
Abstract
New Jersey has made significant investments in their creation of a “statewide” reform to better serve the most vulnerable children and their families. Many states can learn from New Jersey’s statewide reform, which now celebrates completion of its first decade. This article details the historic timeline of the implementation processes as well as the structural components of a system of care. The particular role of each system entity is identified as well as their adaptation of the Child and Adolescent Needs and Strengths (CANS) assessment tool to best serve the children/youth in a statewide system of care. This article also examines the methods for effectively training and embedding the CANS tools within New Jersey’s Division of Children’s System of Care (DCSOC). As the children’s system of care (SOC) celebrates a milestone and its second decade of existence, much data have been accumulated with the next logical step being a series of reviews and systemic update. Result shows the need for planning for transitioning to adulthood especially among a population profile or 16 years and older, which we referred to as “emerging adult” population.
Keywords
Introduction—Implementation of Statewide System of Care
New Jersey’s transformation of its children’s mental health system dates back to 2000 when the Department of Human Services expanded services to serve a “broad” range of children population, including those with high-level emotional and/or psychological challenges that may be at risk of being removed from their home. In 2001, the state created a new infrastructure to include necessary components, services, supports, policies, and procedures while realigning existing services through its Children’s System of Care Initiative or Partnership for Children. Subsequently, the Office of Children’s Services was formed with a new operating system called the Division of Child Behavioral Health Services (DCBHS) to integrate strategies needed to establish the variety of components of this new child-serving “system of care” (Caliwan & Furrer, 2009). A glossary of acronyms with definitions can be found in the appendix.
The Department of Children and Families (DCF) in July 2006 became the first cabinet agency whose mission was devoted exclusively to serve and safeguard the most vulnerable children and families in the state (DCF, 2012a). In July 2012, New Jersey established the Division of Children’s System of Care (DCSOC), formerly the DCBHS, and realigned services for children/adolescents with developmental disabilities, substance abuse, and emotional/behavioral health care challenges and their families (DCF, 2012a).
The original system of care concepts offered by Stroul and Friedman (1986, 1994) were used as a guide for reforming child-serving systems in New Jersey, providing a framework to effectively address the service and support needs of children and youth with significant mental health challenges and their families. The original focus of the system of care philosophy or framework was not to establish a new service delivery “model” or “program,” but rather a “paradigm shift” (Stroul, Blau, & Friedman, 2010). New Jersey’s DCSOC is designed to function in a manner consistent with Stroul et al.’s (2010) updated definition of “system of care”: A spectrum of effective, community based services and supports for children and youth with or at risk for mental health or other challenges and their families, that is organized into a coordinated network, builds meaningful partnerships with families and youth, and addresses their cultural and linguistic needs, in order to help them to function better at home, in school, in the community, and throughout life. (p. 6)
Nearly every state has incorporated aspects of system of care philosophy within their child-serving entities (Stroul et al., 2010). However, as Hodges, Ferreira, Israel, and Mazza (2010) point out, since the inception of this concept more than 20 years ago in response to the crises of “inadequate and fragmented services for children with serious emotional disturbances,” there is no universally agreed upon or shared understanding of systems of care. The fact is that the concept of a “system of care” was developed as an organizational philosophy used to increase collaboration across agencies, families, and youth with the ultimate purpose of improving and expanding the array of services and supports for children with serious emotional disturbance (Hodges et al., 2010).
New Jersey’s DCSOC provides families throughout the state a virtual single point of contact for needed services and supports. The role of the Contracted Systems Administrator (CSA) is to serve as this entry point with a toll free number that is managed 24 hr a day, 7 days a week, 365 days a year to register, track, and coordinate care for children and families. The needs assessment (NA) received by the CSA determines the intensity of services provided for a child/youth and their family. Once a clinical determination has been made, a child/youth is connected with an appropriate level of services which the CSA monitors throughout the length of system of care involvement. The core “system of care” partners are as follows: Unified/Care Management Organizations, Family Support Organizations (FSOs), Youth Case Management (YCM) Services, and Children’s Mobile Response and Stabilization Services (CMRSS; PerformCare, 2012; see Figure 1). Each of these entities exists in all 21 counties and/or regions in the state to ensure a consistent and seamless continuum of care.
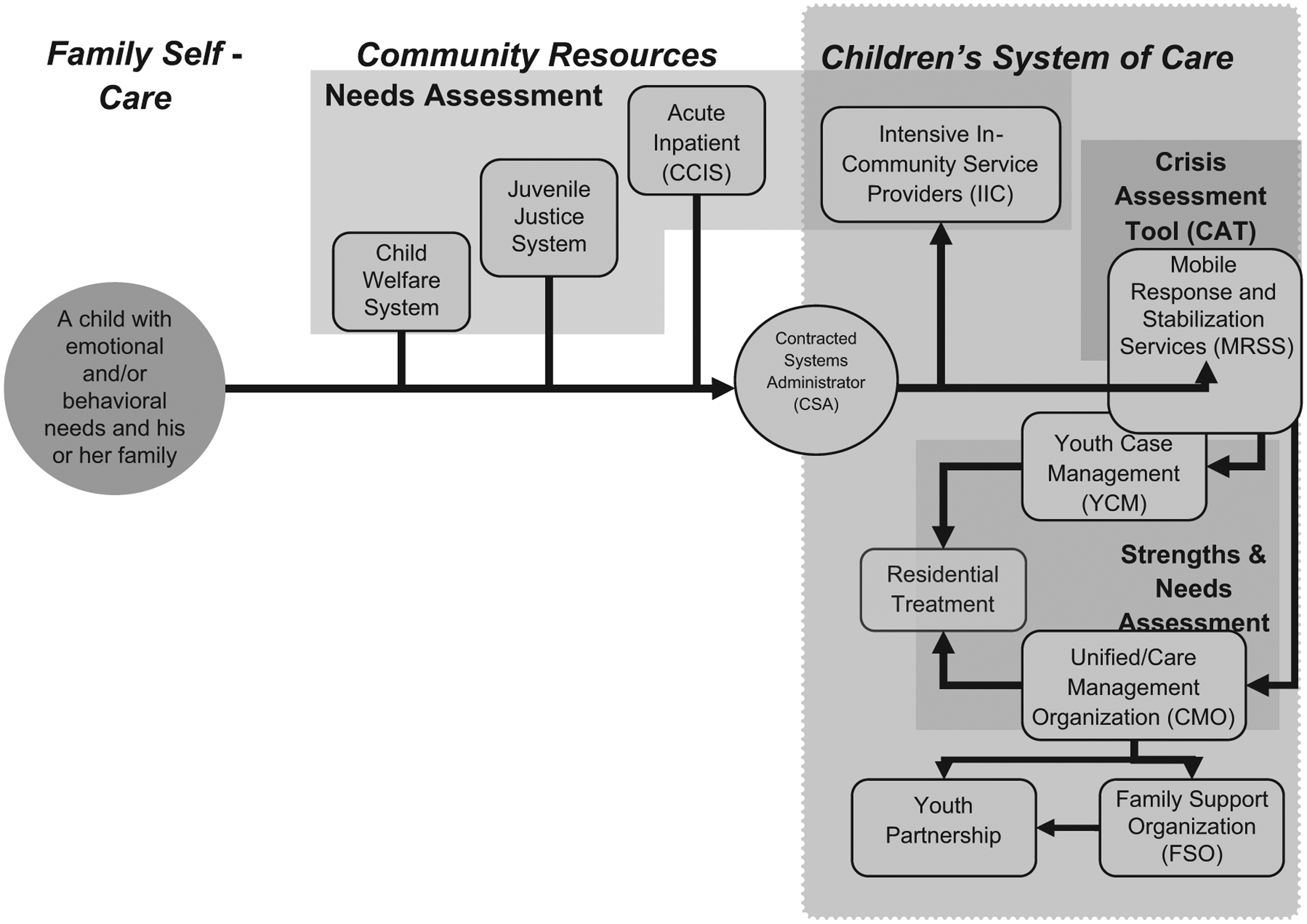
New Jersey Children’s System of Care, as of 2012.
If a child/youth is determined to have highly complex needs with multiple systems involvement, they are referred to a Care Management Organization (CMO). The CMO uses the Wraparound model (Walker, Bruns, & Penn, 2008) to create a child/family team to develop an individualized service plan for the child/youth and their family. The parents/caregivers of these children also receive peer support from the FSO. The FSOs are family-run organizations providing direct peer support for caregivers, as well as offering a plethora of family supports, including family-to-family peer support groups, educational seminars, youth partnership groups, and advocacy to family members of children with emotional and behavioral challenges (PerformCare, 2012). The FSOs ensure that “family voice” is heard and utilized throughout the system of care. Children whose needs are assessed at a more moderate level are connected to YCM Services (PerformCare, 2012).
YCM services are less intensive than CMO services and are provided for a shorter duration of time. The goals of YCM include assessing, monitoring, and connecting children/youth to community-based services. If a child/youth’s needs become more severe during their time with the YCM, a referral to the CMO can be made through the CSA. Unified Care Management (UCM) organizations have been created in selected areas of the state as a result of family voice in the New Jersey system of care. Many families had children in both CMO and YCM which often led to multiple child/family team meetings and plans of care that did not coordinate service planning well. UCMs provide both CMO and YCM levels of care under one roof (PerformCare, 2012).
Children/youth assessed by the CSA to be experiencing non-life threatening crises are eligible to receive CMRSS. CMRSS is available 24 hr a day, every day throughout the year. The goals of CMRSS are to help children/youth who are experiencing emotional and/or behavioral crises by defusing an immediate crisis in their homes, while maintaining everyone in the household’s safety, and preventing unnecessary emergency room psychiatric screenings by keeping the child/youth with their caregivers at home (PerformCare, 2012).
The University of South Florida’s Final Report: Independent Assessment of the New Jersey’s Children’s Behavioral Health Care System (Armstrong et al., 2006) included many systemic recommendations, specifically in the areas of quality improvement, the assessment process, and family involvement as partners to improve New Jersey’s system of care. One of the most essential components of the system of care is the assessment process or more specifically the Information Management Decision Support (IMDS) tools. The IMDS tools that have been fundamentally rooted in system of care are based upon the Child and Adolescent Needs and Strengths (CANS) tools developed by Dr. John Lyons (2004, 2009) and adapted to best serve the children and families in all 21 counties throughout the State of New Jersey.
Therefore, based upon the recommendations offered by the University of South Florida report, a review of the archival data from the first 5 years of New Jersey’s use of the CANS tools period was examined. This information can serve as a starting point for more in-depth analyses for “outcome based” analyses of the system of care (Armstrong et al., 2006). For example, the use of specific focus groups to review the data gathered from this research can be utilized to incorporate system of care revisions and expansions (Armstrong et al., 2006). This research paper utilized archival data, from 2006 to 2010, from a computerized database which examines training methodology, live versus compact disc (CD), and certification data, certified or not certified, to utilize that particular IMDS tools with the system of care.
IMDS/CANS Tools and System of Care
The IMDS and CANS tools are based upon “communimetric” measure, developed from communication theory rather than psychometric theory. Communication theory in a social science context can be traced as far back as the early 1950s, with the early work done by Gregory Bateson, an English anthropologist and linguist. The text Communication: The Social Matrix of Psychiatry (Ruesch & Bateson, 1951) was published and co-authored by American psychiatrist Jurgen Ruesch. Ruesch and Bateson’s (1951) “unified” theory of communication allowed for social scientists to measure social interactions; in this case, it was between psychiatrist and patient. These early pioneers in communication theory went on to scientifically quantify behaviors of people at the individual, group, and society levels to help not only improve understanding from a theoretical stance but to actually aid in alleviating the suffering (Ruesch & Bateson, 1951).
John S. Lyons (2009) in his groundbreaking book Communimetrics takes the tenants of communication theory and applies it directly to the measurement within the various human services settings. The main principle of communimetrics is a “shared” understanding of what is being measured, along with a clear descriptive level of either actionable or non-actionable ratings (Lyons, 2009). The CANS tools have been developed specifically to be used within the communimetric context. These communimetric tools are designed to use a single-item approach (e.g., depression) that allows for meaningful decision making and outcome monitoring (Lyons, 2004, 2009). When information is gained directly from the child/youth and their family through the use of these tools, it allows a system to remain focused on the shared vision of serving children and families, by representing the children and their families at all levels of the system (Praed Foundation, 2012a). In other words, a system of care can function by focusing on the best interests of the children and families it serves if those working directly with children/families have accurate information about the needs and strengths of the children in the system.
The CANS tools have been incorporated throughout the country in almost all 50 states. It should also be highlighted that several foreign countries and several Canadian Provinces also use versions of the CANS. (Praed Foundation, 2012b). See Figure 2 for a more detailed breakdown of CANS usage throughout the United States.
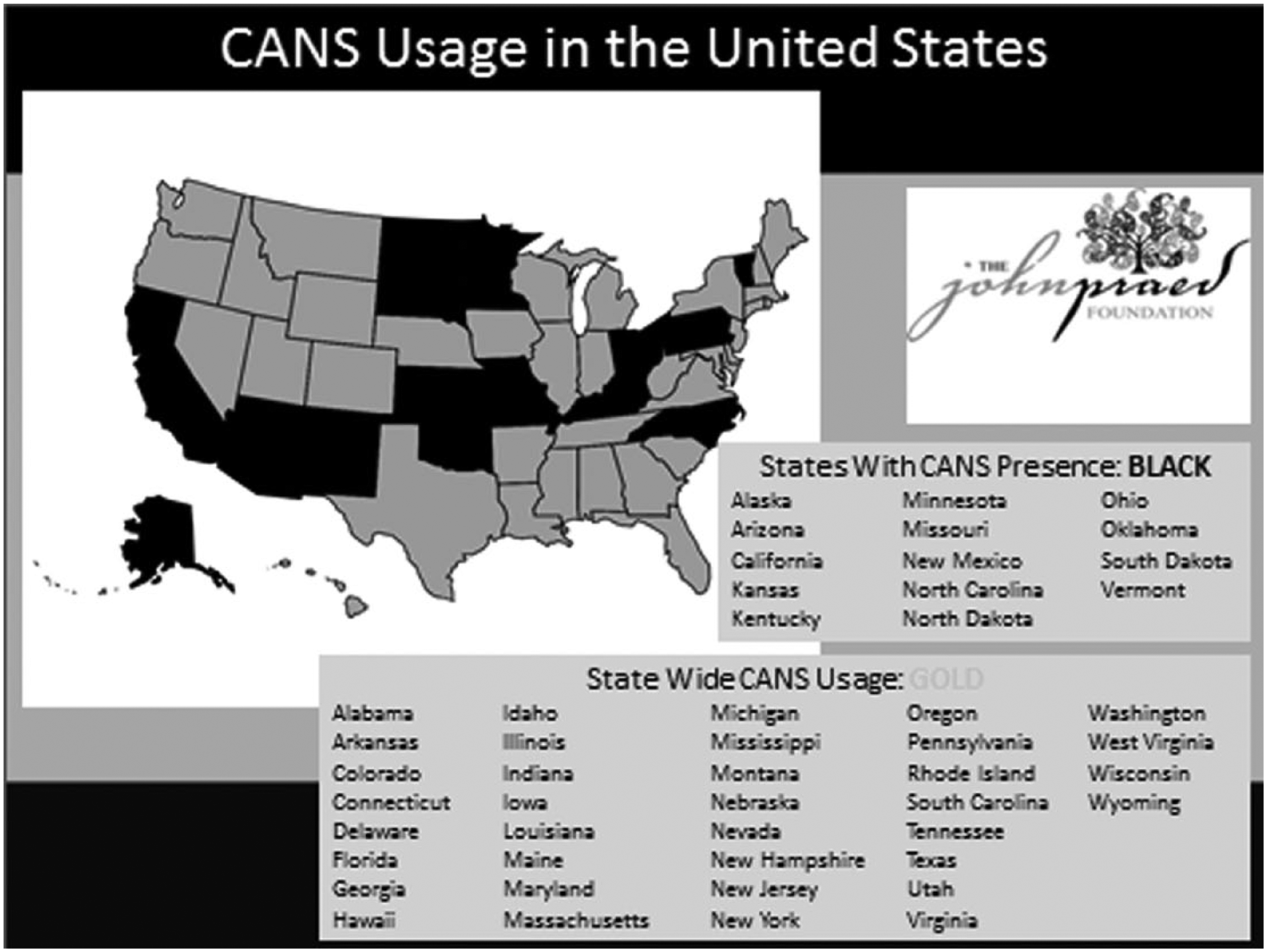
A breakdown of CANS usage.
There are currently three IMDS tools being utilized within New Jersey’s DCSOC; the NA, Strengths and Needs Assessment (SNA), and the Crisis Assessment Tool (CAT). Each of the IMDS tools serves a distinct purpose and is used for children, aged 5 through 18 years. It should be noted that youth can remain part of the system of care up to age 21. Referrals are gathered from DCSOC, Division of Child Protection and Permanency (DCP&P), which was formerly the Division of Youth and Family Services (DYFS), The Juvenile Justice Commission (JJC), or any other child-serving state agencies which demonstrate a clinical need for services provided by the DCSOC, as part of the transition into adult services (PerformCare, 2012).
The referral tool to support decision making about the intensity of need of both children and families seeking services is called the Needs Assessment. It facilitates the rapid and consistent communication of the needs of children who are served through the DCSOC. The NA supports the determination of eligibility by matching the level of intensity of needs to an appropriate level and intensity of care. All children entering the DCSOC have an NA completed. This tool will be used to document and communicate the needs of the child and family, to determine the intensity of service care needed, to serve as a decision support tool, and to inform planning for needed services (PerformCare, 2012).
The NA is then integrated into subsequent service planning in the form of the SNA which reviews and adds to the information summarized in the NA. Those entities referring to the DCSOC for services for children/youth include the following: Families, School Systems (with parental/guardian permission), DCP&P, Medicaid Approved In-Community Providers (licensed clinical therapist), Partial Care Programs, and other Mental Health Providers.
The child/family “team” planning tool utilized to support decision making about the individual treatment planning for children and families within the DCSOC is called the Strengths and Needs Assessment. It supports the rapid and consistent communication of the strengths as well as the needs of children and their families being served through the DCSOC. It is intended to be completed by the individuals who are directly involved with the child/family as part of the child/family team (PerformCare, 2012).
The SNA assessment tool serves to document the identified strength and needs of the child/family throughout the time they are in the DCSOC. The SNA tool is utilized by UCM, Care Management, YCM, and Residential Providers to serve as the documentation of the progress as well as to ensure the child and family receive the appropriate services for the appropriate length of time (PerformCare, 2012).
The other IMDS tool is the CAT which is also a decision support and communication tool designed to allow for the rapid and consistent communication of the needs of children experiencing a crisis that threatens their safety or well-being or the safety of the community. It is intended to be completed by CMRSS who are directly involved with the crisis assessment. The form serves as both a decision support tool and as documentation of the identified needs of the child served along with the decisions made with regard to treatment and placement at the time of the crisis. Whereas the NA and SNA primarily focus on the past 30 days of functioning, the CAT generally examines the last 24 hr regarding crisis and/or risk behaviors that put the child/youth at risk of danger and possible loss of current placement and/or living arrangement (PerformCare, 2012). As all of the IMDS/CANS tools (see Figure 3) are based upon “communimetrics” or communication theory, they support the discussion with regard to decision support or treatment among the multiple disciplines and professionals that are often connected with children/youth (Lyons, 2006).

Current IMDS tools utilized in New Jersey’s Children’s System of Care.
Embedding of CANS/IMDS Tools Within System of Care
From the beginning, University Behavioral Health Care (UBHC)–Behavioral Research & Training Institute (BRTI) at Rutgers University has provided comprehensive training and technical assistance (TTA) services to support statewide implementation of the New Jersey’s DCSOC. Rutgers University is one of the nation’s largest health sciences universities; BRTI has as its ongoing mission the development and implementation of TTA programs which support practitioners in the behavioral health and allied fields to acquire the knowledge and skills necessary to provide services which support the unique needs and strengths of individuals facing complex challenges. The DCSOC TTA program draws on Behavioral Research Training Institute’s commitment to offer competency-based curriculum-designed trainings, based on adult principles of learning and skill development, with the goal of achieving the development of local expertise (Caliwan & Furrer, 2009).
UBHC-BRTI has the responsibility for all DCSOC trainings, including all IMDS tool trainings and certifications. The training of the different stakeholders in the application and use of the individual tools was fundamental to the full implementation of the IMDS process throughout the State of New Jersey (see Figure 4). The goal was to adhere to a timeline of a phased implementation of both the planning rollout of the IMDS tools as well as the strategic training of various system representatives (Caliwan & Furrer, 2009).

Timetable of New Jersey’s Children’s System of Care rollout and training.
In-person or “live” trainings for the IMDS tools were piloted back in mid-2001 and were fully operational by early 2002 (Caliwan & Furrer, 2009). These trainings were performed by UBHC-BRTI staff, who worked closely with the tools developer, Dr. John Lyons. However, as the number of individuals requiring training and certification incrementally increased, UBHC-BRTI began planning (in mid-2003) for the development of both the web-based IMDS certification system and the IMDS distance or CD-based learning feature (Caliwan & Furrer, 2009).
By late 2002, the filming and production of CD-based distance learning along with the web-based online certification system was completed. The “train the trainer” process was replaced by the incorporation of an “IMDS SuperUser” model, which incorporated more detailed training for individuals serving in a senior-level position, by Dr. Lyons along with the Training and Consultant Specialist at Rutgers University. The primary role of the IMDS SuperUser is to maintain, within their agency, the “fidelity of purpose” of the tool, as part of the information management decision and support process. IMDS SuperUsers also assist in ensuring that the IMDS tool(s) are supporting the Wraparound model in New Jersey’s DCSOC. These individuals serve as the “point” person within their agency to assist staff in reliably utilizing the IMDS tool with the children and their families.
This 2-day IMDS SuperUser training utilized additional materials, including adult learning principles, power point templates, and the CD-based or distance learning model. The initial IMDS SuperUsers completing the additional training were within a specific system entity, primarily those from the Care Management Organization or CMO (Caliwan & Furrer, 2009). This IMDS SuperUser training was initiated and maintained with the goal that every system entity had an IMDS SuperUser at their agency to ensure a continuity of valid and reliable usage of the IMDS tool.
By late 2003, all three IMDS tools were solidly embedded into the children’s system of care and live monthly trainings were being held throughout the state (Caliwan & Furrer, 2009). This methodology of training continues to date, and the system of care currently has approximately 2,000 actively certified IMDS users, for all three of the current tools used in the children’s system of care, throughout the entire state (Rutgers University, University Behavioral Health Care-Behavioral Research Training Institute of New Jersey, 2012a).
As of October 2007, the DCSOC required annual recertification which is maintained via the “on-line” computerized system for certification for the three IMDS tools, managed by the BRTI within the Rutgers University (DCF, 2012b). The recertification process for all IMDS tools is the same as becoming initially certified. After taking either a refresher live training or reviewing the CD, individuals take the certification via the “on-line” computerized system (DCF, 2012a). All three IMDS tools have been used in New Jersey since the beginning of the system of care was developed. As of January 1, 2006, there have been approximately 11,500 individual certification records since the IMDS online system went “live” statewide back in late 2002 (Rutgers University, University Behavioral Health Care-Behavioral Research Training Institute of New Jersey, 2012b).
Results: 5 Years of Data
Training protocol for all three IMDS tools is accomplished when the individual attends a 6-hr in-person lecture-styled training or reviews a CD, approximately 50 min in length, which provides the learner with an overview of the children’s system of care, the function and structure of the IMDS tool, as well as the process for certification. There is no cost for “live” training, the CD, or the online certification. It should be noted that the 6-hr in-person or “live” training incorporates both lecture methods as well as small group activity to complete a practice IMDS vignette. The vignette is reviewed by going over each of the items as well as discussing the rationale behind the recommended rating or score. The CDs were not designed to be used independently but in conjunction with an agency’s SuperUser as part of the individual’s new hire orientation process.
After an individual completed either the “live” or CD training, then they can create an account in the IMDS online computerized certification system and complete practice vignettes before taking the actual IMDS certification: These practice vignettes allow the learner to feel comfortable with the overall format of the computerized testing system, while gaining rater reliability on the specific tool. Learners can review their scores on any of the practice vignettes and compare their ratings if they differ from the recommended ratings. Once a .70 reliability or higher is obtained on the practice vignettes, then the individual can proceed to the IMDS certification vignette for that particular tool. Afterward, if an individual receives a .70 reliability rating or higher on the certification vignette, then the individual is deemed certified on the tool, as the validity of the IMDS tools is based upon the CANS which has been demonstrated its correlation of validity and reliability with other measures (Praed Foundation, 2012a).
All certification data are stored within the online computerized system, including the “failed” attempts or those scores which fall below the .70 reliability rating. The primary goal of this research article was to review the data from past 5 years to examine any relationship between the method of training and the certification scores. Since the entire system of care components was completely “rolled out” statewide in 2006, any earlier data would not include all 21 counties and be representative of the entire New Jersey system of care. Therefore, the 5 years will include all IMDS data from 2006 through 2010 for all three IMDS tools, the NA, SNA, and the CAT.
Analyses of CANS/IMDS 2006-2010 Data
The rational for using the cumulative data rather than the individual certification scores was based upon the direct “cutoff” score of .70 for certification. If an individual, regardless of how much below their score fell below .70, was deemed not certified on the IMDS tool and had to retake the certification. The “certification” demarcation was given as long as the individual scored at or above the cutoff of .70. There were other variables that led the researcher to use only the cumulative data. In particular, there were significant revisions made to the training materials over the years, the practice and certification vignettes, as well as changes in key IMDS trainers. The IMDS data from 2006 through 2010 for all three IMDS tools, the NA, SNA, as well as the CAT (see Table 1) were collected from the online database and categorized for analysis as follows: IMDS tool, Pass/Fail Certification, Training methodology (live vs. CD), and year of certification. Chi-square statistics and p values for 2 × 2 analyses were done on the aggregate data.
IMDS Cumulative IMDS Data.

Note. Passing/certification score of .70 or higher. Failing/non-certification score of .69 or lower. IMDS = Information Management Decision Support; CD = compact disc; SNA = Strengths and Needs Assessment; CAT = Crisis Assessment Tool.
Table 1 contains the cumulative data from 2010 (dating back to 2006) in which the chi-square statistic was performed for each of the individual 2 × 2 tables, which is comprised of the data for each year. The chi-square test was utilized to see how far the observed table deviates from the null (or expected) table, which is the table where the number in each cell is proportionate to the number that would be expected simply based on the size of the sample in that cell.
For example, in 2006, the observed total of individuals who had taken the NA tool totaled 213, with 64 passing having “live” training and 61 passing by those trained by CD. This was compared with those who failed the certification with “live” (total 50) and by CD (total 38). The following formula was computed: ([observed − expected] × [observed − expected]) / expected and sum the values for each cell and this becomes the chi-square statistic. Degrees of freedom (df) is equal to (r − 1) × (c − 1), where r = number of rows and c = number of columns. Thus, for a 2 × 2 table, df = 1 (see Table 2).
Chi-Square Statistics and p Values for 2 × 2 Tables of Pass/Fail × Live/CD.

Note. Chi-square statistic (with p value in parentheses) with 1 df. CD = compact disc; SNA = Strengths and Needs Assessment; CAT = Crisis Assessment Tool; df = degrees of freedom.
p < .05 (i.e., the chi-square statistic is statistically significant at the .05 level, meaning that 95 out of 100 times if you observe this result, there is actually a significant relationship there in the population and not just in this sample).
A large chi-square means that there was a greater difference between the expected and observed table. The number itself tells you nothing about the direction of this relationship (i.e., whether the live or CD had a higher pass rate). However, from the overall data collected, individuals attending the “live” training generally had a higher pass rate. This difference was only statistically significant at the .05 level for SNA and CAT in 2007. Obviously, the larger chi-squares indicate a stronger relationship, with regard to differences in pass rate and training methodology (live vs. CD).
Substantive Interpretation of 5-Year Data
The IMDS certification data accumulated from 2006 to 2010 revealed that CD training was as effective, overall, based upon yearly certification scores on all three IMDS tools. Major factors to include in this interpretation are that the IMDS tools were thoroughly embedded into the New Jersey’s DCSOC from the early planning stages and that IMDS SuperUsers have also been embedded into the various system entities, including CMO, UCM Organization, YCM, CMRSS, Licensed In-Community (IIC) Providers, JJC, and DCP&P. Throughout the state, these SuperUsers have been trained, specifically in the “train the trainer” model. Dr. John Lyons has taken part in all of the SuperUser Trainings since 2004 to ensure fidelity in the utilization of all of the IMDS tools within a system of care model. As of 2010, there were over 90 SuperUsers trained throughout the system of care, and embedded into the various organizations and agencies, to offer “in-house” training to their staff utilizing the training materials, various handouts, and CD, provided to them during the 2-day SuperUser training.
The statistically significant difference at the .05 level for SNA and CAT for the year 2007 may be explained by the DCSOC requiring an annual recertification for all those certified on any of the IMDS tools (DCF, 2012b). Obviously, the larger chi-squares indicate a stronger relationship, with regard to differences in pass rate and training methodology (live vs. CD). The number of individuals completing both the SNA and CAT more than doubled from 2006 to 2007 with a chi-square score (0.05 level), which indicates that the “live” training was statistically more effective than “CD” training for obtaining certification.
The BRTI at Rutgers University has the ongoing mission to provide a technical assistance that supports learning the requisite knowledge and skills to provide services and support the unique needs and strengths of families and children with complex needs, in particular the use of all IMDS tools. This TTA varies depending upon the needs of the system of care. Since 2004, BRTI has provided statewide “live” IMDS trainings, offered technical support through email and telephone contacts, and maintained accuracy of the statewide IMDS database.
All three of the IMDS have been successfully embedded into New Jersey’s system of care because of the initial planning and implementation process back in the early phases of the system of care development. In addition, the significant TTA offered by BRTI to support those attempting initial certification as well as recertification on the IMDS tools appears to have had a deep impact on successful certifications. Since 2004 to the end of 2010, BRTI by responding to over 3,400 emails, over 1,700 phone calls equaling some 1,000 hr of IMDS-TTA throughout the entire state (Rutgers University, University Behavioral Health Care-Behavioral Research Training Institute of New Jersey, 2012b).
System of Care Success—Look Toward Future
The planning and incorporation of the IMDS tools, based upon the CANS, from the beginning of New Jersey’s DCSOC (Caliwan & Furrer, 2009), has led to successful training methodologies and certification scores. After the examination of IMDS certification scores, training methodologies, and specific IMDS tools, it appears to have resulted in consistent certification and recertification scores on the various IMDS tools throughout the entire state. The time and energy invested in embedding and coordinating the use of the communimetric tool, such as the IMDS tool, into a system of care appears to have been time and energy well spent.
The IMDS tools are now used throughout New Jersey by other system partners, including mental health, education, juvenile justice, and child protective services, to collaborate in successful treatment planning (Lyons, 2006). The two best strategies to ensure that the measure is being used with both reliability and validity within a system of care are to have annual recertification on the tools as well as utilization of an IMDS SuperUser within various system entities (Lyons, 2004, 2009). The essence of the IMDS tools is based upon communimetric philosophy and they exist to communicate the needs and strengths of a child/youth and their families for use as both tools for treatment and framework system improvements (Lyons, 2004, 2009).
As a system of care develops and matures, the more specific the needs of the populations being served emerge. As the design of the communimetric tools has been focused on the process of gaining information, there is a built-in “flexibility” for them to be tailored to accommodate specific populations (Lyons, 2009; Praed Foundation, 2012b). There are many current versions of the CANS being utilized throughout the country and internationally. Some of variations of them include the CANS–Mental Health (CANS-MH) version that addresses the mental health needs of children, adolescents, and their families; the CANS–Eating Disorders (CANS-EDS3) version designed to adequately measure eating disorders behaviors and symptoms for appropriate treatment planning; and CANS–Autism Spectrum Profile (CANS-ASP) version developed to effectively gather a profile of information of children and adolescents with Autism Spectrum Disorders to support individual/family case planning and evaluation of service systems (Praed Foundation, 2012b).
As the IMDS tools have been successfully embedded into the system of care with the successful use of two different training methodologies, it would not be difficult to revise or add to the IMDS tools currently being utilized. It would also be logical to explore the various CANS versions and the needs of specific population to effectively serve them. The process of determining the system of care needs would be to examine the data and population profiles, gaining feedback from the variety of current system partners, as well as from other child/youth serving entities to increase collaboration efforts.
One significant population profile in the New Jersey’s DCSOC is the 16 and older population or the “emerging adult” population. According to the most recent New Jersey DCF Annual Agency Performance Report, there were over 4,000 youth or 50% of the total Care/Case Management population aged 16 years and older as of June 30, 2011 (DCF, 2012c). Of these 4,000 youth, 32% or 1,280 were African American, more than 62% or 2,480 were males, and 1,826 of these youth were in an “out of home” placement (DCF, 2012c). To plan for these “transitional aged” youth, there needs to be increased knowledge of existing resources and collaboration among entities (McGill & McGill, 2011).
An updated IMDS tool which targets the particular needs of this “emerging adult” group can be easily incorporated to New Jersey’s system of care. The IMDS tools currently utilized are primarily static as to their uses and have been designed for a generic population of age 5 through 18 years (McGill & McGill, 2011). However, there is a more appropriate transitioning form of the CANS called the Adult Needs and Strength Assessment (ANSA), which has been further developed into a CANS version specifically appropriate for the 16- to 25-year-old population called the Young Adult Needs and Strength Assessment or YANSA (Praed Foundation, 2012b). The YANSA is currently in use in many states, including Pennsylvania, Maryland, and West Virginia (Praed Foundation, 2012b).
The incorporation of the YANSA into the IMDS repertoire would be a significant step in building a systemic “bridge” in assisting the “emerging adult” population in the planning process into appropriate adult services (McGill & McGill, 2011). The addition of such a communication tool would assist in more effective planning for transition across systems, in particular, child/youth and adult service systems. New Jersey has been one of few states that have incorporated a system of care philosophy which has been consistent with serving all children/youth regardless of which serving entity they initially enter into for services. The key factor determining treatment services or more appropriately to meet their needs is based upon the communication among all system partners, especially the child/youth and their caregivers.
Footnotes
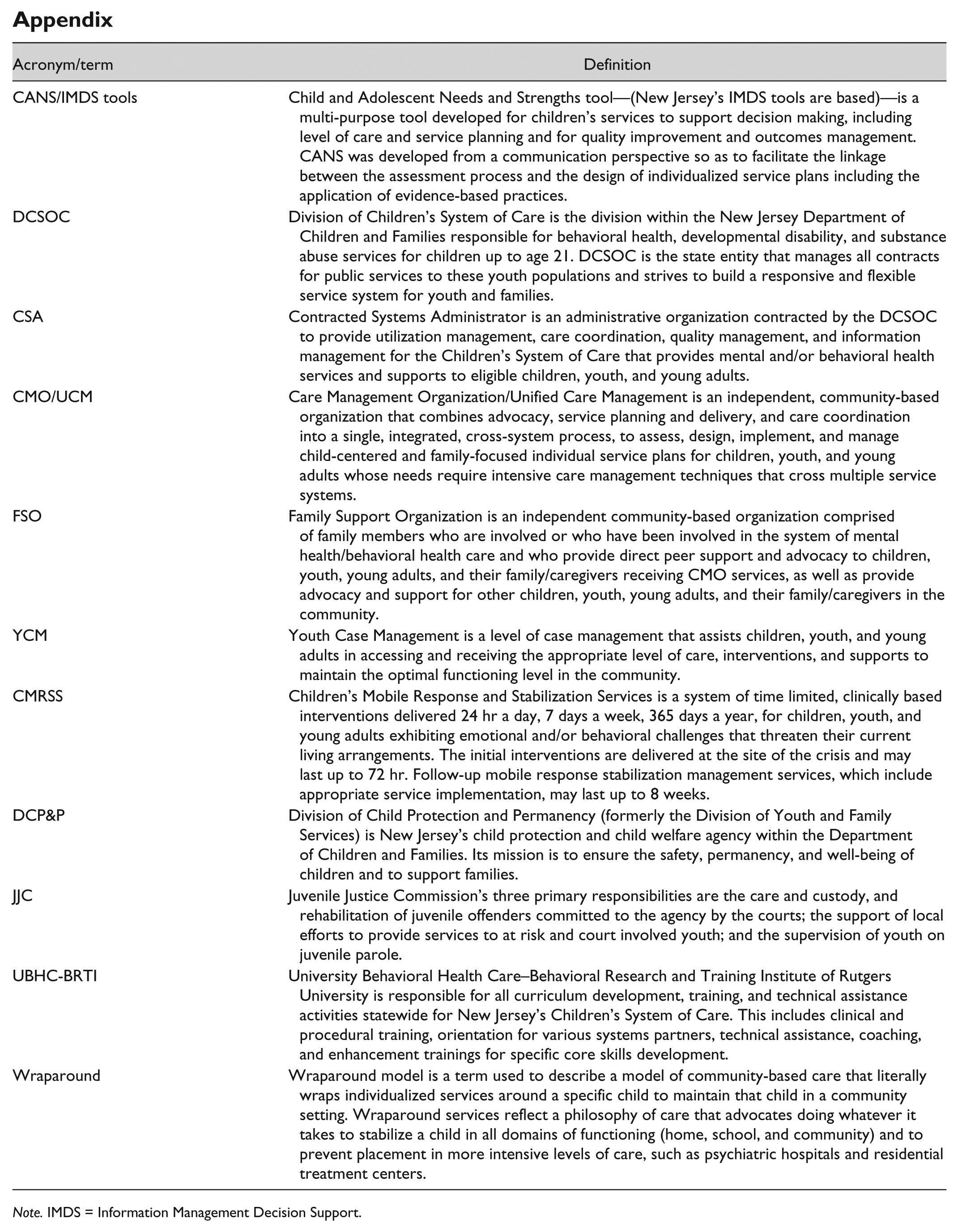
Appendix
| Acronym/term | Definition |
|---|---|
| CANS/IMDS tools | Child and Adolescent Needs and Strengths tool—(New Jersey’s IMDS tools are based)—is a multi-purpose tool developed for children’s services to support decision making, including level of care and service planning and for quality improvement and outcomes management. CANS was developed from a communication perspective so as to facilitate the linkage between the assessment process and the design of individualized service plans including the application of evidence-based practices. |
| DCSOC | Division of Children’s System of Care is the division within the New Jersey Department of Children and Families responsible for behavioral health, developmental disability, and substance abuse services for children up to age 21. DCSOC is the state entity that manages all contracts for public services to these youth populations and strives to build a responsive and flexible service system for youth and families. |
| CSA | Contracted Systems Administrator is an administrative organization contracted by the DCSOC to provide utilization management, care coordination, quality management, and information management for the Children’s System of Care that provides mental and/or behavioral health services and supports to eligible children, youth, and young adults. |
| CMO/UCM | Care Management Organization/Unified Care Management is an independent, community-based organization that combines advocacy, service planning and delivery, and care coordination into a single, integrated, cross-system process, to assess, design, implement, and manage child-centered and family-focused individual service plans for children, youth, and young adults whose needs require intensive care management techniques that cross multiple service systems. |
| FSO | Family Support Organization is an independent community-based organization comprised of family members who are involved or who have been involved in the system of mental health/behavioral health care and who provide direct peer support and advocacy to children, youth, young adults, and their family/caregivers receiving CMO services, as well as provide advocacy and support for other children, youth, young adults, and their family/caregivers in the community. |
| YCM | Youth Case Management is a level of case management that assists children, youth, and young adults in accessing and receiving the appropriate level of care, interventions, and supports to maintain the optimal functioning level in the community. |
| CMRSS | Children’s Mobile Response and Stabilization Services is a system of time limited, clinically based interventions delivered 24 hr a day, 7 days a week, 365 days a year, for children, youth, and young adults exhibiting emotional and/or behavioral challenges that threaten their current living arrangements. The initial interventions are delivered at the site of the crisis and may last up to 72 hr. Follow-up mobile response stabilization management services, which include appropriate service implementation, may last up to 8 weeks. |
| DCP&P | Division of Child Protection and Permanency (formerly the Division of Youth and Family Services) is New Jersey’s child protection and child welfare agency within the Department of Children and Families. Its mission is to ensure the safety, permanency, and well-being of children and to support families. |
| JJC | Juvenile Justice Commission’s three primary responsibilities are the care and custody, and rehabilitation of juvenile offenders committed to the agency by the courts; the support of local efforts to provide services to at risk and court involved youth; and the supervision of youth on juvenile parole. |
| UBHC-BRTI | University Behavioral Health Care–Behavioral Research and Training Institute of Rutgers University is responsible for all curriculum development, training, and technical assistance activities statewide for New Jersey’s Children’s System of Care. This includes clinical and procedural training, orientation for various systems partners, technical assistance, coaching, and enhancement trainings for specific core skills development. |
| Wraparound | Wraparound model is a term used to describe a model of community-based care that literally wraps individualized services around a specific child to maintain that child in a community setting. Wraparound services reflect a philosophy of care that advocates doing whatever it takes to stabilize a child in all domains of functioning (home, school, and community) and to prevent placement in more intensive levels of care, such as psychiatric hospitals and residential treatment centers. |
Note. IMDS = Information Management Decision Support.
Acknowledgements
The authors would like to thank their families for words of encouragement. In addition, a special thank you for key feedback from the following individuals at Rutgers University Behavioral Health Care–Behavioral Research Training Institute: Dr. Kathleen Finnerty, Program Director; and Shannon Zhou, Information Services Consultant.
Authors’ Note
This article is dedicated to the memory of Laura Conigilio, Executive Director of the Passaic County Family Support Organization. It is through the view from “the balcony” that we can fully see our successes and challenges for the future. Her memory continues to be an essence to the children’s system of care, in particular, the “family voice.” Laura you are truly missed but not forgotten.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.