
Abstract
Malaria is a major health problem in many tropical and subtropical countries and in the south of Iran. In this study, due to the importance of the disease in Sistan and Baluchestan province, the influence of temperature, humidity, and rainfall on malaria has been evaluated in areas with a high incidence of malaria. Malaria incidence data were inquired from the Province Health Authority, and climatic variables were inquired from the Bureau of Meteorology from 2000 to 2012 and were analyzed on a monthly basis. Changes in incidence of malaria with climatic factors were analyzed by negative binomial regression by Stata 11, and the correlations were calculated with Minitab15 for determining the potential impact of meteorological variables with and without lags on malaria transmission. The incidence of malaria had a significant positive correlation with the average, minimum, and maximum monthly temperatures and a negative correlation with rainfall and low humidity (<60%). However, humidity >60% had a positive impact on incidence; as in the town of Chabahar after adjusting variables such as rainfall and temperature; every one percent increase in humidity caused a 4% increase in malaria incidence in the same month and a significant 6% increase in the next month. Temperature and humidity over 60% are effective climate parameters in the incidence of malaria. These factors should be considered in planning for controlling and preventing malaria.
Background
Malaria is one of the most important parasitic diseases and one of the most important health problems in a number of countries, particularly countries in tropical and subtropical regions of the world (Azizi, Janghorbani, & Hatami, 2011). Malaria is an acute or chronic infectious disease caused by intracellular protozoan parasites from the Plasmodium genus. The disease is endemic in many countries of the world. Its epidemiologic and entomologic characteristics, the existence of more than 400 species of mosquito vectors, its tendency to drug resistance and the diversity in human sensitivity to this disease, and social, cultural, political, economical, and ecological factors in infected countries make the control of this disease very difficult. Its economic burden has imposed many negative effects on public health (Hatami, 2009).
Between 2001 and 2009, the global burden of malaria has increased to more than 34 million (Edlund et al., 2012). According to the latest estimates from the World Health Organization in 2015, there were 214 million new cases (in a range of 149-303 million) of this disease globally and about 438,000 deaths (in a range of 236,000-635,000) have happened, and almost 306,000 deaths occurred in children below the age of 5 years (World Health Organization [WHO], 2015).
Iran is considered as an endemic country for malaria. Malaria cases in Iran 2002 to 2007 were, respectively, 0.24, 0.38, 0.20, 0.28, 0.23, and 0.24 per 100,000 people. Most cases are now concentrated in three southeast provinces of the country, and 68% of all cases in 2002 occurred in the Sistan–Baluchestan, Hormozgan, and the southern part of Kerman province. In 2007, about 95% of cases were reported from these three provinces. Most of the cases have happened in the Sistan–Baluchestan province, so that in 2002 about 41% and in 2007 about 60% of all cases happened in this province (Mozafari, MostoufioAlmamaleki, & Hashemi, 2012; Raeisi, Nikpoor, Ranjbar, & Faraji, 2009).
The environmental, socioeconomical, and climatological situation of the region and its proximity to the Afghanistan and Pakistan border are important factors related to the high incidence of malaria (Sheikhzadeh, 2010).
The distribution and dynamics of malaria cases is often influenced by biotic and abiotic factors. The effects of abiotic factors such as temperature and rainfall on malaria transmission cycles seem to be important. Rainfall has an important impact on mosquito life and is probably important in the transmission of the disease. While temperature acts as a regulatory force and is probably even more important (Martens, Niessen, Rotmans, Jetten, & McMichael, 1995), relative humidity affects the longevity and activity of the mosquito in such a way that if relative humidity is less than 60% at 8 a.m., disease transmission is likely to get interrupted (Azizi et al., 2011).
Studies have shown that climatic factors have an important role on the prevalence and transmission of malaria, but the effect of different climate variables was not the same in different regions. In Shuchon, China, monthly minimum temperature and precipitation were related to the incidence of malaria in the next month; but in Anhui, precipitation had the strongest relation with incidence (Bi, Tong, Donald, Parton, & Ni, 2003; Zhao et al., 2013). In Burundi, East-Central Africa, precipitation and maximum temperature had an inverse relation with incidence in the same month. The Plasmodium parasite and the Anopheles mosquito need specific climate conditions for proliferation, and these conditions indirectly affect the incidence and prevalence of malaria (Huang, Zhou, Zhang, Wang, & Tang, 2011; Nkurunziza, Gebhardt, & Pilz, 2010). The Sistan and Baluchestan Province has a warm and dry climate. It is the largest province of Iran in regard to area and has the most suitable climatological conditions for malaria transmission (Sheikhzadeh, 2010).
Malaria is a major health and economic problem in developing countries and has a possible association with climate factors. The Sistan–Baluchestan province is a troubled region in regard to malaria. In this study, researchers intended to evaluate the probable influence of temperature, humidity, and rainfall on the incidence of malaria in the malaria-prone towns of Sistan–Baluchestan. The results of this study will help to predict the incidence of malaria and take effective preventive strategies to control this disease.
Method
This article was part of a big project conducted about climate and malaria in three provinces of Iran. We reported the results of other provinces in other papers (Mohammadkhani, Khanjani, Bakhtiari, & Sheikhzadeh, 2016).
The Sistan–Baluchestan Province has an area of 178,502 square meters and is the widest province of Iran. This state includes the Sistan and the Baluchestan region. This province has a common border with Afghanistan in the north and a common border with Pakistan in the east. The southern border of this province is the shores of the Oman Sea (SCI, 2016).
This province is located in the desert and semi-desert region of Iran. The average annual rainfall of this province is about 100 mm and its average temperature ranges from 22°C to 37°C. The average rainfall in different regions is usually between 70 and 130 mm. In summer, the maximum temperature in cities such as Iranshahr and Zabol reaches 50°C. Zahedan is the coldest and Iranshahr is the hottest city of this province. In the southern parts of this province, during winter, the average daily temperature varies between 10°C and 25°C, and relative humidity varies between 50% and 95% during the year (SCI, 2016).
This ecological study was conducted based on the recorded cases of malaria in malaria-prone towns of Sistan–Baluchestan province during 2000 to 2012. The number of cases per month since the beginning of 2000 until the end of 2012 was inquired from the Deputy of Health at Sistan–Baluchestan University of Medical Sciences for the towns (Zahedan, Khash, Saravan, Iranshahr, Nikshahr, Chabahar, Konarak, Sarbaz, Mirjaveh, Dalgan, Suran, and Zaboli) based on the type of parasite.
All cases that happened during the period under study were included in this study. Authors assumed that the whole population was at risk during this time and used all available data. All cases were diagnosed and registered at the local town or rural health center, and the list was sent to the Health Deputy of the Province. The data covered the whole province.
Monthly weather data included average, minimum, and maximum temperatures and rainfall and relative humidity from 2000 to 2012 from different meteorological synoptic stations in the province. However, malaria data were registered in Konarak from 2007 and Sarbaz from 2002. Also, there was no meteorological data for Sarbaz during 2002 to 2004 and Dalgan, Suran, and Zaboli from the beginning of 2008. Therefore, the research stations were implemented in geographic information system (GIS), and spatial analysis was performed and by interpolation methods the unknown values were estimated using Kriging methods.
Finally, the relation between the incidence of malaria (the dependent variable) and climatic factors (average, minimum, and maximum temperature and relative humidity and rainfall were independent variables) was evaluated according to the data distribution and by determining the goodness of fit of models by likelihood ratio tests and the Akaike information criterion (AIC) and Bayesian information criterion (BIC). Eventually, the negative binomial regression model was used. Stata 11 was used for this analysis.
Negative binomial regression can be used for over-dispersed count data, that is, when the conditional variance exceeds the conditional mean. It can be considered as a generalization of Poisson regression since it has the same mean structure as Poisson regression and it has an extra parameter to model the over-dispersion. If the conditional distribution of the outcome variable is over-dispersed, the confidence intervals for the negative binomial regression are likely to be narrower as compared to those from a Poisson regression model.
Zero-inflated regression models attempt to account for excess zeros. The Vuong test can suggest if the zero-inflated negative binomial model is a significant improvement over a standard negative binomial model. In ordinary least squares (OLS) regression, count outcome variables are sometimes log-transformed and analyzed using OLS regression. Many issues arise with this approach, including loss of data due to undefined values generated by taking the log of zero (which is undefined) as well as the lack of capacity to model the dispersion (University of California, Los Angeles [UCLA], 2016).
According to the tests performed, zero-inflation and OLS regression were not the best statistical approach in this study. The Spearman correlation coefficient between each weather variable and the number of cases was determined by SPSS 19. In order to determine the potential impact of lagged weather variables on malaria transmission, cross-correlation analysis was performed by Minitab 16.
Cross-correlations between monthly malaria incidence series and monthly meteorological data time series were analyzed to find the time lag(s) of meteorological factors preceding malaria at which the series showed the strongest correlation.

Map of counties in Sistan–Baluchestan, Iran province.
Results
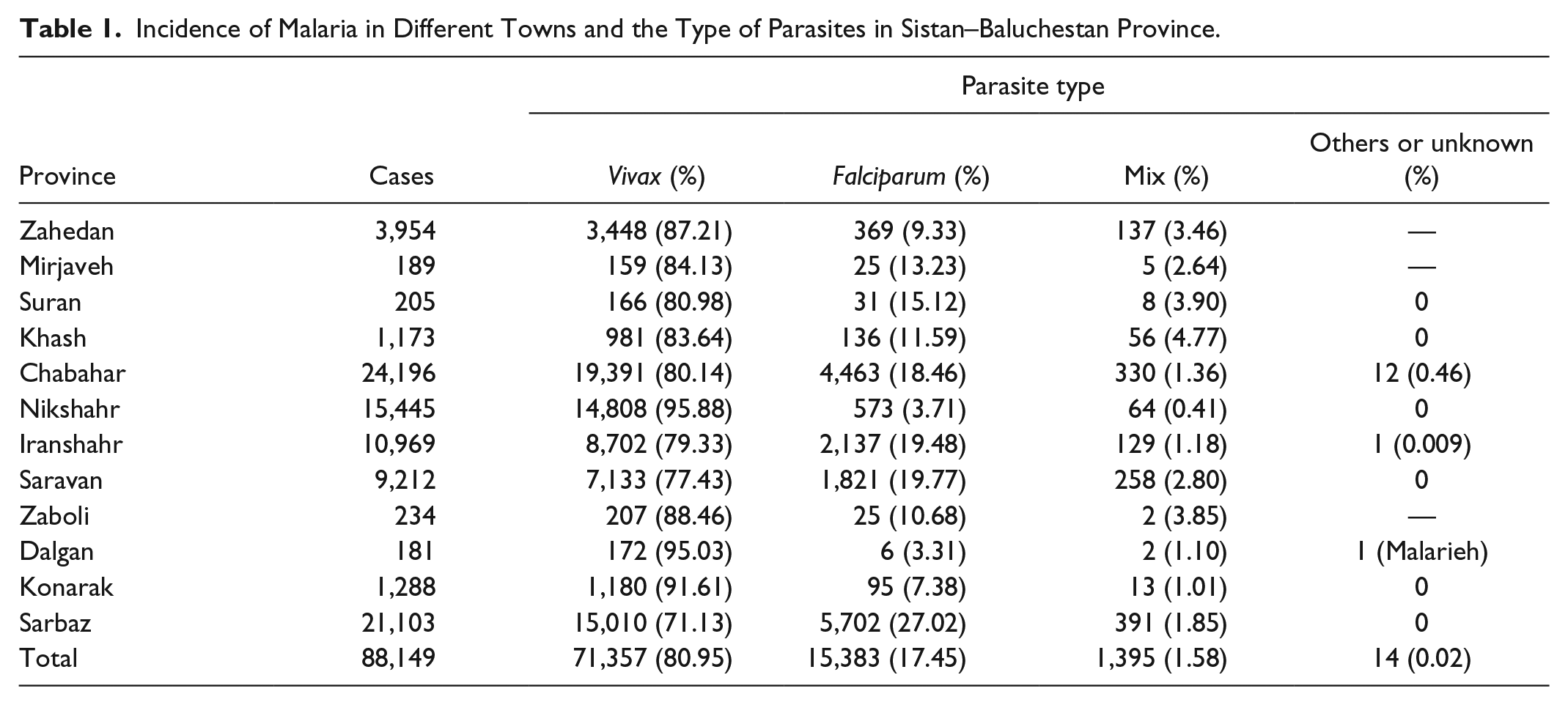
The total monthly number of the reported cases of malaria in Sistan–Baluchestan province was determined in each town. The results showed that during these years, Chabahar with 24,196 cases had the highest and Mirjaveh and Dalgan, respectively, with 189 and 181 had the least number of cases.
Plasmodium vivax was the predominant parasite in Sistan–Baluchestan province with 80.95% of the cases, and in, for example, Nikshahr, 95.88% of the parasites were vivax. Only one case of malaria was reported in Dalgan. The occurrence of disease in different towns and the type of parasites have been shown in Table 1.
Incidence of Malaria in Different Towns and the Type of Parasites in Sistan–Baluchestan Province.
Our study shows that during the studied years, an intermittent “drop & raise” pattern was seen in the incidence of malaria in all towns. Most of the cases happened during the earlier years (2000-2006), and then from 2008 to 2009, the incidence of cases in most towns such as Zahedan, Khash, and Saravan has been declining. Malaria has been declining in Iranshahr since 2002 and in Nikshahr since 2006. In Chabahar, the highest and lowest incidence was 5,278 cases in 2003 and 318 cases in 2011. The annual changes in the incidence of malaria in different towns can be seen in Figure 2.

Annual changes in the incidence of malaria in Sistan–Baluchestan towns.
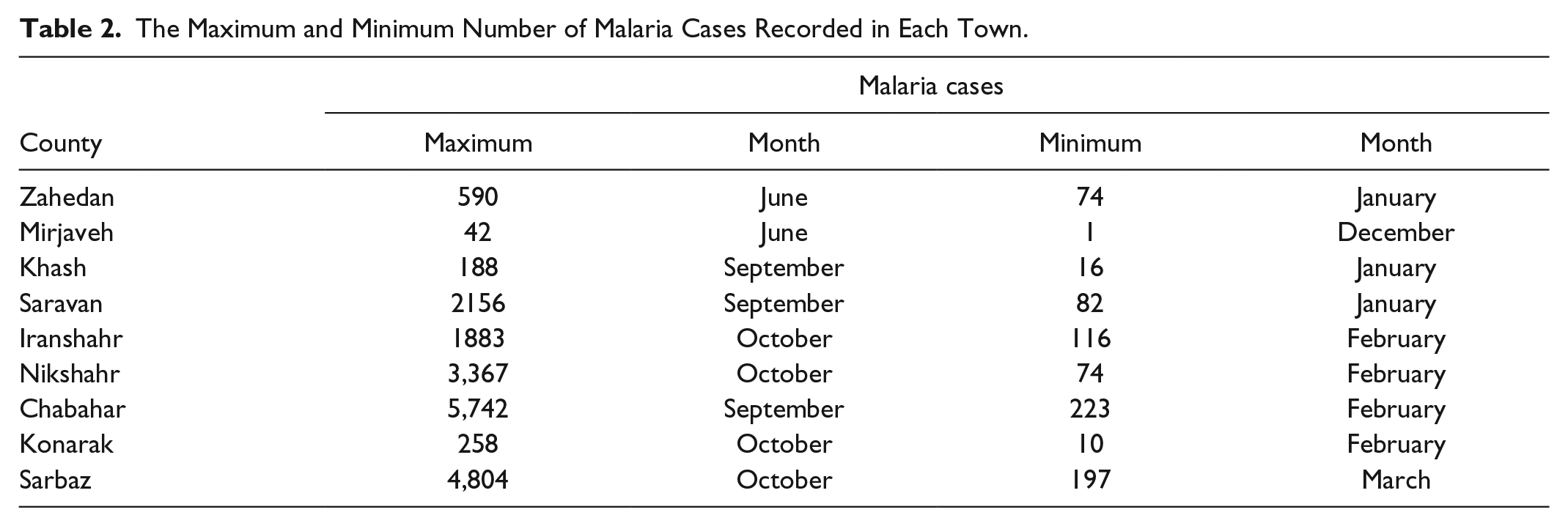
Malaria was reported in all seasons of the year, but had a lot of seasonal variation. Most cases occurred in the summer in all towns, except Sarbaz that had the highest incidence in autumn and was 8,983 cases. After the summer season, most cases of malaria happened in autumn, spring, and winter. The peak of incidence was in June or September/October. The peak incidence in the town of Khash, Saravan, and Chabahar was in September and in Nikshahr, Iranshahr, Konarak, and Sarbaz was in October and in Zahedan it was in June. The rising incidence of malaria was from June to October. January and February had the lowest incidence of malaria. Malaria incidence has dramatically decreased during the years of this study. Months with the highest and lowest incidence can be seen in Table 2.
The Maximum and Minimum Number of Malaria Cases Recorded in Each Town.
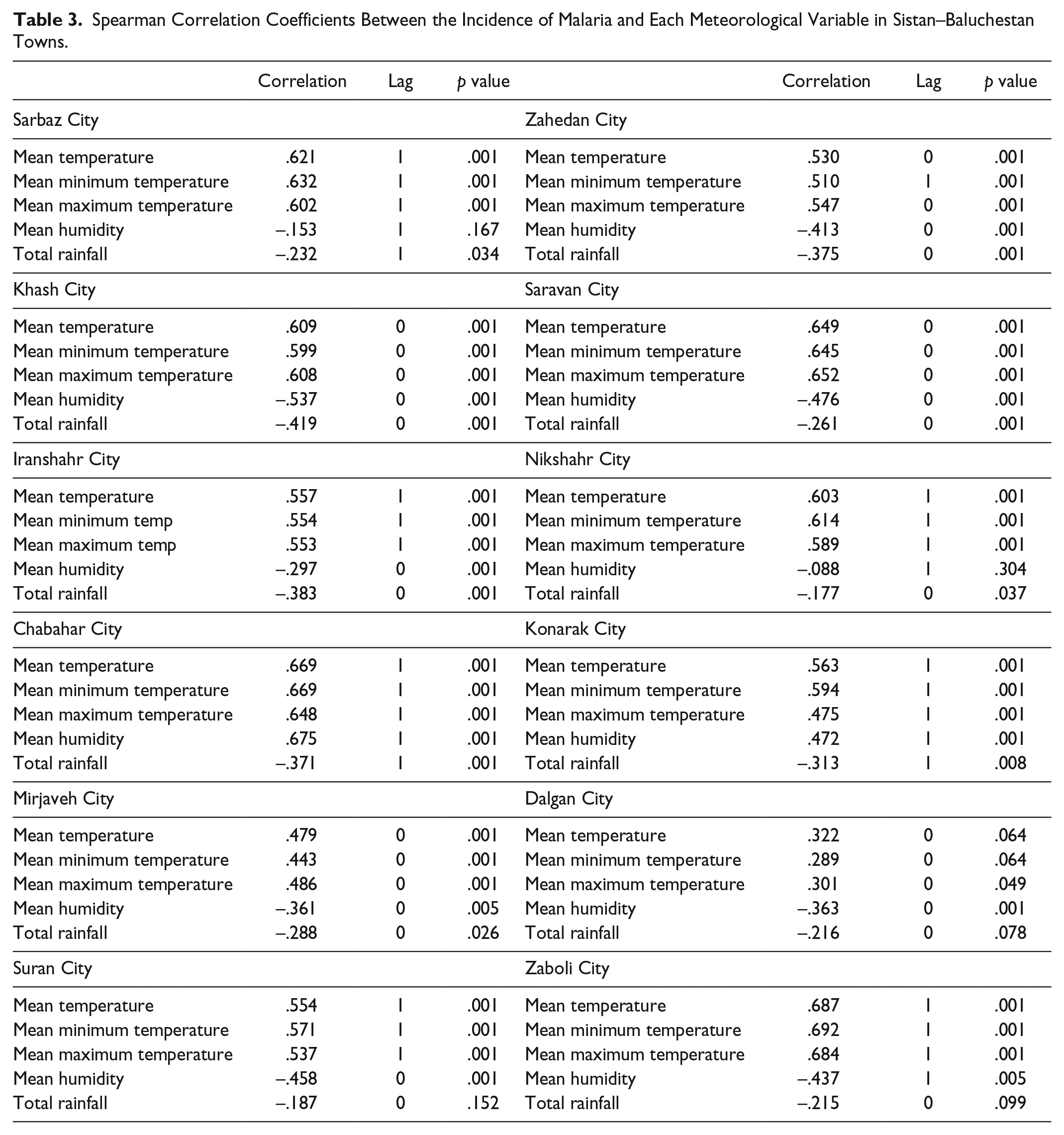
In order to find the relation between incidence and the meteorological variables, first cross-correlations were calculated up to 12 (month) lags and the Spearman correlation coefficients were determined. In all towns, the climatic variables in that specific month and with a maximum delay of 1 month had the highest effect on incidence.
In correlation analysis, the temperature variables (average, minimum, and maximum) in towns such as Iranshahr, Nikshahr, Konarak, Sarbaz, Suran, and Zaboli with 1 month delay and in the towns of Khash, Saravan, Mirjaveh, and Dalgan without delay showed the most positive relation and significant correlation with malaria. In the city of Zahedan, temperature (average and maximum) had a positive significant correlation with incidence in the same month, and minimum temperature of the preceding month had the highest positive correlation with incidence in the next month.
Relative humidity in most towns including Khash, Saravan, Iranshahr, Dalgan, Mirjaveh, and Suran showed a significant negative correlation with the incidence of malaria in the same month. While in Chabahar and Konarak, humidity in a specific month had the most positive and significant relation with occurrence in the next month.
In Chabahar, humidity showed the highest significant correlation (r = .675) with malaria incidence in the next month. Rainfall had an inverse association with malaria incidence and in comparison to temperature and humidity had the lowest correlation with incidence. These results are summarized in Table 3.
Spearman Correlation Coefficients Between the Incidence of Malaria and Each Meteorological Variable in Sistan–Baluchestan Towns.
Negative binomial regression results showed that increases in temperature increase the incidence of malaria. Both the minimum and maximum temperatures in all towns showed a direct correlation with incidence. Disregarding latency, increased humidity was associated with a significant decrease in the incidence of malaria in most towns except Sarbaz and Nikshahr. Overall, increase in rainfall was significantly associated with decrease in the incidence of malaria, except in Saravan, Nikshahr, and Konarak. The results of negative binomial regression analysis have been shown in Table 4.
The Effect of Maximum and Minimum Temperature, Humidity, and Rainfall on Malaria Incidence in the Same Month and the Next Month.
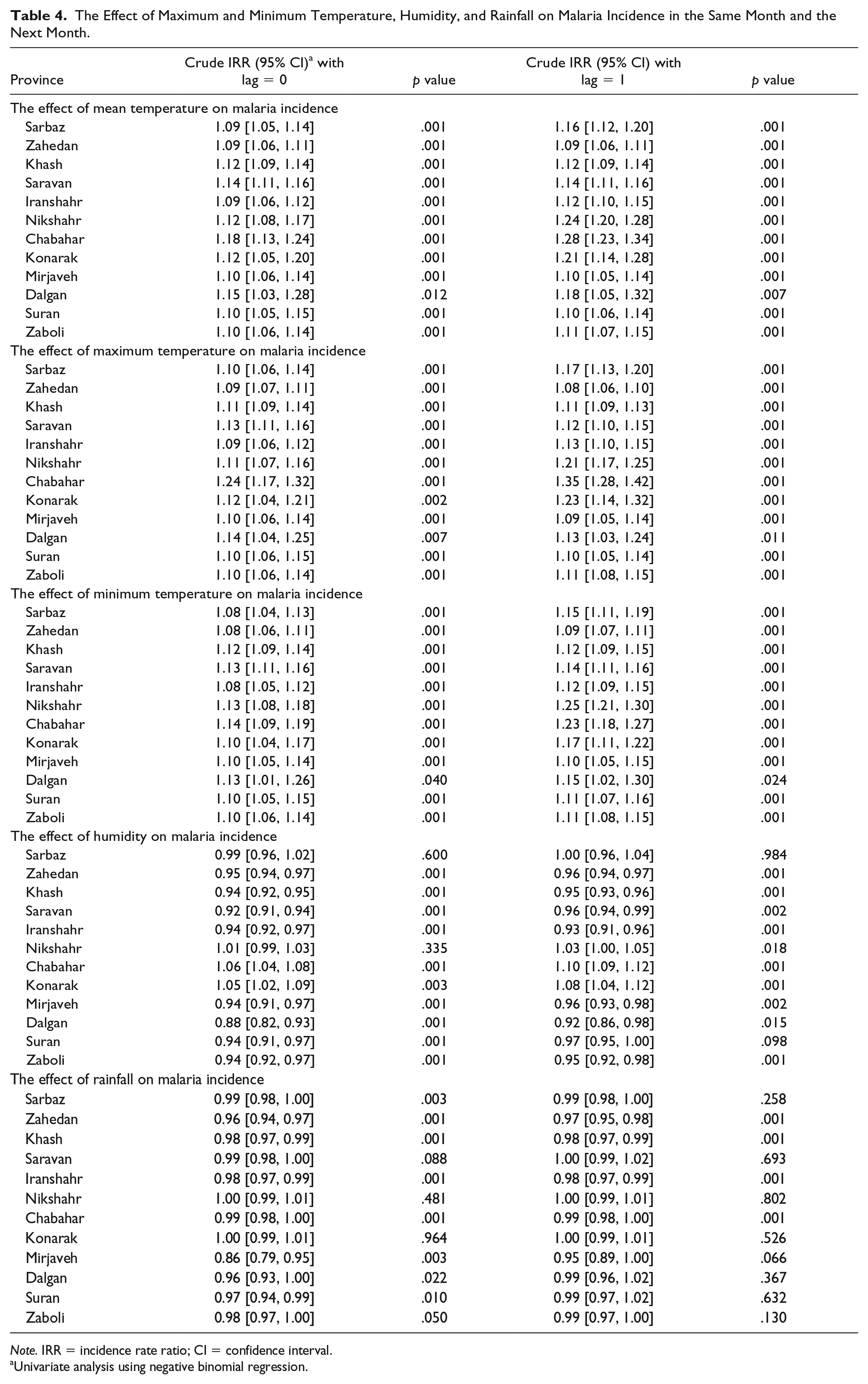
Note. IRR = incidence rate ratio; CI = confidence interval.
Univariate analysis using negative binomial regression.
Given the high prevalence of P. vivax in the province as well as the length of the parasite’s incubation period, in this study the effect of a 1-month lag of climate factors and the incidence of malaria was also analyzed. Again temperature in the previous month caused increase in the incidence of malaria in the next month and the increase was even higher than the same month. For example, in Nikshahr and Sarbaz, an increase in 1°C of minimum temperature in a specific month caused a significant increase of 25% and 15% in malaria incidence in the next month, respectively. This increase was almost 2 times the increased incidence in the same month.
In Sarbaz, Iranshahr, Nikshahr, Chabahar, and Konarak, the increase in maximum temperature was associated with increased incidence by 17%, 13%, 21%, 35%, and 23%. In this province only in Chabahar, Konarak, and Nikshahr, humidity had a direct and significant impact on incidence in both “with a one-month lag time” and “without lag time” analysis. In the one-month lag time analysis, each 1% increase in humidity was respectively associated with a 10%, 8%, and 3% increase in malaria incidence. Variations in humidity and malaria incidence in Chabahar town have been shown in Figure 3.
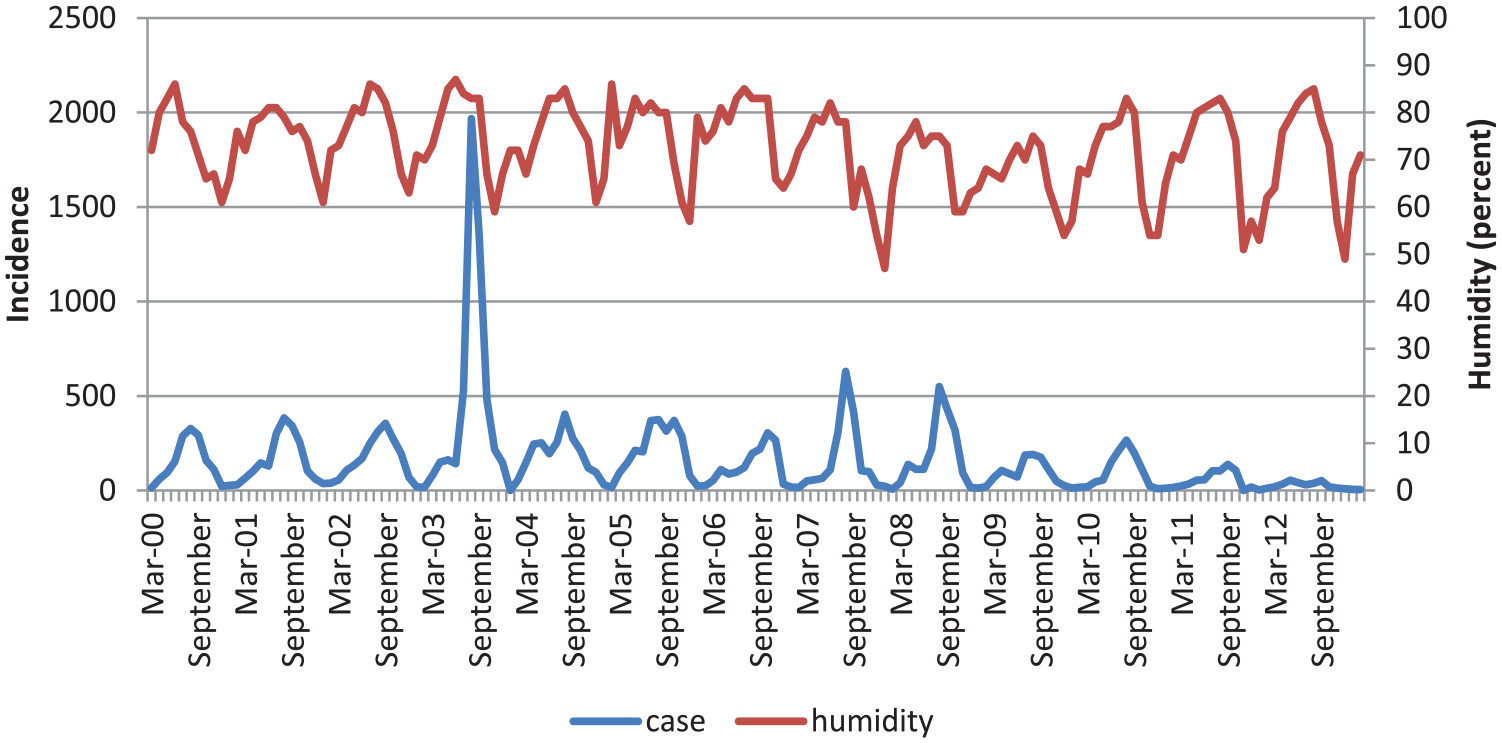
Variations in humidity and malaria incidence in Chabahar town (2000-2012).
As it can be seen in Table 4, no significant relation was found between incidence and rainfall; except that an increase of 1 mm rainfall in Chabahar, Iranshahr, Khash, and Zahedan significantly reduced the incidence rate by 1%, 2%, 2%, and 3%.
Discussion
In this study, temperature had a stronger relation than rainfall and humidity with the incidence of malaria. This relation was direct and significant and stronger after a 1 month lag. In this province, more than 80% of the cases were vivax and the delay of a month was consistent with the generation time of P. vivax that was approximately 8 days in the exoerythrocytic stage, 2 days in the erythrocytic stage, and 9 days inside the mosquito—a total of 19 days (Bi et al., 2003).
The highest incidence rates of malaria infection in Sistan–Baluchestan province was in Chabahar—probably because this town is located in the southern part of the province and the higher temperatures in the south provide a longer time for disease transmission (Ostovar et al., 2012).
Zhao et al. (2013) by multivariate stepwise linear regression analysis showed that the average monthly temperature is the main significant factor that affects the density of mosquitoes (r = 0.844, p = .001). Another study by Nkurunziza et al. (2010) in Burundi in East-Central Africa also showed that the incidence of malaria in a specific month was related to the minimum temperature of the previous month. While Zacarias and Majlender (2011) in a town in Mozambique and Imbahale, Mukabana, Orindi, Githeko, and Takken (2012) in three different regions of western Kenya showed that average temperature does not change the incidence of disease, this lack of association between disease and temperature shows that at least 28°C is required during the malaria transmission period. This minimum temperature was fulfilled in our study.
Alemu, Abebe, Tsegaye, and Golassa (2011) in a town in southwestern Ethiopia during 2000 to 2009 found that average and maximum monthly temperature in a specific month was associated with the incidence of malaria in the same month; but the maximum temperature of the previous month was negatively correlated with the incidence of malaria in the next month. However, in our study, maximum temperature had a positive effect on incidence in both the same month and 1 month later. The relation between minimum temperature and the incidence of malaria in the next month in Alemu et al. (2011) study was direct and significant and similar to our study. A study by Nkurunziza et al. in Burundi in a 12-year period showed that the incidence of malaria in a specific month has a positive association with minimum temperature in the same month and a strong association with minimum temperature of the previous month, and in contrary, the incidence of malaria in a specific month was negatively associated with maximum temperature of the same month. The relation between minimum temperature and incidence in their study is consistent with the results of our study. Since mosquitoes are active at night, minimum temperature has been known as an effective factor in the incidence of disease. In addition to this, due to the evolution of the parasite inside the mosquito and its incubation period, people who got malaria in a specific month were probably bitten by mosquitoes in the previous month, and this explains why the incidence of malaria in a specific month shows a stronger association with the previous month’s minimum temperature. Unlike the results of this study, the maximum temperature in our study was positively correlated with incidence; even though it has been suggested that high temperatures disturb the mosquitoes’ life cycle. This inconsistency can be related to mosquito habits and their adaptation to the region’s climate (Nkurunziza, Gebhardt, & Pilz, 2011). According to the region’s meteorological information, in this region (Burundi region), the average temperature was 20°C and the temperature range was 16°C to 23°C, which is not much different from the temperature in the region of our study.
In towns of Sistan–Baluchestan Province with humidity below 40%, the incidence significantly decreased with the increase in humidity. It has been mentioned that when humidity falls below 60% due to the shortened life span of mosquitoes, transfer does not happen. In Alemu et al.’s (2011) study, moisture was negatively correlated with the incidence of malaria in the next month.
However, in Chabahar and Konarak, both correlation coefficients and negative binomial regression showed that increase in humidity was related to increase in the incidence of malaria. The reason is probably the fact that the average monthly humidity in these areas is between 60% and 80% and is high enough for the incidence of malaria to happen throughout the year, because high humidity will increase the mosquito’s life span and helps the parasite complete its life cycle and transmit the infection (Akinbobola & Omotosho, 2013). In Chabahar, the effect of humidity on the incidence of disease in the next month was even more than temperature, and Spearman correlations showed that the coefficient between the average of temperature and humidity with malaria incidence was .669 and .675, respectively. In Zacarias’ study, humidity had a positive association with the incidence of malaria and was one of the predictor variables of malaria in the region (Zacarias & Majlender, 2011).
Rainfall showed a complex relation with malaria incidence in our study, and by increased rainfall, the incidence of malaria decreased, increased, or remained unchanged. The correlation coefficient between monthly rainfall and monthly malaria incidence was less than the correlation coefficient between the monthly cases of malaria and other weather variables. Rainfall was the least significant influencing factors on the incidence of malaria in our study.
The time and location of precipitation plays an important role in disease transmission. If precipitation occurs before the Anopheles’ reproductive season, rivers and water streams can become places for mosquito breeding, but if rainfall occurs during the reproductive season, it will wash the breeding sites and reduce malaria transmission (Juri, Zaidenberg, Claps, Santana, & Almiron, 2009).
In Alemu et al.’s study in the southwest of Ethiopia, rainfall after minimum temperature was the most important determining factor in malaria transmission, and Imbahale et al.’s study in three different regions of western Kenya showed that rainfall was significantly associated with the occurrence of Plasmodium falciparum malaria. The effect of rainfall on malaria transmission is probably related to the special geographical conditions of each region and is dependent on the local habits of mosquitoes. The southwest of Ethiopia and the regions studied in Western Kenya were regions with mountainous climate and abundant rainfall and had favorable conditions for agriculture, which created suitable sites for mosquito reproduction and therefore mosquito density increased and rainfall was found to be an effective factor on malaria incidence. But in our study, the climate was warm and dry and the amount of rainfall was very low and it evaporated quickly or in some circumstances was so much that flooding happened and washed the larvae’s habitat and destroyed the larvae (Alemu et al., 2011; Imbahale et al., 2012).
The study by Nkurunziza et al. in Burundi over 12 years showed that the incidence of malaria in a specific month was negatively associated with rainfall in the same month. In their study, significant negative correlations of rainfall with incidence were probably due to excessive rainfall and destruction of mosquito larvae habitants and reduced mosquito population density. While in Zacarias’ study in Mozambique over 2 years, rainfall was positively associated with the incidence of malaria and was a part of the predictor variables for malaria in this region (Nkurunziza et al., 2011).
In a recent study in the south of Kerman province, Iran, only temperature was the affecting climate variable on the incidence of malaria. Average maximum monthly temperature with a 1 month lag was a strong and positive predictor of increased malaria incidence, and minimum monthly temperature also had a positive significant relation with malaria incidence in the next month (Mohammadkhani et al., 2016). Although, in Sistan–Baluchestan like the south of Kerman province, temperature changes, especially with a month delay caused the largest increase in the incidence of malaria, but unlike the south of Kerman province in Sistan–Baluchestan, humidity and rainfall also showed some significant effects on the incidence of malaria.
Conclusion
Temperature and humidity over 60% show a significant positive impact on the incidence of malaria in Sistan–Baluchestan. These factors should be considered in planning for controlling and preventing malaria in tropical and subtropical countries. However, the relation between rainfall and malaria incidence is complex and needs to be further investigated in different world regions.
Footnotes
Acknowledgements
The authors would like to thank the Health Deputy of Zahedan University of Medical Sciences for their cooperation.
Author Contributions
M.M. and N.K. designed research; M.M., N.K., B.B., S.M.T., and K.S. conducted research; M.M. and N.K. analyzed data and wrote the paper. M.M. and N.K. had primary responsibility for final content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Kerman University of Medical Sciences, Kerman, Iran (Grant No. 180-92). The funder had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Ethics Approval and Consent to Participate
This project was approved by the Ethics in Research Committee of Kerman University of Medical Sciences.
Availability of Data and Materials
The datasets analyzed during the current study is available from the corresponding author on reasonable request.