
Abstract
In response to the COVID-19 pandemic, this paper provides valuable information to establish new comparative policies between ASEAN countries. The study used disproportionate policy-making that stimulated the understanding of different adaptive strategies. The paper identified the extent of government response policy as a range of proportionate public involvement. The measure of disproportionality was obtained by calculating the regional differentiation in a particular country’s average response to a crisis. This study found that six ASEAN countries are disproportional in their Policy Response to the COVID-19 Pandemic. Thailand is ranked the highest and classified as the most prepared country in terms of Global Health Security, and four countries are classified as normo-action. Indeed, Thailand is one of the countries with the most-prepared health security. Nonetheless, countries deemed less prepared and underreacting include Laos, Cambodia, Malaysia, Singapore, Indonesia, Myanmar, and the Philippines, which have all witnessed continuous rapid growth in COVID-19 infections.
Introduction
The World Health Organization (WHO) revealed on 11 March 2020 that COVID-19 has become a global pandemic. Since then, governments worldwide have faced tough decisions on health security policies, especially in ASEAN countries. The people’s response to the prevention of COVID-19 transmission is vital to be governing and managed (Teter, 2020). Most countries have attempted to enhance their national planning capacities due to lack of funding, conflicting national priorities, and high health workers turnover (Iqbal et al., 2020). Before the recent pandemic, governments responded proportionately to political challenges in their working environments (Wang & Di, 2020). But in the advent of COVID-19, governance has significantly changed (Saud et al., 2021). Since there are different views on whether the government appropriately responds to existing issues in COVID-19, a systematic response is required (Pramanik et al., 2020; Yao et al., 2020). For example, quarantine alone is not enough to prevent COVID-19 (Saud et al., 2020). Hence, the significant impact brought about by the virus is a grave and continuous concern for governments, policy-makers, and front-liners (Tan et al., 2020). What are the challenges faced by governments worldwide, specifically ASEAN state members in the advent of COVID-19? Details concerning COVID-19 cases in all 10 ASEAN countries are as follows: Laos saw 25 new cases in May 2021, bringing the total to 1,327 with one death; Cambodia recorded 506 new cases putting the total at 19,743 cases and 126 deaths; Vietnam confirmed a total of 3,489 cases; Brunei had a total of 330 cases and three deaths. Myanmar had a total of 142,963 cases and 3,210 deaths; Thailand had a total of 85,005 cases and 421 deaths; Malaysia reported a total of 444,484 cases and 1,700 deaths; Singapore had a total of 61,378 cases and 31 deaths; the Philippines recorded a total of 1,108,826 cases and 18,562 deaths; and Indonesia had a total of 1,718,575 cases and 47,218 deaths (ASEANBriefing, 2020).
The COVID-19 pandemic not only greatly affects the health system, but socio-economic status throughout ASEAN countries as well (Dewi et al., 2020; Shahi et al., 2021). In particular, the pandemic’s impact led to immediate interruptions caused by lockdown measures, community-based quarantines, temporary closures of businesses and schools, social protection for vulnerable populations, needed SMEs, and other affected businesses (Gill, 2020). Unlike other situations where regulators commonly encourage firms to develop a policy action plan, public health organizations follow the decisions of scientists and experts of pandemic preparedness (Tan et al., 2020). The study of disproportionate policy-making is enhanced by understanding the challenges between elected official instructional strategies, collected information, and action (Ong, 2020). Several studies in public health focus on categorizing the disease risks and assessing costs to determine if the problem is proportionate to any rational response policy (Zhang & Savage, 2020). However, the literature shows that economic conditions and government demand may lead policy-makers to choose inappropriate or excessive policies based on policy factors (Banerjee et al., 2020). As of today, there have been limited reports on the broad-based pandemic response from ASEAN countries. This, accordingly, increases the need for renewed research that focuses on new policy-making in pandemic response (Teter, 2020). In addition, this article may provide valuable information on developing new comparative policies among ASEAN countries, particularly in response to a global pandemic such as COVID-19.
This article contributes to the existing literature by providing an applicable and valuable research on comparative policy analysis by developing theoretical and methodological reviews. The principle of the disproportionate policy provides a valuable method for determining the degree of transmission variance. The level of government policy response is measured as a assess of how far public involvement in policy is proportionally. Therefore, the country’s average response to the extent to which all disproportionalities exist is determined by considering a domestic variance like a crisis. The current article is structured as follows. The literature review discusses the proportionality of political responses. The methodological measures for developing a disproportionate policy response index are defined in the context of pandemic crises. The “Indicator Function” section discusses the findings on the implementation of the proposed indicators. The conclusion considers potential research possibilities for comparative public policy academics.
The fundamental question of this research is to identify the extent of government response policy as a range of proportionate public involvement. Including to measure of disproportionality and regional differentiation in a particular six ASEAN countries based on their Policy Response to the COVID-19 Pandemic
Theoretical Framework
Proportionate Adaptation and Policy Experimentation
In dealing with the COVID-19 pandemic, public officials are still devising current and potential policy strategies that often have less and inaccurate details (Ceylan, 2020; Lee et al., 2020). All governments in ASEAN began collaborating with public policies or disproportionate political responses when the COVID-19 pandemic emerged (Lal et al., 2020; Teter, 2020). Preliminary research in policy studies such as disproportionate policy reactions is referred to as a form of policy overreaction and a policy instruments database that includes different techniques for coordinating people’s behavior (Iqbal et al., 2020). The policy mechanism is usually designed as sequential components or stages, these are agenda setting, formulation, implementation, and evaluation (Benson & Jordan, 2015; Shiffman, 2008). For instance, through careful consideration of multiple possibilities (Mohsin et al., 2021). Slowly, as policy makers for a variety of reasons make only nominal changes at a time (Shiffman, 2008). Usually unexpectedly, at random junctures, the problem, its solutions, and political developments all meet to be positioned there (Mahmud et al., 2021); and when policymakers believe the problem is suitable for government intervention, it would be easier to implement and widely accepted by the public (Dewi et al., 2020).
The cost and benefit of policy interventions would be greatly influenced by policy actors (Mei, 2020). Expenses and costs are, of course, the market portfolio of economic analysts. Since political analyses started in the 1960s, political scientists have been providing a deep understanding of such policy initiatives’ costs and benefits (OECD, 2015; Ong, 2020). Every policy decision involves uncertainty and 154 risks. Knowledge about the outcomes frequently remains unclear until actual results of policy decisions are formed (Cegarra-Navarro et al., 2014; Zhang & Savage, 2020). Therefore, it is crucial to understand and process health-related information available online. While online sources have accurate and timely health information, misinformation and rumors appear to be equally accessible (Yao et al., 2020). COVID-19 rapidly spreads with an increasing number of positive cases worldwide, which raises concerns about how governments should respond (Teter, 2020). At a conceptual level, under-reactive policy is described as “a systematic stagnant or inadequate response by government officials to high risks or no response at all.” If political deprivation continues for an extended period, there will be a negative policy gap.
Similarly, policy overreactions impose objective and social costs without producing objective compensation and perceived benefits (Teter, 2020). The idea of overinvestment “calls on government spending in a particular policy instrument to reach its value in achieving the objective of policy” (Cegarra-Navarro et al., 2014; Zhang & Savage, 2020). Disproportionate signal responses imply considerable difficulty in information policy output (Teter, 2020). The inevitable balance between many issues recognizes and interprets the problem of decision-making—process weighing the qualities of the issue’s characteristic and competing solutions—are three components of disproportionate responses (Jirangkul, 2018). Hence the gap of the policy response is to make disproportionate policy responses operational (Jovita et al., 2018; Prawoto et al., 2020). While current studies suggest measuring policy (dis) proportionality in a complex and measured way, a more comprehensive, slimmer, intersubjective, and large-scale comparative study measuring approach must be adopted. Indeed, recent studies are focused on individual or small measurements, and the primary source of empirical evidence often uses secondary literary sources. The second gap is the institutional determining factors of the quality of policy-makers’ risk assessment.
COVID-19 Crisis and Government Response
A pandemic is referred to as “an outbreak that crosses international borders and usually affects many globally.” A pandemic may cause sudden, broad range morbidity and mortality and disruption to society, politics, and economy (Tosepu et al., 2020). Many of these countries are in high-risk areas, particularly in Central and West Africa, and may remain vulnerable and require significant international assistance during a pandemic. The continued presence of slums, unresponsive health systems, high prevalence of comorbidities, inadequate sanitation, and aging populations are other environmental and demographic patterns that may increase pandemic severity (Gill, 2020).
Furthermore, for a categorizing the preparation stage and responding to pandemics known as the pre-pandemic phase, the spark period, and the spreading time. Poorly prepared countries may be affected by political uncertainty, lack of public policy, inadequate public health, and deficiencies in essential outbreak detection and response systems (Wang & Di, 2020). On the other hand, well-prepared countries have efficient management systems (van Popering-Verkerk & van Buuren, 2017), stable economies, and reasonable and adequate healthcare costs (Purnomo et al., 2021). Other initiatives to respond to the COVID-19 crisis include school closures, travel bans, public prohibition and education emergency spending, alternative methods of providing social services, and other variable steps to avoid the spread of the virus and the extent of adoption.
Policy-makers and the public reacted quickly and adopted strategies, such as interventions that were more or less achievable in real-time (Shahzad et al., 2020). Countries like Italy, the United States, Spain, and France struggled to contain the infection, perhaps due to a lack of social distancing, despite their advanced health systems in place (Shahzad et al., 2020). In several countries, the number of cases and deaths in late and reactionary crises tended to be significantly rising (Heyang & Martin, 2021). In the beginning, Trump’s administration denied the enormity and severity of the COVID-19 pandemic. It portrayed the crisis as a political point promoted by the Democrats as “a hoax and a cook-up.” President Trump and his officials have been portraying the crisis as being “handled” for over 2 months, saying that the COVID-19 situation is “going to be just fine” “not a matter,” “it [COVID-19] will go away,” “it is flulike,” “Chinese virus,” (Pei et al., 2020). In Italy’s initial phase, the COVID-19 crisis was not a problem. In the original state-of-the-urgent studies, both the media and several political parties were skeptical—while many scientists were alert for weeks about a potential catastrophe. Indeed, several influential Italian legislators engaged in Milan’s public action in late February to suggest that the economy would not suffer from worry or avoid the virus (Pei et al., 2020). Based on rational choice, governments seem primarily to optimize their office time, which is the so-called political survival (Heyang & Martin, 2021).
The paper highlights the ability to respond to a pandemic indicates that policy and decision can be shaped and taken by governments. Hence, the major concern of this research is whether specific policy responses are proportionate to the policy issue’s existence and in a particular six ASEAN countries based on their policy response to the COVID-19 Pandemic.
Materials and Methods
Research Method
This research is a quantitative analytic study. The initial stage began by determining the pandemic score variable suitable to be associated with the global health security variable. The following steps were taken to analyze the appropriateness of the government’s policy response in dealing with the COVID-19 pandemic by comparing the health security capacities of each country with the pandemic score. To examine each country’s policy responses, the following steps were taken (Figure 1). First, researchers mapped ASEAN countries COVID-19 reports based on “ourworldindata” from 29 April 2020 (Teter, 2020). Second, ASEAN countries are classified into three clusters according to doubling time rank (Matei et al., 2020). A high doubling time value shows that country’s infection growth rate is slow, known as a “low pandemic.” We categorize the ASEAN countries’ pandemic level into three indicators: low, normal, and high (Agustiyara et al., 2020). The Global Health Security (GHS) Index, John Hopkins University Detection and Rapid response Indicators were used to compare and evaluate the data (Shahzad et al., 2020). The goal of the GHS is to help understand and measure developments in global-scale capability to detect and respond to infectious disease threats. The results were then divided into three groups, “least prepared” if score <33.3, “more prepared” when score >33.3to 66.6, and most prepared if score 66.6 to 100.
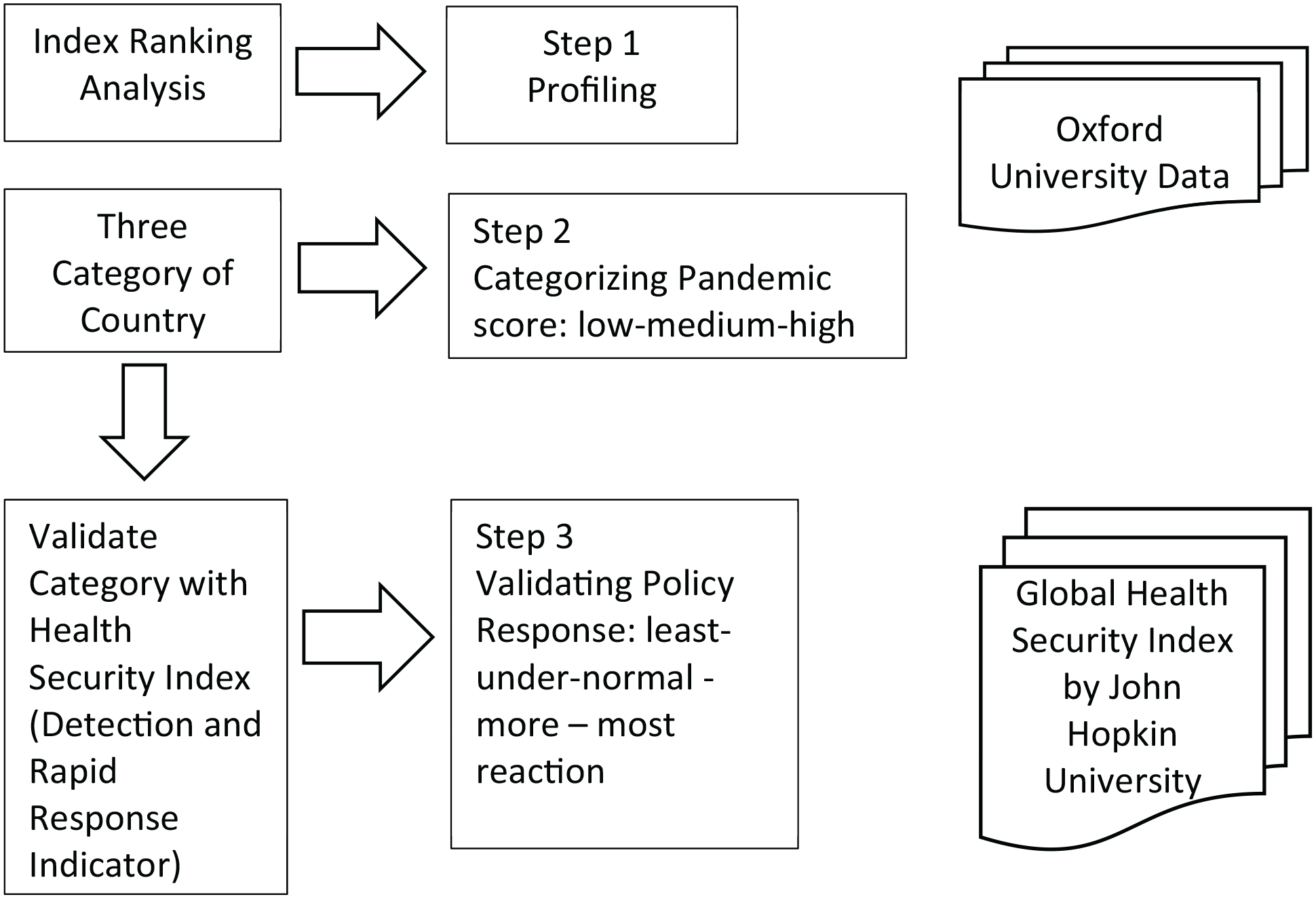
Steps taken to investigate the policy responses of ASEAN countries.
The first category is the detection score. The category was chosen because of the early detection and reporting of disease outbreaks that may spread worldwide and become a pandemic. The detection category includes laboratory systems assessment metrics, real-time monitoring and reporting, personnel on epidemiology, and human and animal environmental data. A cumulative score of 0 to 100 was given consisting of 22 questions based on GHS Index, such as prevention, detection and reporting, rapid response, health system, compliance with international norms, and risk environment. The questions in the GHS Index are designed to determine not only whether a capacity exists, but also whether that capacity is regularly—for example, annually—tested and relies entirely on open-source information.
The second category is rapid response. Rapid response refers to the evaluation of emergency preparedness and response plans, action plans, response operations, linkages between public health and security authorities, risk communication, access to communication facilities, and trade and travel restrictions. There were 22 questions provided with a total score of 0 to 100. We argue that countries categorized as the “most-prepared” have a better response to the pandemic compared to countries classified as “more-” or “least prepared”.
Furthermore, if countries categorized as the “most prepared” have a high pandemic score, their policy response will be deemed to be within the “lowest-reaction” group. On the other hand, when countries categorized as least prepared have a low pandemic score, their policy response will be considered to be within the “more” or “most” reaction group.
The collected data were subsequently analyzed through Global health security (GHS) data at “ourworldindata.gov” database. To assess the relationship between global health security category and doubling time score, one-way ANOVA test was used using Jamovi 1.1.9 software. The mapping data are then presented in (Microsoft Bing) figures and narratives.
Designing Indicators of COVID-19 Pandemic Policy Response
We use COVID-19 pandemic data to illustrate the growth rate of the disease transmission. The data selected for this study promote the policy response to take the necessary steps to reduce transmission rate (Dewi et al., 2020). The increasing COVID-19 cases show a significant spread of COVID-19 worldwide (Lee et al., 2020). However, this figure was relatively proportional to the number of tests performed in the country. Tests are conducted as a way to track the development of the pandemic and to avoid, diagnose, and respond quickly to the disease.
Nonetheless, assuming that a country has done a few studies to diagnose COVID-19 based on the population. The number of positive cases and deaths caused by COVID-19, in this case, would be artificially small. Hence, we used “doubling time” for growth rates to reduce bias. The “doubling time” used in this study measures infectious diseases and shows the extent of control efforts needed to reduce disease transmission. Across several previous studies on infectious diseases, double measurement times were used for SARS and Ebola (Shahzad et al., 2020). Doubling time may detect the impact of the condition on pandemic growth, which indicates that changes in doubling time assess policy effectiveness (Kulkarni & Anantharama, 2020).
Doubling time in COVID-19 refers to the time taken to double the size or volume of a specified amount at a constant growth rate using a formula. The primary source of this data was “ourworldindata.gov” database.
The Formula for Policy Response
Laos had fewer than 50 cases or out of 10 in ASEAN members. While Papua New Guinea and Timor Leste are prospective ASEAN members where the cases are still relatively low: Papua 8 cases, Timor Leste 24 cases. Doubling time calculation results with the above formula are preceded by ASEAN median values (Table 1).
The GHS Indicator and Pandemic Score.

Note. The GHS indicator index is based on 3 categories which are classified as “most prepared”, “more prepared”, and “least prepared”, including reflecting across preparedness for ASEAN countries assessed based on pandemic category (low-high).
Results and Analysis
The study of disproportionate policymaking is motivated by an awareness of disparities between adaptive strategies developed by individuals and the information they obtain (Shahzad et al., 2020), contributing to people’s excessive reaction to the knowledge presented (Mohsin et al., 2021). In the case of disproportionality and regional differentiation in a particular six ASEAN countries, a specific policy solution is proportionate to the strategic factors that may lead policymakers to extent of government response policy as a range of proportionate public involvement (Cegarra-Navarro et al., 2014; Zhang & Savage, 2020).
Since 30 May 2020, COVID-19 had infected 188 countries worldwide with 6,022,022 positive cases (Lee et al., 2020). Countries in South East Asia, which are the 10 member countries of ASEAN, including Timor-Leste and Papua New Guinea (non-ASEAN members), have 87,378 confirmed cases. This study only selected ASEAN countries with Global Health Security data and doubling time, especially in the analyses of prevention, detection, and rapid response. Based on the GHS Index as relies entirely on open-source information: data that analyzed on six ASEAN countries are able to access the information about the country’s existing capacities and plans and pandemic preparedness so they can take concrete steps to indicators and questions following the GHS Index framework.
Table 2 shows that Thailand reported the first case of Covid-19 in Southeast Asia, and Laos reported the last case. Indonesia had the highest number of cases, and Laos had the lowest on 29 July 2020. This is sequentially followed by the Philippines, Singapore, Malaysia, Thailand, Vietnam, Myanmar, Cambodia, and Brunei. The countries included in the high category pandemic were Malaysia, Myanmar, Singapore, the Philippines, and Indonesia.
Country Data Based on Covid-19 Cases.
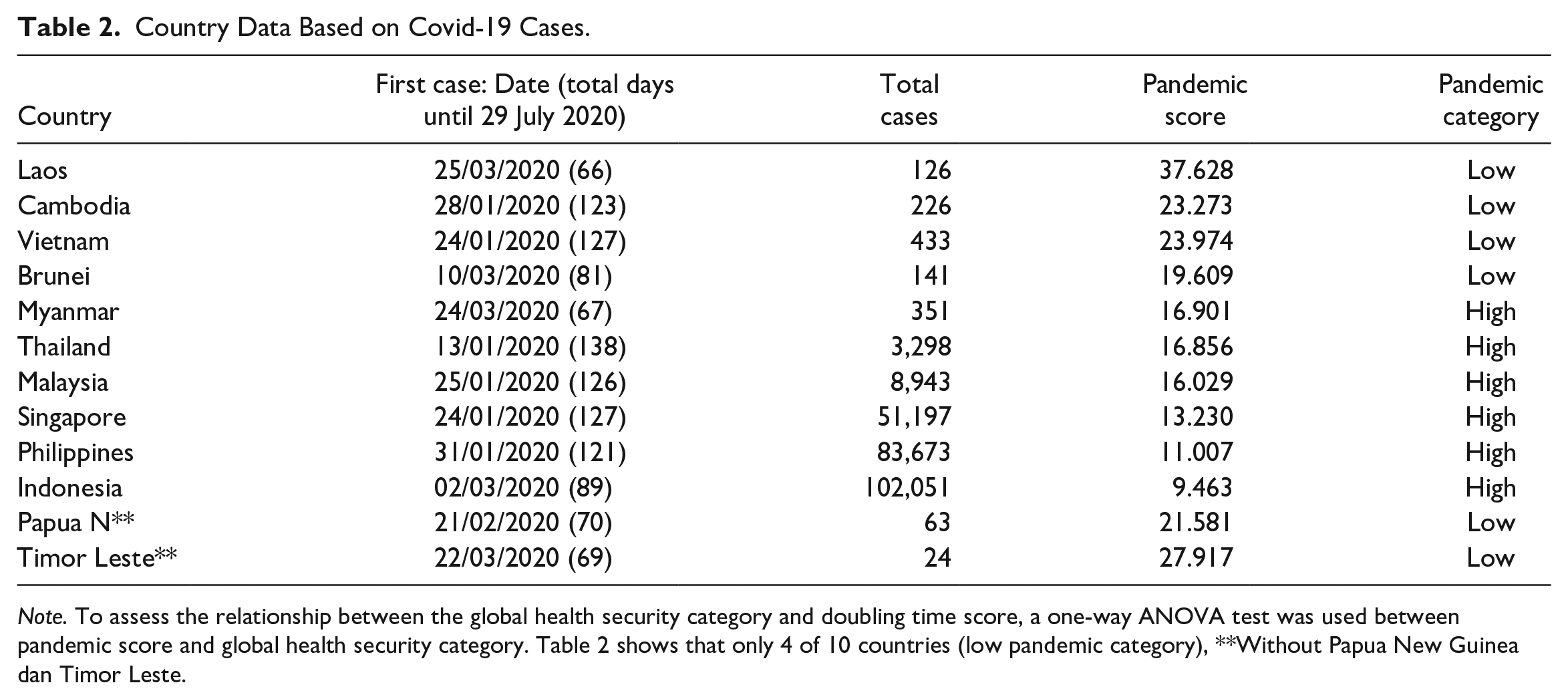
Note. To assess the relationship between the global health security category and doubling time score, a one-way ANOVA test was used between pandemic score and global health security category. Table 2 shows that only 4 of 10 countries (low pandemic category), **Without Papua New Guinea dan Timor Leste.
The World Health Organization’s (WHO) announcement on the COVID-19 pandemic in 11 March 2020 was followed by the strengthening of national responses and regional cooperation, ASEAN as a Regional Actor. COVID-19 affected countries with weaker health systems.
In ASEAN countries, the average cumulative predictor of health protection is 47.73 out of 100 potential estimates. As each ASEAN member state confirmed its first case, the outbreak was initially contained by applying national prevention and control strategies. They included preparational, preventive, monitored, and detected health measures, including public health advice on daily hand washing, proper usage of facemask, and other personal hygiene and sanitation measures. These include public health measures for disease prevention, monitoring, detection, and response.
Table 3 shows that six countries of ASEAN had disproportional policy responses categorized as under-reaction and least-reaction. The country with the least reaction category was Thailand, while the countries with the under-reaction category were Indonesia, Malaysia, Myanmar, the Philippines, and Singapore. The countries categorized as Normo-Action with more prepared GHS index and low pandemic score were Vietnam, Laos, and Cambodia. Countries categorized as Normo-action with least prepared GHS index and low Pandemic category was Brunei. See Figure 2 for the map of policy response, GHS index, pandemic score, and pandemic rank by countries.
Policy Response: GHS Category Versus Pandemic Score.

Note. There is only 1 country out of 10 with most prepared as least-reaction, 8 countries categorized more prepared as 3 countries Normo-Reaction and 5 Countries under-reaction, while 1 country categorized as least reaction and Normo-reaction. Without Papua New Guinea dan Timor Leste.
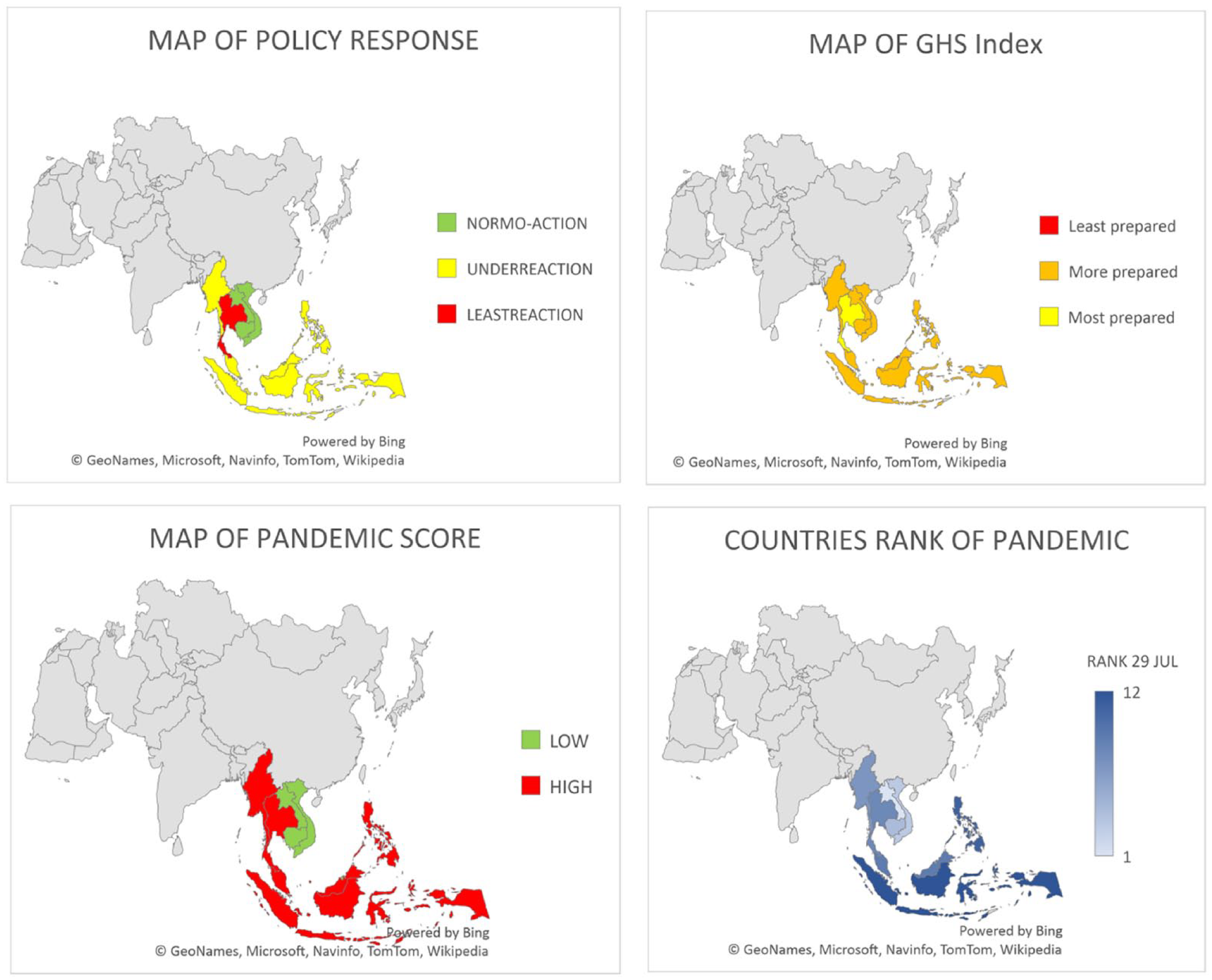
Policy response, GHS index, Pandemic Score and Pandemic rank, of ASEAN countries in 2020.
Due to the emergence of the coronavirus, countless data and data gaps have been found. The most critical issues refer to how we can be efficaciously and adequately prevent, detect, and react to the spread of the disease, and how public and clinical health care cases should be managed. To facilitate national interventions and resolve the shortfalls, and to encourage knowledge and information sharing on a timely basis, regional health systems have been rapidly enabled. Individual countries and the world are now being threatened by the pandemic, the environment, and people’s livelihoods. For each country affected by COVID-19, this included a government-wide and multi-sectoral approach. The pandemic has enhanced regional cooperation and collaboration between its member states and partners in ASEAN. The emergency was illustrated by the early and sustained regional response of the ASEAN Health Sector and Dialog partners, assisted both by the ASEAN Secretariat and non-health sector efforts, to solve COVID-19 and its crisis.
Discussion
Our findings indicate that ASEAN countries need help in improving their capacity and increasing financial support. Implementing interventions to improve the most vulnerable countries’ health security is a global priority (Banerjee et al., 2020). Governments may overreact to ambiguous signals. First, a problem takes a precious position on the agenda-setting, which negatively impacts prioritizing issues. Second, signals typically do not perceive themselves. All interest groups, governments, think tanks, elected officials, and mobilized community should resolve this issue. As a result of its electoral alliance, one party may be more receptive or partial to some problems than another. It should also be noted that the governing party is more prone to or somewhat capable of mobilization (Tosepu et al., 2020).
The findings reveal that Thailand was the most prepared and classified in mitigating pandemic, based on the global health security indicators. On the other hand, Malaysia, Singapore, Indonesia, Myanmar, Philippines were classified as under-reactive countries. Moreover, based on Global health security (GHS) data, the two least reactive countries scored 0 in one of the rapid response subcategories, that is, proper handling. This subcategory evaluated a country’s implementation of International Health Regulations (IHR). When a country scores a zero in this subcategory, it means that in the last year (except chemical and radiological workouts), the country had not completed a biologically threatened IHR experiment with the WHO. Thus, there is no clear evidence in the last years. The country tackled the disease using a post-urgency reaction or a biological threat-focused IHR exercise with the WHO to establish a list of vulnerabilities or best practices.
Therefore, countries did not have adequate opportunity to establish a response strategy to mitigate and manage outbreaks of COVID-19 (Wang & Di, 2020). When other countries struggled to deal with positive cases of COVID-19, the government took a different approach in the early stages of the pandemic. This is meant to avoid the spread of COVID-19 from overwhelming the healthcare system (Tosepu et al., 2020). However, the other effects of lockdowns that governments should consider include deteriorating human mental safety and well-being.
WHO-based awareness efforts were intensified to resolve China and neighboring countries’ COVID-19 outbreaks and the disease was eventually declared a global public health emergency. Six ASEAN member states announced their first cases before the resolution was released. By the end of March, the pandemic affected all 10 ASEAN member states. Including the initial response to COVID-19, such as a timeline of local interventions. This timeline provides an overview of the events in China, Japan, the Republic of Korea, and the ASEAN member states due to initial disease outbreaks. The ASEAN Health Sector has identified the scientific complexity of the current coronavirus and how to adequately deal with the virus based on ASEAN member countries’ initial responses.
Unlike the Laos case, why did Laos have a low number of confirmed cases? Laos borders directly with China; geographically, it also does not have a marine area, it is a landlocked state. The possibility of transmission can only be through air and land transport, this had raised fears of transmission which was considered considerably high as it is located in close proximity to China’s transmission center. As a consequence, since the first outbreak of COVID-19 in December 2019, the Laos government, at the national level, had taken preventative protection measures in line with WHO guidelines for early detection and prevention of COVID-19 outbreaks. The establishment of the National Prevention, Control, and Response Committee for COVID-19 also considered the allocation of emergency funds for COVID-19response, lockdown, and work from home (WFH) implementation.
Those recommendations aim to facilitate understanding by the government initiatives for healthcare professionals and the general public (Teter, 2020). In addition, ASEAN countries again with a too high risk of import and people mobility (Shahzad et al., 2020). WHO supports intensive airport screening and ensures fast identification of the newest coronavirus. Sample selection centers are critical, and the WHO tended to help countries develop their testing procedures (WHO, 2020). However, based on data and communication pertaining to ASEAN Health Sector efforts in Covid-19Prevention, Identification, and Response, the COVID-19 numbers in Indonesia were the strongest at the time among ASEAN countries. The country reported 41,431 cases, as the first case was confirmed in March. The amount surpassed 41,216 cases in Singapore (WHO, 2020) . This occurred because Indonesians adapted to the new normal, being productive might result in ignoring protocols put in place to stop the virus transmission chain (WHO, 2020). Health services often lacked staff qualified to perform examinations, rehabilitation, and they also lacked infrastructure specified in the WHO guidelines, such as airport and hospital quarantine areas or the use of structures and systems that monitor contacts with reported cases. Education, speeding up test results, quicker handling of verified instances and contacts, and maintaining robust infection management measures are essential to maximizing human resources (Teter, 2020).
As COVID-19 quickly spread throughout Asian countries, European countries were alarmed. They began to establish containment measures, inefficient prevention strategies and underestimated the cases (Banerjee et al., 2020). Some countries remained physically distant and imposed lockdowns to avoid COVID-19 transmission in the community (Tan et al., 2020). In their efforts to avoid, recognize, and respond to emergencies, each country has differing ability. Countries have developed emergency management capacity, which shows that effective responses to possible health emergencies, including the COVID-19 pandemic, are possible. Successful outbreak response does not only rely on human resource availability and proper financing and management of emergency logistics (handling of essential supplies required in emergencies).
The WHO and ASEAN EOC Networks can function as a highly integrated regional platform for a global response to crisis and risk reduction (Grundy-Warr & Lin, 2020). Rapid response measures for emergencies remain below standard. Activating emergency management centers at home and abroad and continuing to investigate positive cases of COVID-19 could improve emergency response operations (Ceylan, 2020).
Conclusion
Based on a preliminary analysis of experiences in different countries, the COVID-19 pandemic score rated based on doubling time was directly significant with the health security category. Including preliminary studies conducted by various international institutions (WHO and ASEAN) and several think tanks, some key points can be worked out to develop the framework for pandemic governance of COVID-19. This research concluded that the pandemic policy reaction to COVID-19 in ASEAN countries in its data collection of six countries is disproportionate. Thailand is classified as the most prepared country in the Global Health Security category, which appears to have scored high in the Pandemic score, while four countries are classified as normo-action. Thailand is considered the most-prepared country in the health security category. Countries deemed more prepared with under reaction include Laos, Cambodia, Malaysia, Singapore, Indonesia, Myanmar, and The Philippines, which are all countries that had rapid COVID-19 transmission.
Footnotes
Acknowledgements
The authors would like to thank the reviewers and journal editor for their very constructive comments and suggestions. We also thank Prof Nurmandi from Universitas Muhammadiyah Yogyakarta, Prof Klaus Hubacek from the University of Groningen, the Netherland and Prof P. B. Anand from the University of Bradford who provided insight and expertise that greatly assisted the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.