
Abstract
The number of foreign residents and visitors in Japan is increasing, which necessitates culturally competent care in hospitals. This study aimed to describe the experience of international students who visited hospitals in Japan. In total, nine international graduate students in a medical university participated in semi-structured interviews in English. The interview contents were transcribed and analyzed using content analysis. While participants were satisfied with an efficient medical system and kind staff, they also had difficulty communicating with staff and receiving health care due to language and cultural differences. Participants desired Japanese health care staff speak English, as well as have English documents. The differences from their own countries were mainly medical fees, insurance, the medical system itself, and use of English to communicate with foreign patients. It is necessary to improve staff’s English skills, provide English documents, use multilanguage interpreter services, and explain Japanese hospitals’ medical system.
Keywords
Introduction
In Japan, the number of foreign residents and visitors has been increasing. By June 2020, there were 2.88 million foreign residents in Japan (2.3% of the population), a record high. It is, however, still very low compared with other Organisation for Economic Co-operation and Development (OECD) countries (OECD Data, 2019), and permanent residents account for only 0.64%. Japan’s low birthrate and aging population have met a workforce shortage, and thus, in April 2019, the residential criteria changed to accept more foreign people with specific skills, both low and high skills (Immigration Services Agency of Japan, 2018). Although there is still a 5-year limitation of stay for low-skill workers, high-skill workers can stay unlimited years and be accompanied by family members. The number of international students who can work up to 28 hr per week has also been increasing (Milly, 2020). The number of foreign visitors in 2019 was 31.8 million people, which increased 6 times from 5.2 million people in 2003 (Japan National Tourism Organization, 2020). The Japanese government set a goal to have 40 million foreign visitors in 2020 for Tokyo Olympic and economic activation (Japan Tourism Agency, 2019).
As the number of foreign residents and visitors increases, the number of foreign patients visiting hospitals has also increased. However, Japanese health care workers are poorly prepared to cope with patients from foreign countries. Many studies have reported the difficulties nurses face when seeing foreign patients in hospitals. The most common difficulties reported by nurses were language barriers, cultural differences, patients’ economic problems, and differences in health care systems (Maeno et al., 2011). Leininger (2002) established Culture Care Theory, which describes factors that need to be included for culturally competent care as religion, politics, economics, worldviews, environment, cultural values, history, language, gender, education, and technological factors. To learn about these factors, nurses have to communicate well with the patients. Hashimura and Ohnishi (2016) summarized eight necessary communication skills reported by 120 Japanese nurses caring for perinatal foreign people: communication skills related to understanding different cultures, respecting different cultures, solving problems, utilization of social resources, exchange of information, nonverbal communication, understanding Japanese culture, and preparation for delivery.
Although there are many studies investigating the difficulties nurses and other health care staff have taking care of foreign patients, there are not many studies investigating the experience of foreign patients visiting hospitals in Japan. Usui (2013) surveyed 158 foreign residents (56% Caucasian) and reported low satisfaction with health care due to different languages and cultures. Osaka University Graduate School of Human Sciences and DiversityRx conducted a national survey with 424 foreign patients who sought health care in Japan (Fortier et al., 2016). The survey revealed that language and cultural barriers have a significant impact on the quality of care received by many foreigners in Japan. They reported that foreign people were lost without translation and had trouble with the following four key findings: (a) finding and getting health care, (b) language barriers and interpretation, (c) doctor–patient interactions, and (d) basic communication. In this survey, nearly 80% of participants were from North America, Europe, Australia, or New Zealand, and 73% spoke English as their primary language. A quarter of them were language teachers (Fortier et al., 2016); this study, however, has not been reported as an original research article.
Regarding qualitative studies, Teraoka and Nonaka (2017) reported the cross-cultural experiences of 22 foreign residents who accessed Japanese health care by group interview in Japanese. They reported that foreign residents in Japan faced language barriers, preconceptions caused by differences in physical appearance, and insufficient understanding of cultural differences. Although participants could speak Japanese, they still perceived language barriers. Watanabe and Sakka (2017) interviewed with 13 foreign residents in Fukui prefecture in English and reported the experience visiting hospitals. They reported problems with privacy and confidentiality, cultural differences, mismatch in expectations, differences in medical systems, and language-related issues (both spoken and written). Of the 13 participants, six were from North America, two from Europe, and one from New Zealand. However, 76% of foreign residents in Japan come from eight Asian countries—China, Korea, Vietnam, The Philippines, Nepal, Indonesia, Taiwan, and Thailand—and Asian immigrants may have experienced different difficulties from previous studies (Fortier et al., 2016; Usui, 2013; Watanabe & Sakka, 2017).
Among foreign residents in Japan, students account for approximately 12% (336,847), which is the second largest category following 28% permanent residents, and 53% of the 20s and 30s age group (Ministry of Justice, 2019). However, there is no study reporting experience of international students in health care in Japan. The purpose of this study was to describe the experience in visiting hospitals of international students in a university in Japan.
Research questions of this study were as follows:
Method
Definition of Words
International students were defined as students who were born and raised in other countries and came to Japan to study at the university.
Participants and Setting
Participants were nine international students who agreed to an interview out of 58 international students who had participated in the online survey in a medical university in Tokyo (Kondo, 2018). The university is located in the Tokyo Metropolitan area and accepts an increasing number of international students each year—The majority are from Asian countries, and most specialize in health care fields. Therefore, these students have a double perspective as both patients and health care staff. International students in this university were selected as they were easily accessible, and the majority are from Asian countries. The university has an affiliated hospital, which established the International Healthcare Department in April 2018. Data were collected in the previous year.
Data Collection
Semi-structured interviews taking approximately 30 min were conducted by the first author in English from September to October in 2017. The demographic questions included participants’ characteristics such as age, gender, nationality, Japanese and English ability, native language, study program, years living in Japan, and religion. Japanese and English ability were self-evaluated on five levels (1: Cannot speak, 2: Can speak a little, 3: Able to communicate about daily life, 4: Able to report or understand information using medical terms, 5: Speaks fluently) referring to Usui’s (2013) study.
Interview questions were created referring to Hayashi and Mori’s (2003) study and developed by the authors, including an international student. After obtaining permission from participants, we used an Integrated Circuit recorder for interview content. The interview questions included the following:
With whom did you visit the hospital/clinic?
How did you select the hospital/clinic?
Where did you hear or learn about the hospital/clinic?
Please describe what you were satisfied with at the hospital/clinic.
Please describe what difficulties you encountered and what you were dissatisfied with.
What differences in health care from your own countries did you perceive?
What differences in culture from your own countries did you perceive?
How did you cope with the difficulties?
How would you desire Japanese health care be improved?
Analysis
Interview contents were transcribed and analyzed using content analysis (Elo & Kyngäs, 2008). Content analysis is a method that can be used with either quantitative or qualitative data in either a deductive or inductive way. The inductive approach is recommended when there is not enough former knowledge about the phenomenon or the knowledge is fragmented. The categories will be derived from the data in inductive content analysis. If the structure of analysis is operationalized on the basis of previous knowledge and the purpose of the study is theory testing, deductive content analysis is used, which moves from the general to the specific (Elo & Kyngäs, 2008). Although there are several studies reporting experience in health care of foreign people in Japan, there is not enough knowledge about Asian people and international students. This study uses an inductive approach to deeply understand participants’ experience and discuss based on the four key findings of Fortier et al.’s (2016) report. To ensure trustworthiness and rigor (Elo et al., 2014), the following analysis process was used:
The first author read each participant’s statement several times to become immersed in the data and to acquire general understanding of the content.
The text statement for each answer was divided into meaning units and condensed according to the main content, and the identified units were coded.
The codes were grouped into subcategories and categories for each question by similarities.
For validating the analysis, the second author, who had experience with content analysis, checked the initial analysis. Then, the first and second authors repeatedly discussed and revised the coding and categorizations until a high level of agreement was obtained.
Finally, the third author, who was an international student and had not participated in the previous analysis process, confirmed the coding and categorization.
【 】indicates categories and “ “ indicates what the participants stated.
Ethical Considerations
This study was approved by the Medical Research Ethics Committee of Tokyo Medical and Dental University (Approval Number M2017-050). Interviews were conducted in a private room. Participants were informed both verbally and in writing of the study purpose, confidentiality issues, and their right to withdraw at any time. Participants who agreed voluntarily to participate signed consent forms.
Results
Participants’ Demographics
Participants’ characteristics are summarized in Table 1. The average age was 28.7 (±1.5) years, six (66.7%) were males, eight were graduate students (88.9%), and one was a research student. They had been in Japan for 2.5 (±0.7) years on average, eight (88.9%) came from Asian countries, and eight (88.9%) had religious beliefs. Their average English ability was 4.2 (±0.6) and Japanese ability was 2.2 (±0.6).
Participants’ Characteristics.

What Is International Students’ Experience With Health Care in Japan?
With whom did you visit the hospital/clinic?
Seven participants had visited the hospital 【alone】, five 【with friends】 (three international students and two Japanese friends), and one【with family】 (her husband). The reasons for taking friends or family members were to act as translators, to make participants feel safe, or because the friend had informed them about the hospital.
“Usually with my friend. Because my Japanese language is not so good. If I have one person on my side, I can understand from them.” “Only me. I’m not afraid but I just worry about the communication with the doctor, but from the annual health check of our university, I totally see the doctor can speak English very well. So I am just a little bit afraid of communication.”
How did you select the hospital?
They selected the hospital because they were【recommended】by the university or their friends. It was【easy to access】location, open hours and less crowded, and with English support. They heard the【quality of the hospital was good】. They【searched the internet】by putting key conditions.
“Before I went to see the doctor, I visited my health clinic in our university. And then I got a reference letter that he recommended me to see a specialist.” “The university hospital is good and have some preparation.”
Where did you hear or learn about the hospital/clinic?
Most of them were【recommended】by the university or friends, or【searched the internet】. Some of them【visited without any information】.
“From the foreign student support center in the university. They give me some guidance; where to go when we get sick. They did the orientation when I entered the university.” “I didn’t know anything. I just went there.”
Please describe what you were satisfied with at the hospital/clinic
Areas of satisfaction were classified into three categories—【medical system was good】, 【dealing with different language was good】, and 【attitude of staff was good】—and seven subcategories (Table 2). The category【medical system was good】included the subcategories: process for seeing doctor was smooth, treatment was appropriate, environment was good, and privacy was observed. The process for seeing doctor was considered smooth when the hospital was systematic and efficient and everything was in order. Due to such a smooth process, waiting time was shorter than in their own countries and their expectations. Participants were satisfied that the examination room was well equipped. In addition, they could make a reservation at a precise time because Japanese people are generally punctual. The environment was good with a comfortable waiting area and their privacy was observed in a private room with a curtain.
“It is so organized, so you just follow. They don’t waste time. Everything is at the right place.” “They prepared and saw me. Because I feel pain and almost nearly 1 hour giving birth and they prepared everything to go well. I’m so satisfied with their service.” “Everybody just like sitting quietly on the sofa and waiting the number watching the screen. You know everything is in order and everything is so quiet and nice.” “The most satisfied point is privacy. There are curtains in the room. Even inside the room, it makes you feel privacy.”
Satisfaction When Visiting Hospitals.

In the category【dealing with different language was good】, participants thought it was easy to communicate because medical doctors were able to speak English. There were English documents, technical terms were explained using books, and visual information was easier to understand. They evaluated health care staff’s kindness such as health care staff tried to use easy English and health care staff explained using gestures, which helped participants understand.
“I use sometime English and sometime Japanese. For the doctor, I use English because I want to understand clearly what he says. And the doctor could speak English well. Because I made a reservation with the doctor who can speak English.” “Basically they have some English instruction so we can understand what they want us to do.” “The doctor checks online website, and if they are not able to explain some terms or something or they want ask me something, they try to type English.” “Actually I fortunately saw a Chinese speaking person near the reception. She should be a medical guide? I don’t know how to describe the position but she belongs our university and she can speak Chinese.”
In the category【attitude of staff was good】, participants stated specifically that nurses’ and physicians’ attitudes, such as kindness, politeness, and friendly smile, made a good impression.
“I think the healthcare worker in Japan is so nice. They are always comfortable to me.” “Nurses cannot speak but I think they were quite helpful.” “They know how to respect patients, how to respect people. They give much respect to us.”
Please describe what difficulties you encountered and what you were dissatisfied with
Areas of dissatisfaction were classified into three categories—【language problems】, 【problem of medical system】, and 【problem of staff attitudes】—and eight subcategories (Table 3). Regarding【language problems】, all participants felt it was hard to communicate with health care staff. There were not many health care staff who could speak English, apart from medical doctors. It was hard to explain in Japanese or in English because participants were not native English or Japanese speakers. They felt staff’s explanation was not sufficient because staff saw them as foreigners. Communication was difficult because they did not receive answers to their questions. Written material was hard to understand because it was written only in Japanese for explanation and prescriptions. It was difficult to figure out where they should go in the hospital because the display was only written in Kanji (Chinese) characters.
“How to explain the symptoms and understanding Japanese are main problems.” “We cannot explain fully about our feeling in English or Japanese. That is the problem.” “Not all the time the healthcare worker can speak English. Maybe half of them can speak English.” “The explanation from doctor is not enough. The doctor would explain more in detail to Japanese patients, but it would be difficult to explain to foreign patients and finishes with a brief explanation.”
Dissatisfaction When Visiting Hospitals.
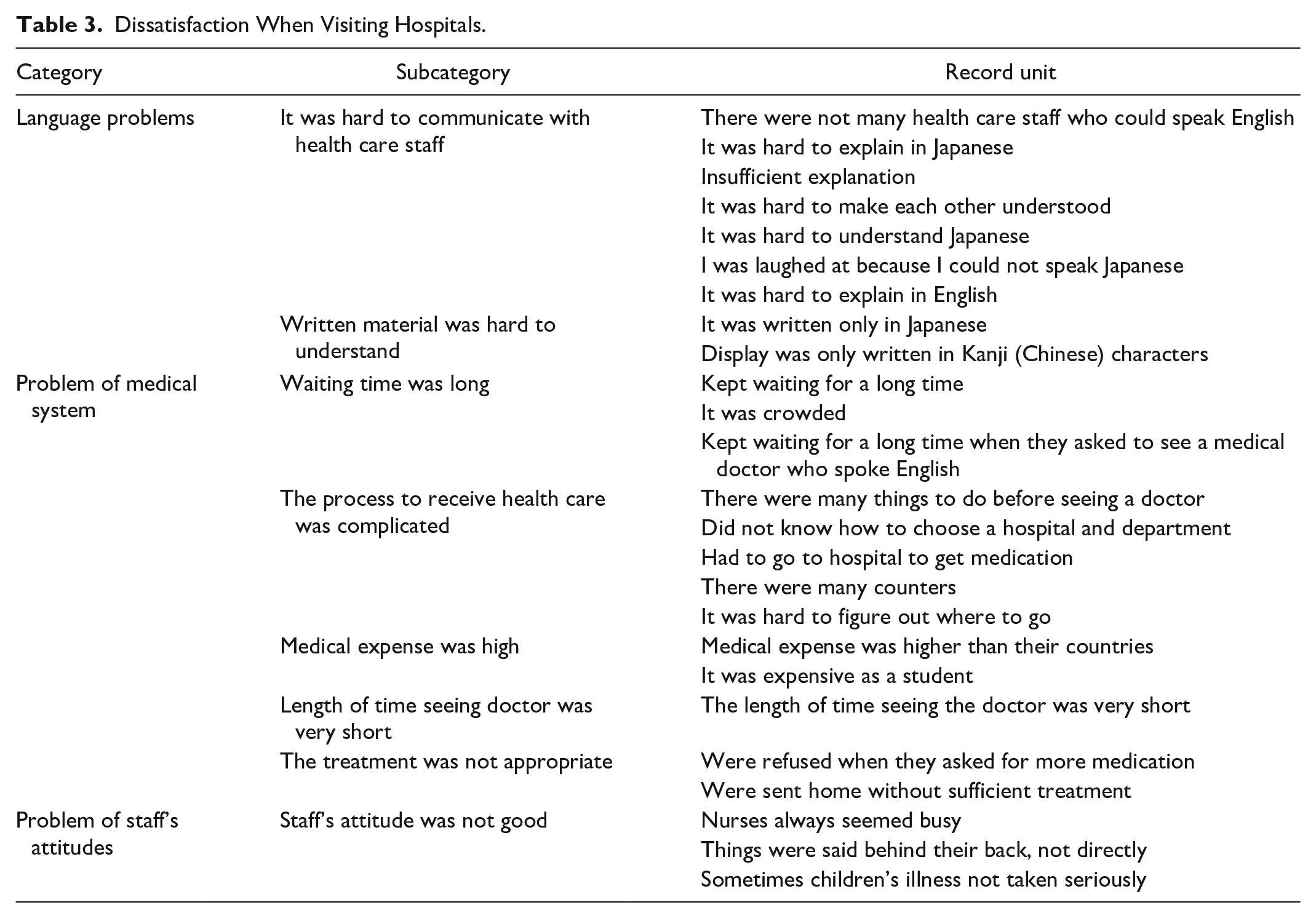
In【Problem of medical system】, participants who answered waiting time was long felt that they had been kept waiting for a long time if they had not made an appointment. They also felt that they had been kept waiting for a long time when they asked for a medical doctor who spoke English, despite having made an appointment. Participants felt the process to receive health care was complicated because there were many things to do before seeing a doctor such as repetition of receptions and examinations. There were many counters and it was hard to figure out where they should go. Participants also stated that the differences between Japan and their own countries made them feel that the process to receive health care was complicated in Japan. For example, some medications are not available without prescription in Japan, or patients can choose hospitals without reference letters in China and Thailand.
“If you make a reservation with a doctor who can speak English, it needs around a week for examination.” “We have to go through many procedures to get the surgery. So we have to meet a doctor, and then go to x-ray and next day I will take CT scan, it takes one month or two months before surgery. I don’t want to take the procedure.” “They need to wait for a long time at pharmacy to get medicine, not in the hospital. I think hospital is so fast. But waiting at pharmacy to get the medicine is too long.” “The system for buying the drug is very difficult. Because we have to get the prescription from the doctor and then go to the drug store, not the private drug store but the public drug store from order to order. So it is very difficult.”
All participants felt that medical expenses were high despite having Japanese national insurance, compared with the medical expenses in their own countries, and because they were students with low income. They felt that the time of seeing the doctor was very short after a long time waiting. They felt that the treatment was not appropriate because they were refused when they asked for more medications or they were sent home without sufficient treatment.
“Medical expense was too expensive compared with my country. For student here I use scholarship you know, but still it’s kind of expensive.” “It was so short check-up to check my nose and throat, and then physical check-up.” “They sometimes are not willing to give you much medication.”
【Problem of staff attitudes】included that nurses always seemed busy, or that staff attitudes to foreign patients differed from those to Japanese patients. Participants felt things were said behind their back, not directly and felt they were discriminated against as foreigners.
“Nurses are so busy, sometimes rushing.”
What Do They Feel Different in Japanese Health Care From Their Own Countries?
What differences in health care from your own countries did you perceive?
The differences in health care system between Japan and participants’ own countries were classified into five categories: 【medical expense/insurance】, 【process of receiving health care】, 【how foreign patients are dealt with】, 【treatment】, and 【attitudes of staff】 (Table 4). 【Medical expense/insurance】concerns use of a national insurance system in Japan, percentage of patients’ out-of-pocket money, and difference in prices. In【process of receiving health care】, participants reported the differences in how hospitals were selected or the payment system. Regarding【how foreign patients are dealt with】, participants reported that, unlike Japan, health care staff speak English when they see foreign patients at hospitals in China, Myanmar, India, and Thailand.
“We are in Japan and we have some insurance especially for kids. It is almost for free. But in my country, it is from your own money.” “In China we can go to the hospital directly. No recommendation paper.” “In China, we need to pay little money first to see the doctor like the clinic fee, then we can go to see the doctor, after we were seen by the doctor; treatment or prescription, they will charge at your card so we will go to the payment center again.” “In Thailand, actually the medical staff especially doctor, maybe they all can speak English. Almost all nurses can speak English. But the level is different by person.” “Most of the drugs are come from foreign countries so all have the English description.” “For cancer patients, we have no radio therapy machine, so there are too many waiting patients. Some people die during waiting.” “In Thailand, we can get drug from any drug store. If we know the name, we can get by ourselves.”
Difference From Participants’ Own Countries.

What differences in culture from your own countries did you perceive?
They felt difference in 【personality】, 【custom】,【religion】, and 【respect for others】in Japan. Description of【personality】included the following: “In Japan, hospitals are always quiet. Chinese people tend not to be so quiet all the time. Here, in our university hospital everybody just like sitting quietly on the sofa and waiting the number watching the screen.” “People try to help. I feel.” “You can make a reservation very exact time. Very punctual. It is ruder in Vietnam.” “Conversation of healthcare staff here is official and formal rather than friendly.”
Description of【custom】included the following: “The family stay at the hospital and take care for the patient, if we have a private room. In Thailand the hospital has many rooms for patients. Some is the shared room, and many patients can stay together.”
Description of【religion】included the following: “Usually in India, we don’t prefer to eat beef or pork. Chicken or fish or ram is ok. But here, I eat everything. No problem. I can eat but I don’t prefer.” “The female doctor is better. I told them I want to be seen by a female doctor but when I gave birth, they were all men. My husband didn’t say anything but he didn’t feel happy.”
Description of【respect others】included the following: “Compared with China, patients in Japan can receive more respect.”
How Do They Cope With the Difficulties and What Do They Desire Japanese to Improve Health Care?
How did you cope with the difficulties?
Strategies to overcome difficulty in hospitals were mainly related to language and were classified into six categories: 【use nonverbal communication】, 【prepare elaborately before visiting hospitals】, 【speculate】, 【ask for help】, 【check terminology as needed】, and 【confirm later】.
In【use nonverbal communication】, participants used gestures and read facial expressions. In【prepare elaborately before visiting hospitals】, they prepared the explanation of their symptoms in Japanese to avoid trouble at the hospital.
“I will prepare when we go to the hospital. I will search online and how to explain my problem before going to the hospital. Prepare in Japanese.” They attempted to understand and【speculated】what healthcare staffs were saying based on their language ability. “When they explain something to me and I do not understand very well, I just guess.”
【Ask for help】included asking family members who speak Japanese to accompany them, calling friends for help, and asking for health care staff who speak English.【Check terminology as needed】meant that participants tried to communicate using the internet and/or dictionary for translation.
“I use Google translation to say my condition.” “I use the dictionary on the application.”
【Confirm later】meant that they voice-recorded explanations and relistened to some parts at home to try and understand.
“Sometimes I would record them. Come back home and I checked with my husband what they said.”
How would you desire Japanese health care to be improved?
Their desires for health care in Japan were classified into three categories:【dealing with English】, 【making the process of receiving health care efficient】, and 【coping with a different culture】(Table 5).【Dealing with English】could be classified into three subcategories: English training for health care staff, use English display and documents, and use interpreter services. In the subcategory English training for health care staff, they desired that health care staff in each section, not only in the department of international health care, be efficient at general communication and using minimal medical terminology in English. Some participants recommended facilitating English communication by using all English textbooks and providing more opportunities to speak with international students in English from the time of student enrollment. Others said that some Japanese health care staff tried not to speak English despite being able to, so they should be challenged more.
“I think it’s better generally try to improve English of staff in every department, not just depending on a specific department.” “It will be better if the medical staff can speak English, but I will not ask them such.” “I don’t expect the country to all change the languages because of some foreigners. This is I think not practical. But Japan will have the Olympic. Maybe it will be better.” “Japan has good medical service, if you can communicate in English well with foreigners, the medical care will be more improved.”
Desire for Health Care in Japan.

Regarding use English display and documents, they desired at least English-language documents, particularly explanation of treatments and medications, which are vital to understanding. In addition, while they sometimes do not understand spoken English, they may understand written English. They desired that all displays on hospital walls be in English.
“Usually I saw the form in Japanese, they don’t have English form. So if they have two languages, it is more easy to understand.” “. . . basically like the directions or where you should wait or something. I think there might be English sign.”
Regarding use interpreter services, they needed English interpreters with medical knowledge or translation software, because difficult medical terminology is used often.
“If some basic English service can be utilized in each department, it will be easier for them.” “I think interpreter service is necessary, but if the patient can speak English, it may not be necessary.” “Someone helps or some machine for translation allow you to make things better.”
Desire for【making the process of receiving health care efficient】included information/explanation about how to choose hospitals and clinical departments, and more conscientious explanation of where they should wait and go, not only as a display, so that foreign patients can understand well. They had to attend hospital to get medications that are available over the counter in their own countries; therefore, they desired that more over-the-counter drugs be made available.
“Make guideline for selecting different section of the hospital.”
For【coping with different culture】, they want to be asked about their religious customs such as taboos on eating some foods or preference for female doctors because it is not desirable in some cultures for a woman’s body to be seen except by her husband. One participant who requested a female doctor said that she and her husband were unhappy because only male doctors were available during delivery. Some participants requested places for family members to stay in hospitals because in Thailand, family members care for patients.
Discussion
This is the first exploratory study reporting experience of international students—mainly Asian, approximately 30 years old, medical background, and could speak English and a reasonable level of Japanese—to identify some of the issues for future research regarding health care in Japan. International students were mainly introduced to hospitals from the university or friends. They were satisfied with the effectiveness of medical system and kind attitudes of staff. They were especially satisfied with the smooth process to receive health care. However, they were also dissatisfied with problems of language, the complicated health care system, and staff attitudes. They had particularly difficulty with communication due to language barriers and needed to be accompanied by friends or family who spoke Japanese. The major differences from their own countries were medical expense/insurance, process to receive health care, and use of English for foreign patients. They also felt cultural differences like Japanese hospitals being silent, a respectful and formal environment, family not being permitted to stay with patients during hospitalization, and less religious custom. They made an effort to use nonverbal communication to solve language problems, but their major desire for health care in Japan was related to language. Participants hoped that staff could have English training and that documents could be provided in English.
Previous studies reported the two major issues for foreign people who visit Japanese hospitals were language and culture (Fortier et al., 2016; Usui, 2013), but the major issues for international students in this study were differences in language and health care systems. Although cultural difference was not reported as dissatisfaction, coping with different cultures was included in desired changes for health care in Japan. Watanabe and Sakka (2017) reported problems with privacy and confidentiality, but in this study participants were satisfied with privacy observation. Regarding mismatch in expectations in Watanabe and Sakka (2017), there were mixed results: Some reported smooth process for seeing a doctor was better than their expectations, but others reported waiting time was long and process was complicated.
Language Barriers and Interpretation
In this study, no participants were native English speakers, but they desired to communicate in English or through English interpreter services although a participant reported difficulty in explaining both in English and Japanese. This may be because they considered that interpreter services in their native languages were not available. They also desired staff in each section to communicate in general English rather than being treated in a specific department of international health care, possibly because they wanted to communicate with their health care staff directly. The Japanese government has been encouraging English education to cope with globalization (Ministry of Education, Culture, Sports, Science and Technology—Japan, 2015, 2018). Many previous studies have also reported the necessity of English training for health care staff (Chiba & Nakayama, 2016; Willey et al., 2016), but most nurses’ level of English remains insufficient to adequately communicate with patients. Kambayashi et al. (2020) reported more than half of nurses in a university hospital and a general hospital in Tokyo answered they cannot speak English at all, and only less than 10% of them answered they can hold basic daily conversation in English. They also reported that most necessary training for nurses to care for foreign patients was foreign language training followed by learning how to cope with different culture. The language training the nurses most wanted to take was daily conversation in English, followed by Chinese and Korean (Kambayashi et al., 2020). Tokyo-to Nursing Association (2020) has foreign language training of English, Chinese, and Korean. Nurses can utilize these programs to improve their foreign languages.
The dissatisfaction due to seemingly inappropriate treatment reported by a participant could stem from the shortage of explanations regarding necessary prescriptions and treatments. Participants took friends and family members with them because they feared having communication trouble with health care staff. However, it is not desirable for people who are not health care workers to play the role of interpreters because they may not be able to interpret precisely and patients may conceal information to protect their privacy (Nagata et al., 2010). In the United States, federal law requires interpreters for patients who speak limited English, but it was still reported that nearly one third of U.S. hospitals fail to offer the service (Cohen, 2016). According to Ministry of Health, Labor and Welfare (2017), only 12.7% of 1,710 hospitals used medical interpreters’ service even though the survey was conducted with hospitals that accept foreign patients selected by Japan Tourism Agency. In the same survey, the most frequent language used to see foreign patients was English (56.8%), followed by Chinese (26.6%) and Japanese (26.0%) (Ministry of Health, Labor and Welfare, 2017). When hospitals do not have their own interpreters, they can use free emergency telephone interpreter services in Tokyo for English, Chinese, Korean, Thai, Spanish, and French although other than English and Chinese are not available for 24 hr or on weekend (Bureau of Social Welfare and Public Health, n.d.). A specified nonprofit organization also has similar telephone interpreter services and medical documents in nine different languages that can be freely downloaded (AMDA International Medical Information Center, 2009). These services should be introduced and used for emergency care or important explanations (e.g., informed consent). However, it is unrealistic to provide interpreters for patients who are hospitalized with 24-hr care. Therefore, it would be desirable for nurses to be able to speak at least basic daily English.
It is also desirable for foreign residents to be able to speak Japanese well. However, despite more than half of participants living in Japan for over 4 years, the self-reported level of Japanese writing and speaking proficiency was low (Fortier et al., 2016). The number of foreign visitors is over 10 times greater than foreign residents, and the Japanese government aspires to increase tourism. Because it is unlikely the tourists speak fluent Japanese, attracting more tourists requires a better care system to accommodate foreign people when they become sick.
On the contrary, participants were satisfied with medical doctors who spoke in English and with the kind attitudes of staff. Participants who were dissatisfied with communication stated that only a few other health care staff including nurses could speak English. Nonaka and Higuchi (2010) reported nurses who had previous negative experience with foreign patients and awareness of their poor language skills had lower confidence in interacting with foreign patients, although they had a strong wish to understand patients from diverse cultures and to provide appropriate nursing care. Nurses, who spend more time with patients than any other health care staff, play an important role in caring for foreign patients (Futami & Hori, 2016). Improving nurses’ English is indispensable for understanding different cultures (Chiba & Nakayama, 2016). Therefore, not only kind attitudes but also more effective and practical English education is necessary in nursing programs so nurses can actively communicate with foreign patients, rather than depending on medical doctors.
Regarding English education in Japan, English-language learning used to start in junior high school, but English activities began introduction in fifth and sixth year in elementary school in 2011, which was also introduced for third- and fourth-year students, and English became a regular subject for fifth- and sixth-year students in 2020 (Ministry of Education, Culture, Sports, Science and Technology—Japan, n.d.). English is taught in nursing programs as well, but requires fewer credits than high school, and the hours and quality of English education may not be sufficient (Willey et al., 2016). It is necessary to have more opportunity to use English on a daily basis like communicating with foreign teachers and international students. It is not only Japan that has difficulty in nursing English education. Kim et al. (2020) reported that nursing undergraduate students in Korea did not think the English curriculum was adequate to sufficiently assist future foreign patients. They indicated team teaching, not only by native English teachers but also with a nursing expert, is the most effective.
There are patients who do not speak English, especially low-skill workers in Japan. In the United States, Sobel and Metzler Sawin (2016) reported that even speaking one or two words of Spanish goes a long way toward establishing connectedness with patients although it is apparently easier when nurses can speak fluent Spanish. It would be quite difficult to master more than one foreign language for Japanese people, but learning one or two words of foreign languages in addition to English would be helpful to establish connectedness with patients who do not speak English or Japanese, in addition to using interpreters.
Doctor–Patient Interactions
Simultaneously, some participants reported poor staff attitudes as they seemed to discriminate against foreign patients and felt doctor explanations were inadequate. This is similar to Fortier et al.’s (2016) report that most doctors communicate basic information and respect patients, but many doctors do not explain conditions or respond enough to questions. In Teraoka and Nonaka’s (2017) study with foreign residents who could speak Japanese, participants reported medical doctors did not talk with them in a satisfactory way and seemed to have barriers with foreign patients. Their participants reported health care staff seemed to immediately assume foreign patients would not understand, even though details were explained in Japanese with consideration of preconceptions caused by differences in physical appearance. Health care staff should not simply judge the patient does not understand Japanese because the patient does not look like Japanese, but should judge the patient’s Japanese ability. This could be also related to language barriers. When you explain in foreign languages, the explanation may be simplified, so when detailed explanations are required, a professional interpreter would be most beneficial.
In this study, while some participants felt they were not treated equally to other Japanese patients, no participants reported they were not treated as having an equal position to medical doctors, unlike Watanabe and Sakka’s (2017) study, where participants felt doctors were in higher position than patients (e.g., paternalistic, little emphasis on equal partnership). This may be because Asian as well as Japanese patients generally consider medical doctors’ status to be higher than patients, and participants did not feel uncomfortable with the situation as Watanabe and Sakka (2017) discussed.
Basic Communication
Regarding basic communication, Fortier et al. (2016) reported respondents had difficulty with basic administrative communications, such as untranslated signs, forms, and other documents, similar to desired health care changes reported in our study, including English display and documents and information/explanation. Some participants stated the process of receiving health care was smooth, but others stated that the process was complicated. This may be due to the differences in health care systems from participants’ own countries. One participant stated they had to pay twice in China, both before and after treatment, which took more time than the system of paying just once in Japan. However, the system in Japan whereby the medical fee is calculated after completing treatment sometimes leads to troubles with foreign patients (Futami & Hori, 2016). For example, patients found they could not pay expenses when charged after the treatment; therefore, an approximate fee should be explained before the treatment or patients should pay a deposit beforehand if the expense is expected to be high (Futami & Hori, 2016). Foreign patients should be informed of such differences in health care systems in addition to providing language support to ensure smooth health care.
Some claimed there was a long waiting time and short time spent actually seeing a doctor; this feeling is not specific to foreign patients but shared by Japanese patients. Although the situation is the same, foreign patients may have a specific anxiety (Hayashi & Mori, 2003), which could be reduced if such details were explained to them.
In this study, some participants were satisfied because they felt their privacy had been protected. However, Watanabe and Sakka’s (2017) research, where the majority of participants were from Western countries, reported that all participants were worried about privacy and protection of personal information when they visited hospitals in Japan. In particular, care taken to minimize the exposure of body parts in the gynecological examination was not sufficient. The previous online survey reported the median level of satisfaction when visiting hospitals was lower for female (61%–80%) than male participants (81%–100%) (although the likely reason was inadequate care for Muslim women, this was not made clear in the study; Kondo, 2018). It is possible that care for privacy in Japanese hospitals is inadequate compared with Western countries.
Finding and Receiving Health Care
Fortier et al. (2016) reported language and cultural difficulties complicate the process of receiving health care. International students can consult the international department and students’ health care center at the university. However, they still had difficulty going through the health care process, and desired information/explanation about how to choose hospitals and clinical departments.
Eight out of nine participants had religious beliefs unfamiliar to Japanese people. Religious customs such as food and prayer rooms should be considered (Agency for Cultural Affairs, 2013; Ministry of Internal Affairs and Communications, 2017). The level of obeying religious practice observed differed among participants; some continued their religious customs while in Japan, others did not. It is necessary, therefore, to ask not only whether they have religious beliefs but also their current customs and to respect those customs. To prevent misunderstandings, the language problem must be solved. As a religious consideration, care for Muslim people is necessary (Futami & Hori, 2016). Muslim women seeking maternal care usually prefer female physicians. If they are not given the option of same-sex health care staff, the necessary care can be delayed (Shahawy et al., 2015). Health care staff have to learn and understand different cultures and values to cope with diversity (Leininger, 2002).
Practical Implications
To relieve language barriers, it is necessary for Japanese health care staff to improve English skills and learn some other languages by attending language training courses; for Japanese schools to improve English education (e.g., team teaching); for Japanese hospitals to introduce interpreter services, to use available services including foreign language documents, and have English displays; and for foreign people to learn some medical Japanese terms when they come to Japan.
It is necessary for Japanese universities to inform international students of available health care resources at the university and to explain the medical systems in Japan.
It is necessary for Japanese health care staff to learn and understand cultural differences and needs, try to explain to foreign patients as detailed as to Japanese patients, and make preparations in advance to cope with diverse patients (e.g., patients who ask for female doctors or specific food).
Limitations and Suggestions for Future Studies
The study sample comprised just nine graduate students who agreed to participate in a university. We could not interview more students because of time constraints and could not confirm saturation. Transferability may be limited to a specific group of international students. Despite being graduate students in a health care university, they had difficulty using Japanese medical technical terms. Foreign people who do not speak English or Japanese would likely have even more difficulties. We did not ask specifically which hospital/clinic participants attended, but they mainly went to hospitals/clinics introduced by the university or friends, which were considered to be relatively accessible for foreign patients; however, problems were still reported. It is necessary to investigate experiences of international students in majors other than health care, foreign residents who do not speak English or Japanese, and those with experience of hospitalization with severe conditions to clarify the various health care needs of foreign people. It is also necessary to investigate the relationship between level of satisfaction with health care and protection of privacy.
Conclusion
This study investigated the experiences of hospital visits as reported by international students in a medical university in Japan. While they were satisfied with the health care system, with its smooth care and kind staff, they also had difficulty communicating with staff and receiving health care due to differences from their own countries. Participants desired that Japanese health care staff speak English, as well as have English interpreter services. It is necessary to improve staff’s English skills, provide English documents, provide multilanguage interpreter services, and explain medical system procedures in Japanese hospitals.
Footnotes
Acknowledgements
This study was conducted as a graduation thesis in Nursing Science, School of Health Care Science at Tokyo Medical and Dental University in 2017, which was conducted using Internatioal Nursing Development’s field cost of the university, and was partly presented at 2nd Academic Conference of Japanese Society for International Nursing in 2018.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.