
Abstract
The purpose of this study was to describe the psychosocial experience of the International Federation of Red Cross and Red Crescent Societies’ nurses upon their return from deployment at an Ebola Treatment Center during an Ebola virus disease outbreak in Kenema, Sierra Leone, between 2014 and 2015. The following three psychosocial aspects related to pre-, during, and postdeployment were explored: stress management, sociocultural exposure, and attitudes from others. This is a descriptive qualitative study with a cross-sectional design. Questionnaires were administered to 50 nurses, of which 44 responded. Eight themes were identified in relation to the three psychosocial aspects of interest: professional- and self-confidence, pragmatism, wellness activities, human contact, cultural competency, professionalism, pariah, and/or hero. One of the most important findings in this article relates to the essential mental health support pre- and during deployment with an emphasis upon return when the risk of isolation and stigmatization is greater. In conclusion, more research is needed about the psychosocial challenges met by nurses to prepare and support them as increasing threat of emerging infectious diseases puts pressure on global health systems.
Introduction
The outbreak of Ebola virus disease (EVD), known as Ebola hemorrhagic fever, that took place in West Africa between 2014 and 2016, was the most widespread and complex EVD outbreak known, to date, in human history. The primary case was tracked to a child in the Republic of Guinea in December 2013 (World Health Organization [WHO], 2020b). Sierra Leone, Liberia, Nigeria, Senegal, the Democratic Republic of the Congo (DRC), and Mali were the countries the most affected by the disease (WHO, 2020a). There had been more cases and fatalities during this last outbreak than any others combined. By June 2016, there had been 11,310 reported deaths globally and 28,639 confirmed cases (WHO, 2016).
The International Federation of Red Cross and Red Crescent Societies (IFRC) has the responsibility for the preparation of its staff and volunteers under a viral hemorrhagic fever (VHF) outbreak such as Marburg disease or EVD. The IFRC is an important player in providing support during catastrophes globally, and as such, it has collaborated tightly with the national and local Red Cross Societies, Ministries of Health, WHO, and Médecins Sans Frontières (MSF) to control as well as overcome the EVD outbreak. The IFRC responded to the crisis by sending a total of 200 international staff members between 2014 and 2015, mostly registered nurses, whose main responsibility was to set up and work at an Ebola Treatment Center (ETC) in Kenema, Sierra Leone. It was the first time that the IFRC planned such an extensive medical intervention in response to a VHF outbreak. The emergency response unit (ERU; IFRC, 2017) system did not have, at the time, a preset outlined structure, nor was VHF training part of the general preparedness plan even though the IFRC’s ERUs had earlier been engaged in other epidemic outbreaks (IFRC, 2014a).
EVD is categorized as an emerging infectious disease (EID; Centers for Disease Control and Prevention [CDC], 2018b) and is therefore a challenge to the international health care profession. EVD is highly contagious and lethal, which can provoke fear of contamination and stigmatization (IFRC, 2014a). In such context, nurses habitually find themselves in a vulnerable and unsafe position (Hayter, 2015), as they are often not sufficiently trained for these new lethal infectious challenges (Jones et al., 2008). Nurses are major actors to global health care (Holmgren, 2017; Kraft et al., 2017) as globalization requires their ability to focus on “issues that directly or indirectly affect health but that can transcend national boundaries” (Koplan et al., 2009, p. 1994). Nurses working with global nursing (Kraft et al., 2017) are likely during their career to find themselves at the forefront of complex humanitarian emergencies (CHE) and even an EVD outbreak in which they play a key role (Fung et al., 2008; Tierney, 2008). Although several humanitarian organizations such as MSF, IFRC, and the International Committee of the Red Cross (ICRC) put a lot of effort in developing and updating safety protocols and training for their nursing staff, there is still limited published research available on working conditions in such setting (Lam et al., 2018; Yin et al., 2011). Research interests have been mostly put on the infrastructure surrounding health care workers during an EVD outbreak, such as infection control and emergency management (Petinaux et al., 2016), construction of specialized medical settings in communities (Pronyk et al., 2016), laboratory research (Iwen et al., 2014; Parkes-Ratanshi et al., 2014), as well as shielding kits and professional conduct (Bazeyo et al., 2015; CDC, 2018b). A shielding kit, also known as personal protective equipment (PPE), is essential when caring for patients with Ebola. It has for purpose to cover the clothing and skin, while completely protecting the mucous membranes (CDC, 2018a).
More specifically, limited amount of research has examined the experience of health professionals working under life-threatening medical circumstances (Belfroid et al., 2018; Noguchi et al., 2016; Zinsli & Smythe, 2009) such as dealing with VHF, which can be the cause of severe psychosocial stress (Hewlett & Hewlett, 2005; Smith et al., 2017; Vega, 2016). It is not only due to witnessing extreme pain and death on a daily basis for weeks at a time but also fearing to be infected. The constant pressure of temperature monitoring, reporting, and quarantine may cause severe psychological disorder for staff such as depression or post-traumatic stress disorder even long after the outbreak (Lin et al., 2007; Matsuishi et al., 2012; Mollers et al., 2015). Therefore, it is imperative to identify the psychosocial stressors to prepare, protect, and optimize the performance of the health care staff. Alarmed health and humanitarian organizations are interested in knowing more about these stressors to plan effectively for future VHF outbreaks (Bisson et al., 2010; von Strauss et al., 2017).
Increased knowledge is needed to best prepare the health professionals in the future event of a VHF. Therefore, the purpose of this study was to describe the psychosocial experience of IFRC nurses upon their return to their home countries from deployment at an ETC during an EVD outbreak. Specific psychosocial aspects related to pre-, during, and postdeployment were explored: stress management, sociocultural exposure, and attitudes from others. This study was initially instigated by the IFRC, and the categorization of these three psychosocial aspects was founded on the specific interest of this organization to increase understanding on the topic. The connection between the three time periods and the psychosocial areas was used as a conceptual framework for the purpose of this research.
Method
Study Design
This is a descriptive qualitative study with a cross-sectional design. This research is part of a larger project regarding global nursing during the EVD outbreak in West Africa, before, during. and after deployment of IFRC nurses (von Strauss et al., 2017; Holmgren et al., 2019). The study has an inductive approach based on a conceptual framework.
Study Context
The IFRC’s first ETC was constructed over a 3-week period in Kenema, Sierra Leone. The center was staffed by international nurses and an even larger number of local nurses. All effort was grounded on methodical organization and preparation to make sure that no health care members were unprotected against Ebola. This consisted of strict training in the use of PPE. There was space for 60 patients. The ETC was divided into three sections: confirmed, probable, and suspected cases. The staff was also responsible for water and sanitation, cooking, providing clean clothes, and arranging safe funerals in addition to the nursing care (IFRC, 2014b).
Sample
The IFRC enabled the data collection by providing email addresses to the last author and principal investigator (PI) of this research. It consisted of a list of nurses who were deployed by the IFRC at the ETC in Kenema between 2014 and 2015. These persons were methodically asked by email to contribute to this study. It included an overall 78 nurses, among which 13 had nonvalid email addresses. Consequently, 65 nurses remained as potential participants. However, among them, 15 did not respond to the request to participate in the study. Of the remaining, 50 email invitations were sent, and 44 nurses gave their informed consent to participate. The age of the participants ranged between 25 and 61 years old. Thirty-six of them were women. Most of the nurses came from Europe, whereas 10 came from Oceania, five from North America, and two from Africa. Thirty-three had previous knowledge of voluntary work with humanitarian deployment and 26 had undergone the ERU training before arriving to the ETC. For most of them, it was their first time at the ETC in Kenema (Table 1).
Summary Table of Demographic Data.

Emergency Response Unit: operational training enabling deployment at short notice at a disaster response.
Data Collection
The participants were invited to answer a questionnaire sent by email. It included 10 questions divided in subqueries (Supplemental Appendix A). The questions covered various psychosocial aspects related to pre-, during, and postdeployment such as stress management, sociocultural exposure, and attitudes from others. The questionnaire covered specific demographic data but also questions allowing qualitative open-ended answers. The questions were grounded on the specific concerns that the IFRC wished to investigate and in agreement with the authors of this study.
Data Analysis
Thematic analysis was used to analyze the data set (Braun & Clarke, 2006). A semantic approach is characteristic of this type of analysis. To begin with, all the answers were written down in an Excel sheet according to each questions and subqueries. The data information was ordered at a descriptive level concentrating on its semantic content and patterns. The questions included handling stress (Questions 3a–b), sociocultural environment (4), and attitudes (8). The data were transferred to a Word document to produce a relevant set of data in relation to the aim of this study. Issues concerning health (Questions 2a–d), teamwork, principles and behavior (5a–b), leadership and management (6a–c), and knowledge transfer (7a–b) have been published in another article (AUTHORS, 2018). Additional questions regarding demographic data (1a–h) were presented under “sample.” The questions “conclusions” (9) and “miscellaneous” (10) were treated as complementary information to this study.
To start with the analysis, the first author (S.P.-B.) read all the data to gain a global comprehension of its semantic content. Preliminary thoughts and relations collected while going through the text were written down. One more time, the data set was entirely read again, and items after items, prominent features were coded methodically and systematically. Color coding was used to visualize the ongoing analytic process. The semantic content associated with an item could contain a number of different codes. These codes were then grouped according to their differences and similarities. The codes that had comparable connotations were grouped together and represented possible themes. In turn, the potential codes were checked according to the semantic content, and then the themes were refined to cover the whole data set and finally given a final name. Examples of the data analysis were presented in this article, and the themes were highlighted through chosen extracts from the data set (Table 2).
Example of the Data Analysis of the Three Psychosocial Aspects.
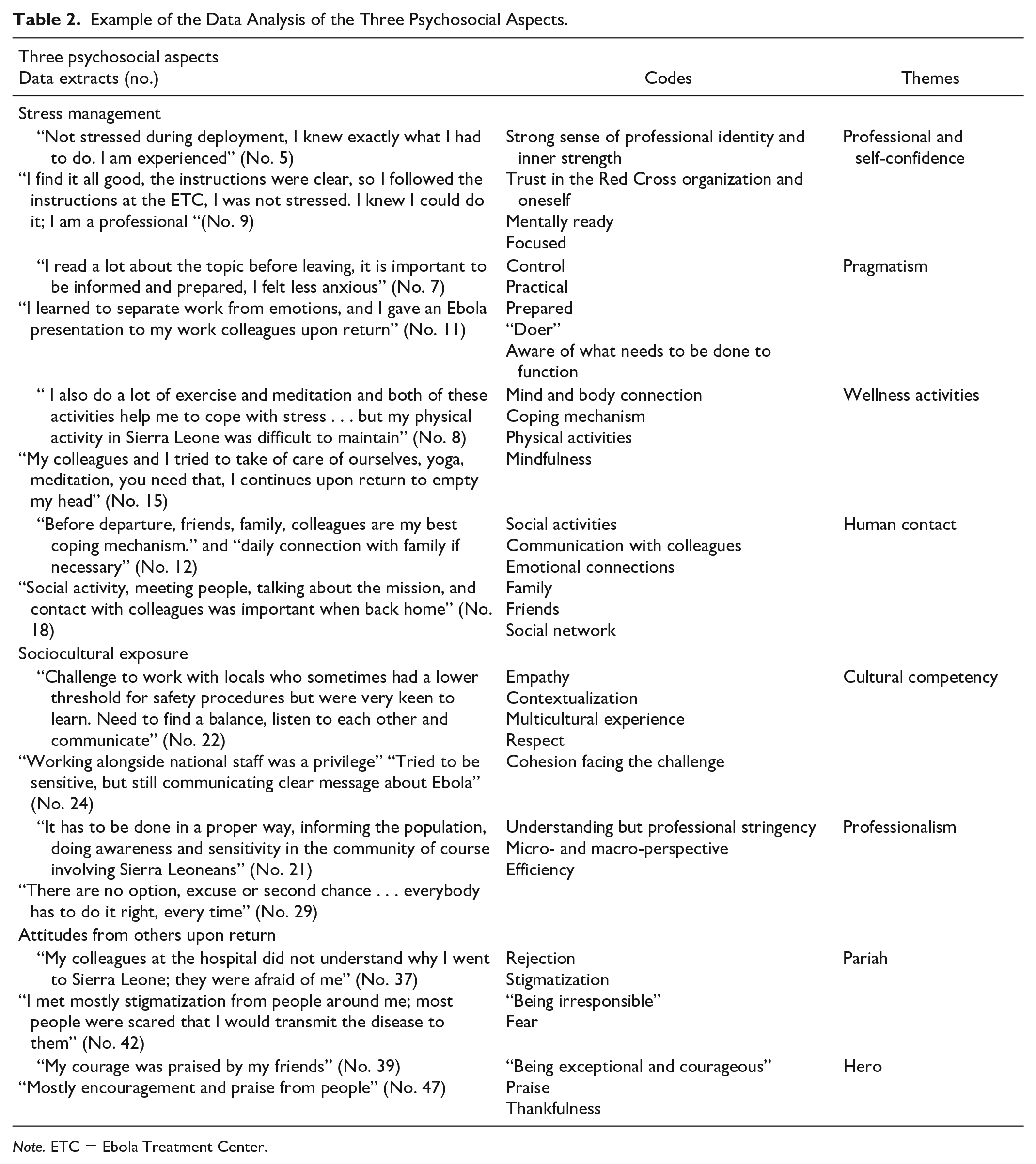
Note. ETC = Ebola Treatment Center.
A rigorous attention to trustworthiness and consistency was applied in this study. A pilot questionnaire was tested at the SRCUC on nurses who had been on assignments in similar crisis settings for the purpose of the validation process. Their responses allowed the researchers to refine the questions with a language more adapted to a humanitarian experience. These nurses also advised the researchers for more open questions allowing more feedback from the respondents. Finally, the questions were tested again on experienced Senior Health Advisors and Emergency Health Services Senior Officers working within humanitarian organizations. After several modifications, the questionnaire became acceptable to the researchers and was ready to be administered to the participants.
Although the analysis was primarily done by the first author (S.P.-B.), the other authors (J.H., P.S., and E.v.S.) were asked to verify the analysis and the results carefully. Consequently, some minor adjustments were made with the coding and a theme was renamed. Although the participants had worked specifically at an IFRC’s ETC, the results of this study are considered as transferrable to similar humanitarian contexts. The analysis was done independently of the IFRC that instigated this study.
Ethical Considerations
The principles of international ethical standards regarding interviews of participants, able to give informed consent to join voluntarily a study, were respected as well as the guidelines from Swedish Law (The Swedish Code of Statutes, 2003).
Ethical principles such as autonomy, integrity, and confidentiality of the informant were followed in accordance with the World Medical Association Declaration of Helsinki (The World Medical Association, 2013).
Results
A summary of the finding resulting from the thematic analysis of the three examined psychosocial aspects (stress management, sociocultural exposure, attitudes from others upon return) in relation to the deployment before, during, and after working at an ETC during and EVD outbreak is presented in Figure 1.

Summary of the findings: The three psychosocial aspects and their related themes.
Four themes were identified regarding stress management: professional and self-confidence, pragmatism, wellness activities, and human contact. All these four themes were present during the three time periods (pre-, during, and postdeployment period). Sociocultural exposure, specific to “the during deployment period,” resulted in two themes which are cultural competency and professionalism. Finally, two themes, pariah and hero, were identified in relation to the third psychosocial aspect which is attitudes from others upon return, particular to the postdeployment period.
Stress Management: Professional and Self-Confidence, Pragmatism, Wellness Activities, and Human Contact
Unexpectedly, considering the context, no participant admitted directly being stressed prior to deployment. However, practical concerns and worries, especially regarding the well-being of their family, were mentioned. Here is a representative quote: “I knew what I was doing and I felt capable but I felt responsible for my family . . . and everything they heard about Ebola on TV” (No. 4). Only one person suggested being stressed during deployment and disclosed: “ . . . of course it was stressful, but fear can be dangerous,” while six of them admitted feelings related to stress after deployment. Here is an example: “People around me do not understand what we lived through, sometimes they were even afraid of contamination . . . I am tired . . . I just need time to reconnect with my life” (No. 2).
Four themes were identified in regard to stress management: professional and self-confidence, pragmatism, wellness activities, and human contact The importance of professional and self-confidence were rather constant under the three periods so as pragmatism, shown respectively with the following quotes: “Good with previous experience, I was just eager to go” (No. 6) and “Upon return I was not afraid but I followed up the protocol. You do what you have to do” (No. 10). However, the prominence of wellness activities seemed to be less imperative upon return in comparison with the pre- and during deployment periods. This is expressed in the subsequent quotes: “Before leaving, it is important to engage in some form of exercise or listen to music. It helps with pressure” (No. 13) and “Especially during deployment, there was a need to exercise but it was difficult” (No. 16). The significance of human contact was described as a recurrent need at all three periods but even more so during deployment at the ETC as almost half of the participants reported it. This was shown by some of the participants: “In regards to traumatic events talking to colleagues was necessary under deployment” (No. 17), “I talked to my relatives and friends . . . I called a nurse who just returned to get more information” (No. 19), and “When back home, I also met with colleagues who had returned from Kenema and shared experience” (No. 20). In overall, the coping mechanisms seemed to shift from independence such as professional and self-confidence, and pragmatism prior to deployment to an increased need for contact with others during and after deployment. It corroborates with the apparent increase after deployment, in the need for contact with others with similar experience to deal with the emotional stress.
Sociocultural Exposure: Cultural Competency and Professionalism
The sociocultural exposure reflected the nursing staff’s level of professional and personal satisfaction regarding their cooperation with the international staff as well as their Sierra Leoneans national colleagues. These co-workers include the medical and humanitarian staff at the ETC in Kenema. Two themes were identified: cultural competency and professionalism. On overall, an overwhelming positive professional working environment dominated their account of this cooperation as 36 nurses reported adapting and collaborating well in the challenging environment with their international and Sierra Leonean colleagues. This general attitude is summarized in this quote: “No problem, only courage and hard work” (No. 23). Cultural competency and professionalism are closely related in this context but have nevertheless distinct implications. A noncompetitive, nonjudgmental, and accepting environment seemed to be the general working atmosphere between the different national backgrounds, which accounts for cultural competency. However, it was described that the Sierra Leonean colleagues did not always respect the professional standard in term of safety. One participant described this experience: “When working with the national staff I felt the constant need to be clear and consistent with the Red Cross guidelines due to the implications of Ebola transmission” (No. 26). Apparently, the international staff communicated this issue directly and effectively. Nonetheless, the remarks did not seem to affect the positive cooperation and the multicultural setting.
Attitudes From Others Upon Return: Pariah and/or Hero
Attitudes varied greatly toward the nurses upon return to their respective home countries after the mission at the ETC. It appeared that it was almost as common to be met as either a pariah or hero or both. Twenty-nine of the returnees experienced negativity and some even stigmatization. One participant reported, “My mother was not allowed by the day-care center to pick-up her grandchildren, the teachers were so afraid . . . they were influenced by what they saw in the media” (No. 35), and another nurse was told, “You will bring Ebola to Europe” (No. 31). Even within the medical profession, negative reactions were encountered. This was expressed by one of the participants: “I had expected that my colleagues at the hospitals would have a higher level of understanding of the disease” (No. 36). Twelve returnees reported only positive reactions as expressed in the following quotes: “My family was so proud” (No. 32) and “I just received congratulation and admiration” (No. 33). Sixteen of the returnees admitted meeting strong polar or mix reactions such as fear, anger from some but also admiration and praise from others. One participant expressed the following quote: “I met polar opposite reactions, either people were proud of the work we did or against it and angry to put the country at risk” (No. 45). The media was often criticized and considered as responsible by the nurses for dramatizing the situation, reporting fake or distorted information about Ebola, which had a negative impact on their life upon return. One nurse illustrated this thinking with this quote: “People see and hear false or incorrect information in the media and get scared for no reason” (No. 41).
In addition to the main findings, additional information added by the nurses under Question 10 of the questionnaire “Miscellaneous” (Supplemental Appendix A) are worth being reported in this article as the comments relate directly to the issue of stress. Twenty-seven nurses made some recurring suggestions related to the improvement of stress management. First, decreasing the workload seemed imperative as the stress and the fatigue can have fatal consequences. Second, increasing mental health support at each time periods, with more emphasis upon return. This is indicated in the following quote: “It is important to know that we always have the possibility to be in contact with a mental health professional when we need it and even more so when we come back from deployment” (No. 61).
Finally, the trustworthiness and reliability in the Red Cross as an experienced organization seemed to have a reassuring effect, positive impact on stress management and anxieties as 15 nurses wrote related comments. The following quote summarizes this believe: “I trust the Red Cross and its network . . . they know” (No. 57).
Discussion
This study explored the complex psychosocial experience of IFRC nurses upon their return from deployment at an ETC during an EVD outbreak between 2014 and 2015. It was found that the nurses coped with stress in a seemingly efficient manner before and during deployment through professional and self-confidence, pragmatism, wellness activities, and human contact. However, stress related to the aftermath of deployment was significantly higher, and contact with persons who had similar experience was often sought after. The sociocultural exposure was in large majority very positive through a combination of both cultural competency and professionalism. Finally, the attitudes from others upon return were often expressed as polar or mix reactions. The returnees reported that they could be perceived as pariah and/or hero. It was unanticipated and even more destabilizing when their medical colleagues back home had such ambiguous reactions. Based on those results, three common elements emerged: the delicate balance of trust in oneself and others, the “out of the ordinary” experience and stigmatization.
Despite the challenging task, the professional and self-confidence, pragmatism, cultural competency, and professionalism seem to be reinforced by a relatively strong sense of trust in oneself and others. The participants described themselves as self-reliant, resilient, and even “self-trusting.” They often expressed trust toward the Red Cross as an organization and trust toward their international and Sierra Leoneans colleagues at the ETC. A recent study shows that trust in the management of an organization buffers the negative effects of a demanding work among humanitarian aid workers (Visser et al., 2016). Most research investigating the relationship between trust and threatening environment has been done in a military context with a focus on dangerous settings (Sweeney, 2010; Sweeney et al., 2009). Such milieus are similar to high-risk situations involving global nursing within a humanitarian crisis. The results of those studies show and corroborate with our findings that trust in oneself and others are necessary components in challenging working conditions. Kramer (1999) argues that there are two main aspects of trust. One aspect emphasizes social and ethical trust and the other one highlights the strategic dimension of trust in relation to an organizational setting: trust as a psychological state and trust as choice behavior. This dynamic of trust described by Kramer (1999) is reflected in many of the participants’ responses.
Furthermore, it can appear indeed as a paradox or ambiguity that more than half of the nurses wrote suggestions in Question 9 (Conclusions) and Question 10a–b (Miscellaneous) about potential solutions on how to relieve stress while so few participants admitted experiencing stress directly (Questions 3a–b). The issue of trust in an organization and experienced stress are intrinsically related. In Antonovsky’s theory, the importance of strong sense of coherence (SOC) is presented as a factor facilitating (mental) health. People with a strong SOC tend to be able to move forward, when in a situation of stress (Antonovsky, 1996). Unfortunately, many nurses did not seem to have experienced this “sense of coherence” characterized by a feeling of confidence and trust in their working environment upon return from deployment. It could partially explain the increase in stress and therefore the need to be in contact with people who had shared similar experience.
“Out of the ordinary” is a thought that comes to mind when examining the responses given by the participants upon return of an EVD outbreak. It is rapidly understood that the context is humanly, psychologically, socially, professionally, and clinically highly unusual even for experienced nurses. Nurses, in general, are unwilling to present themselves as bold and brave individuals in the context of their profession. Even though, it is suggested at times that nurses are almost required specific emotional and spiritual predispositions. Indeed, modern nursing has been reluctant to consider nursing as a “vocational profession” which could be associated by some to motherhood, “feminity,” and even religion, which could therefore be perceived as a “de-professionalization” of the work (White, 2002). Jane Salvage (2004) argues that numerous nurses would feel uncomfortable defining their work as “vocation” but she argues that it is time to reconsider the meaning of the word “vocation” without implying a less value for the nursing profession.
Furthermore, one can wonder about the particular psychological profile, even personality types, of these nurses volunteering to work in the middle of an Ebola crisis, one of the deadliest viruses on earth for which there is no cure yet. To our knowledge, no studies have attempted to investigate the psychological profile of nurses working in such context. Yet, a cohort of 47 humanitarian workers from New Zealand completed the “Big Five” personality inventory and the results showed that these participants were significantly higher than population averages on openness and on agreeableness, but in contrast to the hypothesis, they did not differ significantly on either neuroticism or conscientiousness (Hudson & Inkson, 2007). These results suggest some interesting specificities regarding the psychological profile of these volunteers without being all conclusive. Turner (2014) discusses in her research the importance of resilience in the nursing profession as an emerging concept. She argues that nurses who are highly resilient are less at risk to show clinical signs of stress and it is more probable that they stay in the profession as skilled nurses. She claims that resilience is an imperative quality for nurses to possess because of the stressful nature of the profession of nursing. The “out of the ordinary” context of the study reveals an overall specific and even unique approach by the participants toward adversity and danger such as selflessness, self-reliance, empathy, and confidence. Therefore, we argue for further research regarding the psychological profile and personality traits of nursing volunteers in a VHF outbreak as it could increase preparedness and support related to deployment.
Stigmatization is intrinsically linked to the issue of trust, which was particularly challenged upon return as seen in some of the quotes. In the present study, it was found that human contact was highly valued and especially in the company of people who had similar experience and with whom they did not feel stigmatized. Recent studies regarding the last EVD outbreak in 2014 reported that stigmatization of “Ebola nurses” was not uncommon. Menzel (2015) describes, in an editorial, “nurses as scapegoats in Ebola virus disease” and the urgency to discuss the issue. Stigmatization is humanly and ethically not acceptable and it challenges gravely the psychological state of the health professionals. Humanitarian staff, including health care workers, are in the front line and stigmatization, provoked by fear and lack of knowledge in the community, which is a matter that needs more attention.
The questionnaire developed by the IFRC had for aim to understand how to prepare in a most efficient way the nursing staff that will be deployed in the future to viral epidemic outbreak. The authors consider that the questions fulfill the purpose of the study as the participants had the freedom to interpret the meaning of the questions and answer to them openly and accordingly.
This study has a global perspective as recruitment of nurses within the Red Cross Movement is done by the IFRC all around the world with the assistance of the National Red Cross and Red Crescent Societies. The gathering of data for this study was challenged by the difficulty to get in touch with nurses who engage in temporary missions around the world as almost 17% of the e-mails received via the IFRC were not active.
Limitations
All research has limitations that may potentially affect the results. First, in the case of the present study, it has been methodologically challenging to find informant-nurses because many of them were already engaged in a new assignment somewhere in the world with poor internet connection. Second, the response rate might be considered as low but as the focus, in this qualitative study, is on experiences instead of the number of participants, the responses from 44 nurses are still acceptable. Third, it could be understood as a limitation that no preexisting validated protocols were used. Therefore, to ensure that the participants would respond to the aim of the study, the questionnaire was tested, and in the course of validating the questions, a consensus was reached regarding the consistency of the questions. Finally, we believe that the results of this study are valuable even though the data were collected a few years earlier. Indeed, the findings are still most relevant in view of VHF outbreak and its implications for the Western world’s health care.
Conclusion
A key finding in this article focused on the mental health of nurses. There is a general sense of resilience, control, and optimism regarding stress, but at the same time, the need for enhanced mental health support emerges as an important recommendation to the Red Cross organization. In summary, it seems that the nursing staff demonstrates, as a trend, a particular sense of self-reliance before and during the mission. However, after deployment, the nurses often find themselves in a psychologically vulnerable state possibly due to a “less understanding” psychosocial environment, being isolated from colleagues with similar experience. Therefore, it is during this vulnerable period that an emphasis on specialized mental health support should be planned consistently.
In addition, further research is suggested to examine the psychological dynamic of the nurses working at an ETC. It consists of the delicate balance of trust in oneself and others, characterized by resilience during an “out of the ordinary” context and the ability to deal with psychological vulnerabilities during that period. This type of research should be done not only at the micro-level among nurses but also at the macro level of organizations such as the IFRC, WHO, and MSF. Indeed, these organizations have the responsibility to offer professional mental health support to their staff to avoid neglect and break away from the frequently general belief that the nursing staff is “by nature” resilient. This issue also connects to interrogations regarding specific personality types tending to have the capacity to work in challenging environment. Finally, organizations such as the Red Cross, working with volunteers, need also to consider the mental health of these unpaid workers. Many Red Cross volunteers from the national societies in West Africa were engaged in the Ebola crisis and were left with psychological and social vulnerabilities.
Finally, the issues of psychological vulnerability and stigmatization are often present in their environment upon return. Several nurses have described the negative impact of the media provoking a feeling of powerlessness. Incorrect journalistic statements, fake information and sensationalism, are often blamed for exacerbating fear, which could turn nurses into pariahs in the eyes of the community. It is therefore suggested to improve cooperation with the media in such context.
Supplemental Material
Appendix_A_2020 – Supplemental material for Nurses in an Ebola Viral Hemorrhagic Fever Outbreak: Facing and Preparing for Psychosocial Challenges
Supplemental material, Appendix_A_2020 for Nurses in an Ebola Viral Hemorrhagic Fever Outbreak: Facing and Preparing for Psychosocial Challenges by Stéphanie Paillard-Borg, Jessica Holmgren, Panu Saaristo and Eva von Strauss in SAGE Open
Footnotes
Acknowledgements
The authors thank the nursing staff for participating in the study.
Author Note
Jessica Holmgren is now affiliated to Mälardalen University, School of Health, Care and Social Welfare, Sweden.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Swedish Red Cross University College.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.