
Abstract
To evaluate the health information literacy (HIL) level and influencing factors among digital immigrants in rural China and to investigate their obstacles of online health information seeking. Cross-sectional study. Digital immigrants aged 45 to 65 in rural China. Self-assessment questionnaires and a semi-structured interview were developed to measure HIL among 1,132 participants. Nonparametric tests and multiple linear regression were employed to explain the influencing factors. The HIL level of digital immigrants is low. Age, education level, and experience of Internet use impacted their HIL. Digital immigrants primarily accessed the Internet via mobile terminals, but their poor information skills, their lack of HIL education, and the low readability of online health information are major barriers of online health information seeking. Although respondents recognized the positive effects of health-related information on health promotion, their abilities to seek, evaluate, and apply health information were weak. The government should incorporate HIL into the national health literacy promotion program and strengthen legislative supervision of online health information.
Introduction
Digital immigrants are people who were not born in the age of digital technology popularization and were not introduced to digital technology tools early in life (Diane & Leaunda, 2010). Digital immigrants were required to learn information technology at a specific stage of adulthood (Wang & Myers, 2013) to master the Internet and to integrate into the modern information society (Manafo & Wong, 2012). Social informatization in China started in the mid-1980s. Over the past three decades, the rapid development of information technology has created a relatively clear age boundary between digital natives and digital immigrants in China. Meanwhile, due to social, economic, educational, and other historical reasons, digital immigrants who were kept away from digital culture still exist in China. In general, the older generations tended to escape rather than integrate into the digital age when confronted with the development of information technology. Some scholars have defined this group as “digital refugees” and stipulated age groups for digital immigrants (those born from the 1960s to the 1970s) and digital refugees (those born in the 1950s and before) according to the actual social development situation in China (Yuan & Tang, 2015). The last generation of digital immigrants in China was born in the early 1970s and is currently middle-aged. With the occurrence of health problems and the demands of health information, information literacy becomes an important factor influencing physical health (Zhang & Du, 2010).
Due to differences in age, living habits, and knowledge backgrounds, obvious gaps between digital immigrants and digital natives regarding health information perception, application, motivation, technical ability, and information literacy have been discovered. Some European and American countries have performed in-depth studies on the health information literacy (HIL) of digital immigrants. Tatjana et al. (2016) investigated 354 computer users aged 66 to 89 years living in Belgrade, evaluating their online HIL and assessing factors associated with computer use in this population. The results indicated that the frequencies of computer and Internet use among older adults in Belgrade were similar to those of other populations and that the predictors of increased computer use were lower age, fewer household members, more education, higher income, and fewer comorbidities. Daniela, Marlene, Andreas, and David (2017) analyzed the sociodemographic data and online health information–seeking behaviors of a sample of 562 respondents (mean age 37 ± 15 years, 46% were digital immigrants). This study found that most respondents (79%) used the Internet to seek health information, making it the most commonly used source of health information, even more prevalent than doctors. Kristina, Stefan, Raimo, and Maija-Leena (2012) administered self-assessment questionnaires to 281 elderly people aged 65 to 79 years in Finland and investigated the conditions of their HIL. The results demonstrated that self-rated HIL was associated with an individual’s interest in health information and health information–seeking behavior. Elderly people with low education levels, poor health, and little interest in health information were less able to access and use health information. In addition, research on clinical applications of health information for middle-aged and elderly residents (Thomas et al., 2013), health information behaviors (Daniela et al., 2017; Hartzler et al., 2018; Wang et al., 2016), and health information quality assessment methods (Ashley, Amber, & Thomas, 2011; Elmer, Dawn, Muhammad, & Funda, 2005; Parsley, 2017) has shown that the HIL levels of digital immigrants have proven to be of great significance for improving their health statuses and enhancing the equity of health service utilization.
The health literacy monitoring data of Chinese residents published in 2016 (National Health Commission of the People’s Republic of China, 2017) indicated that 19.13% of Chinese residents had basic HIL (95% confidence interval [CI] = [18.64%, 19.59%]), which showed no significant improvement over the 18.16% (95% CI = [17.81%, 18.52%]) observed in 2012 (National Health Commission of the People’s Republic of China, 2014). The HIL of middle-aged residents more than 40 years old was significantly lower than the average level. However, after searching the Chinese National Knowledge Infrastructure (CNKI) and Medline databases, only a few studies on the HIL of Chinese digital immigrants were found. In 2015, a study from Renmin University of China (Zhou, Song, & Zhang, 2015) analyzed the National Action Plan for Improving Health Literacy in the United States and suggested that the relationship between HIL and health information dissemination and utilization should be recognized from a strategic perspective in China. Li and Zhao (2016) investigated the current utilization of smartphone applications among Chinese digital immigrants in the new media environment and concluded that media literacy was an important factor influencing access to information among digital immigrants. In addition, a study (Yuan & Tang, 2015) applied grounded theory and a qualitative analysis software program (NVivo) to analyze the health information motivation types, motivation intensities, and influencing factors of 20 digital immigrants aged 35 to 50 years. The results indicated that digital immigrants exhibited a strong search willingness in the process of health information searching.
Previous studies often focused on certain aspects (skills, seeking, motivation, etc.) related to health information in populations with similar backgrounds; however, cross-sectional surveys concerning the HIL of digital immigrants in China are rare. The purposes of the present study were to (a) evaluate the HIL level and influencing factors among digital immigrants in rural China and (b) to investigate their obstacles of online health information seeking.
Method
Survey Design
This was a cross-sectional study conducted from July to October 2017. The study population was composed of adult residents from Anhui Province, China. Based on the economic development level, eight rural communities were selected as sampling areas. Selective quota sampling was applied to attain equal subsamples in terms of gender and age. A respondent who fit into one of the subsamples and indicated his or her willingness to participate in the study was asked to complete an HIL self-assessment questionnaire. Approximately 150 questionnaires were administered in each community. A total of 1,200 questionnaires were distributed.
The following inclusion criteria were applied: (a) residents living in a rural community more than 6 months consecutively, (b) aged 45 to 65 years old, and (c) having basic reading and writing skills. The following exclusion criteria were applied: (a) mentally or physically unsuitable to participate in the survey and (b) missing questionnaire responses.
The sociodemographic factors in the present survey included gender, age, education level, occupation, annual household income, and access to the Internet. Referencing the “Occupation Classification Standards” of the National Bureau of Statistics of China, we categorized occupations as follows: offices and public institutions, technical work, commercial and services, and agriculture.
Instrument
We used a modified Everyday Health Information Literacy–10 (EHIL-10) instrument in the present study. The EHIL-10 was initially developed by Dr Raimo, Stefan, and Kristina (2011) to distinguish among different levels of HIL. For the purposes of the present study, we added four items to the original EHIL-10, including one that was used to measure an individual’s ability to express health information, as information expression is the basis for information literacy (Cilliers, Viljoen, & Chinyamurindi, 2018; Elizabeth, 2009). Another item was used to measure willingness to share health information because health information acquisition is reportedly a team task (Rajani et al., 2013). Two items were used to measure the ability to seek and evaluate health information via television, as television is an important medium of public access to information in developing countries, such as China. The modified self-assessment questionnaire uses a 5-item Likert-type scale. Q1, Q2, Q3, Q6, Q7, Q9, Add. Q2, Add. Q3, and Add. Q4 are scored from 1 (strongly disagree) to 5 (strongly agree), whereas Q4, Q5, Q8, Q10, and Add. Q1 are scored from 1 to 5 in a reverse order (see Table 3).
In addition, to better understand the barriers to accessing online health information among digital immigrants, we designed a semi-structured interview and recorded the entire interview process with a digital voice recorder.
Data Analyses
All statistical analyses were performed using SPSS for Windows version 17.0 (IBM, Chicago, IL, USA). Cronbach’s alpha coefficients were calculated to evaluate the internal consistency and reliability of the questionnaire. Exploratory factor analysis (EFA) and Pearson correlation analysis were applied to assess construct validity. Kruskal–Wallis H tests and multivariate linear regression models were employed to explore the effects of demographic factors on HIL. Statistical significance was set to p < .05.
For qualitative analyses, interviews were transcribed. The contents of the interview were classified, and the frequency of each item was counted. Two investigators reviewed the recordings and provided a brief summary of each item.
Ethical Approval
The study was approved by the Ethics Committee of the Bengbu Medical College (reference number 2017054). The survey was completed anonymously. All potential respondents were contacted personally and thoroughly informed about the aim of the study, data processing, and the use of the data. Participation was voluntary, and participants could refuse to participate.
Results
Sample Description
Among 1,200 questionnaires, 1,132 valid questionnaires were collected, for a response rate of 94.33%. The average age of the respondents was 56.44 ± 7.92 years old. Males (48.58%) and females (51.41%) participated roughly equally. The main occupation was agriculture (51.06%), the education level was mainly senior school or below (94.96%), and the annual household income was mainly 40,001 to 100,000 CNY (79.24%). A total of 365 respondents (32.24%) had no experience with Internet use, and another 560 respondents (49.47%) had more than 3 years of experience with Internet use. The respondents’ demographics are summarized in Table 1.
Sociodemographics of Respondents (N = 1,132).
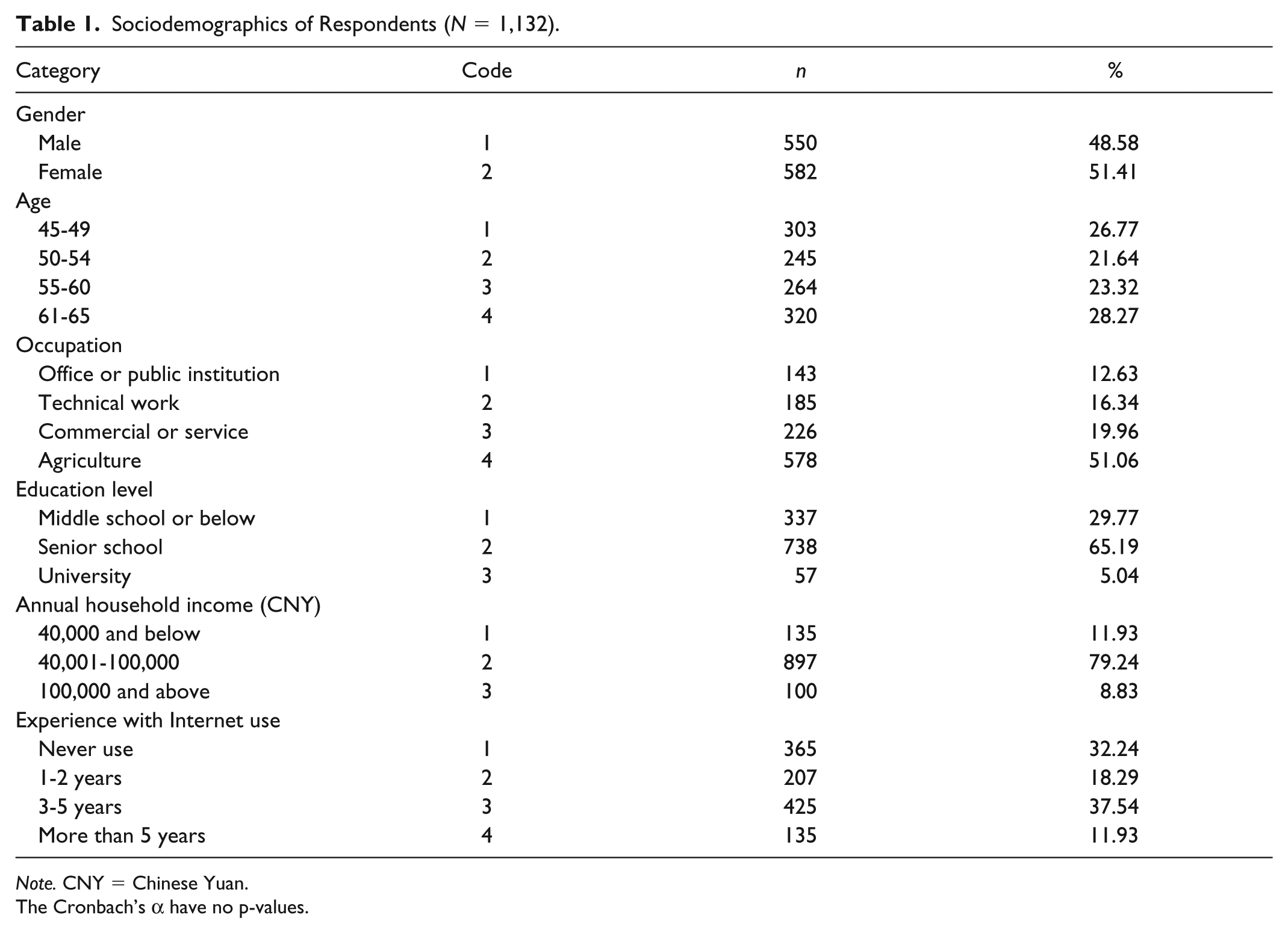
Note. CNY = Chinese Yuan.
The Cronbach’s α have no p-values.
Instrument Reliability and Validity Analysis
To test the validity of the modified HIL questionnaire, EFA (KMO = 0.793, Bartlett’s test of sphericity: approx. chi-square = 2,057.864, df = 81, p < .001; extraction method: principal component analysis; rotation method: varimax factor rotation) was conducted, and four components were extracted, which accounted for 69.83% of the total variance.
The analyses extracted four factors: Factor I (Q2, Q4, Q5, and Add. Q1), which described health information–seeking ability; Factor II (Q6, Q7, Q8, Q10, and Add. Q2), which described health information evaluation ability; Factor III (Q1, Q3, and Add. Q3), which described health information consciousness; and Factor IV (Q9 and Add. Q4), which described health information application ability. Correlation analyses of the four extracted factors showed that Factors I and II (Pearson R = .437, p < .001) and Factors III and IV (Pearson R = .395, p < .001) had strong correlations. In contrast, Factors I and III (Pearson R = .265, p < .001), Factors I and IV (Pearson R = .292, p < .001), Factors II and IV (Pearson R = .240, p < .001), and Factors II and III (Pearson R = .226, p < .001) had moderate correlations. The results of the EFA and correlation analysis indicated that the questionnaire structure had good validity.
The Cronbach’s alpha values of the four subscales ranged from .511 to .739 (see Table 2) in the present study. Considering the limited number of items in each subscale, these low Cronbach’s alpha values were acceptable and indicated moderate internal consistency.
Self-Rated Health Information Literacy Results.

Note. HMS = hundred-mark system.
The Cronbach’s α have no p-values.
HIL Assessment
The HIL self-assessment results of the digital immigrants are shown in Table 2. To better compare the results of the survey, we normalized the HIL scores according to the hundred-mark system (HMS). The average HIL score among digital immigrants was 45.51 (HMS: 65.01). Among the four dimensions, health information consciousness received the highest score (HMS: 78.33), and health information seeking received the lowest (HMS: 58.70). Although more than 37.6% of respondents demonstrated relatively high (HMS >= 80) health information consciousness, the percentages of respondents with an HMS above 80 in health information seeking, evaluation, and application were 2.73%, 6.22%, and 3.57%, respectively. The proportion of respondents with HIL HMS scores above 80 points was only 5.7%. Overall, digital immigrants’ HIL was not a source of optimism.
Demographic Differences in HIL
The health information seeking (χ2 = 163.57, p < .001) and health information evaluation (χ2 = 98.90, p < .001) levels of the younger respondents were stronger than those of the elderly. Respondents with university educations scored the highest in the three dimensions of health information seeking, health information evaluation, and health information application. The lowest scores in all four dimensions were obtained by respondents with education levels of middle school or lower (χ2 = 132.34, p < .001). Respondents who engaged in professional and technical work had higher scores for health information seeking (χ2 = 58.78, p < .01) and application (χ2 = 49.50, p < .01) compared with those who engaged in agricultural work. In addition, respondents who had rich experience with Internet use demonstrated stronger health information seeking (χ2 = 117.50, p < .01), evaluation (χ2 = 69.73, p < .01), and application (χ2 = 128.46, p < .001) abilities. There were no significant differences in HIL among respondents with different annual household incomes.
The results of the multiple linear regression analysis are shown in Table 3. The main influencing factors of digital immigrants’ HIL were age, education level, and experience with Internet use (R2 = .155, F = 13.772, p < .001). Education level was the main factor influencing health information consciousness (R2 = .097, F = 7.119, p = .02). Health information seeking (R2 = .304, F=37.738, p < .001) and evaluation (R2 = .187, F = 18.590, p < .001) were similar; significant influences could be found for age, education, and experience with Internet use. Gender, education level, annual household income, and experience with Internet use were influencing factors for health information application (R2 = .204, F = 23.475, p < .001).
Influence Factor Analysis of HIL in Different Demographic Subgroups (β).
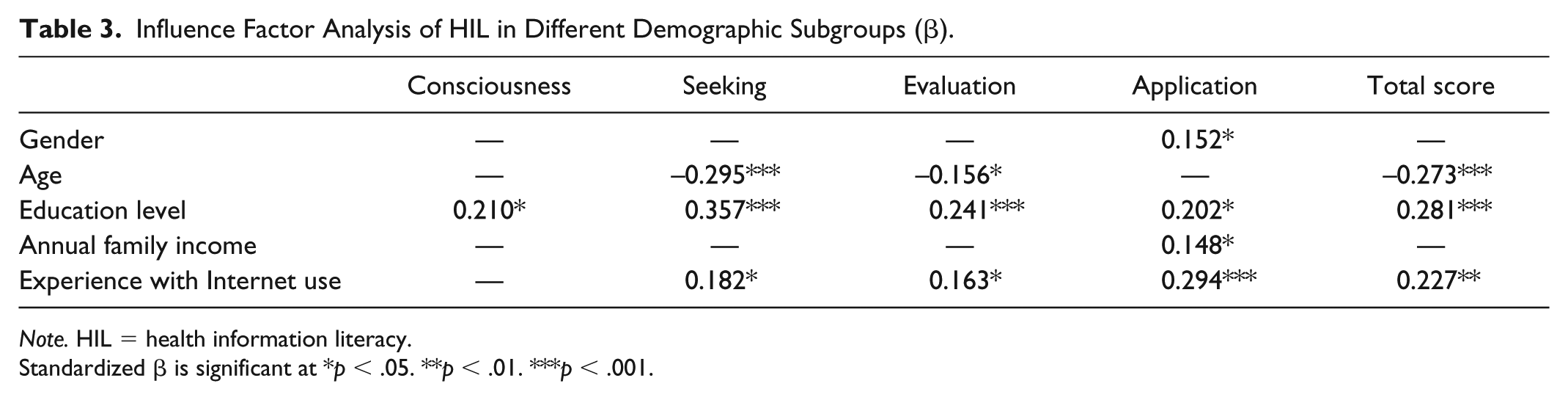
Note. HIL = health information literacy.
Standardized β is significant at *p < .05. **p < .01. ***p < .001.
Obstacles to Seeking Health Information Online
Semi-structured interviews were conducted based on equal distance sampling (d = 20) with 38 of the 767 digital immigrants who had experience with Internet use (see Table 4). The number of smart terminal (smartphone, tablet, etc.) users was much larger than the number of computer users. BaiduTM was the most popular online search engine. Most digital immigrants (30/38) encountered difficulties in understanding online health information, and all respondents claimed that they had never stored and did not know how to store online health information. More than half of digital immigrants responded that they “do not know how to evaluate the quality of health-related websites and articles.” Moreover, the respondents suggested that the government should focus on strengthening HIL education and increasing supervision and control over online health information distribution.
Results of Semi-Structured Interviews of 38 Digital Immigrants.

Discussion
In the present study, we described the effects of sociodemographic factors on the HIL of digital immigrants in rural China. The results were similar to the findings of previous studies (Alexander & Deursen, 2012; Baker, Williams, Parker, Gazmararian, & Nurss, 1999). Respondents with high education levels and rich experience with Internet access were more confident in evaluating health information quality and seeking and applying health information. Compared with males, females were more willing to share and apply health information to improve health, which agrees with the findings for digital natives (Yuan & Tang, 2015). Compared with older digital immigrants, younger immigrants showed greater abilities to seek and evaluate health information. In addition, rural digital immigrants appeared to attach less importance to “where to find health information.” This finding was different from those of a previous study on urban digital immigrants. A possible explanation is that the health literacy level of urban residents is generally higher than that of rural residents in China (Nie, Li, & Li, 2014).
Occupation was another important factor that influenced the HIL of the digital immigrants. Although occupation was not suited for multivariate analysis, univariate analysis showed significant discrepancies in HIL, health information seeking, and application. In the present study, respondents with office and public institution jobs or technical jobs had higher HIL levels than those holding commercial and agricultural jobs. This pattern may have been caused by differences in education levels. People with office and public institution jobs or technical jobs usually attain higher educational levels than those with commercial and agricultural jobs in China.
The current survey finds that smart terminals (mainly smartphones) have become the primary tools by which digital immigrants access the Internet, which is inconsistent with our assumption. In China, computers became popular in the mid-1990s, and the use of smartphones began in the past decade (National Internet Network Information Centre, People’s Republic of China, 2018). Low prices, portability, and multifunctionality are the main reasons for the widespread adoption of smartphones. Support for handwriting and voice input greatly facilitates access for people with low education levels or disabilities. In addition, the current study also proved that Baidu TM is the most widely used search engine in mainland China. The main basis of screening health information for digital immigrants is still the search results ranking, which reminds people of the “Wei Zexi” incident (Wikipedia, 2017). Therefore, strengthening the monitoring of information pulled by search engines is still an important mission for the Chinese government.
The outlook for the abilities to comprehend and save online health information is not positive for digital immigrants, and the difficulty of understanding medical terms remains the biggest obstacle. Certainly, a few health websites have realized this problem in China, such as 39 HealthTM Network (http://jbk.39.net/), which provides hyperlinks to detailed explanations of medical terms to help users better understand health information. Although all 38 digital immigrants said that they had not and would never collect or save a web page, difficulties in mastering the relevant skills were not indicated. After the interview, we attempted to guide some interviewees using a mobile browser to collect web pages, finding that the interviewees could grasp the skill after one operation. Unfortunately, to our knowledge, no work concerning HIL education has been published in mainland China.
In addition, the results of the interviews suggest that online health information providers should provide users with better application experiences in the fields of multimedia material, constructing user-friendly interfaces, regulating health information sources, and guaranteeing the quality of health information. In terms of government action, although HIL was included in the national health literacy survey for the first time in 2012, and the Technical Manual for the Generation and Dissemination of Health Science Information (Media Edition) and Recommendations for Public Recognition and Utilization of Online Health information (2017 Edition) were published in 2017, community education on HIL is still an important task and requires more substantive effort from the Chinese government (Zhang, Chen, & Xia, 2016).
The present study has some limitations. First, barriers to access to online health information are not only affected by personal HIL but are also related to the development level of community informatization, social and cultural environments, ethnic and religious beliefs, and other factors. The survey in this study was performed in eight rural communities of a single province of China, which could have resulted in selection bias and could affect the validity of the study. Second, the development of individual HIL is complex. To our knowledge, special HIL assessment tools for Chinese digital immigrants are lacking, making the evaluation of criterion validity difficult. Although 14 items were included in the current study, this strategy may have been insufficient to guarantee that the assessment reflected the digital immigrants’ HIL. Third, this study used a self-assessment questionnaire and semi-structured interview, but it did not provide a manipulation-based skill evaluation method. Therefore, the results should be regarded as preliminary and interpreted with caution. Despite these limitations, this study is still valuable for understanding digital immigrants’ HIL in rural China and their ideas about online health information.
Conclusion
Currently, the overall situation regarding HIL among rural digital immigrants in China is not positive. Although they can recognize the positive role of health-related information in health promotion, their abilities to seek, evaluate, and apply health information remain weak. Meanwhile, poor information skills, lack of HIL education, and low readability of online health information are major barriers for digital immigrants to seek health information via the Internet.
The Chinese government should incorporate information literacy education into the national health literacy promotion program as soon as possible. Meanwhile, strengthening legislative supervision of the information pulled by Internet search engines and enhancing the monitoring of online health information quality are necessary to improve the environment for the dissemination of health information on the Internet.
Footnotes
Acknowledgements
The author wishes to thank Raimo Niemela (University of Oulu, Finland) for his assistance in assessment tool compilation. We thank American Journal Experts (AJE) for English language editing.
Author’s Note
All authors contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the National Planning Office of Philosophy and Social Science of the People’s Republic of China (grant no.17BGL262).