
Abstract
Discourse about health that focuses predominantly on body weight is referred to as the weight-centered health paradigm (WCHP). In recent years, there has been a significant increase in critical analysis of the WCHP. This has resulted in arguments for a paradigm shift away from focusing on weight and focusing instead on health and well-being. The aim of this study was to identify, critique, and synthesize the values, claims, and assumptions of the WCHP and to develop a framework to be used as a heuristic for building competency to critique the WCHP. Qualitative content analysis of the literature was used to identify themes, relationships between themes, and structure of the framework. The resulting WCHP 3C Framework encompasses the context, critiques, and consequences of the WCHP. The context includes the promulgators and tenets of the WCHP. Critiques of the WCHP raise ideological, empirical, and technical concerns. Consequences of the WCHP include an enhanced adipophobicogenic environment, reduced health and well-being, and reduced quality of life. If used as a heuristic to enhance critical competence, the WCHP 3C Framework may help contribute to a paradigm shift in weight science.
Plain Language Summary
Putting body weight at the center of thinking and talking about health is referred to as the weight-centered health paradigm (WCHP). This has resulted in arguments for a paradigm shift away from focusing on weight and focusing instead on health and well-being. We reviewed the literature to identify the main components of the WCHP. From the results, we created a framework, named the WCHP 3C Framework. The 3C Framework describes the people and industries contributing to the WCHP and the central claims of the paradigm. It also identifies the three major types of critique of the WCHP: ideological, empirical, and technical. Finally, the 3C Framework highlights that the WCHP is contributing to weight stigma and fat phobia, reduced health and well-being, and poorer quality of life. We hope the 3C Framework will contribute to a paradigm shift in weight science.
Background
The message from health authorities in many parts of the world today is that having a body weight that is classified as ‘overweight’ or ‘obese’ is unhealthy. This message manifests in public health and health promotion policies and programs focused on ‘obesity’ prevention. Discourse about health that focuses predominantly on body weight is referred to as the WCHP (Bacon & Aphramor, 2011; Campos, 2004; Robison, 2003b), or the weight-normative approach to health (Tylka et al., 2014). Science philosopher Thomas Kuhn described a paradigm as a collection of ideas, concepts, values, and beliefs that form the foundation for the approaches and techniques used by members of a scientific community. A paradigm provides guidance for the choice of scientific issues to work on and the nature and structure of research questions. The paradigm also guides the choice of research methodology, the way results are interpreted, and the acceptability of different explanations (Kuhn, 1970). The most widely held set of rules or tenets at any given time is known as the dominant paradigm (Barker, 1993). The WCHP is the dominant paradigm in current discourses related to body weight and health.
The Technical Report: From Weight to Well-Being: Time for a Shift in Paradigm? published by the British Columbia Provisional Health Services, described four weight-related paradigms (Provisional Health Services Authority, 2013). In the first paradigm, the body mass index (BMI) categories of ‘overweight’ and ‘obesity’ are problematized, and BMI is said to be reduced through limiting caloric intake and increasing energy expenditure. The second paradigm approaches the medically problematic BMI categories of ‘overweight’ and ‘obesity’ through an ecological lens addressing the ‘obesogenic’ environment. Both of these paradigms place weight in the center of discussions about health, and can be referred to collectively as the WCHP. The third paradigm focuses on optimizing psychological and physical health and well-being of people of all shapes and sizes through intuitive eating and enjoyable leisure and physical activity. The fourth paradigm moves beyond the individual level to promote flourishing in mind and body for all people by acting on the broader socio-environmental factors that impact on health and social issues such as weight bias, stigma, bullying, and discrimination. The third and fourth paradigms can be referred to collectively as the weight-neutral or weight-inclusive (Tylka et al., 2014) approach to health.
In the fields of weight science and public policy related to body weight, nutrition, and physical activity, as well as in the popular media’s portrayal of the ‘ideal’ body, the positivist WCHP (Aphramor, 2012) is the dominant paradigm (Bacon & Aphramor, 2011; Campos, Saguy, Ernsberger, Oliver, & Gaesser, 2006). According to Monaghan, Hollands, and Pritchard (2010), a range of agents is engaged in the ‘enterprising act’ of socially constructing fatness as a ‘correctable’ health problem. These agents are variously described as ‘obesity epidemic entrepreneurs’ (Monaghan et al., 2010), ‘anti-obesity proponents’ (Saguy & Riley, 2005), ‘obesity alliances’ (Strategies to Overcome and Prevent [STOP] Obesity Alliance), ‘obesity crusaders’ (Basham & Luik, 2008), or ‘obesity alarmists’ (Gard, 2011b).
Concomitant with the rise to dominance of the WCHP is the increasing volume of critique from many fields including health professionals, academics, political scientists, lawyers, sociologists, journalists, and members of the community. Detailed critiques on various aspects of the WCHP have been presented in research-based books (see Table 1 for some examples), journal articles, and book chapters (see, for example, Aphramor, 2005, 2010; Bacon & Aphramor, 2011; Basham & Luik, 2008; Bombak, 2013; Campos et al., 2006; Cohen, Perales, & Steadman, 2005; B. Evans & Cooper, 2016; J. Evans, Davies, & Rich, 2008; Lupton, 2014; Monaghan et al., 2010; O’Hara & Gregg, 2006, 2010, 2012; O’Hara, Taylor, & Barnes, 2015a, 2015b; O’Reilly & Sixsmith, 2012; Rich & Evans, 2005; Rich, Monaghan, & Aphramor, 2011; Robison, 2003a, 2003b; Tylka et al., 2014). Popular books are also engaging in critique of the WCHP, proliferating from the early pioneers in the 1980s and 1990s of Such a Pretty Face: Being Fat in America (Millman, 1980), Shadow on a Tightrope: Writings by Women on Fat Oppression (Schoenfielder & Wieser, 1983), Fat!So?: Because You Don’t Have to Apologize For Your Size (Wann, 1998), and Fat and Proud: The Politics of Size (Cooper, 1998), to a vast array of fiction and nonfiction books telling people’s personal stories and either explicitly or implicitly critiquing the WCHP. The ‘fatosphere,’ the collective term for bloggers on the Internet that write specifically about the cultural obsession with avoiding fatness, is a flourishing space for critique of the WCHP (Dickins, Thomas, King, Lewis, & Holland, 2011; Harding & Kirby, 2009).
Examples of Research-Based Books Critiquing the Weight-Centered Health Paradigm.
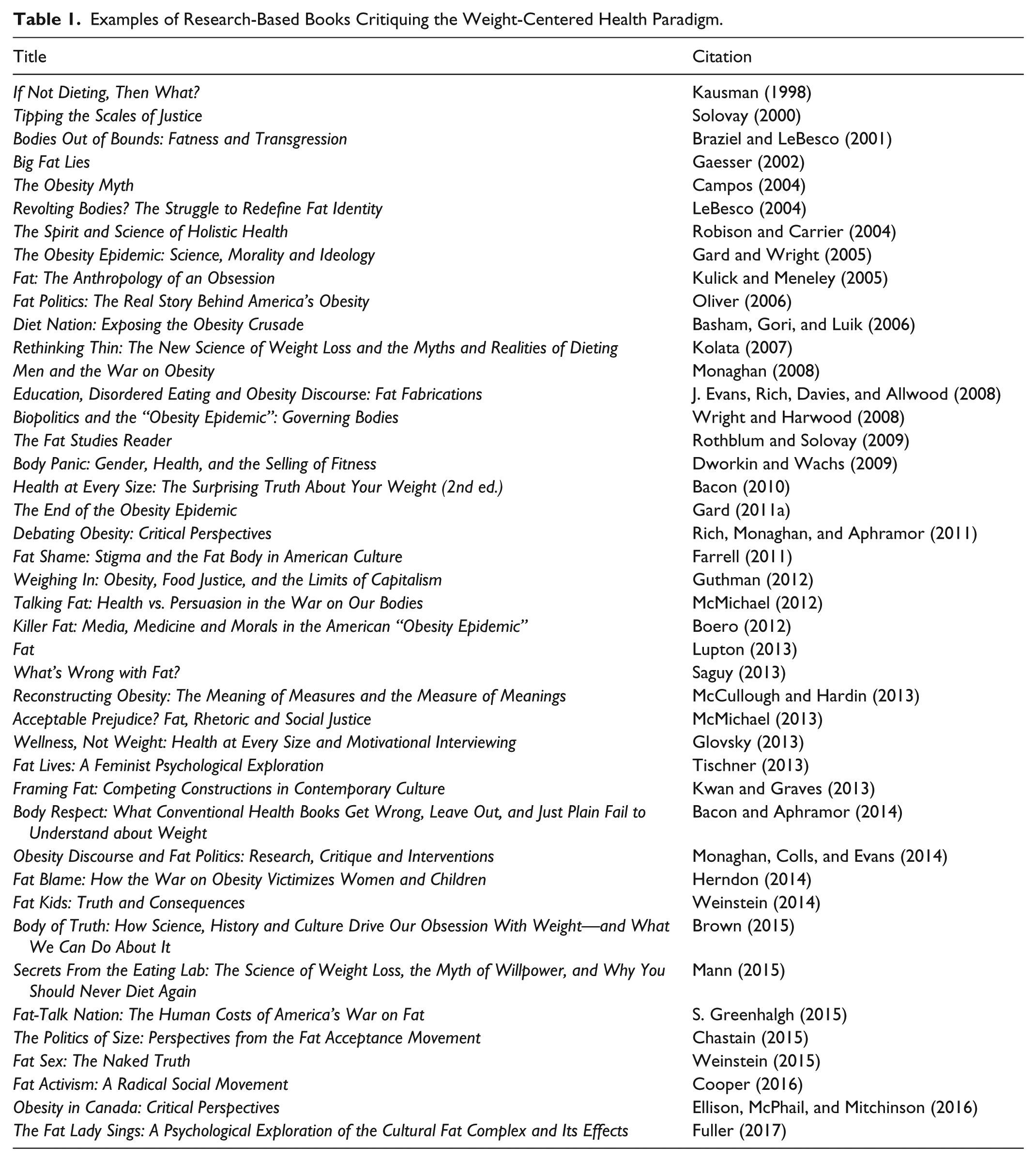
Authors within the academic literature refer to their scholarship as ‘critical weight studies’ (Monaghan et al., 2010), ‘critical obesity studies’ (Gard, 2009), or ‘fat studies’ (Rothblum & Solovay, 2009). The variation in the terms reflects nuanced ideological positions; however, they share common ground in critiquing the claims made by proponents of the WCHP. Despite this growing body of critical scholarship, the WCHP remains dominant in the fields of medicine, public health, health promotion, and within the general community. One strategy for advancing alternative paradigms is to review the values, assumptions, and claims of the dominant paradigm (Barker, 1993; Gokhale, 2007). This narrative review aimed to identify, critique, and synthesize the values, claims, and assumptions of the WCHP. In the review, we favored ‘sense making over cataloging’ (T. Greenhalgh, Potts, Wong, Bark, & Swinglehurst, 2009), meaning that we sought to tease out and present the various narratives about the WCHP rather than produce an inventory of every publication on the paradigm.
Method
The epistemological position of the study was constructivist and critical theory provided the theoretical perspective (Crotty, 1998). Critical theory seeks to identify and analyze the root causes of social issues and to propose ways to alleviate or resolve them. According to Fairclough, Graham, Lemke, and Wodak (2004), the most pressing social problems in the world today are the unjust social relations that stem from the categorization of people that supports and is supported by oppressive attitudes and practices. Critical theory was appropriate for this study because it focused on reviewing one of the most dominant health paradigms evident in current public health and health promotion practice—the paradigm founded on the categorization of people based on their adiposity. The objective of this narrative review was to develop a comprehensive framework for describing the context, critiques, and consequences of the WCHP for the purpose of building competency to critique the dominant paradigm.
An online literature search was conducted for scholarly articles, books, policies, and programs (collectively referred to as documents) that met at least one of the following criteria: (a) describes some aspect of the WCHP, (b) critiques some aspect of the WCHP, or (c) provides evidence related to a critique of the WCHP. Electronic databases used in the search included Proquest, Ovid, PUBMED, Medline, CINAHL, Annual Reviews, JSTOR, PsycINFO, Taylor and Francis Online, Sage Online, Oxford University Press Journals, and Google Scholar. No date limits were set for the search but articles had to be published in English. Search terms were broad and included ‘weight-centred health paradigm,’ ‘weight-normative health paradigm,’ ‘critical weight studies,’ ‘fat studies,’ ‘critical dietetics,’ ‘critical obesity studies,’ ‘obesity critique,’ ‘obesity sceptic,’ ‘war on fat,’ ‘war on obesity,’ ‘anti-obesity,’ and ‘obesity prevention.’ Search terms were used alone and in combination. Reference lists of retrieved documents were reviewed and manual searches were conducted for authors who had published in the field. The search for documents was iterative and ongoing from July 2005 to December 2017. As points of critique were identified, new searches were conducted related to that critique. By the concluding date, over 2,000 documents had been retrieved for analysis. Qualitative content analysis was used to identify themes, the relationships between those themes, and the structure of the overall framework. Documents were initially coded as being related to a priori categories of context, critique, or consequence of the WCHP. Subsequently, documents were coded for emergent subcategories. Iterative thematic analysis of the subcategories and categories led to the development of the final framework. The search and analysis continued until data saturation was reached, and no new themes were emerging. The analysis process was collaborative and no formal measures of interrater agreement were used. Instead, the research team iteratively reviewed the evolving framework and discussed additions or changes until consensus was reached. Terms related to the categorization of body weight—‘underweight,’ ‘healthy weight,’ ‘normal weight,’ ‘overweight,’ ‘obese,’ or ‘obesity’—are presented in inverted commas to signify the contested status of such labels.
Results
The context, critiques, and consequences of the WCHP and the relationships between them are presented in the WCHP 3C Framework (Figure 1), an inductive ‘descriptive categories’ conceptual framework (Shields & Tajalli, 2006). Starting at the bottom left side of the figure, the framework describes the promulgators of the WCHP. Moving upward to the top left of the figure, the tenets of the WCHP that are disseminated by the promulgators are described under nine main categories. The tenets then lead to actions, often referred to as the ‘war on obesity,’ which have been critiqued from a wide range of perspectives. The categories of critique and the numerous themes within each main category are presented in the middle column of the figure. The consequences of the WCHP, as highlighted by the critiques, are summarized in the right side of the figure. Each of these components is now examined in further detail.

Weight-centered health paradigm 3C Framework.
Context of the WCHP
Promulgators of the WCHP
Numerous components of society that promulgate the WCHP were identified. ‘Anti-obesity crusaders’ (Basham & Luik, 2008) or ‘obesity epidemic entrepreneurs’ can be categorized as “creators, amplifiers/moralizers, legitimators, supporters, enforcers/administrators and the entrepreneurial self” (Monaghan et al., 2010; p. 46). In the role of WCHP creator is the scientific community, particularly the field of epidemiology. The popular media amplify the WCHP by uncritically reporting what are presented as scientific ‘facts’ about ‘obesity,’ and heavily propagating the concept of the ‘ideal’ body for health and beauty. By framing ‘obesity’ as an inherently moral issue, the popular media also play the role of moralizer.
Governments, particularly public health departments, legitimize the WCHP by instituting ‘anti-obesity’ task forces, commissioning ‘obesity’ reports, and implementing ‘anti-obesity’ public health policies and programs which include surveillance, screening, and health promotion initiatives.
The weight loss industry and ‘anti-obesity’ campaigners provide opportunist support for the WCHP. Health professionals enforce or administer the rules of the WCHP through their interactions with health care consumers. And for the people that are the ‘target’ of the WCHP, choosing to engage in attempted weight loss signifies their moral worth and civic responsibility. However, they are also required to navigate the weight stigma, discrimination, and other forms of oppression that are an inherent part of the WCHP (Monaghan et al., 2010).
Tenets of the WCHP
The tenets of the WCHP were not explicitly articulated as a comprehensive, universally agreed list in any one document. Synthesis of claims made either explicitly or implicitly by promulgators of the WCHP yielded nine related tenets (Table 2).
Tenets of the Weight-Centered Health Paradigm.
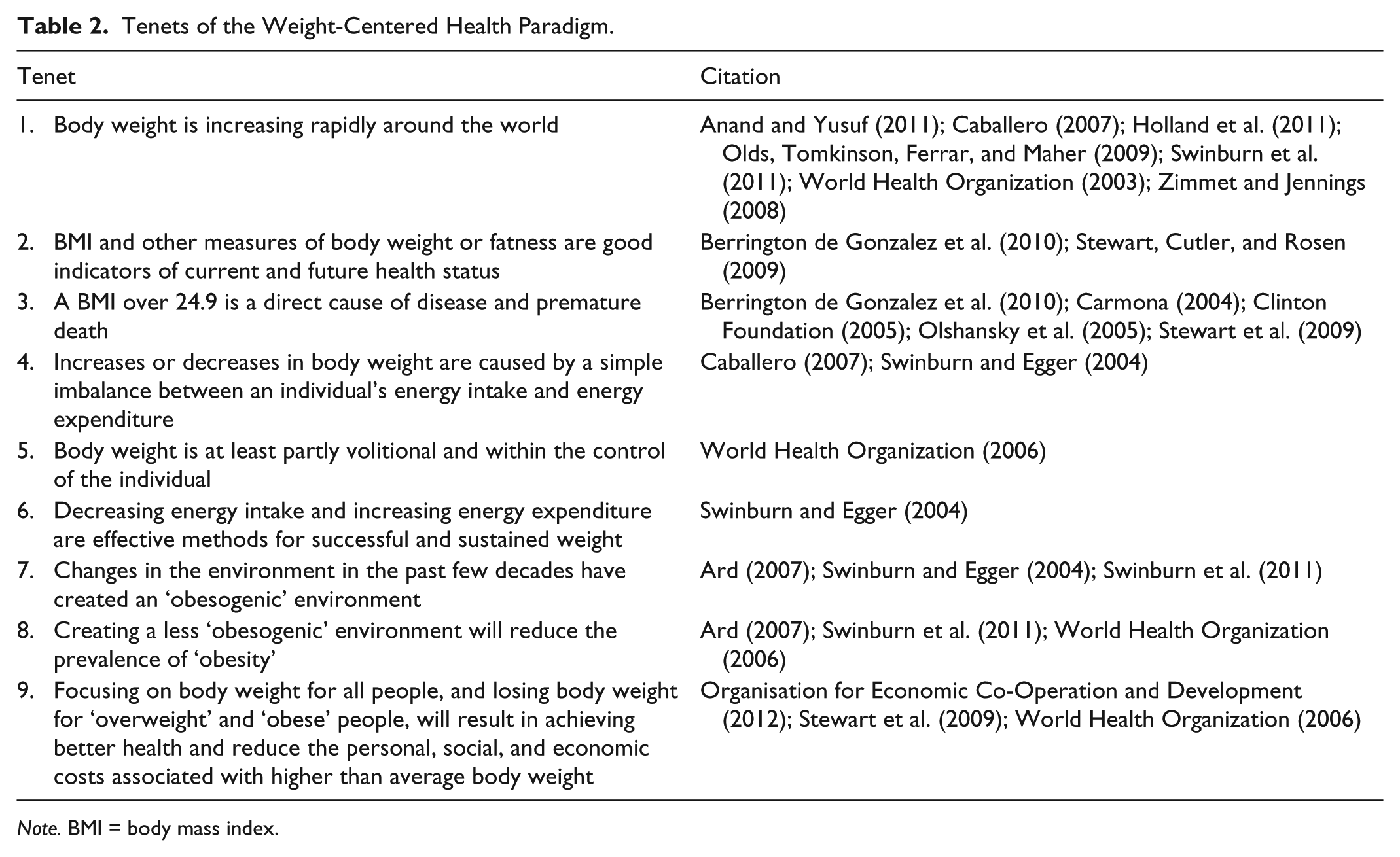
Note. BMI = body mass index.
Critiques of the WCHP
Three major thematic categories of critiques were identified: ideological, empirical, and technical. Within each major category, there were three subcategories. Ideological critiques related to philosophical, ethical, and human rights issues. Empirical critiques related to inaccuracies of the tenets, ineffectiveness of programs developed according to the tenets, and potential unintended (iatrogenic) harms that arise from the application of the tenets. Technical critiques related to the use of a limited strategy portfolio, the role of health experts as policy and program drivers and the absence of people directly affected by these issues, and the focus of program evaluation on behavior change and body weight rather than health and well-being.
Ideological Critiques
Ideological critiques included three thematic subcategories: philosophical, ethical, and human rights. The philosophical critiques subcategory included themes of biomedical and behavioral health paradigm, healthism, neoliberalism, moral panic, objectivism, reductionism, fear-based, gender, class, and race discourses. The ethical subcategory included themes of maleficence, patriarchy, individual blame, disempowerment, continued prescription of ineffective treatment, surveillance and regulation of bodies and behaviors, and undeclared conflicts of interest. The human rights subcategory included themes of contraventions of the rights to health, education, and freedom from discrimination. It is beyond the limits of this article to discuss all of these critiques, so we have selected a limited number for further discussion.
The ‘war on obesity’ has resulted in unwarranted surveillance and regulation by governments and society of people’s bodies and behaviors (Basham, Gori, & Luik, 2006; Consumer Freedom, 2004; Ikeda, Crawford, & Woodward-Lopez, 2006; Kaczmarski, DeBate, Marhefka, & Daley, 2011; Nihiser et al., 2009; Rich, 2010). Such surveillance and regulation are inequitably experienced by women, the poor, and minorities, and therefore result in greater inequalities in health (Dolgin & Dieterich, 2011; Friel, Chopra, & Satcher, 2007; Herndon, 2014; Rail, Holmes, & Murray, 2010; Saguy & Riley, 2005). As a result of its contribution to health inequity, the WCHP has been criticized as being a social determinant of health in its own right (O’Hara & Gregg, 2006) and inconsistent with a human rights approach to health (O’Hara & Gregg, 2012).
In a previous study on the relationship between the human rights enshrined in the Universal Declaration of Human Rights (UDHR) and the WCHP (O’Hara & Gregg, 2012), we found that weight-centered public health policies and programs do not implicitly or explicitly acknowledge or address the potential violations of human rights that arise from their implementation. Of significant concern was that because of weight stigma (to which the WCHP makes a significant contribution), at least 13 of the human rights listed in the UDHR may be contravened. For example, Article 26 of the UDHR states that everyone has the right to education. However, fat people are less likely to attend college or university, irrespective of their level of competence to do so (Fikkan & Rothblum, 2005). Fat women are more likely to have to pay their own college tuition rather than be supported by their parents (Crandall, 1995), and fat students are more likely to be refused letters of recommendation from teachers (Puhl & Brownell, 2001). Fat students show no statistically significant differences in intelligence or achievement test scores, yet receive significantly lower grades in middle school, community college, and university, after controlling for demographic variables, intelligence, personality, and well-being (MacCann & Roberts, 2013).
Empirical Critiques
Empirical critiques focused on the nature and quality of evidence supporting the tenets of the WCHP, and were categorized into three major themes: inaccuracies of the tenets, ineffectiveness of programs developed according to the tenets, and the potential unintended (iatrogenic) harms that arise from the tenets. Critiques about inaccuracies related to Tenets 1, 2, 3, 4, 5, 7, and 9, and were grouped into three thematic categories: inaccurate portrayals of trends in body weight, determinants of body weight, and associations between body weight and health outcomes. Critiques about ineffectiveness related to Tenets 6 and 8, and were grouped into two thematic categories: ineffectiveness for managing body weight and the counter productivity of the WCHP. Critiques about the iatrogenic potential of the WCHP related to Tenet 9, and were grouped into four thematic categories: psychological, behavioral, physical, and social harms. Within each of these thematic categories were numerous themes of specific harms. Psychological harms included body dissatisfaction, distraction from other life goals, discomfort and distress, dutiful thinking, distrust of the body, disembodiment or disassociation from one’s body, and depression. Behavioral harms included delayed living, delayed health care, dieting, and disordered eating and exercising. Physical harms included diminished quality of health care, decreased nutrient absorption, decreased satiety, destabilized body weight, increased disease risk factors, and death. Social harms included dehumanization and discrimination, stigma, prejudice, and other forms of oppression. Some of these critiques are now discussed in more detail.
Inaccurate
The foci of critiques about inaccuracy include (a) the veracity or interpretation of data on changes in average body weight and the appropriateness of terms and language used to describe the extent of these changes (including the ‘epidemic’ discourse; Basham & Luik, 2008; Boero, 2007; Campos et al., 2006; Gard, 2011b; Herndon, 2005; Rail et al., 2010), (b) the depiction of the determinants of body weight as simply too much food and too little movement (Bacon, 2010; Bacon & Aphramor, 2011), and (c) the relationships between body weight, morbidity, and mortality (Basham et al., 2006; Campos, 2004; Campos et al., 2006; Ernsberger & Koletsky, 2000; Gaesser, 2002; Gard & Wright, 2005; Mitchell & McTigue, 2007; Monaghan, 2005; Oliver, 2006; Pieterman, 2007), including erroneously presenting correlations as if they are causations (Bacon, 2010; Gaesser, 2002; Gard & Wright, 2005; Robison & Carrier, 2004).
Trends in Body Weight
Changes in the prevalence of people classified as ‘overweight’ and ‘obese’ according to the World Health Organization (WHO) BMI categories have been used to establish evidence of need for weight-related public health initiatives. The prevalence of people with a BMI classified as ‘overweight’ or ‘obese’ is reported to have increased rapidly throughout the world (Anand & Yusuf, 2011; Campos et al., 2006), and that everyone everywhere is at risk of becoming ‘overweight’ or ‘obese’ (Campos, 2004). The use of such terms such as ‘global,’ ‘epidemic,’ ‘pandemic,’ and ‘globesity’ have contributed to the notion that body weight is increasing exponentially and that these changes are sweeping through the populations of developed and developing countries alike (Caballero, 2007; Swinburn et al., 2011; WHO, 2003). These statements are based on statistical increases in the proportion of people in the ‘overweight’ and ‘obese’ BMI categories over a 30-year period. The relativistic terms ‘doubled’ and ‘tripled’ serve to effectively dramatize these trends, despite the fact that the majority of people are only 3 to 5 kg heavier than they were a generation ago (Campos et al., 2006). Furthermore, these terms give the impression that weight gain has occurred universally across the weight spectrum. However, for people at the thinner end of the spectrum, there has been no average increase in body weight since the early 1990s, while for people in the middle of the spectrum, average weight has increased by 2 to 3 kg (Flegal, Carroll, Ogden, & Johnson, 2002). It is people at the very highest end of the weight spectrum that have seen the biggest increases in average weight of 11 to 13 kg. The effect of these average weight gains is that the bell curve for weight distribution in the population has shifted marginally to the right. Because of the positioning of the BMI cutoff points for each category, this small shift to the right has resulted in a large number of people gaining enough weight to move them from just below the cutoff points for ‘overweight’ and ‘obesity’ to just above the cutoff points, thereby resulting in the ‘doubling’ of ‘obesity’ rates (Campos et al., 2006). These small increases in weight combined with the crude nature of the BMI categorization system resulted in what appear to be major increases in ‘obesity’ prevalence rates over time.
Even given the limitations of the BMI categorization system, ‘obesity’ prevalence rates appear to have stabilized around the year 2000 in many parts of the world. A systematic review of 52 studies examined national trends in childhood, adolescent, and adult ‘obesity’ rates since 1999 (Rokholm, Baker, & Sørensen, 2010). Overall, the authors conclude ‘obesity’ rates for children, adolescents, and adults appear to have stabilized in many countries. Similarly, a data-pooling study by Olds et al. examined data from more than 500,000 children aged 2 to 19 years from nine countries between 1995 and 2008 and found that that there was no overall change in the prevalence of ‘overweight’ and ‘obesity’ in that time (Olds et al., 2011). The language used to describe trends in body weight is not reflective of actual changes in body weight over time, resulting in the suggestion that what we are suffering from is an epidemic of alarmist language (Basham & Luik, 2008; Boero, 2007; Campos et al., 2006; Gard, 2011b; Herndon, 2005; Rail et al., 2010). Basham and Luik (2008) argue that “the implications (of such alarmism) . . . for science policy and for evidence-based medicine dwarf those of any ‘obesity’ epidemic, real or imagined” (p. 244).
Determinants of Body Weight
The second set of critiques relate to the inaccuracy of describing body weight as a simple interaction between energy in and energy out. Physiological characteristics such as body weight result from complex interactions of genes, other biological factors, behaviors, life course experiences, and exposure to biophysical and socioeconomic environments (Gregg & O’Hara, 2007; Krieger, 1994; VanLeeuwen, Waltner-Toews, Abernathy, & Smit, 1999). It is commonly believed that people make conscious and voluntary decisions about eating and physical activity, and that these decisions are therefore able to be manipulated. However, scientific evidence suggests that such actions are largely controlled by a powerful biological system that regulates metabolic rate and the unconscious drive to eat and move (Bacon, 2010; Benton & Young, 2017; Fothergill et al., 2016; Friedman, 2009). It is possible for a person to make conscious behavioral choices that result in weight loss in the short term. However, the unconscious biological system ultimately prevails, and creates biological changes that ensure the body regains weight and returns to homeostasis.
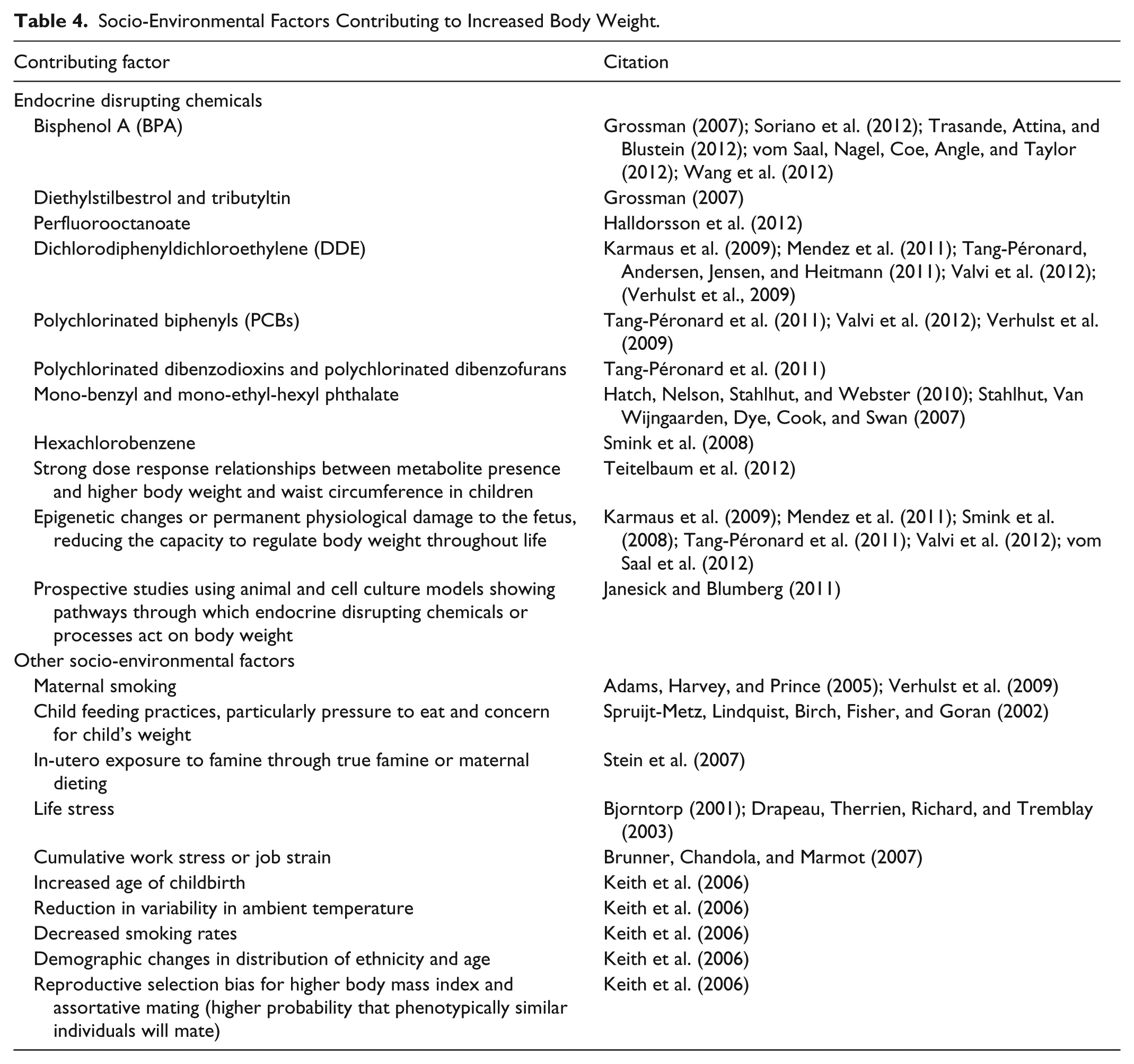
Variations in body weight between individuals in any given population are due to genetics, physiological factors, behaviors, and environmental exposures. The heritability of body weight is the relative contribution of genetics to the variability in body weight in a population. Research on monozygotic twins, non-identical twins, and siblings demonstrates genetic variation within the population accounts for between 70% and 80% of the variability in body weight (Friedman, 2009; Hsu et al., 2005; Wardle, Carnell, Haworth, & Plomin, 2008). This level of heritability is second only to height, and higher than heart disease, diabetes, and cancer, all of which are regarded as strongly heritable (Friedman, 2009). The relatively small increases in average body weight and the slightly larger increases for those in the fattest groups leading up to the turn of the 21st century may be due to the interaction between genetics, physiology, and the environment (Friedman, 2009). This review illuminated a significant number of physiological, behavioral, and socio-environmental contributors to increased body weight (Tables 3 and 4). A counter intuitive finding is that one of the strongest predictors of weight gain is engagement in weight loss dieting, regardless of the actual body weight of the dieter. In other words, dieting is counterproductive to weight loss. This issue is examined further in the section below on potential harms.
Physiological and Behavioral Factors Contributing to Increased Body Weight.

Note. PCOS = polycystic ovary syndrome.
Socio-Environmental Factors Contributing to Increased Body Weight.
In recent years, some of the ‘anti-obesity’ focus in public health circles has shifted from individual responsibility to the role of the so-called ‘obesogenic’ environment in enabling weight gain (Greener, Douglas, & van Teijlingen, 2010). The tenets propose that environments contribute to changes in nutrition and physical activity—referred to as the ‘Big Two’ by Keith et al. (2006)—by making ‘unhealthy’ behaviors the easy or default choice for people (Swinburn & Egger, 2004). However, this seemingly axiomatic relationship between ‘obesogenic’ environments and their purported behavioral correlates has only been tested in a small number of scientific studies. A systematic review of 28 studies showed that there was no association between ‘obesogenic’ dietary behaviors and the food environment (Giskes, van Lenthe, Avendano-Pabon, & Brug, 2011). However, living in a disadvantaged socioeconomic environment was consistently associated with so-called ‘poor’ dietary behaviors. Similarly, with respect to physical activity, systematic reviews have found ‘limited evidence’ of a relationship between the availability or use of active transport and overall physical activity levels in adults (Wanner, Götschi, Martin-Diener, Kahlmeier, & Martin, 2012) and children (Faulkner, Buliung, Flora, & Fusco, 2009).
In summary, the second set of empirical critiques of the WCHP relate to the inaccuracy of describing body weight as a simple interaction between energy in and energy out. Body weight results from complex interactions of genes, physiological factors, behaviors, life course experiences, and exposure to biophysical and socioeconomic environments (Gregg & O’Hara, 2007; Krieger, 1994; VanLeeuwen et al., 1999).
Relationships Between Weight and Health Outcomes
The third theme of inaccuracy relates to the depiction of relationships between body weight, morbidity, and mortality (Basham et al., 2006; Campos, 2004; Campos et al., 2006; Ernsberger & Koletsky, 2000; Gaesser, 2002; Gard & Wright, 2005; Mitchell & McTigue, 2007; Monaghan, 2005; Oliver, 2006; Pieterman, 2007). Life expectancy is the primary health indicator used at the population level. The claim that life expectancy is reduced as a direct result of body weight higher than the ‘normal weight’ BMI category (Nagai et al., 2012; Olshansky et al., 2005; Stewart, Cutler, & Rosen, 2009) is not supported by large epidemiological studies. The largest epidemiological study ever conducted followed 1.8 million people over a 10-year follow-up period and demonstrated an inverted U shaped relationship between BMI and life expectancy, with the highest life expectancy in people with a BMI between 26 and 28 (in the ‘overweight’ BMI category) and the lowest life expectancy in those with a BMI under 18 (in the ‘underweight’ BMI category). Those with a BMI between 18 and 20 (in the ‘healthy weight’ BMI category) had a lower life expectancy than those with a BMI between 34 and 36 (in the ‘obese’ BMI category; Waaler, 1984).
There is mixed evidence about the precise nature of the association between adiposity and all-cause mortality (Gaesser, 1999, 2003b). Some studies show a clear relationship at the extremes of the BMI distribution only—a U shaped curve—but even among these studies, the threshold at which the risk of mortality increases significantly is not distinct. Studies of nationally representative populations in the United States (Flegal, Graubard, Williamson, & Gail, 2005; Lantz, Golberstein, House, & Morenoff, 2010), Canada (Orpana et al., 2009); Denmark (Afzal, Tybjærg-Hansen, Jensen, & Nordestgaard, 2016); Japan (Tamakoshi et al., 2009); Japan, China, Korea, India, and Bangladesh (Zheng et al., 2011); and Hispanic people in the United States (Mehta et al., 2013) demonstrate a protective effect for the ‘overweight’ BMI category (compared with ‘healthy weight’ and ‘underweight’ BMI categories), and no or minimal effect on all-cause mortality for the ‘obese class 1’ BMI category (BMI 30 to <35).
A number of studies using large representative samples have demonstrated a flattened U shaped relationship between adiposity and cancer mortality, with the highest rates of cancer mortality in people in the ‘underweight’ and ‘obese class 2’ (BMI 35 to <40) BMI categories (Calle, Rodriguez, Walker-Thurmond, & Thun, 2003; Pischon et al., 2008). As with all-cause mortality, a BMI in the ‘overweight’ category confers a protective effect compared with a BMI in the ‘healthy weight’ category, even without adjustment for confounding factors such as physical activity, dieting, and weight cycling (Calle et al., 2003; Pischon et al., 2008).
Controlling for factors such as cardiorespiratory fitness or physical activity attenuates all-cause mortality risk associated with BMI, waist circumference, and percent body fat in healthy populations (Sui et al., 2007) and in populations with specific diseases such as diabetes (Ming, Gibbons, Kampert, Nichaman, & Blair, 2000). Active fat people have half the cardiovascular disease (CVD) mortality rates of sedentary people in the ‘healthy weight’ BMI category (Gaesser, 2003a; Wei et al., 1999). Fitness, and to a lesser extent physical activity, attenuates any relationship between fatness and all-cause mortality, CVD mortality, and CVD (Fogelholm, 2010).
There appears to be a stronger relationship between fatness and T2DM rates, and risk factors for CVD and type 2 diabetes mellitus (T2DM), but again, potential confounding factors are not controlled for in the majority of studies (Gaesser, 2010). Criticisms about the crude nature of BMI and the BMI classification system have resulted in mortality studies using other indicators such as waist circumference, percentage body fat, and metabolic syndrome. However, irrespective of the adiposity measure used, crude associations with CVD mortality are attenuated by physical activity or cardiorespiratory fitness (Blair & Brodney, 1999; C. D. Lee, Blair, & Jackson, 1999; D.-c. Lee et al., 2011; McAuley, Kokkinos, Oliveira, Emerson, & Myers, 2010; Wei et al., 1999). Other positive and negative lifestyle factors are potential confounding factors in the relationship between adiposity and mortality, and must be considered in any analysis (Gaesser, 2010). In addition to physical activity, positive lifestyle factors include being a non-smoker, consuming recommended levels of fruit and vegetables, and drinking alcohol in moderation. Negative lifestyle factors include weight cycling; unhealthy weight control behaviors such as skipping meals, smoking, purging, abuse of diuretics, and laxatives; and use of weight loss products and medications. Matheson et al. examined the relationship between the number of positive lifestyle factors and all-cause mortality across BMI categories using data from the US National Health and Nutrition Examination Survey (NHANES) III survey (Matheson, King, & Everett, 2012). Participants with four healthy habits were assigned as the reference group. The all-cause mortality hazard ratio for participants across all BMI categories with zero healthy habits compared with participants with four healthy habits was 3.27 (95% confidence interval [CI] = [2.36, 4.54]).
In contrast to studies demonstrating a positive relationship between body weight and mortality, there is a growing body of literature demonstrating the existence of an ‘obesity paradox,’ whereby a BMI in the ‘obese’ category is protective against mortality and morbidity. Gaesser cites a list of conditions that are less common in people in the ‘obese’ BMI category than in the ‘healthy weight’ BMI category: lung, stomach, colon and esophageal cancer, malignant melanoma, premenopausal breast cancer, chronic bronchitis, tuberculosis, mitral valve prolapse, anemia, type 1 diabetes, premature menopause, and osteoporosis (Gaesser, 2002, 2010). There are a range of cardiovascular conditions in which people in the ‘obese’ BMI category have a more favorable survival risk than people in the ‘healthy’ weight BMI category including aortic atherosclerosis (Barth, Maximilian Buja, Cao, & Brodsky, 2017; Brodsky et al., 2016), hypertension, heart failure (Komukai, 2012; Zapatero et al., 2011), percutaneous revascularization, coronary artery bypass graft surgery, treadmill referrals, peripheral arterial disease, echocardiography referrals, and co-morbid CVD and T2DM (Davenport et al., 2009; Doehner et al., 2012; Hong et al., 2012; Lavie, Milani, & Ventura, 2009; Raiszadeh & Travin, 2010; Sohn et al., 2011; Uretsky et al., 2010). A pooled analysis of five longitudinal studies looking at mortality risk of people with incident T2DM showed that for people in the ‘healthy’ weight BMI category compared with people in the ‘overweight’ and ‘obese’ BMI categories, after controlling for demographic characteristics, blood pressure, lipid levels, waist circumference, and smoking status, the hazard ratio for total mortality was 2.08, for CVD mortality was 1.52, and for non-CVD mortality was 2.32 (Carnethon et al., 2012). A meta-analysis of 20 studies involving more than 250,000 people showed a significantly lower risk of all-cause mortality in people with diabetes in the ‘overweight’ BMI category compared with people in the ‘healthy’ weight category (Gao et al., 2018). Other conditions for which people in the ‘obese’ BMI category have lower mortality risk than people in the ‘healthy’ weight BMI category include being elderly; having end stage renal disease and dialysis, advanced cancer, chronic obstructive lung disease, rheumatoid arthritis, or HIV/AIDS; undergoing lower extremity amputation or general surgery; and having high systemic concentrations of persistent organic pollutants (Davenport et al., 2009; Doehner et al., 2012; Hong et al., 2012; Lavie et al., 2009; Raiszadeh & Travin, 2010; Sohn et al., 2011; Uretsky et al., 2010). The ‘obesity’ paradox also exists for future morbidity. In a study of more than 20,000 people with recent ischemic stroke, after adjusting for confounding factors, people in the ‘overweight’ and ‘obese’ BMI categories had significantly lower risk of a major vascular event in the following 2½ years, compared with people in the ‘healthy weight’ BMI category (Ovbiagele, Bath, Cotton, Vinisko, & Diener, 2011).
‘Obesity,’ and sometimes even ‘overweight,’ are claimed to ‘cause’ or ‘lead to’ CVD, T2DM, some types of cancer, and osteoarthritis (Stewart et al., 2009). As with mortality, many studies have demonstrated an association between these morbidities and body weight, though others have not (Neeland et al., 2012). Similar to studies showing associations between fatness and mortality, studies that have shown associations between fatness and morbidities are criticized for failing to control for potential confounding factors. Physical activity, fitness, weight cycling, and diet history have all been demonstrated to be associated with adiposity, and are therefore confounding factors in any analyses of the relationship between adiposity and mortality or morbidity. A range of social factors such as poverty (Robbins, Vaccarino, Zhang, & Kasl, 2001), social class (Lawlor, Ebrahim, & Smith, 2002), and income (Raphael et al., 2010) are also associated with adiposity, and are therefore additional potential confounding factors in mortality and morbidity analyses. The Whitehall II Study of British civil servants demonstrated a strong inverse association between employment grade and the risk of metabolic syndrome (Brunner & Marmot, 2006), with only 10% of metabolic syndrome being explained by traditional risk factors. The biologically plausible explanation for this is that stress results in chronic inflammation. Chronic inflammation has been demonstrated to be an important risk factor for the development of T2DM, independent of body weight (Festa, D’Agostino, Tracy, & Haffner, 2002).
The other issue challenging the claim that fatness causes T2DM relates to temporal precedence, or the order in which conditions appear. For fatness to cause T2DM, the presumed cause (fatness) must appear prior to the assumed effect (T2DM); however, various studies have demonstrated that metabolic disturbances can be precursors to fat storage and weight gain (Morrison, Glueck, Horn, Schreiber, & Wang, 2008; Odeleye, de Courten, Pettitt, & Ravussin, 1997). In adults, insulin sensitivity after weight loss is strongly associated with subsequent weight gain (Yost, Jensen, & Eckel, 1995). For adults with two parents with T2DM, insulin sensitivity and insulin secretion at baseline both strongly predict weight gain over a 17-year follow-up period, after controlling for initial body weight (Sigal et al., 1997). The effect on weight gain was strongest for those with high insulin sensitivity.
In addition to the literature examined above on the so-called ‘obesity paradox,’ there is a growing body of evidence about the existence of people that are now labeled as ‘metabolically healthy obese’ (Sims, 2001), an ‘intriguing’ phenotype (Ortega et al., 2012) of people are considered to be ‘obese’ according to the BMI category but do not exhibit any ‘metabolic aberrations’ (Kuk et al., 2011). Various studies with nationally representative and other samples have demonstrated that the proportion of metabolically healthy people in the ‘overweight’ or ‘obese’ BMI categories can reach almost 50% (Iacobellis, Ribaudo, Zappaterreno, Iannucci, & Leonetti, 2005; Karelis, Brochu, & Rabasa-Lhoret, 2004; C. M. Phillips & Perry, 2013; Shin et al., 2006; Tomiyama, Hunger, Nguyen-Cuu, & Wells, 2016). Using the NHANES analysis, we calculated that the false positive rate for BMI as a tool to detect metabolic health across the U.S. population was 51%, and the false negative rate was 18%. A high false positive rate (low sensitivity) is problematic due to the psychological effect of a disease label and the burden and costs of repeated assessment, testing, and potentially unnecessary treatment. A high false negative rate (low specificity) is problematic when the disease is asymptomatic, serious, progresses quickly, and can be treated more effectively at early stages, or if the disease spreads easily from one person to another. Metabolic conditions can be asymptomatic and serious, and thus, the extremely high false negative rate for using BMI as the test is problematic. By all measures, the BMI is an extremely poor test to be used as a basis for public health policy and clinical interventions.
In summary, although having a body weight above the ‘healthy weight’ BMI category is said to result in poorer life expectancy, mortality, and morbidity, the evidence from the literature does not support this claim.
Ineffective
The second set of empirical criticisms focus on the ineffectiveness of the WCHP. According to critics, there is no evidence that weight loss programs at the individual level or ‘obesity’ prevention programs at the group, community, and population level are effective in achieving significant and sustained weight-related outcomes (Aphramor, 2010; Bombak, 2013; Ernsberger & Koletsky, 2000; Gaesser, 2009; Guthman, 2012; Ikeda et al., 2005; Kolata, 2007).
At the individual level, many weight loss studies demonstrate short-term success at reducing weight. However, critics argue that such studies generally suffer from a range of methodological problems including small sample sizes, underrepresentation of men, limited generalizability, a lack of blinded ascertainment of the outcome, a lack of data on adherence to assigned diets, and a large loss to follow-up (Simons-Morton, Obarzanek, & Cutler, 2006). Furthermore, critics argue that most weight loss trials do not have long-term follow-up, and so the results over the subsequent 2 to 5 years, when weight gain is most likely to occur, are largely unreported (Robison & Carrier, 2004). Where these results have been reported, weight loss programs have a long-term (2 to 5 years) failure rate of up to 95% (Gaesser, 2000; Mann et al., 2007). Weight loss is not only almost impossible for most people to maintain, but attempted weight loss strongly predicts weight gain (Lowe et al., 2006; Neumark-Sztainer, Wall, Story, & Standish, 2012; Pankevich, Teegarden, Hedin, Jensen, & Bale, 2010; Pietilainen, Saarni, Kaprio, & Rissanen, 2012; Stice, Presnell, Shaw, & Rohde, 2005). Between one third and two thirds of people who lose a substantial amount of weight on a dietary-based weight loss program will regain all the lost weight and more within 5 years (Mann et al., 2007). In addition to being ineffective at producing sustainable weight loss, dieting for weight loss programs do not necessarily result in improved health outcomes. A review of 21 long-term randomized-controlled studies found that weight loss diets lead to minimal improvements in cholesterol, triglycerides, systolic and diastolic blood pressure, and fasting blood glucose, and that none of these correlated with weight lost (Tomiyama, Ahlstrom, & Mann, 2013). Even some ‘anti-obesity’ researchers acknowledge that weight losses will, at best, average 3 to 4 kg after 2 to 4 years among financially well off, highly educated, carefully selected, enthusiastic participants in diet trials, and will be significantly less for people who are poor or uneducated (Katan, 2009). In response to yet another study demonstrating at best, moderate short-term effects, Katan (2009) editorialized in the New England Journal of Medicine that ‘We do not need another diet trial; we need a change of paradigm. . .’ (p. 924).
Likewise at the group, community, and population level, ‘obesity’ prevention programs have been demonstrated to be similarly ineffective. A 2011 systematic review and meta-analysis of 37 childhood ‘obesity’ prevention programs showed an overall mean BMI reduction of 0.15 kg/m2 (Waters et al., 2011). This reduction equates to a mean weight loss of between 0.1 and 0.3 kg, depending on the initial body weight of the child, and is insufficient to significantly reduce the proportion of children classified as ‘obese.’ There were no significant differences in effect based on age group, setting, length or type of intervention, or risk of bias based on randomization. A 2012 systematic review and meta-analysis of 30 ‘obesity’ prevention interventions focused specifically on increasing physical activity in children found similarly equivocal results (Metcalf, Henley, & Wilkin, 2012). The pooled intervention effect was small to negligible for total physical activity, and small to moderate for vigorous physical activity. The effect equates to about four more minutes walking or running per day. There were no significant differences in effect based on age group, BMI, study duration, setting, or quality of study. The authors conclude that these findings may help explain why ‘obesity’ prevention interventions are ineffective in reducing the BMI or body fat of children.
‘Obesity’ prevention programs focused on the adult population are also ineffective at reducing average body weight. A systematic literature review on the effectiveness of programs aimed at the general population, rather than ‘overweight’ or ‘obese’ people specifically, found only nine randomized control trials published between 1996 and 2006 (Lemmens, Oenema, Klepp, Henriksen, & Brug, 2008). Of these, only three studies that had follow-up periods of 1 year or more demonstrated any significant effect on BMI or other measures of adiposity. All studies involved women only, and were conducted with selective rather than representative populations. These studies provide the only evidence of any effect on adiposity, and yet despite their intensity, the results could best be described as modest.
Little evidence exists that reducing the so-called ‘obesogenic’ environment is an effective strategy for reducing the prevalence of ‘obesity’ either. One of the most widely touted interventions addressing the ‘obesogenic’ environment is the Arkansas Act 1220 of 2003: An Act of the Arkansas General Assembly to Combat Childhood Obesity (M. M. Phillips et al., 2010). Impact evaluation on the school environment demonstrated statistically significant improvements including requiring healthy options be provided for student parties and concession stands, banning commercial advertising by food or beverage companies, offering skim milk options for students in cafeterias, and reducing availability of vending machines during the lunch period and sodas in vending machines (M. M. Phillips et al., 2010). Despite these environmental changes, there was no change in the proportion of students in Arkansas in the ‘overweight’ or ‘obese’ BMI categories (Raczynski, Thompson, Phillips, Ryan, & Cleveland, 2009). Similarly, after 28 months of follow-up, the Louisiana Health Project found no significant difference in body fat and BMI in children in schools that introduced strategies to address the ‘obesogenic’ environment compared with the control group (Williamson et al., 2012).
This section has reviewed the literature on the evidence of effectiveness of weight-centered initiatives. The evidence of effectiveness of such programs is limited, and most weight-related public health programs have demonstrated no significant or sustained effect on levels of ‘obesity.’ Weight management programs focused on individuals are similarly ineffective at achieving sustainable weight loss or health improvements and, paradoxically, result in weight gain for most people. The findings from these empirical studies raise important questions about the ethics of recommending ineffective pursuits such as intentional weight loss (Bacon & Aphramor, 2011).
Harmful
The third set of empirical critiques draws on the evidence of harms arising from the WCHP including body dissatisfaction, disordered eating, weight cycling, weight stigma, and body size discrimination (Aphramor, 2005; Bacon & Aphramor, 2011; Bell, McNaughton, & Salmon, 2009; Catling & Malson, 2012; Cogan & Ernsberger, 1999; Cooper, 2010; Ikeda et al., 2006; Kassirer & Angell, 1998; Lawrence, Hazlett, & Abel, 2011; MacLean et al., 2009; Pieterman, 2007; Puhl & Heuer, 2010; Rees, Oliver, Woodman, & Thomas, 2011). Many of these issues have been written about extensively, and the presentation of empirical evidence relating to all of these harms is beyond the scope of this article. However, two of these issues will be explored in more detail: weight cycling and weight stigma.
As described above, most weight loss programs are not only ineffective, they are counterproductive. Diet failure often results in a higher weight than before the diet (Field et al., 2003; Lowe et al., 2006; Stice et al., 2005) and dieters gain significantly more weight than nondieters (Field et al., 2003; Neumark-Sztainer et al., 2012). Across the weight spectrum, the strongest predictors of weight gain in adolescents are dieting and unhealthy weight control behaviors, after controlling for binge eating, breakfast consumption, fruit/vegetable intake, physical activity, socioeconomic status, and initial BMI.
Although weight gain is not automatically an independent health risk factor, destabilized body weight entailing losing and regaining weight, otherwise known as weight fluctuation, yo-yo dieting, or weight cycling (Ernsberger & Koletsky, 1999), is strongly associated with negative health outcomes. A range of cross-sectional, prospective, and experimental studies provide evidence of associations between weight cycling and a variety of health outcomes (Table 5), including increased all-cause mortality, leading to the conclusion that “prescribed weight loss as a target for all-cause mortality reduction among the ‘overweight’ and healthy ‘obese’ is a failed concept both in terms of evidence for benefit and in terms of implementation” (Bosomworth, 2012; p. 521). The evidence of the range of harms associated with intentional weight loss and weight cycling suggests that it is a serious public health issue for people across the weight spectrum, including those in the ‘healthy’ weight BMI category (Montani, Schutz, & Dulloo, 2015), but it is rarely mentioned in ‘anti-obesity’ public health policies and programs.
Relationship Between Weight Cycling and Various Health Outcomes.

Note. CVD = cardiovascular disease; CHD = coronary heart disease; POP = persistent organic pesticides.
Weight-based stigma, or more broadly, weight-based oppression is both pervasive and insidious due to its internal and external sources (Puhl & Heuer, 2010). Internal sources of weight-based oppression include people’s internalized negative attitudes, values, beliefs, and behaviors related to body weight. External sources of weight-based oppression include exposure to stigmatizing or exclusionary social, cultural, economic, political, and built environments; weight bias and discrimination; and weight-based bullying and violence. In studies in the United States, weight-based discrimination has been demonstrated to have similar prevalence to race-based discrimination, with fatter and younger people being subjected to the highest levels of weight-based discrimination (Puhl, Andreyeva, & Brownell, 2008). Weight bias has been demonstrated to exist across all aspects of society (Alberga, Russell-Mayhew, von Ranson, & McLaren, 2016). Evidence of the psychological (Davison, Schmalz, Young, & Birch, 2008; Essayli, Murakami, Wilson, & Latner, 2017; Graham & Edwards, 2013; Griffiths & Page, 2008; Phelan et al., 2015; Savoy, Almeida, & Boxer, 2012), behavioral (Mustillo, Budd, & Hendrix, 2013; Neumark-Sztainer et al., 2002; Pearl, Dovidio, Puhl, & Brownell, 2015; Phelan et al., 2015; Schvey, Puhl, & Brownell, 2011; Storch et al., 2007; Vartanian & Smyth, 2013), and physiological effects of weight-based oppression is mounting. Physiological effects include higher blood pressure (Rosenthal et al., 2013; Unger et al., 2017), T2DM (Wirth, Blake, Hébert, Sui, & Blair, 2014), metabolic syndrome (Pearl et al., 2017; Wirth, Blake, Hébert, Sui, & Blair, 2015), allostatic load (lipid/metabolic dysregulation, glucose metabolism, and inflammation; Vadiveloo & Mattei, 2017), cortisol reactivity (Schvey, Puhl, & Brownell, 2014), and oxidative stress (Tomiyama et al., 2014). Stigmatizing discourses in public health ‘obesity’ prevention programs and policies have been demonstrated in a range of countries (Alberga et al., 2016; Fry, 2012; MacLean et al., 2009; O’Dea, 2005; O’Hara et al., 2015a, 2015b; O’Reilly & Sixsmith, 2012; Pederson, Haworth-Brockman, Clow, Isfeld, & Liwander, 2013; Piggin & Lee, 2011; White, 2012). As the theoretical and empirical evidence base about weight stigma has grown, so too has the call for the field of weight stigma to move beyond the focus on the individual and their experiences of weight-based oppression toward macro-social (Monaghan, 2016) or upstream, population level (Alberga et al., 2016) approach founded in social justice (Nutter et al., 2016).
Technical Critiques
The third major thematic category was technical critiques. This category related to critiques of the technical development and implementation of public health and health promotion policies and programs in the WCHP. Technical critiques included themes related to the use of a limited strategy portfolio, with behavior change and social marketing strategies being dominant (Bombak, 2013; O’Hara, 2014; Tylka et al., 2014; Walls, Peeters, Proietto, & McNeil, 2011), the role of health experts as policy and program drivers, and the absence of people with the lived experience of fatness (Carter et al., 2011; O’Hara, 2014), and the focus of evaluation on behavior change and body weight rather than health and well-being (Carter et al., 2011; O’Hara, 2014).
Consequences of the WCHP
Further analysis and distillation of the critiques described above revealed three major categories of consequences of the WCHP: an enhanced adipophobicogenic environment, reduced health and well-being, and reduced quality of life. The adipophobicogenic environment (O’Hara & Taylor, 2014) is an environment that creates and sustains fat phobia and oppression, including weight bias, prejudice, stigma, discrimination, bullying, violence, and cultural imperialism. Many of the critiques in the ideological, empirical, and technical categories contended that the medical and public health interventions enacted within the WCHP paradigm result in social, economic, policy, and built environments that sustain and heighten fat phobia and oppression. In turn, such fat phobic and oppressive environments contribute to reduced physical, mental, social, and spiritual health and well-being, and ultimately reduced quality of life for people categorized as fat and those who are in fear of becoming fat (Latner, Barile, Durso, & O’Brien, 2014; Salas, 2015; Vartanian & Porter, 2016). As such, it is posited that the WCHP is inconsistent with the values and principles of what has been termed modern, critical, or best-practice health promotion (Aphramor, 2005; Carter et al., 2011; Cohen et al., 2005; O’Hara et al., 2015a; Robison & Carrier, 2004).
Discussion
This study aimed to identify, critique, and synthesize the values, claims, and assumptions of the WCHP and to develop a comprehensive framework for describing the WCHP. Consistent with its roots in critical theory, the purpose of the framework is to serve as a heuristic for building competency to critique the WCHP, and thereby assist in challenging the dominant WCHP. The framework identifies the context, critiques, and consequences of the WCHP. The context includes the promulgators of the paradigm and the nine major tenets within the paradigm. The critiques of the paradigm include ideological, empirical, and technical categories, and each category includes three subcategories of critique. The consequences of the WCHP were synthesized from the critiques, and include the enhancement of an adipophobicogenic environment, and subsequent detriment to health and well-being and quality of life.
Despite the significant volume of critique about the WCHP, for those operating within the dominant paradigm or system, it is difficult or even impossible to imagine any other paradigm. Evidence contradicting the paradigm is either invisible to its proponents or rejected because it does not fit the dominant paradigm (Barker, 1993; Kuhn, 1970). This is known as the ‘paradigm effect’ (Barker, 1993). For those operating within the dominant paradigm, alternative paradigms are imperceptible or nonexistent. When data are presented that fall outside the paradigm, those within the dominant paradigm find these data hard to see and accept. The sheer strength of the dominant paradigm blinds its proponents to other possibilities (Barker, 1993; Gokhale, 2007; Kuhn, 1970). When the paradigm effect is so strong that it prevents the recognition of what is ‘plain to see,’ ‘paradigm paralysis’ has set in (Barker, 1993).
Paradigm enhancing innovations are easy for proponents of the dominant paradigm to see, but paradigm shifting innovations are difficult to envision. As such, although it is acknowledged that weight loss is almost impossible to maintain in the medium to long term and that weight cycling is damaging to health, public health authorities and health practitioners continue to recommend weight loss (paradigm enhancing) rather than maintaining stable body weight (paradigm shifting).
Dieting is recognized as contributing to weight gain, but in response to this knowledge, there are more calls for strategies to restrict false advertising and reduce crash dieting (Swinburn & Egger, 2004) (paradigm enhancing), without acknowledging the forces that lead people to diet in the first place (paradigm shifting). The Arkansas Act 1220 was named as one of the Top 25 Innovations in Government by Harvard University (Ash Center for Democratic Governance and Innovation, 2011) (paradigm enhancing), despite evidence that it has not resulted in any significant changes in childhood ‘obesity’ rates, and calls from advocates for strategies that have been demonstrated to enhance children’s health and well-being (paradigm shifting).
Some WCHP promulgators propose that increasing body dissatisfaction (via the creation of an adipophobicogenic environment) would motivate people to adopt healthy behaviors and to lose weight (Callahan, 2013; Heinberg, Thompson, & Matzon, 2001) (paradigm enhancing), despite evidence that demonstrates the ineffectiveness of such strategies and the harms associated with body dissatisfaction and its psychological and behavioral sequelae. In response to evidence that fat people are subjected to stigma, bias, prejudice, and discrimination, WCHP promulgators argue for weight loss to reduce the experience of oppression or tacit acceptance of stigma and discrimination because they are assumed to motivate people to lose weight (paradigm enhancing). In a bitter twist of irony, there is evidence of a direct causal pathway from weight stigma to weight gain, with or without changes in eating behavior as a mediator, which demonstrates that the adipophobicogenic environment is itself an ‘obesogenic’ environment: a fat hating environment makes people fat. Paradigm shifting strategies would focus on reducing the adipophobicogenic environment.
Kuhn believed that there are anomalies within all paradigms, but they are easily discounted as acceptable levels of error, or simply ignored. The anomalies within the WCHP have been ignored for many years, but as the body of evidence about them grows, they have been acknowledged not as error (paradigm shifting) but as the ‘obesity paradox’ (paradigm enhancing). But for how much longer can such errors and inconsistencies be explained as merely paradoxes?
Acknowledging problems or anomalies within a paradigm that cannot be reasonably explained is the beginning of a paradigm shift. According to Kuhn (1970), when enough anomalies accrue against the dominant paradigm, its proponents will be thrown into crisis. New ideas will emerge or old ideas re-emerge that will gain new followers and eventually challenge the old paradigm. The proponents of the old paradigm will begin to acknowledge the existence of competing ideas, but will seek to discredit them and their proponents. Gokhale (2007) postulates that social and business paradigm shifts are more likely to occur if the new paradigm is holistic, system focused, interdisciplinary, philosophical, healing, recovery oriented, and grounded in spiritual wisdom.
In response to the overwhelming body of critique of the WCHP, a new paradigm has emerged which shifts the focus from weight to well-being. One of the best known models within this paradigm is the Health at Every Size® (HAES®) model, (Health at Every Size and HAES are registered marks of the Association for Size Diversity and Health to prevent misappropriation of the terms for non-HAES oriented products or services; Association for Size Diversity and Health, 2014), which offers a health promoting and humane approach to weight concerns (Aphramor, 2010; Bacon, 2006, 2010; Bacon & Aphramor, 2011; Bacon, Stern, Van Loan, & Keim, 2005; Burgard, 2009; Kater, 2004; O’Hara & Taylor, 2014; Robison & Carrier, 2004; Tylka et al., 2014. HAES is a weight-inclusive rather than weight-normative model. In other words, the focus of the model is on health and well-being improvement, rather than labeling people according to normative categories of weight or BMI. Weight per se is sidelined, but not excluded. It cannot be excluded because of the significant role of weight stigma (both internal and external) as a health determinant, and the differential treatment of people in society and health settings based on their body weight. Society is not weight-neutral, and the contribution of such oppression to the health of higher weight people must be acknowledged. According to Tylka et al. (2014), the HAES model . . . challenges the current cultural oppression of higher-weight people. Specifically, the model seeks to end (1) the stigmatizing of health problems (healthism) and (2) weight-based discrimination, bias, and iatrogenic practices within health care and other health-related industries, as well as other areas of life. The model acknowledges that weight is not a behaviour or personal choice and that normal human bodies come in a wide range of weights and seeks alternatives to the overwhelmingly futile and harmful practice of pursuing weight loss. (p. 7)
The HAES model thus supports policies, processes, and environments that enhance the holistic health and well-being of people of all shapes and sizes. It does not propose that people are automatically healthy at any size, but that all people deserve fair access to opportunities and environmental conditions that will enhance their health and well-being, irrespective of their body size. Given its explicit focus on equity, the HAES model can be defined as ‘a social justice approach to improving the actions, conditions of living and environmental supports for the health and well-being of people at every size.’ Although it includes actions that can be taken by individuals (intuitive eating, joyful physical activity, body positivity), as a critical health promotion model (Gregg & O’Hara, 2007), HAES recognizes the significant limitations of a purely behavioral approach, and instead urges a focus on the social, economic, political, and physical environments that play a far more important role as immediate and underlying determinants of health and well-being. The HAES model includes values and principles that it supports as well as those it explicitly opposes (Association for Size Diversity and Health, 2014; Bacon, 2006, 2010; Gard, 2009; Kater, 2004; Robison & Carrier, 2004; Tylka et al., 2014; see Table 6).
Values and principles of the Health at Every Size model.

In the past 15 years, several studies have investigated the impact of HAES programs on various health and well-being indicators. Two systematic reviews (Bacon & Aphramor, 2011; Clifford et al., 2015) and a subsequent randomized-controlled trial (Mensinger, Calogero, & Tylka, 2016) have demonstrated that the HAES approach was more effective in improving various aspects of physiological, psychological, and behavioral factors than usual care or alternative treatment options. Other studies have shown that HAES curricula at the school and university levels led to improved body image, self-esteem, and eating attitudes in children (Kater, Rohwer, & Londre, 2002; Niide, Davis, Tse, & Harrigan, 2013); intuitive eating, body esteem, anti-fat attitudes, and dieting behaviors in university students (Humphrey, Clifford, & Morris, 2015); and knowledge, attitudes, beliefs, and skills in teachers (Shelley, O’Hara, & Gregg, 2010). Such evidence suggests that the HAES model is superior to the weight-centric approach at improving a broad range of health parameters. The HAES model responds to the critique of the WCHP and provides an evidence-based opportunity for significant paradigm shift (Barker, 1993; Kuhn, 1970).
Strengths and Limitations
This study was conducted within the constructivist epistemology (Crotty, 1998) in which the authors’ roles in conducting the study and constructing knowledge arising from the study is explicitly acknowledged. Other researchers may have constructed a different study, with a different interpretation of the results, dependent on their personal and professional interests, knowledge, and experiences. Further research is needed to test the utility of the WCHP 3C Framework for use as heuristic support for critical questioning and dialogue within and between practitioners, researchers, activists, and people in the community.
Conclusion
The WCHP is the dominant weight-related health paradigm throughout much of the world. Eating disorders therapist Jeanne Courtney captured the differences between the HAES paradigm and the WCHP in this reinterpretation of the light bulb joke (Courtney, 2010): How many weight loss experts does it take to screw in a light bulb? Three. One to stand on the ladder and keep trying to screw a burned out bulb into a socket that doesn’t fit, one to stand under the ladder and tell him he’s doing a great job, and one to write a press release declaring that the three of them have discovered a revolutionary, completely safe and effective new way to screw in light bulbs. How many Health at Every Size experts does it take to screw in a light bulb? The light bulb is fine, the socket is fine, the switch is on, and the room is brightly lit, but it still takes several dozen Health at Every Size experts, with impeccable academic credentials, to publish independent studies proving that there is no need to change the bulb. And those three guys with the ladder still won’t go away.
This study, culminating in the development of the WCHP 3C Framework for describing the context, critiques, and consequences of the WCHP, aims to assist in developing the critical competency of public health and health care professionals, and helps them to ‘step away from the ladder’ and shift their practice from a focus on weight, which has been demonstrated to be hard on people and soft on addressing health issues (Baum, 2016), toward a focus on addressing the socio-environmental factors that contribute to health equity for people of all sizes, an approach which is soft on people but hard on the determinants of health, and therefore results in better health and well-being for all.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.