of different types of support (such as emotional support and instrumental support) by embracing an overall reciprocity of support between older adults and their adult offspring when examining the association between intergenerational support and health of older adults (Q. Huang et al., 2017). Previous studies that examined the relationship between the reciprocity of support and the health of older adults often drew on equity theory, which emphasizes the importance of maintaining equity of exchanges among social actors (Pritchard, 1969). Accordingly, older adults who are successful in balancing their provision and reception in maintaining equity of exchange among generations have a better health outcome than those who provide or receive too much in the exchange. However, what equity theory suggested contradicts the Chinese cultural norms of interdependence among family members, where support is provided without immediate reciprocation. The equity theory may not be appropriate for understanding the relationship between the reciprocity of intergenerational support and health among Chinese older adults. Drawing on theory of esteem enhancement, we argue that, in intimate relationships, support providers can derive benefits, such as enhanced self-esteem and value, from contributing to the well-being of others even in the absence of reciprocal support or immediate rewards from those who receive support (Tesser, 1988; Väänänen et al., 2005). Therefore, it is possible that the under benefited older adults, defined as older adults whose support provided is larger than support received in intergenerational relationships, may have a higher level of well-being and better health conditions compared to those who have a balanced exchange.
To test and verify the hypothesis of the theory of esteem enhancement regarding the intergenerational relationship and health of older adults. This study aims to examine the relationship between the reciprocity of intergenerational support and self-rated health (Herein referred to as SRH) among older adults in China. We also attempt to investigate the moderating role of gender in this focal relationship. The consideration of gender differences is crucial due to the cultural expectations of gender roles as well as the division of labor in the Chinese society (S. Liu et al., 2019; Luo & Chui, 2018; Zhang, Chen, Feng, 2015). As such, the gender-based division of labor may impact the effect of intergenerational support on health outcomes. Studies suggest that older women prioritize unity among family members more than older men and are more likely to engage in support provision and social contact-seeking behaviors (S. Liu et al., 2019; H. Pan et al., 2021). Therefore, compared to older men, older women’s well-being and health status may be more influenced by interactions with intimate others, making it essential to examine the moderating effect of gender in reciprocal support and health status.
Intergenerational Support and Self-rated Health
The common measure of intergenerational support is the transfer of resources such as financial, emotional, or instrumental support from one generation to another (Chen & Silverstein, 2000; S. Liu et al., 2019; Silverstein et al., 2006). Empirical studies have found that intergenerational support can be beneficial for the health and well-being of Chinese older adults, although the effects might vary by types of support. For example, providing and receiving emotional support was found to benefit the physical health, life satisfaction, and psychological well-being of Chinese older adults (Chen & Silverstein, 2000; Krause & Liang, 1993; S. Liu et al., 2019; X. Liu et al., 1995).
Studies examining the impact of provision and reception of instrumental support on health outcomes yielded inconclusive results. X. Liu et al. (1995) found that neither receiving nor providing instrumental support from/to adult children directly affected the health of Chinese older adults. Two related studies found that providing financial support to adult children did not improve life satisfaction or the psychological well-being of older adults (S. Liu et al., 2019; Silverstein et al., 2006). Receiving financial support, such as remittances from adult children, improved the psychological well-being of older adults (Chen & Silverstein, 2000; Silverstein et al., 2006).
Nonetheless, a number of studies revealed that intergenerational support may have adverse effects on the overall health and cognitive functioning of older adults. For example, using panel data collected from older adults in Anhui province, W. Mao et al. (2019) found that an increase in the receipt of both household chore assistance and personal care assistance was associated with a faster decline in health over time. S. Li et al. (2009) found that the provision of instrumental support by adult children had a negative impact on SRH among older men, while the provision of financial support also had a negative impact on SRH among older women. These findings suggest that receiving support within intergenerational relationships may potentially compromise the autonomy and self-esteem of older adults, ultimately resulting in a decline in their health (Li et al., 2009; W. Mao et al., 2019).
Self-rated health (SRH)—usually measured by a single item question using response options including very good, good, fair, poor, very poor. SRH has been widely recognized as an indicator of overall health status in research and clinical settings, and has been shown to be a strong predictor of morbidity, mortality, disability, and utilization of health services (Chandola & Jenkinson, 2000; Idler & Benyamini, 1997; Mossey & Shapiro, 1982; Zajacova & Dowd, 2011). However, the reliability of SRH can be influenced by a variety of factors, including individual characteristics, social and cultural factors, and the context in which the self-rating is made. For example, a study conducted in the U.S. found that individuals from ethnic minority groups and those with lower levels of education had lower reliability of SRH (Zajacova & Dowd, 2011). In a study conducted in Sweden, it was found that SRH demonstrated good overall reliability, with observed among older men in comparison to younger men (Lundberg & Manderbacka, 1996). Other socioeconomic status indicators such as income and occupation were also found to be related to the reliability and predictive accuracy of SRH (Crossley & Kennedy, 2002).
In terms of cultural differences, existing literature yields inconclusive results regarding the cross-cultural validity of SRH. Studies conducted in the Europe generally found that there were no significant differences among ethnic groups concerning the correlation between SRH and mortality (Chandola & Jenkinson, 2000; Jylhä et al., 1998; Strawbridge & Wallhagen, 1999). This suggests that it is appropriate to utilize a single item measure of SRH to evaluate health status across various ethnic/cultural groups. However, recent studies conducted in the U.S. indicated that cultural pattern in subjective health measure like SRH might not always correspond with objective health measures (Bzostek et al., 2007; Erving & Zajdel, 2021). For example, Black, Latinos, and Asians tended to rate their health status more negatively than non-Hispanic whites in the U.S. Although SRH has been widely used as an indicator of morbidity and mortality in China, its reliability has not been fully evaluated. In a recent study conducted in China, Y. Pan et al. (2022) examined the reliability and validity of two commonly used versions of SRH. The response categories of the SRH scale developed by WHO includes “very good, good, fair, bad, and very bad,” whereas the version mainly used in the U.S. used categories such as “excellent, very good, good, fair, and poor.” The authors found the reliability of two versions of SRH was generally good among middle aged and older Chinese population, and two indices showed great predictive validity of mortality. Taken together, this study used SRH as our primary outcome variable among older Chinese adults.
Equity Theory or Theory of Esteem Enhancement: The Reciprocity of Support and Health
Among previous empirical studies that examined the relationship between the reciprocity of support and the well-being of older adults, most studies drew on equity theory (Pritchard, 1969). Equity theory emphasizes the importance of maintaining equity of exchanges among social actors. Accordingly, people who are more successful in balancing their provision and rewards in the exchange have a better health outcome than those who lose or gain too much in the exchange. In particular, equity theorists argued that equitably treated individuals in a relationship lead to enhanced well-being, whereas those who are involved in an inequitable relationship often feel uneasy and become distressed by the relationship (Väänänen et al., 2005). The balanced exchange of resources is the key to continuing social exchange relations. If the actors perceive that they are not gaining from the exchange, they may discontinue the exchange and evaluate the interaction negatively. At the same time, those who are over benefited (i.e., support provided is smaller than the one received) from the interaction may feel guilty and distressed.
Specific to the reciprocity of intergenerational support, a balanced exchange of supporting resources between generations often leads to favorable health outcomes for older adults (Q. Huang et al., 2017; Ramos & Wilmoth, 2003). In a study conducted in Brazil, Ramos and Wilmoth (2003) found that older adults (aged 60 and above) who maintained a balanced exchange (i.e., support provided is approximately equal to support received in the social exchange) with their relatives reported fewer depressive symptoms than those who received more or provided more support in social exchanges. A study conducted in China also found that older adults (aged 65 and above) who maintained a balanced level of reciprocal support with their adult children were more likely to report better self-rated health than those with an unbalanced level of reciprocal support (Q. Huang et al., 2017). The explanations of these studies were largely drawn on equity theory, viewing the interactions with family members being no different from interactions with others. That is, the interaction between older adults and their adult children should follow the general calculating of gains and losses rule in social interactions. If older adults were under benefited (i.e., support provided is larger than support received), they might perceive their interaction with their children as more costly than rewarding. For instance, they could use their money to purchase better health care services and living conditions instead of providing it to their children. Thus, being under benefited in intergenerational relations might impair the health of older adults (Q&x46; Huang et al., 2017). On the other hand, previous research (W. Mao et al., 2019) also showed that being in an over benefited exchange relationship might deteriorate the general health of Chinese older adults (aged 60 and above) in rural areas. This is largely because older adults who received more support than they provided were more likely to perceive themselves as dependent and incompetent than those who maintained balanced reciprocal support. In such cases, excessively relying on the support of their children might harm the self-esteem of over benefited older adults, making them feel guilty, frustrated, and depressed. Prolonged emotional stress, in turn, might damage their mental and physical health in the long run.
However, the premise of equity theory is that, in intimate relationships, the interactions between individuals still follow the principles of social exchange based on benefits and costs. We argue that this premise largely contradicts the Chinese cultural norms that emphasize the interdependence among family members. It is common for family members to provide support to one another without expecting the direct/instant reciprocation. In this sense, equity theory may not accurately and fully capture the relationship between the reciprocity of intergenerational support and health among older adults.
In this study, we turned into the theory of esteem enhancement to explain the focal relationship between intergenerational support and health. The theory of esteem enhancement is based on the idea that intimate relationships arise from specific affective ties between persons instead of from equity calculations. In intimate relations, the well-being of those involved takes precedence over the need to earn a reward for providing assistance (Väänänen et al., 2005). Instead, in the intimate relationship, it is the other’s welfare that is of primary concern, and one often provides all of the other’s needs without expecting reciprocation (Clark & Mills, 1979; Finkel et al., 2017). In addition, support providers may eventually benefit themselves through contributing to others’ well-being in intimate relations even without reciprocal support or immediate rewards from support receivers. This is because support providers gain esteem and value through “altruistic” behaviors (Pfattheicher et al., 2022). Consequently, supporting close persons may contribute to the well-being of support providers in long-term intimate relations (Ten Bruggencate et al., 2018).
Taken together, the equity theory ignores the heterogeneity in the non-equilibrium support. And a previous review article clearly revealed that older adults who were under benefited in intimate relations reported lower levels of mental distress and loneliness compared to the over benefited counterparts (Fyrand, 2010) The perception of being over benefited might lead to feelings of dependence and a perceived lack of autonomy, which could lead to declined health, mental health, and life satisfaction (W. Mao et al., 2019; Ramos & Wilmoth, 2003; Shu et al., 2021). To our best knowledge, there is no direct evidence that comprehensively compares the effect of older adults who are over benefited, who are under benefited, and those with a balanced exchange, and this is the focus of the current study. According to the theory of the esteem enhancement, it is possible that the under benefited older adults may even have better health and well-being than those with the balanced exchange because of their enhanced self-esteem and value.
Gender Differences in the Focal Relationship
Few studies have examined the moderating effect of gender while examining the relationship between the reciprocity of intergenerational support and the health status of older adults in China. Gender differences have to be considered as they are closely related to expectations of certain roles in the Chinese cultural settings (S. Liu et al., 2019; Zhang, Chen, Feng, 2015). The traditional division of household labor is still prevalent in China, although the social status of women has greatly improved in recent years. Women are still responsible for taking care of their families and household chores, whereas men are expected to provide financial support to their families (Luo & Chui, 2018). This gender-based division of labor might further influence the effect of intergenerational support on health. Studies revealed that older women tended to prioritize unity among family members more than older men (S. Liu et al., 2019; H. Pan et al., 2021). From a sociocultural perspective, women are socially expected to be more empathic and altruistic toward their loved ones than men. Therefore, the support and helping dynamics of intimate relationships may also be more influential on women than on men. In particular, previous research showed that women seem to be less well-off than men when they feel over benefited (Väänänen et al., 2005). It appears that females tend to behave in a “tend and befriend” manner when faced with various environmental stresses, focusing on protecting family members and increasing social contacts. The tendency to provide social support and aid may be closely related to female neuroendocrine mechanisms and health as similar findings have not been discovered among men (Taylor et al., 2000). Taken together, compared to their male counterparts, women’s well-being may be more influenced by interactions with intimate others. They may become support providers more often and enjoy giving support more than men (Zhang, Feng, Liu, et al., 2015) due to their expected social roles and biobehavioral tendencies.
Conceptual Framework and Hypotheses
Based on the abovementioned theoretical and empirical background, we developed our conceptual framework (see Figure 1). This study aims to examine the relationship between the reciprocity of intergenerational support and self-rated health (Herein referred to as SRH) among older adults in China. In addition, this study aims to investigate the moderating role of gender in this relationship. We proposed the following hypotheses:
Hypothesis 1. Compared to those with a balanced level of reciprocal support in the intergenerational relationship, older adults who are under benefited from the intergenerational support have better SRH, whereas those who are over benefited from the support have worse SRH.
Hypothesis 2. The association between the reciprocity of intergenerational support and SRH of older adults is likely to be moderated by gender. That is, the impact of the reciprocity of intergenerational support on SRH differs between older women and older men.

Conceptual framework.
Methods
Data
We analyzed data collected in Wuhan, China. Wuhan is the capital city of Hubei Province and is known as the political, economic, commercial, financial, cultural, educational, and transportation hub of central China. By the end of 2018, 22% of the individuals in the city were 60 years old or older. The survey was mainly conducted in the Jianghan district, one of the seven major districts in Wuhan. The research team recruited participants through convenient sampling. Through local contacts, the researchers were able to communicate with the administrative directors of 11 sub-districts (Jiedao in Chinese) out of 13 sub-districts in Jianghan. The administrative directors then distributed questionnaires to multiple communities (each sub-district has around 8–10 communities) that they administered. Finally, the directors and other administrative staff recruited survey participants from the communities and helped our research team collect the questionnaires from the respondents. Communities within each sub-district and participants within each community were selected primarily on the basis of convenient sampling.
Oral informed consent was obtained from participants before they filled out the questionnaires. The oral consent was obtained based on the following procedure: First, we introduced our research team’s affiliation and our study purpose; following this, we let the participants know the estimated time to fill out questionnaire; and after that, we let the participants know the voluntary nature of the study, and shared that the information they provided would only be used for research purpose. To maintain confidentiality, we refrained from requesting personally identifiable information, and the data collected will solely be utilized by our research team. The inclusion criteria for our survey participants were older adults who were at least 55 years old and who lived in Jianhan district. Between May and July 2017, the researchers successfully collected data on 850 community-dwelling residents from the Jianghan district in Wuhan. Since the focal research object is to examine the reciprocity of intergenerational support older adults who did not have adult children were excluded. After multiple data imputation and excluding respondents who do not have adult children (17 respondents were excluded), the final analytical sample consists of 832 older adults who have at least one adult child. This research received full ethical approval from the University of Hawai‘i at Mānoa, Institutional Review Boards (CHS#22774).
Measures
Dependent Variable
Health outcome was measured by the subjective rating of the general health status of respondents. SRH is widely recognized as a trustworthy measure of one’s overall health condition, as well as an established indicator of mortality and other negative health outcomes (Wu et al., 2013; Yamada et al., 2012; Zajacova & Dowd, 2011). Additionally, there is evidence that its credibility has been growing over time and people are increasingly able to provide more precise assessment of their own health (Jylhä, 2009). In the current study, participants were asked to rate their overall health using a five-point Likert scale by answering the question, “overall, how would you rate your health (1 = very poor, 2 = poor, 3 = fair, 4 = good, 5 = very good)?” This scale was recommended by the WHO and has been widely used in Europe (De Bruin, 1996). In the Chinese context, this version of five-point scale of SRH was also considered to be a reliable indicator of one’s general health status (Y. Pan et al., 2022). In the analyses, we recoded it into a variable that contains three response categories: 1 = Poor/Very Poor; 2 = Fair; and 3 = Very good/Good.
Focal Independent Variables
Intergenerational support was assessed by the frequency of providing and receiving economic support, housework support, and emotional support to/from adult children in the past 12 months. To measure the downward (from older adults to adult children) support, we asked respondents how often they provided the following help to their adult children: (a) Offered money or paid their bills; (b) Helped them with housework; (c) Listened to their worries and opinions. We also assessed upward (from adult children to older adults) by asking respondents how often their adult children offered them with the above-mentioned kinds of help. The values of alpha reliability of downward support and upward support are .61 and .64, respectively. Specifically, we recoded each of the three types of support into variables having three responses: 0 = never, 1 = seldom/sometimes, and 2 = often/very often. In addition to the six individual support items (three types of upward support and three types of downward support), a continuous variable termed “reciprocity of intergenerational support” was also created to determine the difference between the summed score of providing and receiving support. The alpha reliability of the six individual supporting items is .60. We further converted this continuous variable into a series of dummy variables, including (a) older adults who reported a balanced reciprocal support, (b) older adults who were under benefited from the support (they provided more support than they received), and (c) older adults who were over benefited from the support (they received more support than they provided). If the participant has multiple children, we explored the general situation of intergenerational support between them and all their adult children.
Moderating Variables and Control Variables
Gender (female = 1) was used as a moderator. Control variables included age (in years), educational attainment (in years of schooling), employment status (currently employed = 1), household income (three categories: monthly income is less than 3,000 RMB, monthly income is between 3,000 RMB to 8,000 RMB, and monthly income is above 8,000 RMB), marital status (currently married = 1), living arrangement (living with adult children = 1), number of adult children (number of children that are currently alive), number of chronic diseases (we asked the respondents to report whether they had been told by a doctor, nurse or therapist that they had any chronic conditions such as coronary artery disease, stroke or brain hemorrhage, cancer, etc.), and activities of daily living (need any help = 1).
Analysis
Multiple imputations were applied to handle the missing data. The missing rate for the dependent variable was 4.4%, and for the independent variables ranged from 9.2% to 11.9%. The multiple imputation algorithm was based on the Markov Chain Monte Carlo (MCMC) method and was conducted using SPSS version 21. Bivariate analyses using the independent samples t-test and chi-square test were performed to determine the differences in focal variables by gender. Results from both univariate and bivariate analyses were presented in Table 1. Four ordered logistic regression models were constructed to investigate the effects of focal independent variables on SRH and results were summarized in Table 2. Model 1 used a series of dummy variables—reciprocity of intergenerational support, and Model 2 replaced it with six individual support items. Model 3 added interaction terms between the reciprocity of intergenerational support and gender, and Model 4 added interactions between six individual support items and gender. For each ordered logistic regression that we constructed, we used Wald test to examine whether the model violate the proportional odds assumption. The results were used to determine whether ordered logistic models are appropriate to examine our focal relationships.
Sample Characteristics by Gender.

Notes. t-test was performed for gender and intergenerational support; chi-square test was performed for gender and self-rated health as well as for gender and ordinal variable-balanced intergenerational support.
P < .05. **P < .01. ***P < .001; ns stands for statistically nonsignificant; GD stands for gender differences; means and standard deviations (in parentheses) are provided for continuous variables and percentages (PCT) are provided for categorical and dichotomous variables.
Ordered Logistic Regressions: Regress Self-rated Health on the Reciprocity of Intergenerational Support and Control Variables.

Notes. odds ratios are reported.
stands for the reference group; standard errors are in parentheses.
P < .10. *P < .05. **P < .01. ***P < .001.
Results
Descriptive Statistics
Descriptive statistics for the whole sample and the stratified subsamples by gender were presented in Table 1. As shown in Table 1, close to 35% of the surveyed older adults rated their health as very good or good, more than 55% of them reported their health as fair, and only around 10% of them had poor/very poor SRH. Nearly 40% of the older adults reported that they were under benefited from reciprocal support, and less than 20% of them were over benefited in intergenerational exchange. Approximately 41% of older adults reported that they provided equal levels of intergenerational support compared to their adult children. The mean scores of provided economic support, housework support, and emotional support were 1.00, 1.25, and 1.38, respectively. The mean scores of received economic support, housework support, and emotional support were 0.95, 1.08, and 1.26, respectively.
The average age of the respondents was approximately 67.5 years, and the mean educational attainment was approximately 11 years. Around 5% of older adults were currently employed, and around 77% were currently married. Approximately 48% of the older adults were currently living with their adult children, and on average our respondents had 1.32 adult children (still alive). Nearly 22% of the respondents belonged to the low-income group, about 59% of them belonged to the middle-income group, and only 19% were in the high-income group. In terms of health conditions, on average, older adults had approximately 1.37 chronic diseases, and approximately 93% of them did not need any help in doing activities of daily living.
The results of the bivariate analysis showed that older women had better SRH than older men. More older women than men reported that they provided more intergenerational support than their adult children. Older women also reported significantly higher mean scores of provided housework support and emotional support to their adult children than older men.
Results of Ordered Logistic Regression
The ordered logistic regression models constructed to determine the effect of intergenerational support while controlling for sociodemographic indicators were presented in Table 2. The test of the parallel-line assumption yielded insignificant test statistics (P > .05 for all constructed models), which means all models did not violate the proportional odds assumption. In other words, ordered logistic regression are appropriate to examine our focal relationships. The dependent variable, SRH, ranks from 1 (poor/very poor) to 3 (good/very good) in an ascending order. As shown in Model 1, “under benefited” was significantly and positively associated with SRH (b = .32, P < .10) for the whole sample. Thus, older adults who were under benefited from intergenerational support were more likely to have better health conditions than poorer health conditions compared to those maintained a balanced support pattern. Their odds of having better SRH were 37% (exp [.32]-1) higher than the odds of those who maintained a balanced support pattern. No significant association was found between over benefited and SRH. Therefore, Hypothesis 1 was partially supported by our data. As shown in Model 2, among all the intergenerational support indicators, economic support provided (b = −.31, P < .10) and housework support received (b = −.40, P < .10) were significantly and negatively associated with SRH. Thus, older adults who provided more economic support and who received more housework support from their children were less likely to have better SRH. By contrast, housework support provided (b = .36, P < .05) and emotional support provided (b = .35, P < .10) were significantly and positively associated with SRH. In other words, older adults who provided more housework support and who provided more emotional support to their adult children were more likely to have better SRH.
Model 3 and Model 4 examined the moderating effect of gender. Results showed that the interaction between “under benefited” and “female” (the dichotomous variable of gender) was significant and positively associated with SRH, suggesting that, a gendered pattern did exist in the association between “under benefited” and SRH. Specifically, the main effect coefficient of “under benefited” on SRH was 0.21 and the interaction effect coefficient was 0.85. Based on the main effect and interaction effect, we calculated that, among female older adults, the odds of those who were under benefited from support that having better SRH were 1.89 (exp [.85–.21]) times the odds of those who maintained a balanced support pattern with their adult children. Among males, the odds of those under benefited from support that having better SRH were 19% (1-exp [−.21]) lower than the odds of those who maintained a balanced support pattern. Therefore, Hypothesis 2 on gender differences was supported. As shown in Model 4, the interaction term between provided economic support and female was significant and negatively associated with SRH, suggesting that, gender did moderate the association between provided economic support and SRH. Based on the coefficient of main effect (−0.71) and the coefficient of interaction effect (0.58), we calculated that, among female older adults, frequently providing economic support decrease the odds of having better SRH by 12% (1-exp[−0.71+0.58]), whereas, among male older adults, frequently providing economic support decreases the odds of having better SRH by 51% (1-exp[−0.71]).
Figure 2 visualizes the moderating effect of gender in the association between “under benefited” and SRH. The Y axis indicates the probability of each SRH outcome. The dashed line indicates the relationship between “under benefited” and SRH for female older adults. The solid line indicates the relationship between “under benefited” and SRH for male older adults. As shown in this figure, being under benefited in reciprocal support increases the probability of having very good/good SRH and decrease the probability of having poor/very poor SRH for female older adults. By contrast, being under benefited in reciprocal support slightly decreases the probability of having very good/good SRH and increases the probability of having poor/very poor SRH among male older adults. These findings reconfirmed the moderating role of gender in the focal relationships.
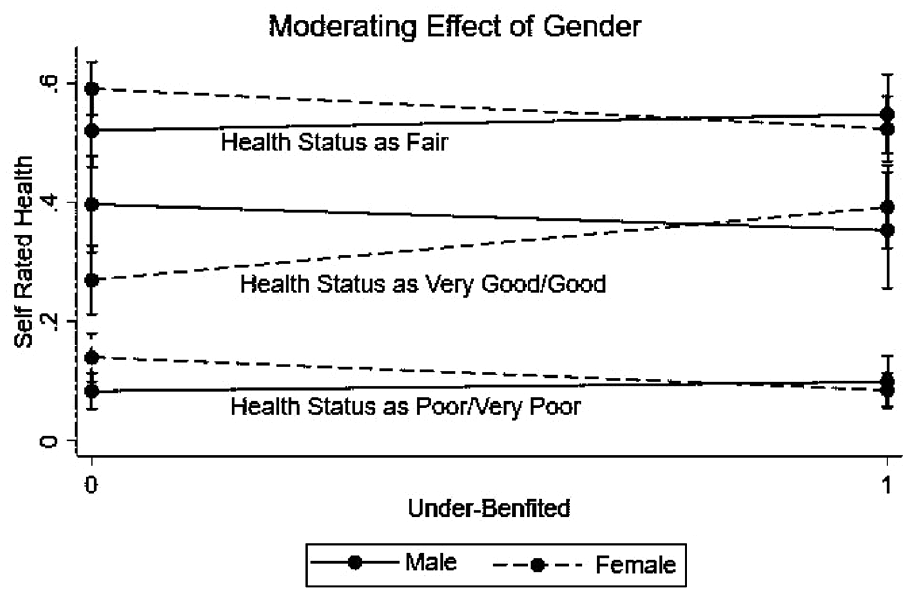
Visualization of moderating effects of gender on SRH.
Discussion
In this study, we found that there were more female older adults providing more support than receiving in intergenerational relationships than male older adults, while more older men than older women had a balanced level of support with their adult children. In addition, we found that, compared to those with a balanced level of reciprocal support in the intergenerational relationship, older adults who were under benefited from the intergenerational support had better SRH, whereas no significant association was found between over benefited and SRH. These findings partially supported Hypothesis 1. We also found that gender moderated the association between the reciprocity of intergenerational support and SRH. Specifically, older women who were under benefited from the support had better SRH than older women with a balanced level of reciprocal support. In contrast, older men who were under benefited from the support had worse SRH than older men with a balanced level of reciprocal support. Therefore, Hypothesis 2 was supported.
Based on results from the bivariate analyses, more female older adults were under benefited from intergenerational support than their male counterparts. More older men than older women maintained a balanced level of reciprocal support with their adult children. This gender disparity suggests that the traditional division of household labor still exists in China. Although some women started to earn more and had higher social status than their husbands, they were still expected to bear more responsibilities and care for their families (Luo & Chui, 2018). Additionally, women in China generally retire earlier than men. For men, retirement is generally compulsory at 60, while women with professional or government jobs must retire at 55 and 50 for those with other occupations (Zhang et al., 2017). Consequently, older women also have more time to help family members.
Our study also showed that providing more support than receiving was related positively to SRH among older adults for both gender groups. Our results are inconsistent with those from a recent study based on the 2010 Survey on the Social Status of Women in China, where the authors found that older adults with a balanced level of reciprocal support had better SRH than those with an unbalanced level of support (Q. Huang et al., 2017). Based on the equity theory of aging, Huang et al. argued that a balanced exchange of resources across generations is the key to continuing social exchange relations. We argue that the conclusion reached by Huang et al. overlooks the heterogeneity of unbalanced reciprocal support. Older adults who are over benefited or under benefited from intergenerational support may experience disparate effects on their health outcomes. According to esteem enhancement theory, individuals may gain a great deal of esteem and value from assisting family members (Väänänen et al., 2005). Our finding indicates that older adults who were under benefited from intergenerational support had favorable SRH compared to those who had a balanced level of reciprocal support, which provides evidence supporting the theory of esteem enhancement. In intergenerational relations, the well-being of family members takes precedence over the need to earn a reward for helping them. Therefore, older adults often provide for their adult children’s needs without expecting reciprocation. By assisting family members, older adults can also enhance their well-being by reinforcing their sense of purpose and meaning in life. This can strengthen their self-efficacy and allow them to become more intimate with others (F. Huang & Fu, 2021), which, in turn, may help them better cope with adverse physical or psychosocial experiences in later life and maintain good health status (Dorfman et al., 2009). Therefore, the theory of esteem enhancement offers greater explanatory power over the equity theory in this study.
Our findings also indicate that the traditional Chinese filial piety norm has been gradually diminished by the rapid socioeconomic transition in the past several decades. The traditional filial piety norm emphasizes that adult children should support and care for their aging parents to fulfill their filial duties (Dong & Zhang, 2016). In the modern era, the filial piety norm also emphasizes the interdependence and co-residence among generations (Smith & Hung, 2012). However, rapid economic growth and unprecedented mobility among young adults have slowly changed the traditional intergenerational living arrangements. Consequently, non-traditional households have increased substantially, and many older adults live with their spouses only or live alone (X. Mao & Han, 2018). Maintaining balanced support with adult children is difficult in empty-nest households (older adults live alone or with their spouse only). In addition, many older adults are aware of the financial burden of their adult children as many of them expect to live and purchase real estate in big cities. Thus, older adults have lowered their expectations for upward support (especially the economic support). Older adults who are financially strong might even provide downward financial support to their adult children. Offering more support to adult children provides a sense of purpose and meaning for older adults and follows the current mainstream ideology in the rapidly aging Chinese society that emphasizes the importance of laoyousuowei (being active and productive in later life).
Our results also revealed that gender could moderate the relationship between the reciprocity of intergenerational support and SRH. Specifically, older women who were under benefitted from the support had better SRH than older women with a balanced level of reciprocal support. In contrast, older men who were under benefitted from the support had worse SRH than older men with a balanced level of reciprocal support. This finding is in line with the previous research where authors found that giving more support than receiving in intimate relations positively affected the health status of women in Finland (Väänänen et al., 2005). The gender differences may be explained from a sociocultural perspective. As indicated by our descriptive statistics, older women provided significantly more housework and emotional support to their adult children than older men. This suggests that women bear more responsibilities in the family than men. At the same time, older women in China prioritize harmony and intimacy among family members more than older men (H. Pan et al., 2021). Consequently, they are expected to show more altruistic behaviors toward their family members by traditional norms. comparison, men are more likely to be involved in economic activities outside families. Even though some of them share the responsibility of taking care of family chores with their wives, they only undertake tasks that are “flexible and fun” (Zhang, Feng, Liu, et al., 2015). Due to the influence of traditional Chinese culture, many female older adults, however, view their tasks as obligations rather than burdens (Zhang, Chen, Feng, 2015). Therefore, when older women provided more support to their adult children, they fulfilled a culturally valued role. According to the role theory (Baker et al., 2005) and the activity theory (Havighurst, 1963), maintaining a social role after retirement is important for the well-being of older adults. The gratification of performing a culturally valued social role might particularly help enhance the SRH of older women in China.
The revealed gender differences also suggest that older men are more likely to stick to the filial piety culture than older women. The filial piety is a Confucian doctrine, emphasizing that adult children are expected to have the responsibility to care for their aging parents. Many older adults view the support from their children as the repayment for raising them. Therefore, providing more support than receiving suggests the fulfillment of filial duties by adult children, whereas receiving more support from aging parents, on the other hand, indicates a deviation from the filial piety norm (S. Liu et al., 2019). In this sense, for older adults who strongly adhere to the filial piety culture, providing more support than their adult children would deteriorate their health.
Our study had some limitations. We collected cross-sectional data from one study site, which prevented us from making causal inferences and generalizing the findings for the entire population of older adults in China. In addition, generalizability may have been further weakened because older adults were recruited primarily through convenient sampling where participants were selected based on their availability, accessibility, or willingness to participate in the study. Therefore, “young old” and older adults with better cognitive and physical function may be overrepresented, and “oldest old” and those with limited cognitive and physical function may be underrepresented. So, the health status of the Chinese older adult’s population may be overestimated in our sample and this overestimation may further affect the generalizability of findings. Moreover, our sample exhibits an overrepresentation of older women and an underrepresentation of older men, considering the importance of gender in shaping focal relationships, it may be necessary to apply a more sophisticated sampling strategy to make the gender ratio in our sample more representative of the study population in future research. In addition, some important control variables such as self-esteem, sense of control, smoking, and drinking behaviors were not included in the survey, which limited our ability to comprehensively understand the association between reciprocal support and SRH. Finally, self-administered questionnaires might be inaccessible to older adults with limited education and reading ability.
Despite these limitations, our study highlighted the importance of considering the impact of gender differences when examining the relationship between intergenerational support and SRH for Chinese older adults. We also showed that the heterogeneity of unbalanced reciprocal support may need to be considered while examining this focal relationship. For future research, it is important to examine the role of aging parents as supporters and contributors in Chinese families, instead of only considering them as the receivers of care and support from their adult children. Additionally, our findings emphasized the necessity of developing social psychological models that are more sensitive to gender differences in order to better explain health and health related behaviors of Chinese older adults.
Conclusion and Implications
In conclusion, this study investigated the relationship between the reciprocity of intergenerational support and SRH, as well as the moderating role of gender in this relationship among Chinese older adults using data from 832 participants in Wuhan. Our results revealed that older adults who received less intergenerational support than they provided reported better SRH compared to those whose overall level of reciprocity was balanced. In addition, older women who were underbenefited in intergenerational support had better SRH than those with balanced support, while older men who were under benefited had worse SRH than those with balanced support.
Our findings provide evidence to support the positive and productive aspect of aging among Chinese older adults who are able to contribute substantially to their families and at the same time have health benefits. Policymakers and practitioners should recognize the valuable contributions that Chinese older adults make within the family, particularly through the provision of intergenerational support to their adult children. This shift in perspective could lead to more empowering policies—such as providing financial incentives to older adults to help them better support family members, especially those who require long-term care—to cultivate the productive and engaging potential of Chinese older adults. Findings on the moderating role of gender suggests that, when planning and implementing health interventions that involve intimate social relationships such as intergenerational relationship, it is crucial to take into account how the distinct dynamics of these relationships impact the health of both older men and older women as the same dynamic may produce divergent outcomes for different gender group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shanghai Philosophy and Social Science Planning Youth Project [Grant Number: 2022ESH005].
Ethical Approval
Not Applicable
Data Availability Statement
The data are available from the corresponding author upon reasonable request.