
Abstract
Epidemiological transition, population ageing, and pandemics posed new challenges to the health system. Current global situation demands many new competencies within the scope of teaching public health in medical schools. The aims of this study were to identify the needs of public health competencies for medical doctors in Thailand and to assess the level of integration for technical collaboration in teaching public health. The national survey of all Thai medical schools applied the list of public health competencies framework recommended by the World Health Organization, Southeast Asia Regional Office (WHO-SEARO). Qualitatively, community representatives from 11 sample villages were interviewed in the focus groups and representatives from stakeholder organizations, particularly employers in the in-depth interviews. Data integration applied recursive mixed-method approach. While the survey identified that health economics, disaster management, leadership, and teamwork are not well addressed in curriculum, employers, and national health authority uttered the need to strengthen the health system sciences and leadership in new generation medical doctors. Almost two third of medical schools could not apply interdisciplinary integration to teach such public health subjects. Furthermore, experiential learning and role play are recommended, in addition to the usual teaching method and multiple-choice questions. Thai communities expect doctors to serve the community, lead the primary healthcare team and train the health professionals and community health volunteers. Therefore, future medical doctors require interdisciplinary competencies. The findings of this study may provide evidence to step forward to a national framework of public health core competencies and interdisciplinary collaborations.
Plain language summary
As we know prevention is better than cure, public health, the art and science of preventing diseases and promoting wellbeing of the population, deserves to be a priority subject in medical schools. Current global situations such as population ageing demand many new competencies within the scope of teaching in medical schools. The aims of this study were to identify how faculties think about the needs of public health competencies for medical doctors in Thailand and to assess how multi-disciplinary experts work together in teaching public health. The researchers invited all Thai medical schools to this survey in 2017. They applied for a check list developed by experts of World Health Organization, Southeast Asia Regional Office (WHO-SEARO) and surveyed medical schools. Then the researchers listened to the community representatives from 11 sample villages across the country and representatives from stakeholder organizations such as the Ministry of Public Health. They investigated survey data and interview narratives to understand the situation and construct future recommendations. The survey identified that health economics, disaster management, leadership and teamwork are not well addressed in curriculum whereas employers and national health authority uttered the need to strengthen the health system sciences and leadership in new generation medical doctors. One third of medical schools could not apply interdisciplinary integration to teach such public health subjects. Furthermore, experiential learning in the community and role play techniques are recommended as learning approaches to apply in public health education. Thai communities expect doctors to serve the community, lead the primary healthcare team and train the health professionals and community health volunteers. The findings of this study may provide evidence to step forward to a national framework of public health core competencies and interdisciplinary collaborations.
Introduction
Public health competencies and health system-oriented practices are essential components in the education of the new generation of medical doctors in the 21st century (Duvivier et al., 2015). Epidemiological transition demands newer competencies of medical graduates (Duvivier et al., 2015). New-generation medical doctors require system-oriented, multidisciplinary approaches to tackle the challenges facing health systems and address epidemiological transition, population aging, and demographic transition, along with climate change, disasters, and pandemics. Consequently, medical schools are tasked with nurturing doctors who can respond to all these changes. Research triggering transformative changes in educational institutions and medical schools has become mandatory in order to align medical education, especially public health competencies, with health system changes.
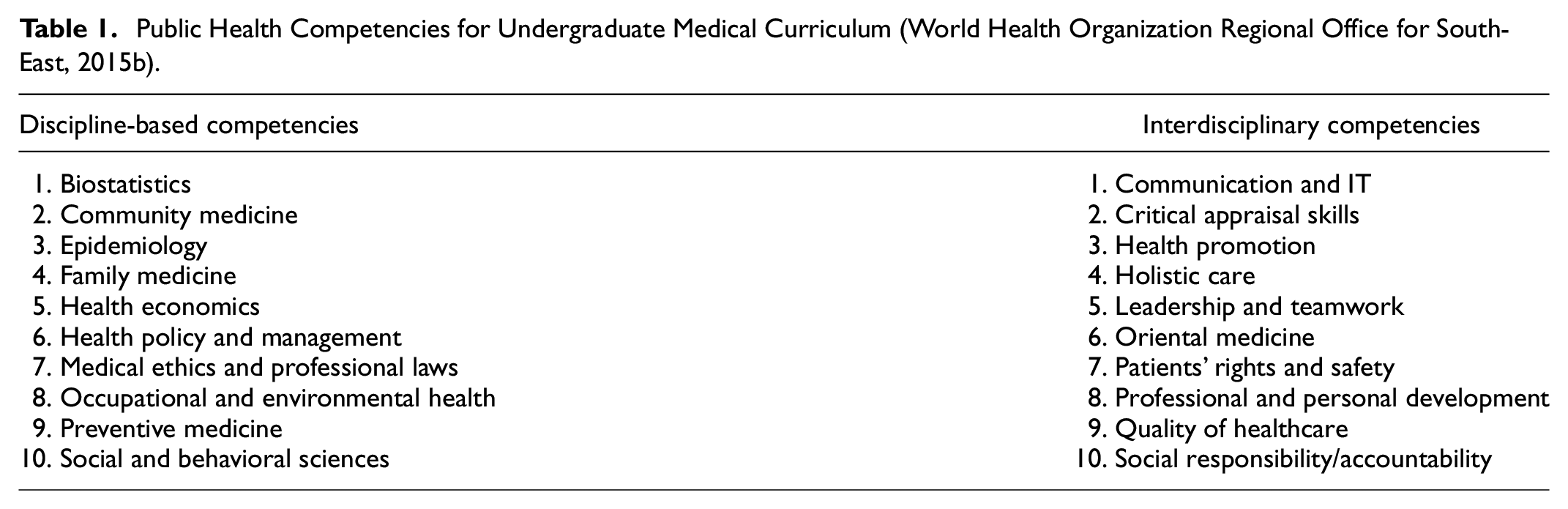
Public health core competencies are the essential sets of knowledge skills and attitudes transcending the boundaries of disciplines, independent of programs and topics. Recently, the World Health Organization, Southeast Asia Regional Office (WHO-SEARO) published a teacher’s guide for training those teaching public health in undergraduate medical schools (Teacher/Facilitator Guide: Regional training programme on improving teaching of public health in medical schools in the South-East Asia Region, WHO SEARO, 2015; World Health Organization, 2014; World Health Organization Regional Office for South-East, 2015a) and defined the competencies regionally after a series of expert meetings (World Health Organization Regional Office for South-East, 2010). Afterward, a regional level training of master trainers was organized in January 2015 (Teacher/Facilitator Guide: Regional training programme on improving teaching of public health in medical schools in the South-East Asia Region, WHO SEARO, 2015; World Health Organization Regional Office for South-East, 2015a). It produced specific training outcomes and hints for further implementation to improve teaching public health in each countries (World Health Organization Regional Office for South-East, 2015b).
Many countries have developed core competencies in public health to be applied by all medical schools (Chamberlain et al., 2008; Finkelstein et al., 2008; Institute of Medicine, 2003; Johnson et al., 2008; Kaufman et al., 2015; Morley et al., 2017; Core Competencies for Public Health in Canada, Public Health Agency of Canada, 2014; Zenzano et al., 2011) such as India, South Africa, Canada, and United Kingdom (Dankner et al., 2018; Gillam & Bagade, 2006; Gillam & Maudsley, 2010; Institute of Medicine, 2003; Johnson et al., 2008; Shewade et al., 2017). Recently a framework to evaluate such efforts for teaching public and population health in medical education was introduced in the United States.(Johnson et al., 2020) A recent meta-analysis identified the lack of consensus about scope and competency level of public health is as a major challenges and integration of public health subject to others subjects as a solution (Abdul Kadir & Schütze, 2022), Therefore it is important to conduct nation-wide assessment of the public health instruction in medical schools. Furthermore, such a study that can provide information about current core public health competencies taught in undergraduate medical schools has yet to be conducted in Thailand and countries in Southeast Asia (Lyon et al., 2016).
Thailand is expected to become an example of how to initiate transformative changes to improve public health teaching in medical schools. In Thailand, medical curricula are defined not only by the medical faculties, but also by important stakeholders such as employers, accreditation bodies, and the public in each country; therefore, they are highly contextual. Likewise, the competencies prioritized in each country are different.
The curricula of all medical schools in Thailand are reviewed and revised every 6 to 7 years to be up to date before being approved by the Medical Council of Thailand. In 1971, the Thai Medical Consortium organized the third National Medical Education Conference and set up a policy to improve the teaching of medical students by adding social and preventive medicine into the curriculum. In addition to the new subjects, the medical students were sent out to provincial hospitals to gain more clinical experience. In 2012, the Medical Council of Thailand revised the standard of the medical curriculum by adding the content of community medicine, so that every medical school would teach their students similar subjects. The eighth National Medical Education Conference was held in 2009, with the theme “People-Centered Healthcare.” It was suggested to revise the curriculum by integrating “patient safety” into the curriculum. This way, it was expected that, after graduation, doctors would be able to provide healthcare to the majority of people sick with common diseases and also for the population’s health. The suggestion also emphasized holistic care and included prevention, rehabilitation, and health promotion. This provides clear evidence that public health has been incorporated into the medical curriculum.
The theme of the ninth National Medical Education Conference in 2015 was “Revise Medical Education for the Future Doctor.” Important recommendations for medical schools were made, such as the following: (a) “To organize the healthcare delivery system of Thailand to be the most efficient, it needs to have doctors working in both government and private sectors with appropriate competency. The appropriate competency means that the doctor can be a specialist, general practitioner, teacher, researcher, or administrator. So, the medical schools should manage the way to produce different kinds of doctors”; (b) “Medical education should be of international standard but suitable for the Thai context. Medical schools should set the goals for their competencies that can respond to the needs of the health system and their lifestyle.” From these policies, it can clearly be seen that the goal to distribute doctors to cover the population adequately was set. Lertrattananon et al. (2019) reported on the opinions of 28 residents training in family medicine in Thailand, regarding their public health competencies while they were medical students. These residents reported that they were weak in communication with patients, care of emergency cases, and care of gynecologic and pediatric cases, and they did not have enough work experience in the community.
In Thailand, all medical curricula must be approved by the Medical Council of Thailand. However, there is no agreement about the contents of the public health curricula. During preparation for the ninth National Medical Education Conference in 2015, the second subcommittee analyzed the curricula and found that each medical school had different contents and a different emphasis on community medicine and family medicine. This stimulated us to study the situation of public health content in the curricula of undergraduate medical schools in Thailand.
The general objectives of this study were to identify the needs of public health competencies for medical doctors in Thailand and to assess the level of integration for technical collaboration in teaching public health. The specific objectives were (a) to explore how regionally defined public health competencies are prioritized and being addressed to teach public health in undergraduate medical schools in Thailand and (b) to identify the need for public health competencies for the health workforce in the view of employers (c) to understand how people expect from medical doctors to contribute to public health in Thailand. The findings of the study are expected to provide evidence suggesting the areas of integration among medical schools and also among departments teaching public health. Ultimately, we hope to set a national framework of public health core competencies for Thai medical schools to serve as a common platform for interdisciplinary collaborations and transformative changes.
Materials and Methods
It was a mixed-method study in which quantitative and qualitative data were collected recursively in multiple steps applying the convergent parallel design (QUAN →← QUAL). Quantitative and qualitative data were collected recursively in multiple steps. The quantitative part is the national survey of all medical schools in Thailand. The survey used the list of public health competencies framework recommended by the World Health Organization, Southeast Asia Regional Office (WHO-SEARO) to find out how those were being addressed in teaching undergraduate medical students at medical schools across the country. A total of 17 out of 21 Thai medical schools participated in the national survey. Qualitative inquiries applied 11 focus group interviews of community representatives from sample villages and in-depth interviews of representatives from stakeholder organizations, particularly employers. The quantitative analysis applied descriptive analysis using STATA 15, and the qualitative findings were validated by interrelating the meaning of themes from word clouds created in NVivo 12. The quantitative study applied systematic measurement regarding teaching public health in undergraduate medical schools whereas the qualitative study explored how the community understood the meaning of public health and the viewpoints of stakeholders who are major employers of medical doctors. Finally, the data integration was applied in a mixed methodology (QUAN →← QUAL) approach in which the quantitative and qualitative investigations were simultaneously carried out and the findings of each approach were interpreted in an integrated manner to lead to conclusions.
This study was implemented in the following steps:
Stakeholder meetings and analysis.
Data collection and analysis through national survey.
Focus-group interviews.
In-depth interviews.
Stakeholder Meetings and Stakeholder Analyses: Identifying stakeholders is the very first step of participatory action research which entails the measurement of the problem, reflection on the problem, the participation of stakeholders to construct changes leading to a transformative action plan, and execution (Martí, 2016). This comprises research, participation, and action. However, this article reports mainly the results from the research part of the PAR cycle as the subsequent processes are ongoing with the participation of stakeholders from around the country following this publication. The stakeholders participated in research design, instrumentation, and data collection. The stakeholders in terms of power, interest, and legislation relating to the improvement of teaching public health in medical schools in Thailand were identified as follows:
1. Faculties that teach public health in medical schools.
2. Researchers of the current project.
3. Representatives of authoritative bodies:
3.1. Medical Council of Thailand.
3.2. Ministry of Public Health.
3.3. Rural Doctors Association.
4. Community practice: public health educators.
Mixed-method approaches: A quantitative methodology and qualitative inquiry were applied and interrelated to obtain a comprehensive answer and action model to improve the teaching of public health in medical schools. Data that are meaningful and stimulatory to start a change are essential to begin the PAR cycle. The study comprised the following data to synthesize an action model (Tavakol & Sandars, 2014):
1. National survey.
2. Qualitative inquiries:
2.1. Focus group discussions with the communities.
2.2. In-depth interviews with the employers.
National Survey
A survey instrument was developed by a team of authors with stakeholder participation and sent to the national experts, the Department of Human Resources for Health and Fellowship, WHO-SEARO experts, and foreign experts to validate its contents. It is provided in the Supplemental Appendix.
Study Population
The study population comprised all 21 medical schools in Thailand. For the national survey, the sampling frame consisted of all medical schools in Thailand providing an MD degree. A mailing survey approach was applied.
Respondents of the Survey
The survey questionnaires were sent to all medical schools in Thailand by addressing them directly to the dean of the medical schools and also to the head of the department teaching public health. Two participants from each institution were invited to participate in the study: (a) the dean of the medical school and (b) the person most responsible for teaching public health in each faculty of medicine.
For qualitative inquiries, purposive sampling was applied to include medical schools from different provinces that were different in terms of geography, demography, sociology, and epidemiology.
Survey Data Collection
The Institutional Review Board approved this study. The approval of each medical school and the informed consent of each respondent were acquired for data collection.
The survey data collection from August 2017 to December 2018 consisted of three sources of data:
Structured questionnaires.
Open-ended questionnaires.
Curricula maps.
Structured Questionnaires: A questionnaire was carefully prepared to be respondent-friendly. The instrument was developed and finalized with the participation and consultation of stakeholders. The content of the survey instrument was thoroughly checked to be congruent with the objectives of the study. A panel of experts secured the validity of the instrument by carefully checking its content and face validity. A pilot study was conducted before the actual survey to test how comprehensive and time-consuming the questions were to make it respondent-friendly.
Secondly, the curriculum map was requested from each faculty. According to the present study objectives, researchers aimed to seek evidence-based practices to improve the teaching of public health in medical schools. The survey aimed to acquire representative evidence that might challenge the conventional way in which the curricula are modified.
The investigation of the following areas was carried out:
Public health competencies, such as disciplinary and interdisciplinary competencies, currently being addressed in each medical school.
Local faculties’ opinion relating to priority of the WHO-recommended public health competencies (Table 1) in each school.
Integration level among departments teaching public health and other competencies.
The country’s need of specific competencies in medical graduates.
The teaching staff or academic workforce’s delivery of those competencies to students.
Techniques applied in teaching public health subjects (Teacher/Facilitator Guide: Regional training programme on improving teaching of public health in medical schools in the South-East Asia Region, WHO SEARO, 2015; World Health Organization, 2014);
Techniques applied in assessment of public health subjects (Teacher/Facilitator Guide: Regional training programme on improving teaching of public health in medical schools in the South-East Asia Region, WHO SEARO, 2015; World Health Organization, 2014);
Evaluation of public health courses within the medical curriculum.
Public Health Competencies for Undergraduate Medical Curriculum (World Health Organization Regional Office for South-East, 2015b).
Open-Ended Questions: The survey followed a systematically structured quantitative approach to find the current situation of public health teaching in medical schools. A few open-ended questions were embedded in the survey instrument to explore the free ideas of the respondents beyond the structured questions. After the survey findings, the adequacy of the information and evidence was assessed.
The structured questionnaires were sent to medical schools through the national networks of medical education such as the Thai Medical Consortium. The content of the questionnaires covered the following topics:
Public health competencies taught in the current public health curriculum (Table 2);
Priority of regionally defined competencies in each regional context.
Perceived barriers for implementation.
Required support for sustained activity.
The Situation of Addressing Regionally Defined Public Health Competencies in Medical Schools of Thailand (2017).
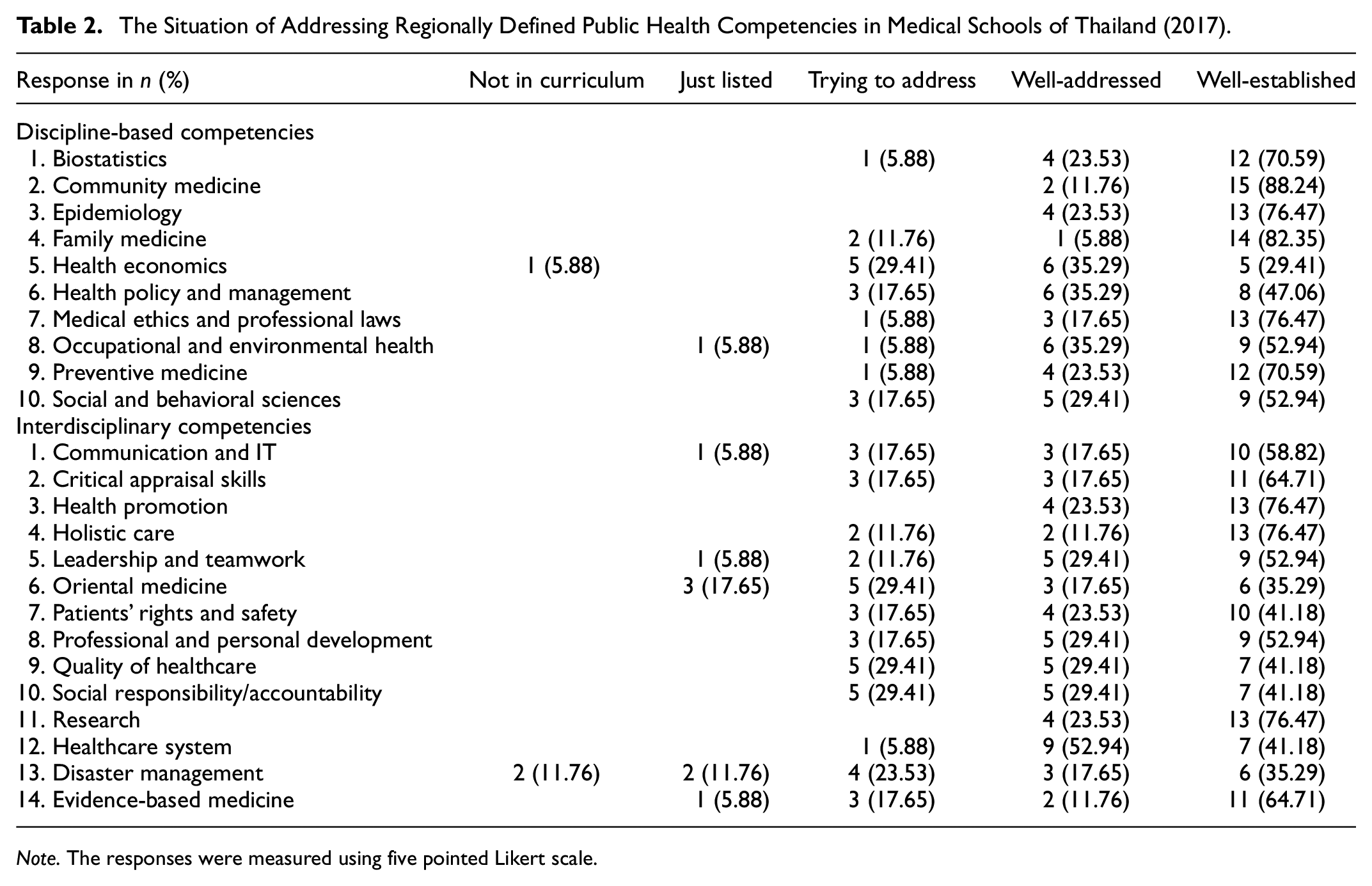
Note. The responses were measured using five pointed Likert scale.
Survey Data Analysis
The survey data were analyzed using a descriptive approach presenting the mean, median, and percentage using STATA SE version 16. The qualitative data were collected by Thai researchers and translated into English after confirmation by at least three researchers who spoke both Thai and English. Afterward, the narratives were coded into themes. In addition, the narratives were analyzed using word cloud analysis in NVivo 12 Plus.
Qualitative Inquiries
A qualitative approach was applied (a) to understand the expectations of people in different Thai contexts relating to the health competencies of medical graduates and (b) to understand the expectations of organizations and employers relating to the public health competencies of medical graduates.
We sought to better understand how people, in different contexts of the Thai communities, defined the meaning of public health medicine and health system-oriented practice. The public health competencies advised by the WHO and adopted at the national level might or might not sufficiently address the needs of the community served by each medical school (Stalmeijer et al., 2014; Tavakol & Sandars, 2014). Researchers, therefore, proposed this qualitative part of the study to explore the meaning and the importance of public health reflected by the communities and the services they expect from future medical graduates. Therefore, it was important to appropriately identify the setting and participants for this study. The medical education researchers visited the communities served by the medical schools. Thailand has several areas of differing contexts in terms of public health needs, and social and cultural diversity. Therefore, researchers chose the locations using a purposive sampling approach as shown in Figure 1. The communities in urban areas, rural areas, border areas, and disaster-prone areas, across all regions of Thailand, were purposely selected as the study site communities. A field study was applied via focus group discussions to gather data from the key informants of the community. These informants were interviewed via focus group discussion to better understand their expectations of the contributions of medical doctors in the scope of public health and health system-oriented approaches. The focus group discussions comprised the following stakeholders: (a) the local leader of the lay board, (b) health volunteers, (c) attendants of primary care units, (d) family members of the attendant, and (e) nurses from primary care units. The team comprised a researcher, an assistant researcher, and a note-taker. The narrative inquiry did not pose any serious ethical problems. The participants’ privacy and their sense of security were assured by informing them about the study before beginning the focus group discussion. Local medical schools were requested to assist in organizing the focus groups. The data were recoded as notes and audio records.
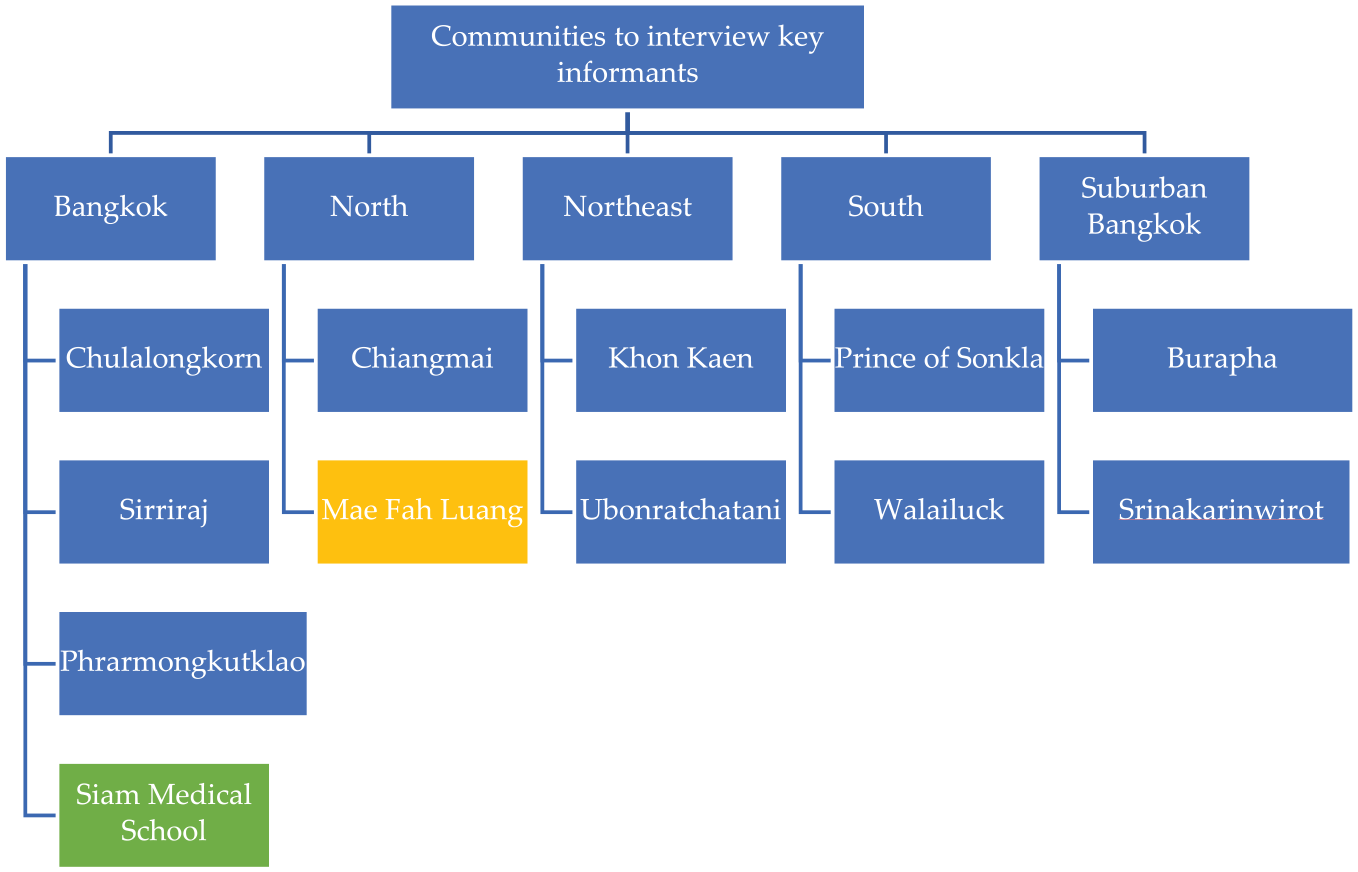
The selection of communities for qualitative inquiry in the communities.
The analysis was undertaken by way of content analysis as soon as data saturation was reached. The people’s opinions of the need for public health competencies were recoded, categorized, and summarized into the public health competencies. These narrative inquiries were undertaken to investigate the context-specific public health education and competency of medical doctors. The findings were validated by interrelating the meaning of the themes. Subsequently, the findings were interpreted carefully to see the similarities and differences among the findings from the survey, the findings from interviews with employers, and other concurrent study findings.
These narrative inquiries attempted to investigate the context-specific public health education and competency of medical doctors. The findings were validated by interrelating the meanings of the themes. The analysis applied word clouds in the NVivo 12 software.
Focus Group Discussion with the Communities The focus group interview content was prepared to identify the expectations of the communities with respect to the contribution of medical doctors in the scope of public health and health system-oriented approaches.
The following focus group questions were answered by the interviewees:
Engagement question: When was the last time you met a medical doctor for yourself or another person?
What was your experience of a medical doctors’ service for the community?
What is your expectation of the medical doctor for the community?
What is your opinion and experience of a medical doctor as the leader of the team serving the community?
Is there anything else you would like to say about doctors’ engagement with the community?
The focus group discussion comprised the following stakeholders: (a) local leader of the lay board, (b) health volunteers, (c) attendants of primary care units, (d) family members of the attendant, and (e) nurses from primary care units. A total of 11 multi-stakeholder focus group discussions were conducted in primary healthcare settings (Figure 1).
In-Depth Interviews Exploring the Needs of Employers
There remained a gap and clear necessity to highlight the view of multiple stakeholders with a direct interest in the public health competencies of the medical graduates. Thus, additional narrative inquiries were conducted in the form of in-depth interviews. The interviews were arranged with the following stakeholders:
The Ministry of Public Health (MOPH) permanent secretary and heads or representatives of related departments.
The Association of Provincial and Regional Hospital Doctors.
The representative of the Thai Medical Council of Thailand.
The trustworthiness of the research findings was built by eliciting the standpoints of medical teachers, institutions, employers, and the public. Invitation letters were sent to the above persons to make an appointment for interview by the research team. In the interview, the interviewer explained the proposal and showed the table of competencies to the interviewees. The interviewees were asked to comment on the list from their perspective as employers.
Following the aim of highlighting the view of multiple stakeholders with a direct interest in the public health competencies of medical graduates, narrative inquiries were conducted in the form of in-depth interviews. The trustworthiness of the research findings was built by considering the standpoints of medical teachers, institutions, employers, and the public.
The interview results were recorded and statements were analyzed in a tabular form. Each statement representing an idea of the responder was counted to obtain the frequency of the same idea across all sites. The most frequent ideas were listed as matters of priority. Subsequently, the ideas were listed in order of priority, representing the needs of the communities.
Results
Results and Discussion of National Survey
Respondent Information
We invited all 21 medical schools in Thailand. There were 19 replies from 17 medical schools. Two medical schools sent two replies. Therefore, altogether, there were 17 respondents, yielding a response rate of 80.95%. The oldest medical school was 131 years old, and the youngest was 11 years old as of 2019. All of the medical schools were more than 10 years old. The median age of the establishments was 29 years old. Schools aged ≥30 years were classified as “old,” while those aged <30 years were classified as “new”; 47.6% of the medical schools were “old.” The number of students enrolled in each medical school ranged from 32 to 313 per year. The median number of students enrolled per year was 135. Schools enrolling ≥100 students per year were classified as “big” schools, while those enrolling <100 students per year were classified as “small” schools; 58.8% of the medical schools were “big.” Regarding accreditation, 76.4% of the medical schools received recent accreditation from the World Federation for Medical Education (WFME) or Institute for Medical Education Accreditation (IMEAC). The number of teachers was significantly different between “old” and “new” schools and between “big” and “small” schools. There were only three private schools.
In 2016, WHO-SEARO introduced a set of defined competencies recommended for medical schools in Southeast Asia. We applied this set to find out how the medical schools addressed them (World Health Organization, 2014; World Health Organization Regional Office for South-East, 2010, 2015b).
The survey sought information regarding (a) the public health competencies including both disciplinary and interdisciplinary competencies which were currently being addressed in each medical school (Tables 1–3), (b) the local faculties’ opinions about the priority of the World Health Organization (WHO)-recommended public health competencies in each school (Table 4), (c) the integration level among departments teaching public health and other competencies (Table 5), and (d) the country’s need for specific competencies in medical graduates (Table 6).
Faculties’ Opinion on Priority of the WHO-recommended Public Health Competencies in Medical Schools of Thailand (2017).
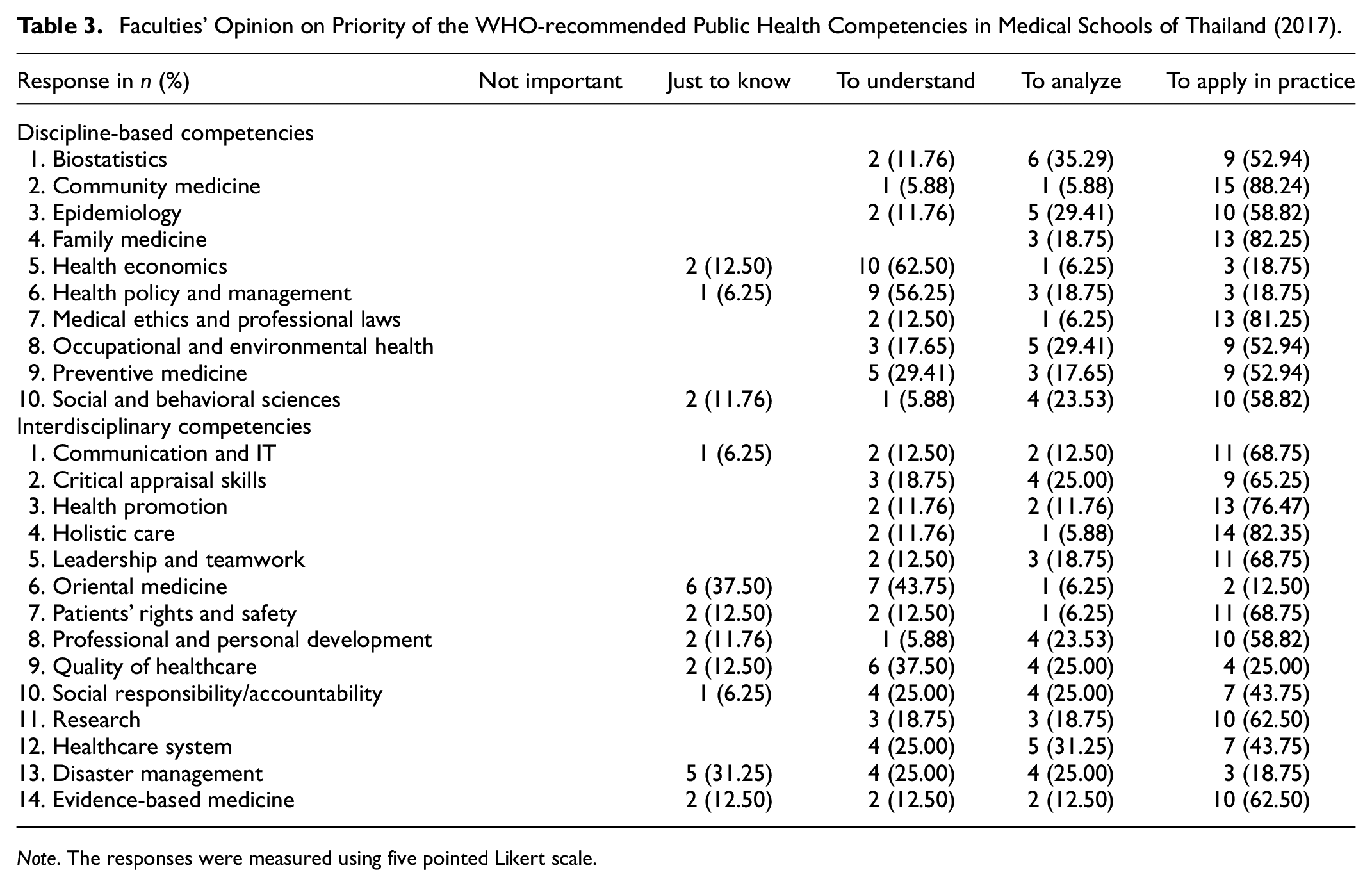
Note. The responses were measured using five pointed Likert scale.
Integration Among Many Departments to Deliver Public Health Competencies in Undergraduate Medical Schools in Thailand (2017–2018).

Note. The responses were measured using five pointed Likert scale.
Country’s Need for Public Health Competencies in Medical Graduates in Thailand (2017–2018).

Note. The responses were measured using five pointed Likert scale.
Summary of the Communities’ Expectations of Medical Doctors: Qualitative Findings from Focus Group Interviews in the Communities Across Thailand.

Current Situation of Addressing Regionally Defined Public Health Competencies
The discipline-based subjects were found to be better addressed than the interdisciplinary competencies. The disciplinary-based competencies are basic competencies in public health and most medical schools have traditionally addressed these disciplines. With the changing health problems and newer challenges to the health system, new competencies require the integration of multiple specialists. Some competencies were not addressed in many medical schools. Health economics, for example, was yet to be addressed in more than 25% of the medical schools. The interdisciplinary competencies may also be delivered not only by the public health department but also by the other departments. However, some interdisciplinary competencies such as the healthcare system and health promotion were mostly confined to the public health departments. Health promotion was addressed in all medical schools, whilst the healthcare system was addressed in almost all schools, with one school answering that it was trying to address it.
Priority of Public Health Competencies
We asked the following question: “The priority of public health competencies is different in varying places and countries. How does your medical curriculum give priority to following public health competencies in the undergraduate medical curriculum?” (Table 3)
The Thai medical schools generally follow the guidance of the Thailand Medical Council. They all conform to regulations set by the Thailand Medical Council with accreditation according to the WFME. However, they are autonomous with respect to selecting the competencies and crafting the content of their curricula. Two medical schools answered that health economics was on a “just to know” basis, and only one school answered that health policy and management was “just to know.” This highlights the level to which these two competencies are addressed, as shown in Table 2. When possible, it is necessary to discuss with the faculties teaching public health what competencies they consider teaching, as well as why and how. Among the interdisciplinary competencies, more than one-third of medical schools answered that disaster management was on a “just to know” basis. It is necessary to further explore this to see whether it is addressed by departments other than those teaching public health.
Integration in Teaching Public Health
We asked the following question: “Integration among multiple departments may have been designed to teach a broad range of public health subjects in your medical school. What level of integration exists to address the public health competencies in the undergraduate medical curriculum of your school?” (Table 4)
The results showed that there was a high level of integration in Thai medical schools to deliver interdisciplinary competencies. (Table 4) Regarding the healthcare system, however, almost half of the schools did not integrate it. The same was observed for disaster management, health policy and management, and health economics. Considering the need to address those subjects in many schools, we should find out how to integrate them among the faculties within a school or faculties, enabling expertise beyond the schools.
Country’s Need for Public Health Competencies in Medical Graduates
We asked the following question: “To what extent do current medical graduates possess public health competencies? This answer will assist preparing the need forpublic health competencies in future doctors.” (Table 5)
The purpose of this question was to determine the faculty’s opinion on the current graduates’ strengths and the possible need to strengthen the competencies of future graduates. The responses showed that interdisciplinary competencies were considered as needing to be strengthened. This result is important and matched with the qualitative findings. The faculties’ answers highlighted the need to strengthen health economics, health policy and management, and disaster management. Another competency to strengthen was social responsibility and accountability. This competence could also be addressed by other departments in medical school. Regarding Oriental medicine, as well as leadership and teamwork, the findings pointed out that these areas also needed to be strengthened as the community sees doctors as leaders. However, stakeholders in Thailand should discuss and decide on their need for Oriental medicine competency from the MDs.
The study showed that 35% of medical schools did not have integration to deliver public health competencies in Thailand (2017–2018) (Figure 2).

Proportion of medical schools in Thailand which had system integration to deliver public health competencies in 2017.
Teaching Methods Applied in Teaching Public Health in Undergraduate Medical Schools in Thailand
Teaching methods applied in the delivery of public health in medical schools were explored.
The colored graphs above clearly show how different methods are applied by departments teaching public health in Thailand (Figures 3 and 4). Community-based learning (yellow) and self-directed learning (green areas) indicate that the departments applied experiential learning and active learning strategies in delivering the public health competencies. Disaster management was mostly taught via lectures. This probably indicates that the drills and simulation games were not yet available. Resources, infrastructure, and collaboration is fundamental for this topic. Evidence-based medicine was taught mainly by lectures but also required small group discussions and seminars. Health economics was uniquely delivered through web-based lectures unlike many other discipline-based competencies (Figure 4).

Teaching methods currently applied in the delivery of disciplinary-based competencies of public health.
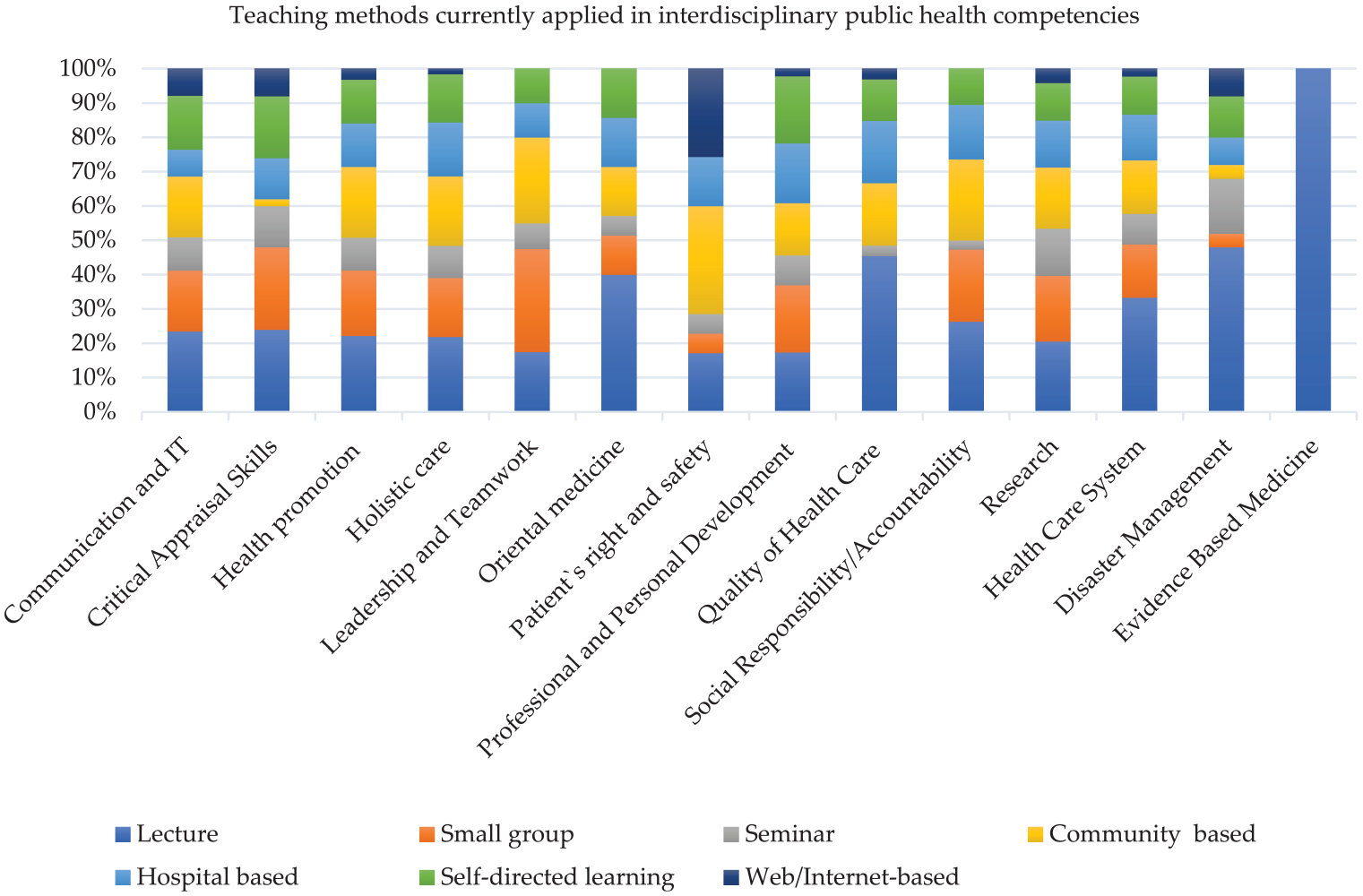
Teaching methods currently applied in the delivery of interdisciplinary competencies of public health.
Assessment Methods Applied in Teaching Public Health in Undergraduate Medical Schools in Thailand
In Thai medical schools, the community and family medicine departments applied different methodologies for the assessment of public health competencies (Figures 5 and 6) (World Health Organization, 2014). The use of multiple-choice questions (MCQs) was the main methodology for the assessment of discipline-based competencies. Interestingly, the presentation of projects was clearly applied in the assessment for both research and health promotion. There was no assessment for oriental medicine, social responsibility, and disaster management in the Thai medical schools, reflecting the results of the competencies shown in Table 5.

Assessment methods currently applied in undergraduate medical schools for discipline-based competencies in Thailand (2017–2018).

Assessment methods currently applied in undergraduate medical schools for interdisciplinary competencies in Thailand (2017–2018).
Results of Qualitative Inquiries
Results of Focus Group Interviews
Most of the participants’ discussions were based on their experiences of meeting a doctor at the hospital for treatment and advice. Their impression of the visits showed that they were satisfied with the doctors’ advice. The findings were based on people’s expectations of medical doctors in the community setting. Two different questions were used, but the answers reflected the same opinion after analysis of coded words using the word cloud. They expected that doctors should visit the community, provide advice in the primary health care unit (PCU), and educate the people regarding health. (Table 6)
The FGD results indicated people’s expectations of future medical doctors. Community residents may not have much opportunity to see a doctor. The findings indicate that they want doctors to visit the communities more often to provide advice to PCUs, conduct home visits to bedridden patients, and educate people in the communities. Regarding the doctor’s role and leadership in the community, most opinions point out that doctors rarely come to the community, typically only visiting the communities for health promotion and prevention campaigns. It is interesting to have a better understanding of how community residents perceive the doctor’s role, as shown in Figure 7. According to this finding, community-integrated projects or campaigns may serve to improve the engagement between doctors and the community. However, at the time of our study, most of the communities did not have a doctor and were instead served by the primary healthcare team. This represents a public health project that can be implemented by departments teaching public health. Lastly, the interviews sought to determine the types of competencies the doctors were expected to have. They were expected to get in touch with the community more often, lead the primary healthcare team, train the health professionals and volunteers in the primary healthcare team, and educate the community for better health. The greatest overlap that emerged between the surveys and FGDs was a need to strengthen social responsibility/accountability.

People’s opinion of what public health competencies doctors should have.
The other ideas regarding doctors’ activities that each appeared in only one community were that doctors should improve ethics, listen to patients’ complaints, provide good communication, advocate government policy, advise people about the rational use of drugs, have a good doctor–patient relationship, provide care for mental illness, chronic illness, and family problems at least once a month, conduct home visits, train the community volunteers, be the one who treats the patient in the daytime and nighttime, evaluate volunteer performance, and participate in community activities (Figure 7).
Results of In-Depth Interviews
The findings in the in-depth interviews indicate that the new generation of medical doctors should have competencies for administrative skills and knowledge about legislation. They should have a good understanding of the healthcare delivery system, health promotion, interpersonal relationships, and communication in order to lead teams. Other suggested competencies were media competency and health economics, in addition to basic science and clinical competencies.
As can be seen from the results, the needs of the community are not related to the competencies of doctors. The community residents trust that the doctors are well trained; instead, they are more concerned about the distribution of doctors, with no doctors working in the village. The representatives agreed that the WHO recommendations for competencies are suitable for the country. However, one opinion was that there are many elements that should be combined and reduced.
Discussion
In this study, the national survey could identify how core public health competencies for future medical doctors are delivered at the medical schools in Thailand. The study is a strategy-seeking part of the project to improve the teaching of public health in medical schools through a transformative education strategy. Furthermore, the study explored how regionally defined public health competencies recommended by WHO-SEARO are prioritized and being addressed to teach public health in undergraduate medical schools in Thailand.
The study identified that multidisciplinary integration is required to overcome gaps in existing human resources and experts in specialized areas such as health economics. Lyon et al. also reported a similar study in the United Kingdom in 2016 (Lyon et al., 2016). The current study had a better response rate (80.95%, 17 schools) compared to the previous study in the United Kingdom (75%, 13 schools) due to higher stakeholder participation. We also sought advice from another previous study in the United Kingdom. Both of these studies identified similar challenges faced when improving public health teaching in undergraduate medical schools. There is a human resource gap with an apparent need for more teachers to be experts or trained. Therefore, scaling up the training of master trainers initiated by WHO-SEARO is required in each country to improve public health teaching.
Teaching public health as a subject has also become diverse with the growing need for inter-disciplinary competencies for future doctors. (Chiolero, 2023; Sullivan et al., 2018) Integration among the departments is crucial to enhance inter-disciplinary competencies such as health system science, disaster management, social responsibility and accountability, research, and evidence-based medicine (Table 3). When we measured the level of integration, we counted positive outcomes as those schools which can deliver the public health competencies in an integrated approach and if the integration has been in place. Such integrated teaching was hard for more than a third of medical schools in Thailand (Figure 2). Applying the findings of this current study, a national framework of public health competencies can be developed. Furthermore, national stakeholders may identify the potential human resources and integration pathways in the country or professional networks in the ASEAN region or WHO-SEARO region to overcome the gap.
In addition to the survey findings, the study revealed public opinions and employers’ views. From the focus group interviews carried out in the 11 community health centers associated with the medical schools in different parts of the country, it was shown that people in the communities seemed to have good knowledge of the referral system used in Thailand (Figure 7). The people in all 11 of these communities were aware that if they become sick, they must go to see the doctors in the hospital and when they get better, they are referred back to the local health centers in the community close to their homes (Figure 7).
As for primary healthcare, the people know that they can receive primary care from a team of other health personnel. However, they still want care from doctors to assure them that they have received proper care. The expectations of people in the communities in relation to the doctors are listed in Table 6, from the most frequent to the least frequent statement (Table 6). Key findings in the in-depth interviews highlighted the “care in the community, home-based outreach and person-centered care for the older persons.” Such findings are going along with the current situation in Thailand which is facing increasing demand for health care and cost, and escalating family caregivers’ burden due to age-related multiple-morbidity, in the context of fast population ageing (M. N. Aung et al., 2022). The finding reminded medical educators of the importance of community-integrated care services and the need to prepare new generation doctors’ ability to cooperate, coordinate, and collaborate with the communities.
A recent study in Spain highlighted pedagogical, didactic, and curricular efforts to prepare new medical residents for working with the community. It stated that multiple agencies are to be involved to broaden the community health training by giving a balance of training to work at primary health care than to hospital rotations (Cardo-Miota et al., 2023).
Educating health professionals, especially medical students, is at the core of constructing a health system. Therefore, research examining the delivery of core public health competencies for undergraduate medical students is important in each country to bring about transformative changes to tackle emerging challenges facing the health system. Many countries, however, still do not have such evidence. This is the first such study in Thailand and Southeast Asia that examines how core public health competencies are delivered to undergraduate medical students in Thailand.
It may be of great benefit to define what level of competencies is required for an ordinary medical doctor in the future and to prepare a common text for use in undergraduate medical schools in Thailand. For example, it is likely that there is a lack of faculties for teaching health economics, or that it might be an elective subject in some medical schools (Figures 5 and 6). Shedding light on this area may lead to faculty development and gap-filling. Experts, such as health economists, usually work in big medical schools or schools of public health, but in limited numbers. Collaboration among the medical schools and the faculties of public health would be a solution as a national approach. Moreover, as WHO-SEARO organized the training of master trainers in 2015, medical teachers who teach public health can be provided with opportunities to update their excellence in required areas. Participatory action research is required. The current study findings can serve as the starting point of the PAR cycle among teachers, medical schools, and the medical council.
Regarding the doctor’s role and leadership in the community, most of the opinions pointed out that doctors rarely come to the community, typically only visiting the communities for health promotion and prevention campaigns. Therefore, field research projects for medical students in the communities may also serve to fill this gap, as well as represent an experiential learning opportunity. As we can see from the results, the needs of the community are not related to the competencies of the doctors, whom they trust to be well-trained. The community residents are more concerned about the distribution of doctors (Table 6). Lastly, in terms of the WHO recommendations for competencies, the representatives agreed that they are suitable for the country.
Communities are keen for doctors to work near their vicinity. This is understandable; however, it is determined not only by medical education but also by whether doctors are happy to work in the primary healthcare setting (Sullivan & Galea, 2021). Similar findings addressing work with the communities were reported recently in Japan as the modern framework of community medicine where the health system response to super aging society has been crafted as a community-based integrated care system through the visions of community, care systemization, and coworking with resident citizens (Kotani, 2023; Kumabe et al., 2023). As a result, the contemporary integrated community care system in Japan can provide, medical care in the local community, home health care in the community, and end-of-the-life medical treatment and care for multiple morbidity.
Within this area, the survey findings identified that social responsibility and accountability are competencies that need to be improved (Figure 7, Table 3). The experiential learning approach can be applied to promote students’ understanding of working with local communities in order to lead the health care service delivery team and empower community-integrated health promotion. In addition, role play in the class can serve for cognitive stimulation and self-learning, and stimulate their interest in interprofessional-collaboration (Bharti, 2023).
Limitation and Strength
The study had limitations. Although the response rate is reasonably strong, five medical schools did not participate in the study. One of those five was a big and long-established medical school. Although the quantitative sample and results may not change very much by their participation, further steps of the curricular change nationally may require the participation of all medical schools and institutional awareness of the result findings from each school. In the future study, and also in the future steps, researchers may try to persuade the participation of all medical schools through the regulatory bodies and professional networks. Another limitation is that the questionnaires did not include questions about the teaching of gerontology in medical school.
Recursive mixed-method design assured the strength of the study. Particular strengths of the study are (a) a good response rate in the national survey, (b) qualitative inquiries investigated in many communities across the country, and (c) in-depth interviews with employers. Such a holistic approach gave us thorough a understanding of teaching public health in medical schools and trustworthy evidence to support future improvement in medical education. The findings are expected to be useful nationally, regionally, and internationally for teaching and learning global health.
Recommendation and Implications
The findings of the study are directly useful nationally to call for the improvement in teaching public health to future medical doctors. The findings in Thailand are also useful as an excellent example for other countries in Asia and around the world.
Specifically, the current study findings are to be implied as the initial steps of future Participatory Action Research (PAR). The current study did not launch the action part of PAR as it needs a longer time. After acquiring the evidence from this study, a stakeholder meeting to design an action model and a cycle of change is recommended (Martí, 2016). The findings of the present study are expected to contribute to the evidence to design further actions and transformative changes through:
Engaging policymakers, educators, and health professionals to improve the teaching of public health in medical schools to initiate change.
Collaboration of medical schools to improve the teaching of public health in the undergraduate medical curriculum though a national framework of public health competencies.
Repeating the PAR cycle to bring about better models and transformative education, leading to improved public health teaching through interdisciplinary integrations.
The areas of integration and evidence-based pedagogical strategies can facilitate transformative education. While integrated curriculums are in place in every medical school in Thailand, it is alarming that 35% of medical schools still could not apply integration of faculties, experts, from different disciplines to teach public health. The finding is expected to trigger rapid advocacy, exchanging thoughts for improvement and innovative ideas to form further research leading to the creation of transdisciplinary learning for public health.
Furthermore, the instrument that was applied in this study can be used in many other countries to replicate similar studies for improving teaching public health or global public health in medical schools.
Conclusions
Thailand has celebrated its second decade of universal health coverage (UHC) (Tangcharoensathien et al., 2018). It has increasingly faced the challenges of population aging and the need to establish long-term care, pandemic containment, air pollution alleviation, and UHC for immigrants (M. N. Aung et al., 2021; T. N. N. Aung et al., 2022; Paoin et al., 2021). As it is facing new challenges in public health, the strategy for the development of human resources for health is critical for the future. In this study, we conducted a national survey of medical schools to investigate how public health competencies are delivered to medical students, in addition to listening to the people in the community and employers of medical doctors. There are several competencies that need to be focused on, particularly health economics, health policy and management, and disaster management. Integration within each faculty of medicine or beyond the faculty of medicine would be an operational strategy for health policy and management and disaster management. The number of teachers who teach public health is rather small. This might impact subjects requiring specialist knowledge such as health economics. Schools have counteracted this by carrying out web-based lectures. Further discussions among medical schools, as well as with public health schools, may provide a solution to overcome this issue.
Triangulation of the findings from the survey, FGDs, and in-depth interviews, representing the opinions of faculty members, community residents, and MD employers, showed that health policy and management, health systems, health economics, and social responsibility and accountability are the competencies that need to be improved. We believe that bringing this evidence to multiple stakeholders of medical education and public health teaching may lead to the creation of a national framework for public health competencies and further actions.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241251987 – Supplemental material for A National Assessment of Public Health Instructions in Medical Schools of Thailand
Supplemental material, sj-docx-1-sgo-10.1177_21582440241251987 for A National Assessment of Public Health Instructions in Medical Schools of Thailand by Myo Nyein Aung, Vanich Vanapruks, Pornchai Sithisarankul, Pajaree Yenbutra, Suthee Rattanamongkolgul, Krishna Suvarnabhumi and Pongsak Wannakrairot in SAGE Open
Footnotes
Acknowledgements
The article is dedicated to Professor Vanich Vanapruks who committed to the study until her last days. Thin Nyein Nyein Aung, Department of Family Medicine, Faculty of Medicine, Chiang Mai University, is acknowledged for support with data analysis and data management. Anna Lyon, Faculty of Public Health, Fellow of the Higher Education Academy, Institute of Clinical Sciences, College of Medical and Dental Sciences, University of Birmingham, is acknowledged for the advice in designing the research instrument. Staff and faculties who supported the data collection and implementation are heartily acknowledged. Richard Lawrence Mann is acknowledged for refining the English language in this article. Thet Htoo Pan, Department of Global Health Research, Juntendo University, is acknowledged for her assistance in preparing documents and reading proofs.
Author’s Note
This research was conducted while Myo Nyein Aung was a faculty at WHO Collaborating Center for Medical Education, Faculty of Medicine, Chulalongkorn University. He is now an associate professor at Department of Global Health Research, Graduate School of Medicine, Juntendo University and Advanced Research Institute for Health Sciences and Faculty of International Liberal Arts, Juntendo University, Hongo 2-1-1, Bunkyo Ku, Tokyo 113-8421, Japan; and can be contacted at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the MRF 2560—004 (MedResNet Medical Research Foundation), Medical Research Network of the Consortium of Thai Medical Schools, through the grant “National study of public health core competencies in undergraduate medical schools, Thailand.”
Ethical Approval
The Institutional Review Board of the Faculty of Medicine, Chulalongkorn University approved the ethics of this study (219,60, dated 20 June 2017).
Institutional Review Statement
This study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Written informed consent was obtained from all the subjects involved in the study.
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
Data are available and can be delivered on request to corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.