
Abstract
Internet health information is used by patients for health care decision making. Research indicates this information is not necessarily disclosed in interactions with health professionals. This study investigated primary health care nurses’ engagement with patient online health information use along with the respondents’ disclosure of online sources to their personal health care provider. A questionnaire was posted to a random sample of 1,000 New Zealand nurses with 630 responses. Half the respondents assessed patients’ online use (n = 324) and had encountered patients who had wrongly interpreted information. Health information quality evaluation activities with patients indicated the need for nursing information literacy skills. A majority of respondents (71%, n = 443) used online sources for personal health information needs; 36.3% (n = 155) of the respondents using online sources did not tell their personal health care provider about information obtained. This study identifies that there are gaps in supporting patient use but more nursing engagement with online sources when compared with earlier studies.
Introduction
Internet health information is an important education resource commonly sought by patients to support their health care decision making. An online survey of 12,262 respondents from 12 countries found that three fifths used online health information and 46% of this group used the information to self-diagnose health problems (McDaid & Park, 2011). Internet use in New Zealand is almost universally accessed by under 40-year-olds and is cited as the most valued medium for information (Gibson, Miller, Smith, Bell, & Crothers, 2013).
People independently seeking out online health information are motivated to develop their knowledge about health conditions and possibly adopt new lifestyle patterns (Fox, 2007). Supporting the development of confident decision-making skills is an important aspect of health education to strengthen beliefs about self-efficacy (Coleman & Newton, 2005). Self-efficacy is an aspect of the social learning theory developed by Bandura (1986) and is defined as “beliefs in one’s capabilities to organize and execute the courses of action required to produce certain attainments” (Bandura, 1997, p. 3).
The Internet enables information access to support decision making but the medium has “noisy” characteristics. Noise in a communication sense is defined as interference with message exchange and common understandings of the message (Bartol, Tein, Matthews, Sharma, & Scott-Ladd, 2011). DeVito (2012) identifies four noise types: physical, physiological, psychological, and semantic. These noise types can interfere with accessing and understanding online health information. Physical noise is external interference such as poor computer or mobile device screen visibility as a consequence of small font or popup advertisements. Physiological barriers include poor vision and cognitive issues. Psychological noise occurs when there is mental interference to the message being understood such as an emotional response to particular information or pre-existing biases. Semantic barriers are produced through complex and specific terminology and the lack of shared meaning between the sender and receiver.
External and intrinsic barriers to health information message reception can be mitigated with health literacy skills. Health literacy is underpinned by knowledge and skills in accessing, understanding, discerning, and applying information to make effective health management decisions and to seek appropriate health care (Keleher & Hagger, 2007). The need for online health literacy skills is demonstrated in a study testing online information literacy by van Deursen and van Dijk (2011). In this study only 35% of the participants were able to use the information they found for beneficial decision making. Education was the most important contributor to strategic Internet use by the study participants.
Nurses have a role to play in developing patient health literacy skills to support the efficacious use of online health information. Nurses’ education activities require an understanding of resources available, including online information, which will support people’s knowledgeable engagement in care decisions. There is the need to enquire about the information patients are independently sourcing to build skills and efficacy, as well as developing their evaluation skills in judging the quality of the information. Teaching about information evaluation provides the opportunity to model assessment strategies to ascertain the quality and applicability of online information. Along with self-efficacy, modeling is an important concept in social learning theory, the central tenant being that learning is stimulated through observing behaviors and that “coded information serves as a guide for action” in the future (Bandura, 1986, p. 47).
This study is located in the primary health care (PHC) setting where increasingly long-term conditions are being managed. The PHC sector is the key site for patient education as the first point of contact with the health system (King, 2001) along with providing the majority of ongoing care for people who have chronic conditions (Caughey, Vitry, Gilbert, & Roughead, 2008). In New Zealand, PHC nurses contribute to structured education for people with chronic illnesses with assessment, care planning, and regular monitoring activities (Ashworth & Thompson, 2011; Henty & Dickinson, 2007). Teaching patients how to productively use online health information is an opportunity to develop reciprocal knowledge-based relationships as reported in a study of oncology nurses’ experiences of patients’ online information use (Dickerson, Boehmke, Ogle, & Brown, 2005). On one hand nurses can alert patients to critical information assessment techniques, and on the other, patients can increase nurses’ understanding of the information they have independently sourced and found as being meaningful and useful in their illness diagnosis and management.
Background
Patients use the Internet to clarify and extend the information provided by doctors and other health professional (Bowes, Stevenson, Ahluwalia, & Murray, 2012; Kivits, 2006; Knapp et al., 2011; Pletneva, Cruchet, Simonet, Kajiwara, & Boyer, 2011) and value the anonymity and accessibility attributes of Internet searches (Horgan & Sweeney, 2010).
Evidence over the last decade shows that many nurses have not yet made the transition to acknowledging patients’ independent information-seeking activities and incorporating online health information in patient education. A survey of 1,170 Spanish nurses found 72.8% felt online material was relevant to very relevant to patients and 73% had discussed online information with at least some patients, but 54.4% would not recommend online information to patients (Lupiáñez-Villanueva, Hardey, Torrent, & Ficapal, 2011). The issues around nursing engagement with online information are longstanding as illustrated by an older Scottish survey of 130 general practice nurses where 73% of the nurses accessed the Internet but only 29% would refer patients to Internet information (Wilson, 1999).
New Zealand studies have also traced broader nursing engagement with a notable feature being the minority of respondents who assessed patients’ use of online information (37% of postgraduate nursing respondents [Gilmour, Scott, & Huntington, 2008], 11% of undergraduate nursing respondents [Scott, Gilmour, & Felden, 2008], and 24.4% of nursing respondents working in medical wards [Gilmour, Huntington, Broadbent, Strong, & Hawkins, 2012]). These studies also consistently found that a very small minority of the nurses in the study settings worked to develop patients’ information evaluation skills.
There is research interest on the effect of disclosure of independently accessed Internet information on relationships between patients and health professionals. Patients’ reasons for discussing health information during medical consultations include wishing to make the best possible use of the time, along with seeking clarification and reassurance (Bowes et al., 2012). However, some patients, including those who are health professionals, choose not to discuss the information they found with their doctor: 47% of patients and 38% of health professional patients in a Health on the Net survey of 524 participants (Pletneva et al., 2011) and 31% of nurse respondents working in medical wards (Gilmour et al., 2012).
Imes, Bylund, Sabee, Routsong, and Sanford (2008) surveyed 714 Americans about constraining factors in discussing online health information with health care providers. Important factors were fear of disrupted relationships with the provider, intruding upon the health professionals’ authority, worries about being perceived in a negative way for bringing up information, and concerns about the health care professional dismissing the information as invalid. McMullan (2006) argues that health professionals vary in their responses to health information users. Threatened health professionals use their positioning as expert to guide the consultation, in contrast patient-centered practitioners work collaboratively with clients. McMullan also suggested there is a group of health professionals who guide patients to useful sites. The validity of this latter approach is supported by survey findings where 80% of patients wanted health professionals to provide trustworthy online information (Pletneva et al., 2011).
Patients’ concerns about locating trustworthy information are supported by the large body of published work focused on the quality of online health information. In a systematic review of research assessing the quality of online material, 70% of the studies suggested there were quality issues (Eysenbach, Powell, Kuss, & Sa, 2002). More recent empirical work shows that quality concerns are an enduring theme in the literature. Recent studies report information quality concerns with websites on health topics such as oncology information (Lawrentschuk et al., 2012), online infant sleep recommendations (Chung, Oden, Joyner, Sims, & Moon, 2012), and common pediatric issues (Scullard, Peacock, & Davies, 2010). A study of the compliance of websites with asthma education guidelines found that only 8.8% met all the guideline criteria with the implication that nurses needed to be knowledgeable about the most accurate sites so they could be recommended to their patients (Meadows-Oliver & Banasiak, 2010).
Primary health nurses who are working in the first point of health contact need to be alert for opportunities to strengthen clients’ beliefs about self-efficacy and develop information evaluation skills. Research findings highlight a range of issues with evidence of (a) limited nursing engagement with online health information sources in patient education, (b) substantial patient use of online sources as a backup to health professional education, (c) patient perceived barriers to the communication of information sources with health professionals, and (d) quality concerns with some online material.
Study Aims
A premise of this research, informed by the issues raised in the literature review, is that patients may not volunteer to health professionals their information sources for a variety of reasons. There is also the possibility that the information sources, or patients’ interpretations of information, may be flawed in nature. The aims of this research were to establish PHC nurses’ assessment of patient online health information use and their support with patient evaluation of online education material, and explore PHC nurse’s reasons for non-disclosure of information sources to their personal health care providers. Personal health care providers are defined for the purposes of this study as health professionals who provide personal health care to the respondents and their families.
Methods
The study used a cross sectional survey research design. A cross sectional study systematically collects quantifiable data from the population of interest at one point in time (Bryman, 2012). The data were collected from a random selection of PHC nurses using a mailed questionnaire. The findings reported in this study on nurses’ engagement with patient’s online use were from one section of the questionnaire which also included sections on nurses’ online access and heart failure education resources and activities. The survey questions elicited predominately quantifiable data through the use of fixed response items. There were two open-ended items generating textual data. The textual data were analyzed qualitatively using a content analysis approach. Qualitative content analysis involves the categorization of textual data through the identification of patterns and themes (Julien, 2008).
Study Sample
Sample inclusion criteria were currently working in PHC settings and selection of the Nursing Council of New Zealand categories “Primary health care” and “Practice nursing” at the time of annual practicing certificate renewal. Exclusion criteria were not currently working in the PHC sector and not agreeing to be contacted for research purposes. There were 4,673 practicing nurses in the relevant categories at the time of the survey and 2,780 of the group had agreed to be contacted for research purposes. The minimum survey sample size was calculated as 197 with an 80% probability of getting a statistically significant result with a population correlation effect size of .2, based on an alpha level of .05. A sample of 1,000 nurses was randomly selected from the Nursing Council of New Zealand data base.
Instrumentation
The study questions were based on a questionnaire used previously with nurses working in medical wards (Gilmour et al., 2012) and informed by a review of research literature. The questionnaire was further refined for the PHC sector but changes from the questionnaire used in the earlier study (Gilmour et al., 2012) were minimal. New questions were developed about the frequency that respondents’ asked clients if they accessed the Internet for health information, and their awareness of patients’ misconceptions because of incorrect Internet health information. The questionnaire was piloted with five PHC nurses to check for face validity along with questionnaire flow, length, and clarity.
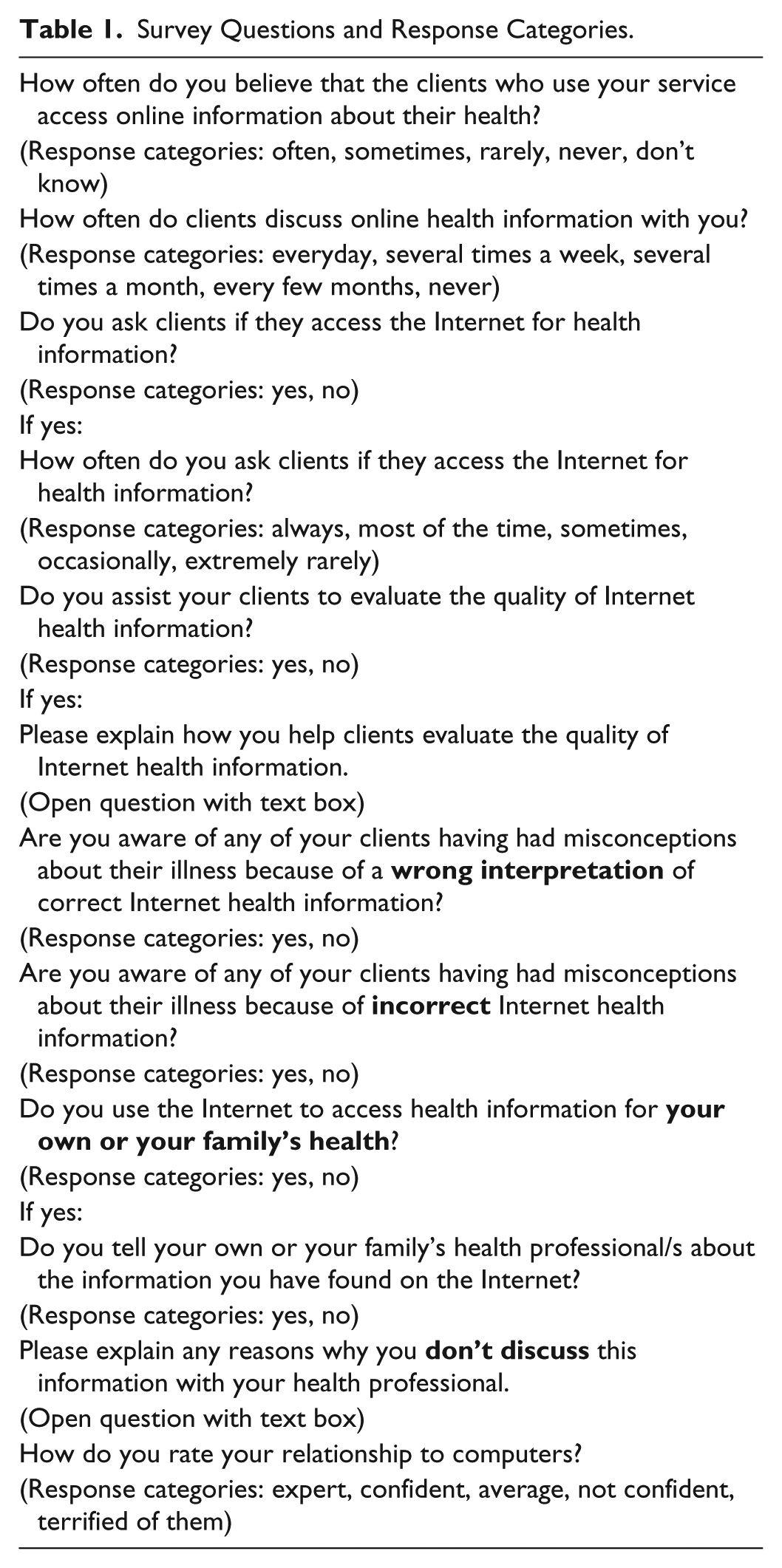
The questionnaire had 12 items (Table 1). Four questions collected ordinal data; the topics were respondents’ perceptions of clients’ online information use, frequency of client discussion about online information, frequency of assessment of patient use, and confidence with computers. Six questions collected categorical data; topics included assessment of patient use, awareness of patients’ misconceptions, and respondents’ use for personal health care. Two open-ended questions generated qualitative data; respondents were asked how they worked with patients to develop information evaluation skills and why respondents did not discuss information found on the Internet with their personal health care provider where applicable. In addition, demographic characteristics were collected on age, gender, ethnicity, and nursing qualifications.
Survey Questions and Response Categories.
Data Collection
The 1,000 questionnaires were mailed out in April 2010. There was a follow up 2 weeks after the first mail out with a thank you and brief reminder, and a second mail out after 4 weeks to those who had not replied with a replacement questionnaire. Data collection was carried out from April until June 2010.
Ethical Considerations
The University Human Ethics Committee (Application 09/68) approved the study. An information sheet was posted with the questionnaire covering the survey aim and a statement that the respondents were anonymous to the researchers. An administrator separate to the research team managed the mail out and the follow up processes.
Analysis
The questions generated categorical, ordinal, and qualitative data. SPSS 20.0 (IBM SPSS Inc., Chicago, IL, USA) for Windows was used for the statistical analysis. Summary statistics are presented along with a categorical data test of proportions (Pearson chi-square), the Mann–Whitney test for ordinal data group differences, and a non-parametric data correlations test (Spearman’s rank correlation co-efficient, [rs]). The respondent total number varies according to the topic as answering questions was voluntary. Nurses who did not work with patients who accessed online health information (n = 12) are not included in the analysis of relevant topic areas.
The qualitative data were analyzed using an inductive content analysis approach whereby interpretation was informed by the respondents’ textual data rather than a pre-existing theoretical viewpoint (Julien, 2008). The analytic process began with a close reading of the texts followed by the development of codes, where extracts of text are named, and then the codes were grouped into categories. The qualitative data were initially coded and grouped into seven categories for each open-ended question by one researcher, the codes and categories were then confirmed by a second researcher. The textual data categories were also quantified with a count of the comments by categories (Bryman, 2012). Quotes are included in the findings to illustrate and validate the choice of categories.
Results
Response Rate
The final response rate was 65.5% (630 valid responses); 39 nurses informed us they were no longer eligible as they were not working in the PHC sector. The sample statistical power is calculated as being a 99% probability of getting a statistically significant result with a population correlation effect size of .2, based on an alpha level of .05.
Sample Description
Almost all respondents were female (99%, n = 620), the mean age was 49.45 years with ages ranging from 23 to 70 (Table 2). The major ethnic groups were New Zealand European (80.7%, n = 501) and Māori (9.2%, n = 57). The sample differs from the overall New Zealand registered nurse workforce, 92% of the New Zealand overall nursing workforce is female, the average age of the workforce is 45.6 years, 68% are New Zealand European, and Māori are 7% of the workforce (Nursing Council of New Zealand, 2011). However, there is a close match with the PHC workforce where 97% are female, 76% New Zealand European/Pakeha, and 9.8% are Māori (Nursing Council of New Zealand, 2011).
Sample Demographic Characteristics.

Assessing Patient Use of Online Health Information
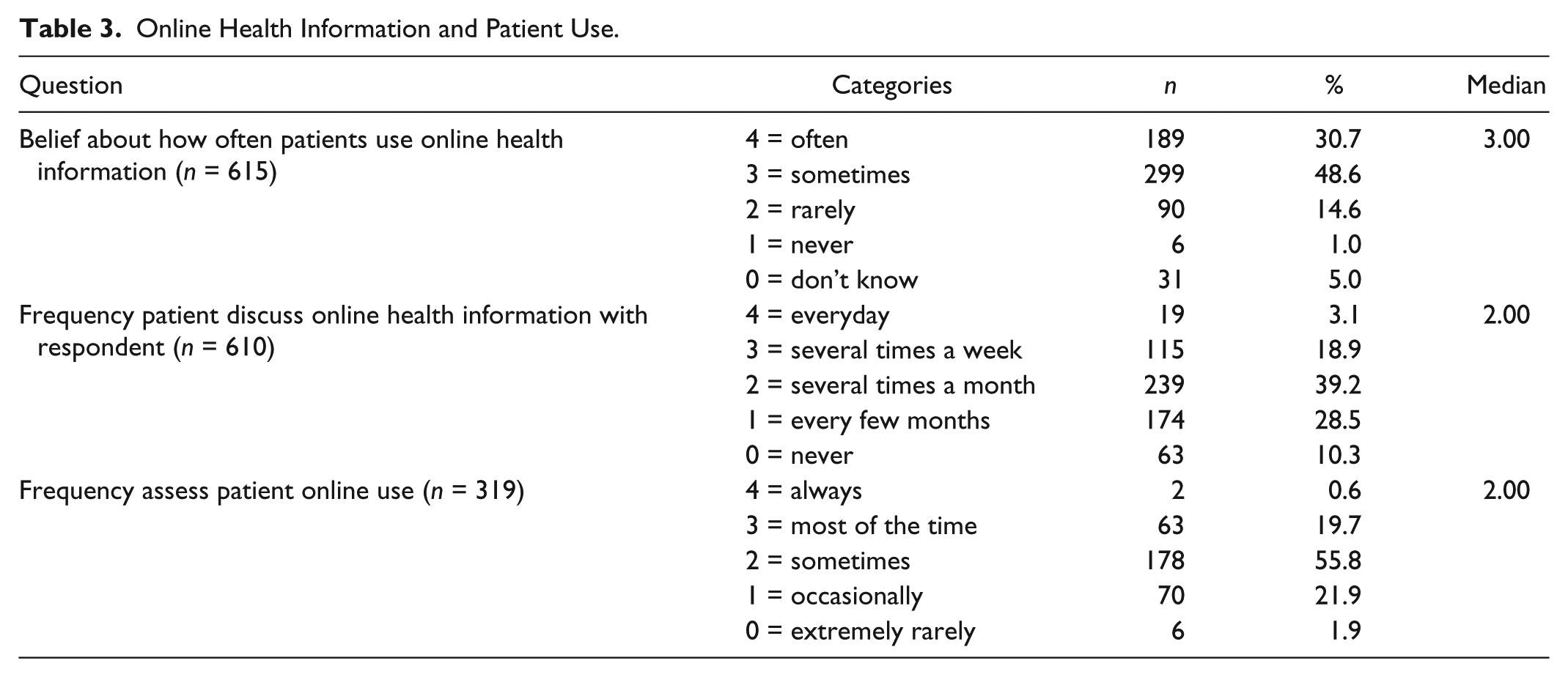
Most respondents (79.3%, n = 488) believed that patients used online health information at least sometimes and 61.2% (n = 373) encountered patients requesting to discuss this information with them several times a month or more (Table 3). Half the respondents (53%, n = 314) had encountered patients wrongly interpreting Internet health information and 44.4% (n = 266) were aware of patients’ misconceptions due to incorrect information. About half the group (52.8%, n = 324) asked their patients if they accessed online information with 20.3% (n = 65) of this group assessing patients use most of the time. Nurses who assessed patient’s use scored significantly higher on confidence with computers (U = 39746.0, N1 = 323 [mean rank 327.95], N2 = 289 [mean rank 282.53], p < .001) compared with the non-assessing respondents answering these questions. The assessment of patients use was significantly associated with nursing qualifications, χ2(1, N = 605) = 16.408, p < .001. Two thirds (62.9%) of nurses with postgraduate qualifications assessed patients’ online use as compared with 46.1% of nurses educated to degree level or less. There was also a significant positive correlation between the frequency of asking patients if they accessed the Internet for health information and level of qualification (rs = .196, N = 315,p ≤ 0.001). Assessing patients’ use was significantly associated with awareness of patient misconceptions because of incorrect interpretations of online health information, χ2(1, N = 591) = 12.292, p < .001; 59.9% of assessing nurses were aware of incorrect interpretations compared with 45.5% of non-assessing nurses.
Online Health Information and Patient Use.
The mean age difference between the group that assessed patient use (49.47 years) and the group that did not (49.38 years) was similar as was the mean nursing years of experience (25.52 years for group that assessed, 24.46 years for the group that did not).
Evaluating Information Quality
Under half of the total group (46.9%, n = 282) helped patients evaluate information quality. Comments about evaluation strategies were collated into seven categories, a small group of three respondents commented that it was too difficult to teach evaluation skills. The respondents who did assist with evaluation used various strategies (Table 4). Referral to reputable sites such as ministry and non-governmental organization sites was the most cited specific approach (n = 113) with one respondent excluding Google and Wikipedia as search possibilities.
Assisting Patients to Evaluate the Quality of Internet Health Information.

The other categories were driven by patient provided material and two different positions were discernible. One category centered on teaching patients evaluation skills with 42 responses. Respondents provided education about how to check sources and use established guidelines to assess sites and information. The other categories took a protective stance. One major response category (n = 66) centered on information evaluation from the viewpoint of the respondents’ knowledge. The information was reviewed in term of research quality and respondents’ “encouraged discussion” with patients. The other major categories were focused on respondents’ cautioning patients to be careful of online sources (n = 28) and referring the patient on to other health professionals and specialities (n = 13).
Nurses and Personal Online Information Use
The majority of respondents (71%, n = 443) used online health information for their personal needs and 36.3% (n = 155) of that group did not tell health professionals about online information they had found. The reasons for non-disclosure were varied (Table 5). The most frequently commented on category was not having a reason to discuss the information (n = 35), other related categories were confidence in the personal health care provider’s knowledge base (n = 16) and the complementary nature of the information (n = 11). Contrasting concerns were also expressed about disrupting the relationship with the health professional through volunteering information (n = 18). A respondent commented that “some doctors are not on happy to be questioned by nurses” suggesting that being a nurse in this instance complicates the relationship when more information is required from personal health care providers. Some respondents (n = 8) felt they could be judged in a negative sense as not being knowledgeable enough. There were also comments about lack of time to fully discuss the material as the “response are too complicated” and “doctor’s are too busy.” A small group had little or no opportunity for discussion because of lack of contact with a health provider.
Respondents Reasons for Not Discussing Online Health Information With Their Health Professional.

Discussion
Developing health literacy requires collaborative relationships between health professionals and patients. Enquiring about information sources is important as patients will not necessary initiate a discussion. Nearly half the respondents in this study were aware of patients’ misconceptions about information they had read, findings congruent with an earlier study in the medical ward context (Gilmour et al., 2012). Internet users can decide to discontinue medical treatment when it conflicts with information they have found (Weaver, Thompson, Weaver, & Hopkins, 2009); it is therefore prudent that health professionals are proactive in checking with patients their information sources. Patients with very limited knowledge and little access to online information can be identified and fully supported using a variety of media such as hard copy resources, visual and plain language information catering for limited health literacy, and face-to-face individual and group sessions.
The research findings showed greater engagement with patients’ online health information use in the PHC sector compared with an earlier study of medical ward nurses (Gilmour et al., 2012). More PHC nurses (61.2%) were involved in patient discussions about online information several times a month or more compared with medical ward nurses (30.7%), asked their patients if they accessed online information (52.8% compared with 24.4% of medical nurses), and helped patients evaluate its quality (46.9% compared with 24.9% of medical nurses). One possible explanatory factor is the differences in the proportion of nurses with advanced education in the two groups. More than 40% of the PHC sample had postgraduate qualifications compared with 24.2% of the medical ward sample (Gilmour et al., 2012). There was a significant association between postgraduate qualifications and assessment of patient online use in both studies.
Evidence suggests postgraduate study to master’s level does influence practice approaches. A systematic literature review of the relationship of master’s-level education with patient care identified themes of “increased confidence and self-esteem; enhanced communication; personal and professional growth; knowledge and application of theory to practise; and analytical thinking and decision making” (Cotterill-Walker, 2012, p. 57). The knowledge-base and critical appraisal skills gained through in-depth scholarly work support efficient access and evaluation of relevant information sources. Opening up conversations about knowledge sources also demands careful communication so as not to alienate patients who may otherwise feel examined about their information sources.
The assessment and evaluation differences between PHC and medical wards can also be attributed to work organization and relationship with patients. In the PHC setting, there is the opportunity to work with patients intensively over a period of time. In contrast, in a medical ward environment, many nurses may care for a patient during short hospitals stays: a New Zealand study finding that on average medical ward stay, patients were cared by 10.7 nurses (Whitt, Harvey, McLeod, & Child, 2007). Minimal or no continuity of care will be a barrier to developing a comprehensive understanding of patients’ information needs even though hospitalization is an ideal time to provide educational resources (Driscoll, Davidson, Clark, Huang, & Aho, 2009).
Just under half of the respondents (n = 282) assisted patients to evaluate the online information. This aspect of education is the key element in developing patient self-efficacy in using online information in a personally productive way. Nurses require information literacy skills to be able to develop patient evaluation skills. Information literacy includes the ability to recognize information needs, identify and find information sources, assess quality and applicability, and then “analyze, understand, and use the information to make good health decisions” (Medical Library Association, 2003). The evaluation activities conveyed by nurses in this study centered around three key activities: opening up a two-way dialogue through inviting discussion about information sources, referring patients to reputable sites, and empowering through teaching how to judge the validity of online material. The process of evaluation was underpinned by knowledge and critical appraisal skills to judge the authority of the sites along with the use of guidelines and evaluation tools. Useful evaluative tools discussed in nursing literature include (a) the GATOR approach, an acronym for genuine, accurate, trustworthy, origin, and readability (Weber, Derrico, Yoon, & Sherwill-Navarro, 2010) and (b) the 5Cs website evaluation tool which covers credibility, currency, content, construction, and clarity (Roberts, 2010).
The study finding that 36% of the nurses did not discuss their personal health knowledge sources with their doctors is congruent with other research findings (Gilmour et al., 2012; Pletneva et al., 2011). Some respondents were concerned about disrupting relationships and feeling judged. These barriers to disclosure suggest a communication style by some health professionals where there is little or no invitation to develop a two-way dialogue exploring patients perceptions of their condition. When nurses are concerned about sharing their use of online resources for personal health information with their family doctor, these feelings may well influence their decisions related to engaging in such a discussion with the patients.
The study limitations include the response rate of 65.5%. The information that accompanied the questionnaire stressed that the responses from non-users of online information was important to the study but response bias is likely. Nurses familiar with Internet health information will, in all probability, be more interested in completing the questionnaire and therefore be over represented. The study also relies on the respondents self-report of practices and behavior. Most importantly in terms of limitations, this study focuses on one aspect of health education only, nurses’ engagement with patients independently seeking online material. Education strategies are wide ranging depending on patient preferences and the availability of online and hard copy educational resources.
Study Implications
Skill in the evaluation of online sources and their active incorporation into practice needs to be considered a basic competency for nurses in the PHC setting. Targeted professional development activities can be aimed at improving the incorporation of online resources into practice, developing nurses’ knowledge of useful patient websites and applying evidence-based approaches to determine the reliability of the sites. It is inevitable that people’s use of the Internet to support decision making in all aspects of life including health will rapidly increase and nurses’ engagement with this significant change in the practice landscape can no longer be optional. Patients’ self-directed information-seeking activities provide new opportunities for the development of health and information literacy skills.
Conclusion
The Internet is a powerful information and communication modality in today’s societies. Online information is used by the public for self-diagnosis of health issues and to supplement information provided by health professionals. The appropriate use of Internet informatics may empower and assist health care consumers to achieve better health. There is also evidence of quality concerns which coupled with patient reluctance to discuss information with health professionals raises questions about potential harm through information omissions and lack of expert peer review. This study contributes to the literature on nurses and their engagement with online resources for the purposes of patient education in the PHC setting where increasingly long-term conditions are managed. More nurses in this study engaged in proactive assessment of patient use of online material and supported the development of evaluation skills as compared with reports by nurses in earlier studies. Active engagement in the medium by nurses and patients has the potential to contribute to the development of health literacy and increase patients’ positive and knowledgeable engagement in health care decisions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study was funded through a Strategy to Advance Research Grant provided by the New Zealand Tertiary Education Commission.