
Abstract
Traditional Chinese medicine (TCM) is an important component of China’s medical system. How to educate TCM practitioners in China, therefore, has become a crucial issue. To contribute to this issue, the current research identified the competency model of TCM practitioners in China and developed an evaluation for TCM students. We combined Bloom’s taxonomy with our model construction to examine the current TCM practitioners’ requirements. Following the protocol of developing a measurement, we interviewed 20 TCM practitioners, conducted two rounds of surveys in China (n = 220/n = 489), ran exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), and examined the correlation between the measurement and self-rated outcomes. The evaluation tool of TCM students consists of five factors: modern medical knowledge and skills, TCM medical knowledge and skills, professional ethics, communication and cooperation skills, and clinical practices. The reliability and validity of our evaluation tool were testified. Our work may contribute to TCM education in China.
Keywords
Introduction
Traditional Chinese medicine (TCM) is currently flourishing on the health markets all around the world (Hsu, 2008). As a historical alternative medicine, TCM plays an important role in China’s medical system. By the end of 2015, the TCM outpatient service accounted for 15.7% of total medical services in mainland China; 41.87% of senior citizens (over the age of 65) and 53.59% of children aged 3 and under got TCM health management service; the output value of TCM industry was 86.5 billion yuan (about 12.9 million US$; State Administration of Traditional Chinese Medicine, 2017). By the year of 2014, there were 545,000 TCM practitioners in mainland China (National Bureau of Statistics of China, 2015) and over half a million TCM practitioners engaged in medical work around the world apart from mainland China (Jiang, 2017).
As TCM has grown in importance, TCM education has become a rising concern. In mainland China, mainstream TCM education occurs at the college or university level, including at 23 TCM universities or colleges and through a TCM major at Capital Medical University and Xiamen University. Numerous works have already examined the importance of education for one’s profession, but there is still a gap between higher education and practice for medical students, for example, some students may not know how to communicate with patients or how to deal with complex cases (e.g., Frederiksen, 2010; Hansen, 2001; Hariprasetya, Wiyono, Imron, & Arifin, 2016).
The competency perspective may fill this gap. This concept was proposed by McClelland (1973), referring key behavioral attributes for performance. Since then, researchers found out that building a competency model can help to direct one’s career development (Enz & Siguaw, 2000). A competency model will also help to improve curriculum design and identify a proper career development path (Noe, 2008). In 2002, the Institute for International Medical Education put forward global minimum essential requirements (GMER) in medical education, which concludes seven domains, that is, professional values and attitudes, scientific foundations, population health, clinical skills, critical thinking, information management, and communication skills (Institute for International Medical Education, Core Committee, 2002).
There are a few research and documents related to a competency model for TCM practitioners. For example, in mainland China, Tang (2014) developed a competency model based on GMER, while Xu, Luo, Ren, and Guo (2009) proposed a model for famous and veteran TCM physicians. The State Administration of TCM in China holds a qualification exam once a year, which can be regarded as an official competency requirement (State Administration of Traditional Chinese Medicine, 2017). There are also some standards outside mainland China. The Pan-Canadian Standard for Traditional Chinese Medicine Practitioners and Acupuncturists: Entry-Level Occupational Competency Profile (Canadian Alliance of Regulatory Bodies for Traditional Chinese Medicine Practitioners and Acupuncturists, 2018) is a model adapted in Canada, which includes nine components, that is, interpersonal skills, professionalism, practice management, TCM foundations, fundamentals of biomedicine, diagnostics and treatment, acupuncture techniques, herbal therapy and management, and safety. This model is a model which has the comprehensive perspective on TCM practitioners’ competencies. The Objective Structured Clinical Examinations held in Taiwan Region and the assessment of overseas qualified TCM practitioners in Australia are also examples. All of these previous literature suggest how a qualified TCM practitioner should be.
However, given our focus on TCM education in China, we still needed a tool to assess TCM students’ core competencies. Considering the lack of this evaluation tool in current research, we developed one, following the protocol of developing a measurement. We interviewed TCM practitioners in China to identify core competencies, developed a scale based on these competencies, and administered questionnaires to validate the scale. Because in mainland China most TCM students who become doctors work at hospitals (rather than clinics), we clarified that the main work setting in our research was China’s hospitals.
Theoretical Framework
Developing a TCM Competency Model for Education
As McClelland (1973) proposed the concept of competency, scholars have continued to explore it. Spencer and Spencer (1983) believed that motivation, idiosyncrasy, self-concept, attitude, and behavioral skill are essential to individual’s success. Boyatzis (1983) argued competencies are potential traits, which would lead to good performance. In the perspective of lifelong learning, people need several personal competencies, including life values, necessary knowledge, practical skill, and so on (Friesen & Anderson, 2004). Paquette and his colleagues (2006) demonstrated a knowledge engineering process where knowledge and competencies, learning design, and delivery model were constructed in an integrated framework.
In education, the meaning of competency is to examine whether graduates or approaching graduates have the right qualifications that meet future career requirements. In Asame and Wakrim’s (2017) model, competency is a set of personal characteristics (skills, knowledge, attitudes, etc.) that a person acquires or needs to acquire, to perform an activity inside a certain context with a specific performance level. For medical practitioners, some scholars have focused on the practical clinical physician requirement (Martimianakis & Hafferty, 2013; Vaughn et al., 2015), while others made connections with modern medical education (Atkinson, Tan, Brennan, & Granville, 2014; Lee, Oh, Kim, Lee, & Shin, 2010; Talbot, 2004). The GMER is an example for medical education, comprising of sciences basic to medicine, clinical knowledge and skills, professional values, behavior, and ethics (Institute for International Medical Education, Core Committee, 2002).
In building a tool for TCM education based on a competency model, we decided that Bloom, Engelhart, Furst, Hill, and Krathwohl’s (1956) taxonomy of educational objectives could bridge education and competency. This model includes three domains: knowledge-based cognitive domain (Bloom et al., 1956), emotive-based affective domain (Simpson, 1966), and action-based psychomotor domain (Krathwohl, 2002). The knowledge-based cognitive domain of TCM education could relate to the modern and traditional Chinese medical knowledge, which students and practitioners are required fully to understand and master. The emotive-based affective domain could relate to how individuals react emotionally in a particular situation to improve the individual’s morale (Bloom et al., 1956). The Chinese Oath for a Medical Student says, “Health entrusted, Lives confided” (Ministry of Education of the People’s Republic of China, 1991), which sets a moral standard for TCM students. The action-based psychomotor domain could be about the ability to master the physical operation skills (Harrow, 1972). For TCM practitioners, this would involve clinical practices such as the diagnosis of complicated cases and clinical study of a particular disease. By considering Bloom’s taxonomy, we could identify the core competencies for TCM practitioners and apply it in education.
Key Factors of TCM Practitioners’ Competency
Key factors of professional competency have been defined by several scholars: knowledge, ethics, and independent judgment (Parkinson & Chew, 2016); job performance in a fair and ethical manner (Stan, 2016); a role that fulfills the task and organizational demands (Wendy & Strebler, 1994); an ability comprising skills, knowledge, and attitude; and so on (Ron, 2004). From the above research findings, knowledge, skill, ethics, and organization are the keywords emphasized in previous studies. As our focus is on TCM students who will work at hospitals in China, based on previous literature and interviews on Chinese TCM practitioners, we assume that the TCM practitioners’ core competencies fall in the following five domains: modern medical knowledge and skills, TCM knowledge and skills, professional ethics, communication and cooperation skills, and clinical practice.
Modern medical knowledge and skills
Modern medicine (called “Western medicine” in China) is an evidence-based discipline and the main component of the current Chinese medical system. In the qualification examination for TCM practitioners, Diagnostic Fundamentals, Epidemiology, Internal Medicine, Medical Ethics, and Sanitary Legislation are the compulsory subjects (State Administration of Traditional Chinese Medicine, n.d.). The Chinese government is promoting the combined treatment of TCM and modern medicine (Li, 2011), and integrative treatment has been successful in medical markets (Cheung, 2011). Researchers on modern medical knowledge and skills research have focused on different aspects (Borsoi, Rieder, Stein, Hofhansl, & Dorner, 2014; Madigosky, Headrick, Nelson, Cox, & Anderson, 2006; Mark, Steven, Jason, & John, 2006); for example, the modern medical service capacity includes medical basic operational skills, symptoms and diagnosis, history-taking, and somatoscopy (Jin, Jia, & Sun, 2013). In our model, modern medical knowledge and skills refer to logical thinking ability, pharmacology, pathology, and laboratory report interpretation in the actual operating environment.
TCM knowledge and skills
TCM is based on traditional Chinese philosophy, which includes concepts of yin-yang and the five elements (Cao, 2004), while also having great development and modernization in recent decades (Yan & Ni, 2012). Public sectors have set some requirements for TCM practitioners. The local government of Taiwan Region is carrying out Objective Structured Clinical Examinations, which considered TCM Internal Medicine, TCM Gynecology, TCM Pediatrics, Acupuncture, TCM Orthopedics, and Traumatology as the main testing subjects (Y. Chen, Hou, Lin, & Tung, 2015). Meanwhile, in the qualification examination for TCM practitioners in mainland China, the requirements include TCM Basic Theory, TCM Diagnostics, TCM Materia Medica, TCM Formulae Pharmacology, TCM Internal Medicine, TCM Surgery, TCM gynecology, TCM Pediatrics, and acupuncture (State Administration of Traditional Chinese Medicine, n.d.). The World Health Organization (WHO; 2010) defined TCM training as “covering the basic theories of traditional Chinese and allopathic medicine, as well as the knowledge and skills required for the qualified and safe practice of TCM and relevant research.” In the current research, we would consider all the above information to identify elements of TCM knowledge and skills.
Professional ethics
Given that the work of medical practitioners is to cure sickness and save the patient, their professional ethics requirement is higher than most other occupations (Bakshtanovskii & Sogomonv, 2007). Professional ethics codes have been established for different branches of medicine, for example: The Code of Medical Ethics of the American Medical Association (American Medical Association, 2003), the American Association of Naturopathic Physicians’ Code of Ethics (American Association of Naturopathic Physicians, 2015), and the American College of Sports Medicine (ACSM) Certification (Riebe, 2013). To codify TCM practitioners’ professional ethics, we need to clarify the profession’s nature and spirit. As TCM therapy has more than 3,000 years’ history in China, and has recently been greatly developed and modernized (Xu & Yang, 2009), the nature and spirit of this profession have been both inherited and carried forward, that is, curing sickness and saving the patient have never changed, while keeping pace with latest scientific developments and adapting to social change are new challenges. We suggest that the definition of TCM practitioners’ professional ethics is being responsible to their occupational task, abiding to relevant laws and regulations, and meeting moral standard set by society.
Communication and cooperation skills
Communication and cooperation skills play a vital role in any social system (Miller, Butts, & Rode, 2002). For medical practitioners, successful communication with patients and their relatives and cooperation with their colleagues are crucial for their work (Institute for International Medical Education, Core Committee, 2002). The medical system of China is quite different from other countries in that modern medicine and TCM are two parallel systems. As a result, Chinese patients may have a confused impression about TCM (Lam & Sun, 2013). A TCM practitioner may therefore need to have better skills in communication and cooperation than someone who is exclusively a practitioner of modern medicine. In our view, the communication and cooperation skills of TCM practitioners involved not only relationships with patients and colleagues but also the relationship between modern medicine and TCM (e.g., having an open mind to different schools of TCM).
Clinical practice
Clinical practice is an action-based psychomotor component. WHO (2014) released WHO Handbook for Guideline Development, which is regarded as the most authoritative set of guidelines for clinical practice. Also, many countries have started to establish their own clinical practice guidelines, for example, Clinical Practice Guidelines in the United States (National Center for Complementary and Integrative Health, National Institutes of Health, 2017) and Clinical Practice Guidelines in China (Lai & Hou, 2015). Inspired by these guidelines, we examined the comprehensive practical ability of TCM practitioners, for instance, in self-promotion, treatment of specific diseases, adaptability to organizations, and so on.
Methodology and Results
In the previous section, we have discussed the key factors of TCM practitioners’ competency in China. To operationalize this model and contribute to TCM education, we developed an evaluation tool for TCM students working in Chinese hospitals, as seen below. Following Churchill’s (1979) and Hinkin’s (1998) suggestions, the current research took a three-session procedure to develop a measurement. First, we generated the initial item pool from semi-structured interviews and a literature review and formed an initial version of scale. Then, we conducted the first round of survey, which included this initial scale, and did item reduction to form an improved version of scale. Finally, we conducted the second round of survey, including the improved scale, and evaluated the reliability and validity.
Item Generation and Filtering
We conducted a series of semi-structured interviews with 20 TCM practitioners to generate the initial item pool. All the practitioners work at medical schools and/or hospitals. Their average age is 33.7 (SD = 4.2) and their average tenure is 7.7 (SD = 3.9); 90% of them received a master’s degree, while the remaining 10% have a doctoral degree.
All of the participants were required to answer a series of questions on their work experience, what they learned from their practice, and their perspective on how to become a good TCM practitioner. We also ask them about their ideas on the internship of TCM students. To find out more detailed information on their work experience, we also conducted a behavior event interview (BEI).
Using text analysis techniques, we identified several themes related to competency. According to our theoretical framework, the results were clustered into five domains, which were the aforementioned five factors, that is, modern medical knowledge and skills, TCM knowledge and skills, professional ethics, communication and cooperation, and clinical practices. Based on this, we developed the items for TCM practitioners’ core competencies, adding items retrieved from previous literature. Table 1 shows this initial item pool, with defined five most crucial themes.
Initial Item Pool.

Note. (R) means reverse coded. The column Source represents where the item came from, that is, from interviews (I) or from literature (L) or from both of them (I & L). The column Remained represents whether the item remained or not after content adequacy test. TCM = traditional Chinese medicine.
After identifying five critical themes and generating related items, we needed to filter appropriate items for the competency model. We did a content adequacy test. In this process, we invited 10 TCM practitioners, not involved in our interviews, to evaluate our initial items. They were required to assess the relevance and importance of each item to the main theme and to give comments on the content and expression of items.
In the end, eight items were excluded through this process, for one of the following reasons: (a) the item was irrelevant to being a TCM practitioner, (b) the item was not important to current TCM practice, and (c) the item was not well defined or not suitable for TCM in Chinese context.
Initial Item Reduction and Evaluation
Using the items filtered in the above step, we developed a questionnaire including them and related questions regarding participants’ information. For items related to knowledge and skills, we used a 4-point response format, ranging from 1 = barely mastered to 4 = fully mastered. For items related to ethics, communications, and practices, a 5-point Likert-type format was adopted, ranging from 1 = strongly disagree to 5 = strongly agree.
The questionnaire was administrated in a survey initiated by a TCM college in Zhejiang Province, designed to evaluate the efficacy and quality of medical students’ internships. All the targeted students had more than a half year’s experience working in the hospital. All of them participated voluntarily, and the results were kept confidential; 220 students completed the questionnaire, yielding a response rate at 37.0%. Among them, 68.6% were female, and the average age was 21.5 (SD = 0.8).
Note that the reason to choose this sample was in line with our goal to develop an evaluation tool for TCM students based on competency. First, these students already have the necessary knowledge and skills to be a competent TCM practitioner; thus, the model of formal TCM practitioners (doctors, pharmacist, etc.) would be appropriate for them. Second, due to their limited work experience, validating the model among them could contribute to the education implications of the current research as well as to the TCM literature.
Following Hinkin’s (1998) suggestion, we tested correlations among items. As all the inter-item correlations were below .700, it suggested that we avoided too much redundancy and artificially inflated estimates of internal consistency.
Then, we ran exploratory factor analysis (EFA), adopting principal factor analysis to extract factors and using the varimax approach to rotate. Given the response style was different in Part I and Part II, we ran EFA separately. Kaiser–Meyer–Olkin (KMO) coefficients for Part I and Part II were .936 and .884, respectively, and Bartlett’s test of sphericity were both significant, indicating that factor analysis could be performed validly. Two factors for Part I and three factors for Part II emerged, according to eigenvalue criterion in conjunction with a scree plot. The criteria to exhibit an item are as follows: (a) factor loading less than .40 and (b) cross-loading greater than .40. Thus, one item was excluded in Part I, and two items were excluded in Part II. Table 2 presents the result of this process, showing the factor loading of each item.
Results of Factor Analysis.

Note. (D) denotes items were deleted after initial item reduction; Factors I to V were named as TCM knowledge and skills, modern medical knowledge and skills, clinical practices, communication and cooperation skills, and professional ethics, respectively. TCM = traditional Chinese medicine.
Factor I contains important medical knowledge and skills in modern medicine, which could help TCM practitioners achieve more accurate diagnosis; thus, we termed it modern medical knowledge and skills. It includes six items. Factor II consists of six items, labeled TCM knowledge and skill, which are related to key knowledge and skills that a TCM practitioner should master. Factor III, termed clinical practices, includes eight practices embedded in action-based psychomotor that could lead to better performance in an actual working environment. Factor IV, communication and cooperation skills, refers to the communication with patients, non-professional people, colleagues, and supervisors, and includes 13 items. Factor V, professional ethics, refers to moral requirements in the work and includes nine items.
We estimated the internal consistency for each factor. The Cronbach’s alpha coefficients of the five factors are .864, .886, .905, .832, and .747, respectively. The overall Cronbach’s alpha coefficient is .939. These results suggested this scale was reliable.
A confirmatory factor analysis (CFA) approach was also conducted in the evaluation. Following the result of EFA, we construct a three-order model: all items belong to five factors listed above—among them, modern medical knowledge and skills along with TCM knowledge and skills belong to second-order Factor A; professional ethics, communication and cooperation skills, and clinical practices belong to Factor B; then, Factors A and B belong to third-order main factor (TCM practitioners’ competency; this model correlates Factors A and B). According to the result of CFA, this model fits the current sample well, χ2 = 1,537.1, df = 813, χ2/df = 1.89; comparative fit index (CFI) = .826; and root mean square error of approximation (RMSEA) = .064. Figure 1 demonstrated the standardized weights of these items on their belonging factors.

Structure of TCM practitioners’ competency.
In addition, we computed the composite reliability for the five factors (Bacon, Sauer, & Young, 1995). They were .866, .898, .752, .839, and .906, respectively, which were all above .700, the criterion suggested by previous scholar (Nunnally, 1978).
Replication
Although the data above provided some evidence that the measurement of TCM practitioners’ competency model was valid and reliable, following previous literature, we did replication.
In this round of survey, the questionnaire was distributed in another TCM college located in Yunnan Province. Similar to the first round of survey, the second round surveys also invited the participation of TCM students who had more than a half year’s internship at the hospital. The questionnaire included our evaluation tool, a scale based on GMER (Tang, 2014), and the evaluation of internship and their future career. As a replication in similar setting, it could exclude the influence caused by different college or location, thus validating the robustness of this competency model. All participants were voluntary to response, and the data were confidential; 459 students completed this survey (response rate = 57.3%), among them, 66.0% were female, and the average age was 21.7 (SD = 1.1).
We did CFA to testify construct validity. Our hypothetical model is the same three-order model described before, which showed good fit (χ2 = 1,944.6, df = 813, χ2/df = 2.39, CFI = .868, RMSEA = .055). Figure 1 depicts the weights of these items on their belonging factors.
For comparison, we also developed alternative models: (a) a two-order model in which five factors belong to one second-order main factor (χ2 = 1,974.3, df = 814, χ2/df = 2.43, CFI = .867, RMSEA = .056); (b) combining communication and cooperation skills and clinical practices together, keeping other categories the same (χ2 = 2,270.6, df = 815, χ2/df = 2.79, CFI = .834, RMSEA = .062); (c) combining professional ethics and clinical practices together, keeping others the same (χ2 = 2,380.3, df = 814, χ2/df = 2.92, CFI = .821, RMSEA = .065); (d) combining modern medical knowledge and skills and TCM knowledge and skill together, keeping others the same (χ2 = 2,483.1, df = 814, χ2/df = 3.05, CFI = .809, RMSEA = .067); and (e) all items belong to one main factor (χ2 = 4,178.6, df = 819, χ2/df = 5.10, CFI = .616, RMSEA = .095). The result indicated that our hypothetical model was the best model.
In this step, the Cronbach’s alpha coefficients of the five factors were .874, .904, .792, .832, and .900, respectively. The overall Cronbach’s alpha coefficient is .939, and the composite reliabilities for the five factors are .878, .914, .794, .836, and .901, respectively.
We also investigated the convergent validity by computing the correlation coefficient between the current measurement and a scale based on GMER (Tang, 2014), which was .543 (p < .001), suggesting this measurement can assess the competency of a medical practitioner.
Moreover, we attempted to examine the predictive validity. We asked the students several questions, including self-assessment on their performance during internship, perceived effectiveness of their internship, the willingness to pursue their education, their willingness to be TCM practitioners, and their confidence they will become good TCM practitioners. Table 3 revealed the correlations among these factors, and the TCM competency was positively related to above five factors.
Correlation Among TCM Competency Factors and Outcomes (n = 459).
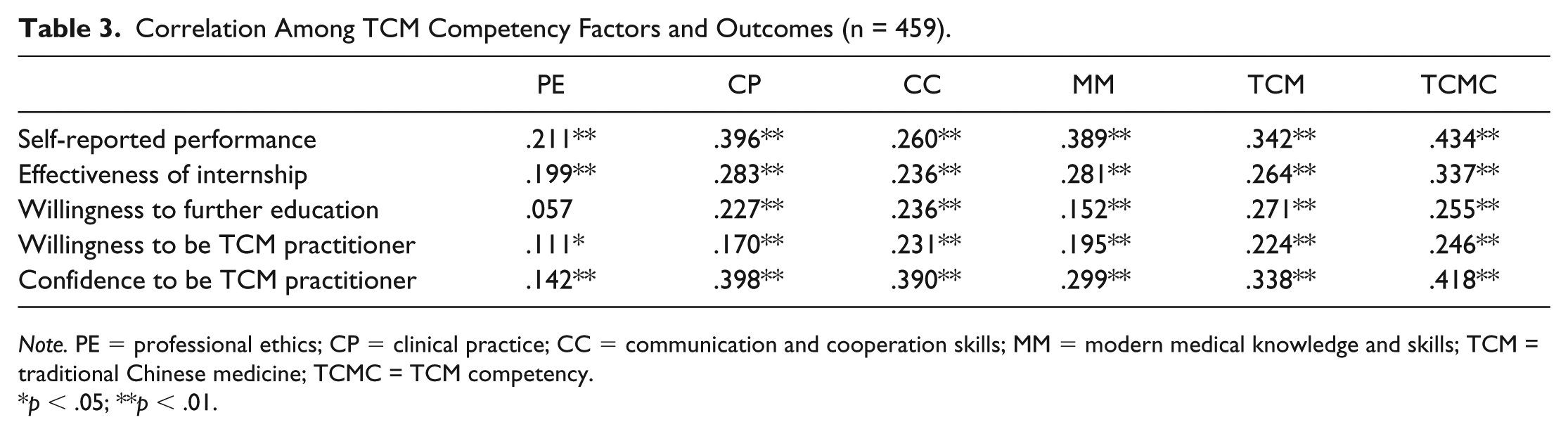
Note. PE = professional ethics; CP = clinical practice; CC = communication and cooperation skills; MM = modern medical knowledge and skills; TCM = traditional Chinese medicine; TCMC = TCM competency.
p < .05; **p < .01.
To conclude, the replicated survey provides evidence for the reliability and validity of this measurement.
Discussion and Conclusion
For a long time, researchers on medical education focused on knowledge, skills, and ability (Borsoi et al., 2014; Denton et al., 2009; Liabsuetrakul, Sirirak, Boonyapipat, & Pornsawat, 2012; Madigosky et al., 2006). These categories were not adequate, however, to evaluate the competency of a medical practitioner. Researchers started to try to evaluate medical competency by examining medical education from different perspectives, including the method of medical pedagogy (J. Chen et al., 2013; Kirby, Crawford, Smith, Thompson, & Sargeant, 2011; Lavranos, Koliaki, Briasoulis, Nikolaou, & Stefanadis, 2013) and medical curricula (Baerheim et al., 2007; Ostgathe, Voltz, Nauck, & Klaschik, 2007). We agree that it is quite necessary to review the medical education process to identify a competency model for medical education. On one side, we apply TCM practitioners’ practical needs in the actual hospital environment; on the other, we use the Bloom’s taxonomy to construct a competency model for medical students who are at the internship stage or are approaching graduation.
The current study follows the protocol suggested by previous scholars (Churchill, 1979; Hinkin, 1998) to identify the competency model of TCM practitioners and to develop an evaluation tool for TCM students. This measurement contains five factors, that is, modern medical knowledge and skills, TCM knowledge and skills, professional ethics, communication and cooperation, and clinical practices, which would play major roles in the work activities and career development of TCM students.
Note that we choose samples of students who have more than a half-year internship. This could be a proper career moment for assessment, because it is a time of transition. These students were nearly equal to a freshman doctor, and they have acquired a similar set of medical knowledge and skills as formal TCM practitioners. Yet they still lacked experience to deal with various patients and difficult or complicated cases.
Although the results of Table 3 might be influenced by common method bias, it still has some relevant implications. If we were to compare these coefficients, we could find out that different competency factors may have different effects on different outcome factors. For example, when the students assessed their performance during internship, the effectiveness of their internship, and their confidence to be a good TCM practitioner, clinical practices have the highest coefficient, implying practical experience would be the core competency. And professional ethics has low correlation coefficients with every outcome factor, suggesting it was more like a basic requirement rather than a distinguishable competency.
This research has some theoretical contributions. First, it followed a standard protocol for developing an evaluation tool. In general, our measurement reflects the core competencies for TCM students and practitioners. Given its reliability and validity, further TCM research could take this measurement as a tool to analyze and solve deeper research questions. Second, based on Bloom’s taxonomy, we connected three fundamental education domains to the competency factors, which is an educational perspective, and combined universal theory with specific subject education. Furthermore, to some extent, the current TCM educational concept does not satisfy the actual need of TCM practitioners (Ran & Jun, 2016). Combined with Bloom’s taxonomy theory, our model may help to revise the TCM education concept.
This result also contributes to education practices. First, it helps the TCM universities or colleges establish a better education program for TCM students. This research started by identifying many ability factors related to the current education system, but finally screened out factors that turned out to be relatively unimportant; the administrators of these schools could adjust their programs accordingly. Second, the design of the current qualifications for TCM practitioners and the trainee internship are not based on the actual requirements for hospitals. The current study could shed light on the improvement of the occupational qualifications for them. Last but not least, our study can help the policy makers allocate financial support. Sun, Zheng, Wang, and Li (2018) have discussed the allocation of TCM education appropriations and projected the trend of appropriations, and this research advances that analysis. With a better understanding of the competency of TCM practitioners, educational spending could better guide TCM development in China.
There were also some limitations in our research, which we would improve in future studies. First, we should make a follow-up research design and collect data on the actual career development of the subjects of our surveys after graduation. By this procedure, the external validity of this study would be further confirmed. Second, we could develop a supervisor-rated version of this evaluation tool. Due to the goal of contributing to TCM education, a supervisor-rated version would be a better evaluation and assessment of education quality, rather than self-rated scale.
In addition, our findings only applied to the work setting of hospitals in mainland China. Considering that TCM practitioners outside China might mainly work in a different work setting (e.g., in North America, most TCM practitioners work at clinics), their competencies might be different. Also, some TCM practitioners in mainland China are trained personally without formal higher education and usually work at clinics (they can be qualified as a doctor through special government programs); their competencies might be different, too. This might be a concern of the generalization of our research. Thus, we would like to collect data from these special populations in the future. This would help us to apply our findings to TCM education globally.
To conclude, the current study identified core competencies for TCM practitioners and operationalized it as an evaluation tool for TCM students at universities and medical schools in mainland China. Our work could contribute to TCM education in China and may shed light on TCM students’ career development.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Educational Science Planning Program of Zhejiang Province, P.R. China (2019SCG137).