
Abstract
Service quality in health care institutions is an emerging phenomenon, and many hospitals are concerned about providing quality service to their patients based on information obtained by the patient’s perceptions of service quality. First, we aimed to determine patients’ perception of service quality offered at Council for Health Service Accreditation of Southern Africa (COHSASA)–accredited private hospitals in Nigeria. And that included reexamining the dimensionality of SERVQUAL (the test tool) based on our sample data. Second, we aimed to find out whether there are any existing gaps between patients’ expectation and perception of the service quality. Third, this research is an attempt to test the perceived quality effects on patients’ satisfaction and repurchase intentions toward health services. Quantitative research was conducted via self-administered questionnaires to patients who attended a randomly selected COHSASA-accredited private hospital in Nigeria and analyze their data using a variety of quantitative procedures including structural equation modeling, factor analyses, and paired-samples t tests. A systematic sampling method was used, and a total of 228 questionnaires were used for the final analyses. SERVQUAL was found to be a three-factor variate comprising the following: tangibility, reliability, and sensitivity. Our results concluded that perceived quality was significantly lower than expected quality despite being accompanied with positive levels of satisfaction and repurchase intentions. Finally, patient’s satisfaction was found to fully transmit the indirect effects of two of the three factors, quality sensitivity and reliability, onto repurchase intentions, whereas tangibility does not exert indirect significant influences over repurchase intentions via patient satisfaction.
Keywords
Introduction
Any organization services, or products that desire growth and sustainability in the hypercompetitive environment of the 21st century, must be able to provide services and products that can meet the ever-changing needs of customers. To be able to gain competitive advantage, an organization must provide quality services that can engender customers’ satisfaction and loyalty. In this regard, the construct of quality is generally based on perceived quality, which is defined by Parasuraman, Zeithaml, and Berry (1988) as a “global judgment, or attitude, relating to the superiority of service.” According to Parasuraman, Zeithaml, and Berry (1985), a gap often exists between management and customers’ perception of service quality. For example, management perception of customers’ expectations could be at variance because management may not necessarily know what the customers desire from the organization.
The quality of health care service delivery in Nigeria is far below what is obtainable in the Western world, where there are often, the state-of-the-art medical technologies and innovative medications (Abiodun, 2010). In Nigeria, there is a paucity of training for medical staff as well as lack of renowned and well-equipped medical outfits (Fatunde, 2009). Patients often complain of long waiting time, majorly due to a significant disparity between patient and medical staff ratio (too many patients for too few medical staff). Communication between patients and medical staff is often poor, and sometimes the experiences between patients and medical staff are so poor that a switch from one hospital to another or from one physician to another becomes necessary with a few choices available for the patients (Adepoju, 2018). These switches can cause serious disruptions in the continuity of care with a negative impact on the outcome of care. The patients are often less informed and less knowledgeable about what constitutes quality service from patients’ perspective. Besides, the patient mix has also changed tremendously. Hospitals often encounter widely traveled patients who are increasingly more aware of what good health care service entails. These patients continuously demand better service quality. To remain competitive and sustainable, the provision of high service quality by health service providers becomes critical.
Although many researchers have studied service quality in many industries including the health sector and made their contributions available in the literature, there is a scarcity of information on service quality in health sector from countries in sub-Saharan Africa. Thus, the overall aim of this study breaks down into three main objectives. First, we attempt to revalidate SERVQUAL (the test tool) to check for its original dimensionality within the study context. Second, we assess the patients’ perceived health care service quality offered by private hospitals operating in Nigeria and accredited by the Council for Health Service Accreditation of Southern Africa (COHSASA; at the time of conducting this study) to help these hospitals leverage on current technological advances to bridge or reduce the existing gap between patients’ expectation and perception of the service quality provided by the organization to maintain its relevance both to the patients and financier of the service. Third, we investigate the effects of perceived quality effects on patients’ satisfaction and repurchase intentions using a theory-backed hypothetical model.
Literature Review and Hypotheses
Setting of Study
Our study was conducted at Chevron Hospital Gbagada, which was selected as a setting for our study based on a random selection among the four COHSASA-accredited private hospitals in Nigeria. The hospital is facing an increasing demand for higher patient satisfaction by its customers despite the dwindling funding by the management; the hospital needs to critically determine the perception of service quality from the patients’ perspective and channel its scares resources accordingly. This is particularly important because of a few and recent reports of poor service quality in Nigeria (Aregbeshola, 2019) with a potential threat to a hitherto exiting high patient satisfaction rating. A negative patient satisfaction rating could create a negative image for the hospital (Mahmoud & Reisel, 2014). Although Chevron Hospital Gbagada has been providing quality service, the need to sustain and/or improve on the existing positive perception of service quality by the patients appears to become more and more imperative.
The Chevron Hospital Gbagada has witnessed a significant budget cut in the last few years because Chevron Nigeria Ltd, the funding organization, is being faced with dwindling revenue as a result of the fall in oil prices. Yet, the patient and the organization still expect the hospital to continue to render quality service. Therefore, the need to provide services that are attractive to patients while containing cost has created the need for health care managers to evaluate and track the quality of services provided. To prevent customers’ complaints from a dissatisfied service, this research attempts to understand what Chevron Hospital Gbagada needs to put in place to meet or exceed patients’ perception of quality service and to identify new strategies that can be recommended to Chevron Gbagada management to close any gap between expectation and perception of quality services within the organization. The findings of this research are intended to provide some guidance on how service quality should be determined in health organizations in sub-Saharan Africa where there is a paucity of literature on this topic. In completing this research, we leveraged on theoretical framework and opinions of researchers on what constitutes service quality in the health care system.
Conceptual Framework
Recently, quality in health care service has generated a lot of interest in a sector that previously paid less attention to this topic. It is increasingly being linked to organizational sustainability in an ever-increasing competitive business environment. Service quality has also been identified as a major link between customer’s satisfaction and loyalty, essential determinants of organizational sustainability and competitive advantage (Cronin, Brady, & Hult, 2000).
The achievement of quality of services can be viewed as a goal and a marketing tool at the same time in the sense that attainment of high-quality service quality can bring about customers’ satisfaction. It becomes imperative therefore for companies to measure the quality of services they provide. In 1985, Parasuraman et al. developed a tool called SERVQUAL for measuring the quality of service. This tool was improved in 1988 and is based on perceived quality. SERVQUAL evaluates five distinctive service dimensions, and these dimensions are tangibles, reliability, assurance, responsiveness, and empathy. Tangibles deals with the physical facility and amenities/equipment of the firm. Reliability is the ability of the employees to perform the promised services dependably, correctly, and timely. Responsiveness is the willingness of employees to help customers in a prompt manner. Assurance is the ability of the staff to be courteous to customers, exhibit knowledge in what they do, and command trust and confidence. Empathy has to do with the ability of the employees of the organization to pay attention to the needs of the customers by caring and meeting individualized needs (Parasuraman et al., 1988).
Although many other models of service quality have been developed, SERVQUAL appears to be the most prominent despite the controversies raised by some researchers (Cronin & Taylor, 1992), which have to do with adapting an expectation–disconfirmation model rather than simply measuring attitudes.
Critics of the SERVQUAL model argue that a performance-based measurement is a better approach toward the measurement of service quality as the definition of quality is purely consumer dependent. Again, as service is intangible in nature, the SERVQUAL ignores expectation when measuring service quality, tending to leverage on performance as the single most important customer satisfaction outcome (Sharma & Ojha, 2004), thus suggesting that the performance-based measurement approach (SERVPERF) aligns more with the existing attitude and customer satisfaction literature and is generally agreed to be superior to the perception-expectation approach.
Although widely criticized in service quality literature, SERVQUAL remains a preferred model for measuring service quality across different sectors and has remained a generic instrument for measuring service quality. The advantages the SERQUAL model according to Rohini and Mahadevappa (2006) as cited by Padma, Rajendran, and Sai (2009) include,
Its acceptance as a standard for assessing different dimension of service quality;
Its validity and reliability for several service situations;
The instrument has few items and can easily be filled by respondents; and
It has a standardized analysis procedure to aid interpretation and result.
This leads us to posit the following hypothesis:
The developers of the SERVQUAL model suggested that service quality should be measured by subtracting customer perception from expectation scores. Positive scores signify higher service quality and vice versa (Parasuraman et al., 1985). SERVQUAL can, therefore, help service providers including health care institutions to identify their areas of strengths and weaknesses, though the developers do recommend that modifications in the scale are allowed to accommodate specific sector needs (Parasuraman, Berry, & Zeithaml, 1991). As no gap analyses have been undergone regarding health services offered by private hospitals in Nigeria (to identify the direction of the gaps scores), hereby, we state the following:
Service encounter is a term that has gained prominence in the marketing literature in recent years. The construct of service encounter is important for service quality because it is during the series of encounters with the service, customers assess and evaluate quality. Subsequently, Czepiel, Solomon, and Surprenant (1985) describe service encounter as the period of time, whereby a customer has a direct interaction with a service. This interaction is all-embracing and involves the contact and interaction of a customer with all aspects of the service organization, including the physical structures, equipment, and staff. Service encounter can also occur without any human interaction (Bitner, Booms, & Tetreault, 1990).
The health care organization frequently offers services where there is often a face-to-face interaction with customers. This means that managers of health care organizations should put a strategy in place that can ensure that employees are well motivated to provide an excellent service encounter to customers. Physical structures and equipment should also be attractive to customers. Many researchers including Bitner et al. (1990) have shown a link between service encounter and customer satisfaction. Lee, Chua, and Han (2017) have also shown in their study that a higher service encounter performance and physical environment have a positive impact on overall customer satisfaction and loyalty.
As each service encounter contributes to overall customer satisfaction and their willingness to continue to make use of the service, it is important for health organizations desiring excellent service quality and competitive advantage to understand, measure, and optimize their core service delivery process to ensure that each service encounter is perceived as being excellent (Voorhees et al., 2017).
Based on the above review, we hypothesize the following:
Method
Chevron Hospital was randomly selected among the only four COHSASA-accredited private hospitals in Nigeria at the time of collecting data for this research. The Chevron Hospital Gbagada is manned and funded by Chevron Nigeria Ltd, a multinational oil and gas organization. It was founded in 1999 with the sole aim of providing quality health care services for both the employees and retirees of the organization, as well as their eligible family members. And given the fact that Chevron is a COHSASA-accredited hospital, Chevron Hospital is assumed to function in line with COHSASA’s mission statement which avows that it exists “to assist healthcare facilities in developing countries to deliver quality healthcare through sustained improvement, using internationally recognized standards, patient safety principles and operational research” (COHSASA, n.d.). Chevron Hospital Gbagada has created a niche for itself in the area of quality health care delivery, having served as the referral center for the two other hospitals manned and funded by Chevron Nigeria Ltd, one in Lagos and the other in Warri, each in Lagos and Delta States of Nigeria, respectively. In an effort to benchmark its service quality with international standards, the management of the hospital recently engaged the COHSASA to carry out an accreditation exercise for the hospital.
A systematic sampling method was used, and to select the 300 participants, every sixth patient was enrolled. This approach was adopted because of the relatively large study population of about 2,000 patients who visit the hospital every month. The figure was determined based on the hospital attendance trend in the last 1 to 2 years. The 300 patients were drawn from adult patients who attended both the inpatient and outpatient services of the hospital between June 1 and 30, 2017 (1 month). The different clinics where patients were recruited include antenatal clinic, medical outpatient (MOP), general outpatient clinic (GOPD), surgical out-patient clinic (SOP), and occupational health (OH). Nondisclosure agreements (NDAs) were signed, and all questionnaires were made anonymous. Furthermore, all required approvals were obtained before the administration of the test tool. In addition to demographics, both version of the survey included the 22-statement SERVQUAL. Single-item measures of patient satisfaction and repurchase intentions were added to the postexperience survey. In total, 72 patients did not agree on taking part in the survey. Therefore, a total of valid 228 interviewer–administered questionnaires were only used for the final analysis. Both confirmatory and exploratory factor analyses were used to assess the dimensionality of SERVQUAL. Paired-sample t tests were undergone to test the significance of the service quality gaps. Eventually, path analysis as a structural equation modeling approach was carried out with bootstrapping optioned to test the path from perceived quality to repurchase intentions via patient’s satisfaction as a mediator. Eventually, the aforementioned tests were run using SPSS V. 25 and AMOS V. 23.
Results
Demographic Survey Result
The majority of our sample were GOPD-recruited. Furthermore, 55% of respondents were males and over 50 years of age. In addition, 75% were retirees and their spouses. This shows that most of the patients who attend Chevron Hospital Gbagada are people in the middle age and elderly categories. For there to be such a large pool of patients in these age categories in a country where the life expectancy is 48 years and 52 years for men and women, respectively, it means that at least the technical service quality provided by the hospital must be quite good. The fact that majority of patients are not particularly young may have some implication on what could be considered as measures of service quality. Li et al. (2015) suggested in their study that older people may tend to pay less attention to certain aspects of functional service quality and get easily satisfied with services provided, particularly, if those services satisfy their technical needs.
Hypotheses Testing
We tested the structure of SERVQUAL using confirmatory factor analysis. Results came to refute the five-factor dimensionality that was stated by H1, as our statistics referred to poor fit for the measurement model to our data, e.g., χ2/df = 6.88 > 3; root mean square error approximation (RMSEA) = .16 > .08; comparative fit index (CFI) = .78 < .90; Tucker–Lewis index (TLI) = .71 not close to .95 (Bentler, 1990; MacCallum, Browne, & Sugawara, 1996; Mahmoud & Grigoriou, 2017; Tucker & Lewis, 1973). Thus, as recommended by Byrne (2010, 2016), we performed an exploratory factor analysis (EFA) to conclude the valid dimensionality of quality. EFA results reveal that expected/perceived quality is a three-factor variate comprising of tangibility, reliability, and sensitivity. With internal consistency alphas ≥ .7 (Hair, Black, Babin, & Anderson, 2010) and average variances extracted (AVEs) > .5 (Fornell & Larcker, 1981), the new constructs are deemed to be valid and reliable (See Table 1 and Table 2).
Exploratory Factor Analysis.

Note. CR = composite reliability; AVE = average variance extracted.
Intercorrelations and Descriptives.
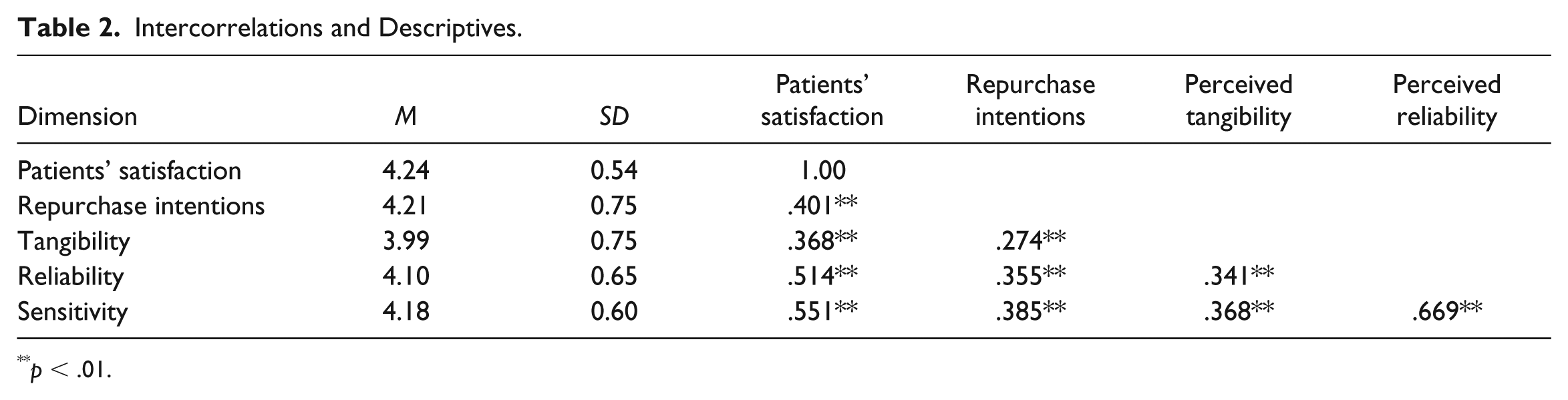
p < .01.
To test the gaps between expected and perceived quality (see Table 3), we ran paired-samples t test. Our results show that perceived quality was significantly lower than expected quality, i.e., Pair 1: perceived tangibility–expected tangibility (t = −9.87, df = 227); Pair 2: perceived reliability–expected reliability (t = −11.16, df = 227); Pair 3: perceived sensitivity–expected sensitivity (t = −14.35, df = 227); despite our sample held positive levels of expected quality, i.e., expected tangibility (t = 45.92, df = 227), expected reliability (t = 55.60, df = 227), expected sensitivity (t = 81.20, df = 227), as well as perceived quality, i.e., perceived tangibility (t = 19.77, df = 227), perceived reliability (t = 25.65, df = 227), perceived sensitivity (t = 29.95, df = 227). These inferential statistics were accompanied with positive levels of satisfaction (t = 34.85, df = 227) and repurchase intentions (t = 24.35, df = 227).
Hypothesis 2 Testing Results.
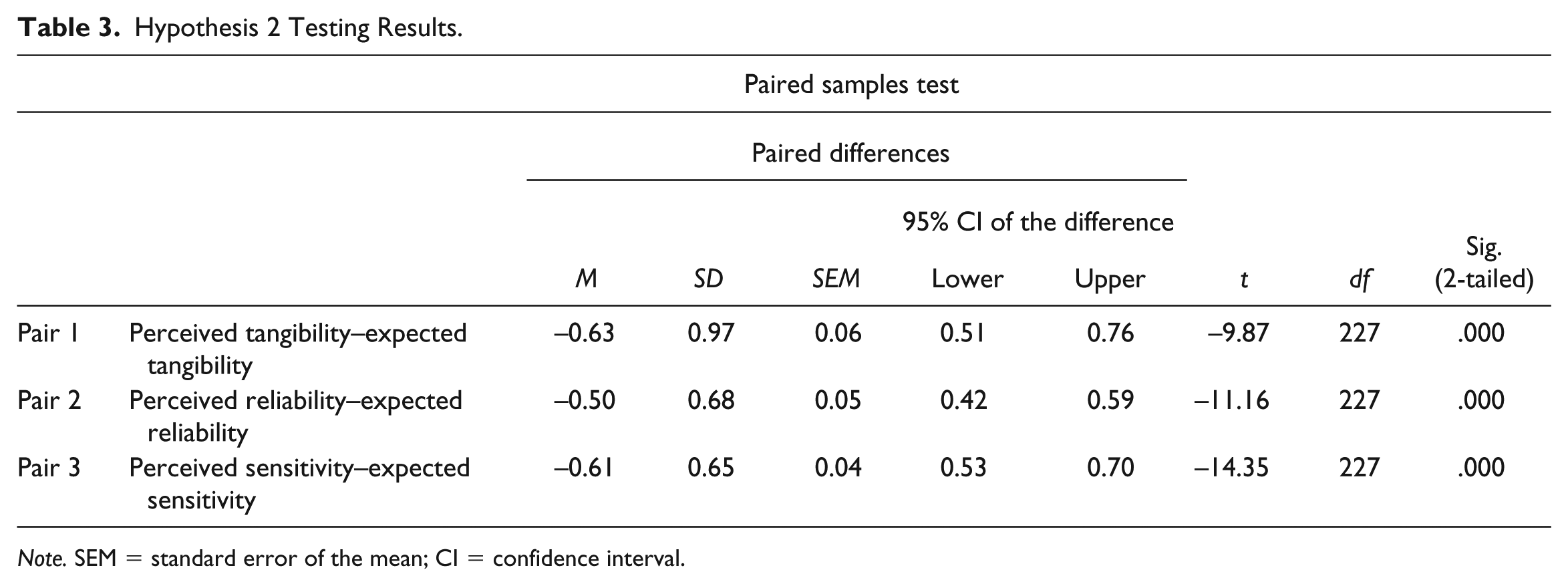
Note. SEM = standard error of the mean; CI = confidence interval.
Path Analysis
We performed path analysis to test the hypothesized path (H3) from perceived quality to repurchase intention via patient satisfaction. Bootstrapping was also employed as part of testing the mediating role of patient satisfaction between quality gaps and repurchase intentions. The three dimensions of perceived quality significantly related to satisfaction, that is, tangibles (β =.15, p = .13), quality sensitivity (β = .24, p < .001), and reliability (β = .35, p < .001). Patient satisfaction was found to significantly predict repurchase intentions (β = .40, p < .001). All in all, and based on Baron and Kenny’s (1986) work, we found that patient’s satisfaction fully transmits the indirect effects of only two dimensions, quality sensitivity (B = .12, p < .05) and reliability (B = .21, p < .01), onto repurchase intentions, whereas the third dimension, tangibles (B = .08, p = .15), does not exert indirect significant influences over repurchase intentions via patient satisfaction. Finally, our statistics (Meyers, Gamst, & Guarino, 2017) imply that the alternate model has a good fit to our data, χ2/df = 2.06 < 3; standardized root mean square residual (SRMR) = .04 < .1; RMSEA = .06 < .08; CFI = .98 > .95; TLI = .96; adjusted goodness of fit index (AGFI) = .91 > .90. Hereby, we conclude that H3 is partially valid (see Figure 1).

Path model testing.
Discussion
This research was designed to investigate patients’ perception of service quality in COHSASA-accredited private hospitals in Nigeria, and the impact of perceived quality on customers’ satisfaction and repurchase intentions. Chevron Hospital Gbagada was selected randomly for this study—as one of COHSASA-accredited Hospitals in Nigeria. The study was conducted with the use of survey questionnaire to revalidate the SERVQUAL measurement model within a Nigerian context, identify the gaps in certain service quality dimensions, and detect their direction and significance. Furthermore, we attempted to test the path model linking quality gaps to repurchase intentions via satisfaction using a structural equation modeling approach (SEM). H1 was rejected and perceived quality was found to be a 3-dimension variate comprising of tangibility, reliability, and sensitivity. The change in the structure of the SERVQUAL is in line with previous research that concluded structural changes in attitudinal measures due to cultural variations (e.g., Mahmoud, 2013; Mahmoud, Grigoriou, Fuxman, & Reisel, 2019; Mahmoud, Grigoriou, Fuxman, Hack-Polay, et al., 2019).
The perception scores were generally lower than expectation scores, thus, H2 was accepted. This implies, given the new dimensionality of the perceived quality structure, a decline in the scores of the tangibles, sensitivity, and reliability gaps. This finding is in line with previous research. For instant, notwithstanding, the patients reported higher levels of repurchase intentions than average which, based on our path analysis, was mainly due to the positive levels of satisfaction sourced by favorable perceptions of sensitivity and reliability despite being less favorable than what was expected by the patients. Such positivity can be linked to the 5-year rise in life expectancy in Nigeria from 47 in the 1990s to 52 in 2015 (Anyamele, Akanegbu, & Ukawuilulu, 2015).
The findings of this study must be treated with caution by the management of Chevron Hospital Gbagada because there has been a recent increase in the proliferation of conglomerate hospitals within the Lagos metropolis. This development will definitely influence patients’ expectations of medical services because of the changing nature of consumer behavior. In addition, there is a need to constantly review the expectations of patients through regular customer surveys, and where expectations fail short, improvement can be achieved through total quality management programs. For example, sharing information and communicating effectively with staff (Mahmoud, Del Rosario, Reisel, Pantsios, & Hack-Polay, 2018) have been found to boost total quality management (TQM) application in organizations (e.g., Mahmoud, Alatrash, Fuxman, Hack-Polay, & Grigoriou, 2019; Mahmoud, Alatrash, Fuxman, Meero, & Yafi, 2019).
Because patients’ satisfaction can be improved by an excellent patient–staff interpersonal relationship (Padma et al., 2009), the Chevron Hospital management should ensure that the medical staff are well motivated to interact nicely with patients. For example, offering staff high levels of job security can boost their job satisfaction and other positive organizational outcomes (Mahmoud & Reisel, 2015), which has been found to be increasing health service quality and hence patient satisfaction (Mahmoud & Reisel, 2014). Research has shown that good staffing ratios of patients to medical staff are associated not only with good patient outcomes but also with increased patient satisfaction levels (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002). The staff–patient ratio should be increased by new hiring. The existing staff remuneration can be increased, thus chances for health worker strikes over wages can be lowered (Abiodun, 2010). The staff should also be trained on emotional intelligence. Where it is not possible to increase staff strength, the hospital should provide a platform that can enable patients to make use of smart applications, thus reducing patient–staff interactions. In this regard, such applications should be designed to deliver informative content as Internet users tend to be more active, selective, and constructive in information processing (Mahmoud, 2014).
On the whole, continuous TQM activities should be integrated into the daily routines for the hospital, and this should be followed by a 2-year external accreditation exercise. TQM is used to obtain competitive advantage in hospitals as it encourages employees to strive to achieve zero mistakes, the first time and always. TQM and quality improvement processes have resulted in improved service quality in health care organizations (Alkhenizan & Shaw, 2011; Sadiq Sohail, 2003). Any gaps identified should be immediately mitigated. Regular customers’ satisfaction survey should be conducted, and service quality adjusted to meet patients’ needs.
Limitations and Research Implications
This study was conducted in a hospital in Nigeria where the standard of practice is much higher than what is obtainable nationwide, and so the findings of this study cannot be used to represent the perception of service quality in a typical Nigerian hospital.
We concluded a new dimensionality of SERVQUAL in a Nigerian health care setting. The measurement model was found to comprise three factors rather than five. Therefore, we encourage scholars to run SERVQUAL revalidations (including invariance analyses) for health services in future studies, especially in sub-Saharan Africa to detect any possible changes of the 31-year-old instrument.
The age distribution of respondents was skewed toward an older population. This can affect what could be considered as measures of service quality. Further study should focus on a health care system that has equal representation in terms of patients’ age and employment status.
This research was a quantitative research, thus, combining qualitative and quantitative (triangulation) research on the evaluation of service quality dimensions and its correlates could deliver more insightful findings in future research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.