
Abstract
In Shanghai, one of the biggest modern cities in the world, community-based health care providers are largely underutilized. As a result, valuable medical resources are wasted. The present study examined the relationship between the variables of perceived risk and patient anxiety on intentions to use community health clinics, because these two variables are closely related to decision making. A survey measuring these variables was distributed near community health clinics in Shanghai (n = 869), and structural equation models were constructed to analyze the data. Results show that patient anxiety was associated with contracting diseases and positively related to the intention to seek services from community-based providers, whereas their perceived risk of these providers had a negative relationship with such an intention. Moreover, the knowledge that some community clinics were not as good as large hospitals was positively related to perceived risk. Policy implications are discussed based on the findings.
Introduction
Shanghai is one of the biggest modern cities not only in China but also in the world. As of 2017, Shanghai had a population of more than 24 million and a gross domestic product (GDP) of 469 billion US dollars (Zhou, 2018). Despite the economic boom, the health care situation has been critical in Shanghai. For example, the aging population has kept growing in Shanghai. As of 2017, a total of 4.84 million residents in Shanghai were aged 60 or over (Shi, 2018). The growing aging population has been placing substantial pressure on the city’s health care system.
To cope with such a critical situation, Shanghai has invested significantly in the health care sector. For example, in 2017, the Shanghai municipal government spent over 6 billion US dollars in health care (Shanghai Municipal Government, 2018). As of April 2018, Shanghai has established more than 5,000 medical institutes, including 360 hospitals and 4,593 community-based clinics (National Health Commission of the People’s Republic of China, 2018). Notably, since 1950s, Shanghai has had a long tradition of investing in community-based clinics because these clinics are convenient for residents seeking timely treatments, physical examinations, health care education, vaccinations, and other medical services (Statistical Bureau of Shanghai, 2018; Xu, 2008). Despite this investment, a dilemma in decisions to seek health care has come to light in recent years. A recent survey conducted by the Shanghai municipal government found that more than half of responders were reluctant to seek services from community-based clinics. As a result, high-cost hospitals remain overloaded with patients, while low-cost and convenient community health care providers do not receive an adequate number of patients (Statistical Bureau of Shanghai, 2018). In addition, a more recent study found that in Shanghai, about 82.49% of health care services were provided in large hospitals; in contrast, 12.79% of health care services were provided in community-based clinics (Li et al., 2018). Thus, investment and policies made by the municipal government were inconsistent with patients’ choices.
Community-based clinics and their services have their advantages. Most diseases that patients seek treatment for from large hospitals are common or frequently occurring and can be treated by community health care providers. As a result, about 65% of out-patient care and 77% of inpatient treatment in large hospitals could be transferred to community health care providers (Du, 2006). Consistently, the Institute of Medicine has long acknowledged the value of community health care (Donaldson et al., 1996). That is, community health care providers not only offer medical services but also build a strong tie between personal and family health care and communities. This dilemma leads to a waste of valuable medical resources.
The present study aimed to advance our understanding of this dilemma from the perspectives of psychology and medical decision making. More specifically, the study examined the psychological factors that are associated with utilizing community health care providers. Although the current study focuses on Shanghai, the implications generated from the study can be applied to other regions. First, urbanization and aging are happening all over the world, particularly in developing countries (Shetty, 2012). As a result, their health care systems face significant challenges (Durrani, 2016). Second and more importantly, underutilization of community health care services occurs not only in Shanghai but also in other areas in China, Bangladesh, and even the United States (Diamond, 2017; Qian et al., 2010; Yaya et al., 2017). Therefore, the implications and lessons learned from Shanghai in the current study may also be applied to other regions in the world.
Theoretical Background and Hypotheses
The present study aimed to unpack the dilemma faced by the community clinics in Shanghai. To this end, the study focused on two variables that are associated with people’s evaluation and choice of health care providers: perceived risk and emotion (i.e., patient anxiety [PA]). The variables were chosen based on two perspectives. First, as reviewed below, past research in the fields of public health and medical decision making has demonstrated the relationship between these two variables and health care selection and use. Hence, it is reasonable to test the role of perceived risk and PA to advance our understanding of the patient choice dilemma in Shanghai described above.
Second, the variables of perceived risk and PA have been shown to play a role in judgment and decision making, including consumer choices (Zhao et al., 2015, 2019). For example, Grewal et al. (2007) found that perceived risk was negatively related to intention of making a purchase. It is worth noting that seeking and choosing health care services in patients has been associated with the field of consumer behavior (Andereck, 2007; Tomes, 2016). For instance, Reeder described the relationship between patients and physicians as consumers and producers (Reeder, 1972). Thus, from the perspective of consumer behavior, we predicted that perceived risk and PA will be associated with intention to use community clinics. Hence, based on research on both health care and consumer behavior, the present study aimed to understand the underutilization of community health clinics (CHCs) in Shanghai by examining the role of perceived risk and PA as well as other factors. We detailed our hypotheses below.
Perceived risk and intention of seeking community health services
Bauer (1960) proposed that consumers experience risky feelings when they face unexpected consequences for their actions. Thus, how people perceive the potential risk associated with their purchase is associated with their subsequent actions. Accordingly, consumer buying behavior can be considered a kind of risk-reducing behavior, because people strive to avoid or minimize risk during the decision-making process. If consumers cannot reduce the perceived risk, they will abandon the process of purchasing an item (Conchar et al., 2004). For example, perceived risk was found to be the main barrier to online shopping (Mitchell & Greatorex, 1993). Similar to the research on consumer buying behavior, perceived risk has been found to be associated with intention to use medical resources. For example, a negative relationship was found between perceived risk (due to concerns about information quality and/or personal privacy) and intentions to use medical websites and mobile applications (Schnall et al., 2015; Tang et al., 2019).
Furthermore, perceived risk varies based on different kinds of products. Compared to the attitude toward tangible goods, people’s perceived risk toward intangible goods (such as haircuts or car repairs) tends to be greater, because it is more difficult to evaluate the consequences after consuming intangible goods (Popli & Mishra, 2015). Similarly, most people may have difficulty in evaluating the quality of medical procedures during or after their treatment due to their limited medical knowledge. While a majority of studies focus on tangible goods, perceived risk associated with health care services—a kind of intangible good—deserves further investigation. Following the findings stated above, we hypothesized the following:
Disease-related anxiety and intention of seeking community health services
Emotion has long been shown to correlate with decision making (for review, see Lerner et al., 2015). In particular, emotion relates to how consumers evaluate products. For example, consumers in a positive mood tend to use less information to evaluate products when compared to controls (Isen & Means, 1983). By contrast, consumers with anxiety (at a moderate level) seek more information about the products and tend to be more goal-focused (Hill, 2010). That is, anxious consumers are more motivated to achieve their goal by purchasing the product.
Following previous studies, we predicted that emotion will be associated with patients’ tendency to use community health care providers. More specifically, we focused on the anxiety associated with contracting diseases. This was our focus, because in the context of health care, patients who seek treatment due to contracting diseases are more likely to experience anxiety (Salkovskis et al., 2002). In some patients, anxiety and stress prevail when they receive medical surgeries (Gallagher & McKinley, 2007). Moreover, anxiety due to sickness is correlated with patients’ concerns about their health and their treatment-seeking behavior or hospital stays (Herrera-Espiñeira et al., 2009). Thus, we hypothesized the following:
Relationship between perceived risk and anxiety
Thus far, we have proposed that both perceived risk and PA are related to the intention to use community health care providers. The present study also aimed to clarify the relationship between these two variables. It was proposed that in an uncertain context, emotion is related to perceived risk (Isen & Means, 1983). More specifically, increased perceived risk is related to increased anxiety. For instance, people with greater anxiety were more likely to interpret ambiguous stimuli as threatening and experience more risk (Eysenck, 1992). In another example with community residents, those who perceived more risks in their life events also reported a higher level of anxiety (Tripp et al., 1995). Therefore, we predicted the following:
Health service provider heterogeneity (HSPH) and perceived risk
To comprehensively understand the psychological intention to use community health care providers, the current study also examined two sources that correlate with perceived risk and PA: service provider heterogeneity and health involvement.
Provider heterogeneity is the knowledge of quality differences among different providers (Schmalensee, 1982). Examining a large number of options is positively related to uncertainty and confusion and, in turn, to perceived risk. For instance, Bettman (1973) found that more heterogeneity among goods and services increased difficulty of choice and perceived risk. Similarly, it was found that greater perceived risk was associated with more heterogeneity in six kinds of consumer services (e.g., hairdresser, hotel, bank etc.; Conchar et al., 2004). In the domain of health care, people from different countries list quality as one of the primary factors to consider when choosing providers (Overtveit, 1996; Qian et al., 2010). Furthermore, patients consider poor quality in health care services as a risk to their safety (Lu & Roughead, 2011; Schwappach, 2014). Conceptually, if people perceive more heterogeneity among health care providers, they should be more careful when choosing a health service provider. Therefore, we advanced the following hypothesis:
Health involvement, perceived risk and PA
Heath involvement refers to a person assessing the relevance of health issues according to his or her inherent need, value, or interest (Zuzanna et al., 2008). As a result, a high degree of health involvement may involve greater perceived risk. Consistently, a study with 1,729 U.S. adults found perceived risk was positively related to decisional health involvement (i.e., desire to make decisions about health; Dillard et al., 2010). Therefore, in the context of community health care providers in Shanghai, we predicted the following:
As for the relationship between health involvement and anxiety, the literature is scarce. In one study, female patients showed a more active role than male patients in the decision-making process during health care (hence, a higher level of involvement). Meanwhile, female patients also experienced greater anxiety in this process (Nilsson et al., 2013). Presumably, those who have more concerns about their health may experience more anxiety regarding health. Thus, we predicted the following:
Health involvement and HSPH
As discussed, health involvement correlates with people’s intention to search and process information about health care providers. Those who care more about their health status (hence greater health involvement) are more likely to examine the qualification of health care providers, engage in discussion with providers, and make shared medical decisions (Friedrichs et al., 2016). Additionally, based on the feedback and interaction with patients, patients with greater health involvement can help improve health care quality and health care safety (Sharma et al., 2018). Following these studies, in a conceptual manner, those with greater health involvement are more likely to scrutinize the health care providers and find more heterogeneity across the providers. Thus, we hypothesized the following:
Overview
As discussed, the present study aimed to advance the understanding of the underutilization of community health care providers in Shanghai. While the proposed factors of perceived risk, PA, health involvement, and provider heterogeneity have been tested in the domains of consumer behavior and health care, this study specifically examined their associations with intention to use community clinics in Shanghai. We hope this study will shed light on medical decision making and generate implications for the optimization of health resources. Figure 1 summarizes the variables and hypotheses.
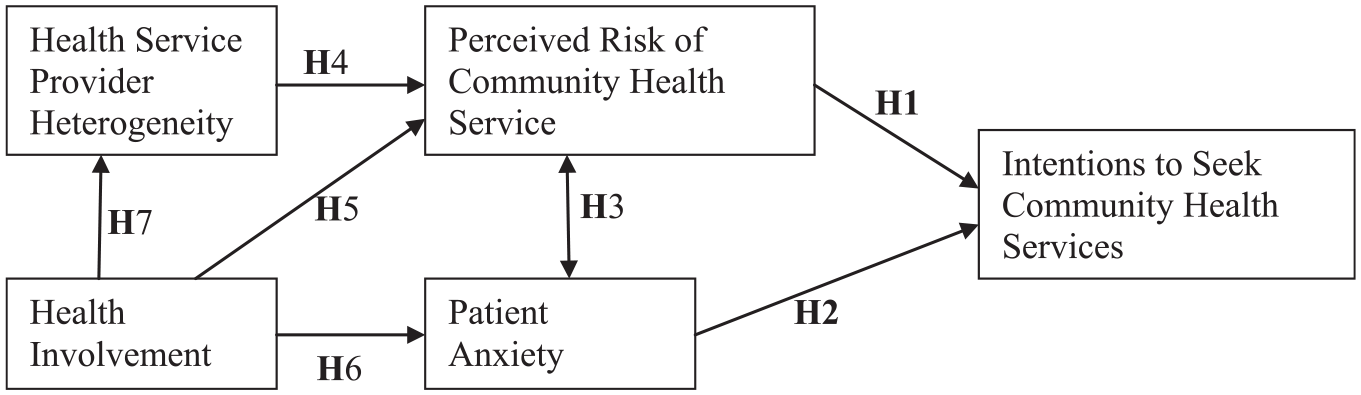
Proposed model that summarizes the hypotheses being tested in the present study.
Methods
Participants
The study adhered to the Belmont Report and was approved by the Academic Committee (i.e., Institutional Review Board (IRB)) at the author’s institution in Shanghai. Trained research assistants handed out a questionnaire in local communities near CHC in all 14 counties in Shanghai to collect data. Participants who completed the questionnaire did so voluntarily and received a gel pen and a pack of napkins as compensation for their time. The survey posed no risks to participants, and they could withdraw from the questionnaire at any time. Participants were debriefed after completing the questionnaire. All records were de-identified and kept confidential.
In 4 months, 869 respondents participated in the study. In addition to the scales measuring participants’ attitudes toward community health care, demographic variables including age, gender, education, income, occupation, and insurance status were also collected. Results of these demographic variables are found in Table 1 of the Results section.
Frequency of Demographic Characteristics of Survey Respondents.

Materials and Procedures
A series of scales were employed to test our hypotheses. These scales were developed and tested in previous studies.
Health Involvement (HI) Scale
HI was measured with a 5-point scale adopted from a previous study (Zuzanna et al., 2008). The scale consists of three items: “Health means a lot to me” (HI1), “I care a lot about health” (HI2), and “Health is very important to me” (HI3) (1 = absolutely disagree, 5 = absolutely agree). Based on the present sample, the Cronbach’s α was .90. Note that all Cronbach’s α described below were generated from the current sample.
Patient Anxiety Scale
The present study focused on PA that was related to contracting diseases. Accordingly, PA was measured with a 4-point self-rated scale (1 = not at all, 4 = very much) tested by Court et al. (2010). Three items were included: “When contracting common diseases, I am tense” (PA1), “When contracting common diseases, I feel upset” (PA2), and “When contracting common diseases, I am worried” (PA3). The Cronbach’s α was .824.
HSPH Scale
This scale was adopted from Burnham and colleagues’ work (Burnham et al., 2003). The scale contains two items: “The quality of service varies a lot between different service providers in this medical industry” (HSPH1), and “Different service providers in this industry offer very different programs/features” (HSPH2) (1 = absolutely disagree, 5 = absolutely agree). The Cronbach’s α was .741.
Perceived Risk of Community Health Service (PR) Scale
The scale of perceived risk of community health service (PR) was adopted from Jacoby and Kaplan’s work (Jacoby & Kaplan, 1972). The scale measures risk attitudes toward qualifications of physicians and nurses and the quality of the services in the CHCs. This scale includes eight items: “Physicians in community health centers have low medical technical level” (PR1), “Physicians in community health centers are less experienced” (PR2), “Physicians in community health centers are less qualified” (PR3), “The attitudes of the community health centers physicians are not as good as expected” (PR4), “Nurses in community health centers have low medical treatment level” (PR5), “Nurses in community health centers are less experienced” (PR6), “Nurses in community health centers are less qualified” (PR7), and “The attitudes of the community health centers nurses are not as good as expected” (PR8) (1 = absolutely disagree, 5 = absolutely agree). The Cronbach’s α was .887.
Intentions to Seek Community Health Services (IS) Scale
This is a two-item scale developed by Zithaml et al. (1996). The scale was used to measure the dependent variable in this study. The items were as follows: “How likely are you to go to community health clinics when you need treatment of common diseases next time?” (IS1) and “What is the chance that you will recommend community health clinics to others?” (IS2). Responses were measured with a five-point Likert-type scale (1 = very unlikely, 5 = very likely). The Cronbach’s α was .757.
Results
Demographic Variables
Across all participants (n = 869), the age ranged between 18 and 89, with a mean and standard deviation of 42.41 and 13.63, respectively. Table 1 shows the results for rest of the demographic variables.
Descriptive Statistics of the Scales
Table 2 presents the means, standard deviations, and correlations of the demographic variables and questionnaires in the present study. Age was positively related to the tendency to use community health care services. Interestingly, the intention to use community health care services was negatively associated with education and income, possibly due to people with higher socioeconomic status tending to use more prestigious services (e.g., large and comprehensive hospitals) as cost may not be a serious concern. There was no relationship between insurance status and the intention to use community health care services.
Descriptive Statistics and Correlations of the Demographic Variables and Questionnaires.
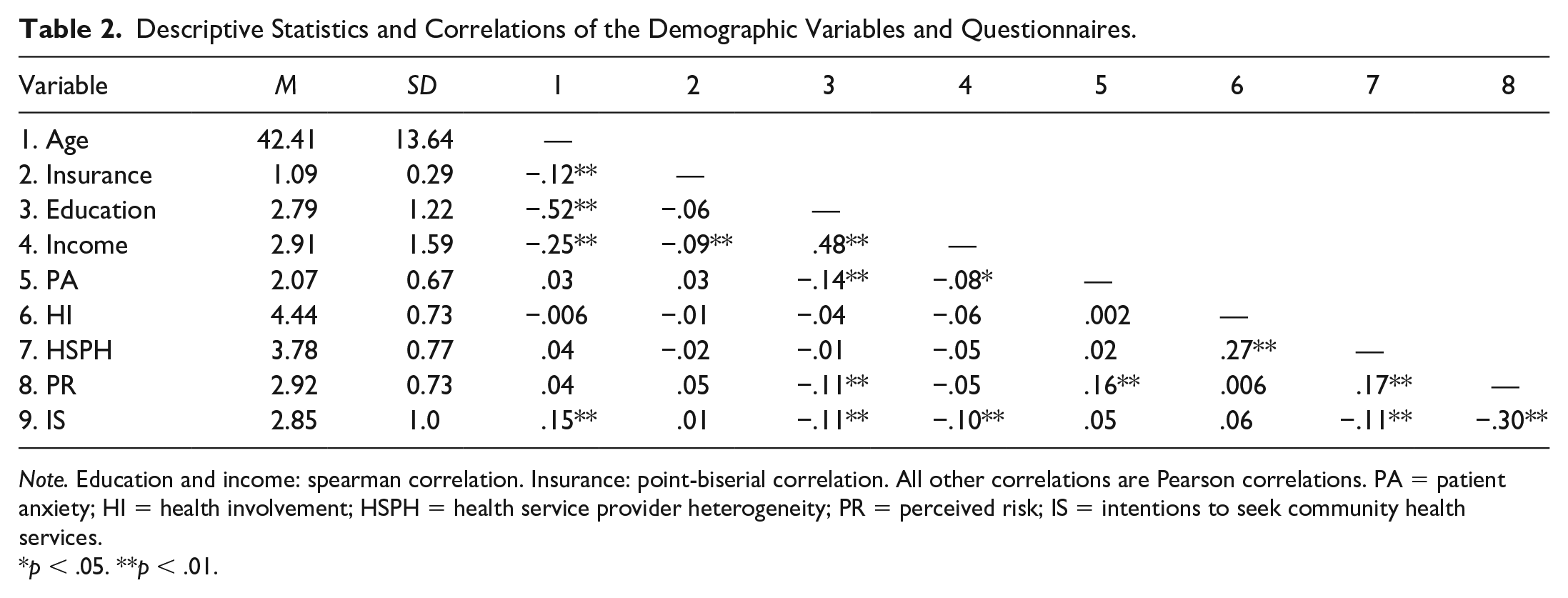
Note. Education and income: spearman correlation. Insurance: point-biserial correlation. All other correlations are Pearson correlations. PA = patient anxiety; HI = health involvement; HSPH = health service provider heterogeneity; PR = perceived risk; IS = intentions to seek community health services.
p < .05. **p < .01.
Testing of Hypotheses With Structural Equation Modeling
With Amos 22, structural equation models (SEM) were constructed to test the hypotheses. The maximum likelihood function was used to fit the model and estimate the parameters. Based on previous literature, the following criteria were used for model fitting: normed χ2≤ 3, root mean square error of approximation (RMSEA) ≤ .10, comparative fit index (CFI), and Tucker Lewis Index (TLI) ≥ .90 (Jia et al., 2017). Figure 2 exhibits the proposed model based on the hypotheses. The model fit the data well, with normed χ2 = 2.85, CFI = .97, TLI = .96, Akaike information criterion (AIC) = 482.8, and RMSEA = .046.

Structural equation modeling demonstrates the relationship between perceived risk and patient anxiety and intention to use community-based health services.
Before interpreting this model, we tested several alternative models to examine the possible relationships between PA, performance risk (PR), and intention of seeking community health care services (IS). First, to further validate association of PA and PR with IS, we eliminated them from the model one at a time and found poor fit. That is, when eliminating the path from PA to IS, AIC increased to 490.2. When eliminating the path from PR to IS, AIC dramatically increased to 565.2. Second, PA solely measured the anxiety caused by contracting disease. Hence, we predicted no relationship between heterogeneity and PA. To empirically test this, we added a path from heterogeneity to PA and found that it was not significant (coefficient = .004, p = .908). Moreover, the model fit was poor, with AIC = 486.8.
As illustrated in Figure 2, the final model confirmed several findings derived from our hypotheses. First, as predicted, perceived risk had a negative relationship with the intention to use community health care services. By contrast, PA that dealt with contracting diseases was positively related to patients’ intention to use community health care services (H2). Second, perceived risk was positively related to PA (H3). Third, health care provider heterogeneity was positively related to perceived risk (H4). Fourth, consistent with H5, those who had a higher level of health involvement perceived greater risk. Inconsistent with H5 and H6, health involvement was not related to either perceived risk (coefficient = -.051, p = .153) or PA (coefficient = -.013, p = .61). Hence, there was no direct relationship between health involvement and perceived risk. This non-significant relationship indicates that the negative emotion that the patients experienced may be associated with fear or anxiety of diseases rather than with a generic attitude toward health. Finally, as hypothesized, those who engaged in a greater level of health involvement perceived more heterogeneity among different health care providers (H7).
Discussion
The health care system in Shanghai is unbalanced. On the one hand, large hospitals are overcrowded, and patients have to spend a significant amount of time and money seeking health care services in these hospitals. On the other hand, patients generally lack sufficient intention to seek health care services from community-based providers, although the government has invested heavily in these providers. Consequently, the affordability of and access to medical resources continues to be an issue.
The present study examined the psychological factors that underlay such an unbalanced system. Specifically, the study tested the association of perceived risk and PA with the intention to use community health care providers. These two factors have a strong relationship with consumer motivation and medical decision making. Not surprisingly, it was found that anxiety related to contracting diseases was positively associated with patients’ intention to seek health care from community-based providers. By contrast, perceived risk was negatively related to such an intention. Importantly, the present study identified that perceived heterogeneity among health care providers correlated with perceived risk. In other words, with greater perceived variability, patients feared that they might select a poor provider over a good one and perceived more risk. Moreover, those who showed greater concern about health (i.e., were more involved) perceived greater heterogeneity across different providers.
The present study generates implications regarding community health care services. First and foremost, the quality of community-based health care services should meet patients’ demands. Although increasing the number of community clinic physicians may result in more health care service opportunities, service quality is a greater concern. In China, most community-based clinics are transformed from local and village clinics, and physicians in these community clinics are less educated and experienced (Yang et al., 2010). Unfortunately, as noted in He et al (2015), data regarding medical malpractice and disputes have been historically poorly documented, prohibitively difficult to obtain and not accessible to clinicians. We also made an inquiry to Shanghai Municipal Health Commission and were informed that no such data was available. Thus, we are not able to provide direct evidence demonstrating that there are higher malpractice, mortality, or morbidity rates in the community clinics than in the large and high-ranking hospitals. However, patients and the public can infer the quality differences based on other clues. For example, in 2018, in comprehensive large hospitals, 51.4% and 20.3% of physicians had a bachelor or an advanced degree, respectively. In contrast, in CHCs, the percentages of physicians who had a bachelor or an advanced degree were 45.1% and 3.3%, respectively (Chinese Public Health Yearbook, 2019). Thus, the public may perceive quality in the CHCs poorer than high-ranking hospitals.
Hence, in addition to simply increasing the number of community physicians, increasing the quality of community health care services is crucial. There are several approaches to address the quality issue. First, as reported by World Bank, sending physicians to large and high-ranking hospitals could significantly improve their professional skills (Liang & Langenbrunner, 2013). Second, physicians, including ones working in the community clinics, are required to pursue continuing medical education (CME), including online education. These physicians are required to participate in CME organized by medical institutions at national, provincial, municipal, and district levels to fulfill at least 25 credits each year. CME is used to keep high professional morals, improve skills, and meet the public demands. Performance on CME is taken into consideration for staying license and promotion (Miller et al., 2015; Wong et al., 2017). Third, inviting experts from large hospitals to act as guest physicians in community-based clinics can provide quality services to local residents in a convenient manner (Xu, 2008). In addition, it is beneficial to strengthen referral so that it is easier to transfer patients from community clinics to large hospitals if necessary. This approach has achieved success in urbans areas in the United Kingdom (Starfield, 2012).
The second implication relates to the role of government. In mainland China, the vast majority of community clinics were government funded. Private CHCs only accounted for a marginal share and decreased in its number (Wei et al., 2015). On the one hand, the central and local governments have invested heavily in supporting community clinics. For example, by 2015, there had been more than 34,000 government-funded CHCs providing essential health care services to 706 million people (UNAIDS, 2017). On the other hand, while capital investment is important, our results suggest another psychological implication based on the relationship between perceived heterogeneity and perceived risk. That is, if someone is not familiar with the services provided by the CHCs, she or her is likely to perceive the risk and ultimately decide not to use the CHCs. For example, a lack of understanding and trust toward the CHCs was found in Chinese residents (Pan et al., 2006; Wu et al., 2017). Also, in Pan et al. (2006), fewer than half of Chinese responders knew that CHC provided rehabilitation services and health education. Thus, in addition to capital investment, local governments should also play a role in promoting community-based health care services. For example, local government should use more resources (e.g., television, radio, newspapers) to introduce community-based health care services, including first contact and accessible care, continuity of care, integrated care for multiple health needs, and coherent links with secondary care (Starfield, 1992). More importantly, standards about the community clinics should be established and made clear to the public.
In addition, community outreach is beneficial because it can enhance people’s understanding of common diseases and relevant treatments available in community clinics and, in turn, increase patients’ motivation to visit such clinics. Take, for example, in southwest China, after officers and volunteers visited and promoted CHCs in 7 townships and 49 villages, there was an increase in utilization of child health care, postpartum care, and chronic disease care services provided by these clinics (Yuan et al., 2012). Similarly, in Miami-Dade County in the United States, the community outreach program called Living for Health was found to motivate residents to access and utilization of community health centers (Almufleh et al., 2015). Moreover, advisory platforms (e.g., health care hotlines) and family doctors can also play consulting roles in helping people understand the function of community-based health care providers (Xu, 2008).
With modernization and a growing aging population, the health care dilemma faced by Shanghai also occurs in other regions of the world. Therefore, the findings generated in the present study have potential implications for other regions. Future studies can test whether the findings can be replicated in other big cities all over the world, particularly in developing countries.
This study discovered some novel findings; however, two limitations should be addressed. First, the study was a correlational one and results should be interpreted with caution. For example, whereas we found a negative relationship between perceived risk and the intention to use CHCs, more causal evidence is needed to demonstrate that greater perceived risk leads to a reduced intention to use CHCs. Second, although the present study uncovered the relationship between anxiety and the intention of seeking health services, the broad role of emotion in treatment seeking remains unclear. The scale used in the study solely focused on the anxious feeling that was associated with contracting diseases. Thus, it is not clear whether greater perceived risk toward the community-based health care providers results in a higher level of anxiety (or other types of emotion) and subsequently reduces the intention of using these providers. Future studies should use more comprehensive scales to examine the role of emotion in medical decision making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.