
Abstract
The COVID-19 pandemic created an unprecedented global crisis as the virus affected many, and lives were restricted by public health measures. Public Safety Communicators (PSCs; e.g., 9-1-1 operators, call-takers, dispatchers) faced unique challenges in their work as the pandemic progressed with shifting workloads as well as requirements to continue to work and to work in-person. Moreover, PSCs were the person to call when there was a medical or public safety emergency during the crisis of the COVID-19 pandemic. Given extant literature already suggesting PSCs have a high prevalence of mental health disorders, we conducted an online survey of PSCs (n = 333) in Canada striving to interpret the nuance in PSCs experiences, with a focus on the effects of the COVID-19 pandemic. Responses to open-ended items were coded into four areas impacted: self-reported increase in stress, specific operational stresses and organizational stresses experienced by PSC during COVID-19, and the COVID-19 precautions implemented in communicator workplaces. Lessons learned from PSC experiences can be harnessed to better support essential crisis responses while maintaining and supporting employee wellness.
Plain language summary
The COVID-19 pandemic impacted the lives of people around the world as people became sick with COVID-19 and were impacted by public health measures put in place by governments. Public Safety Communicators (PSC: also known as 9-1-1 operators, call-takers, dispatchers) continued to work during the COVID-19 pandemic and experienced many changes to their workload. Furthermore, PSC were the person to call if there was a medical or public safety emergency during the COVID-19 pandemic. Before the COVID-19 pandemic research found that PSC have high screening rates for mental health disorders, so the research team conducted an online survey which allowed PSC across Canada to express their self-reported mental health with a focus on the impacts of the COVID-19 pandemic. In the survey participants were able to type in responses to prompts. Survey responses written by PSC were analyzed and four major categories were found: self-reported increase in stress, specific operational and organizational stressors experienced by PSC during COVID-19, and the COVID-19 precautions implemented in communicator workplaces. The researchers present these categories by using quotes from the written responses submitted by participants in their survey. This research can help to better support PSC in their job by finding ways to improve wellbeing.
Keywords
Introduction
The COVID-19 pandemic profoundly affected the global population, creating an unprecedented experience as the public was affected by the virus, and subsequent government regulations restricted citizens through imposed public health measures (Venkatesh, 2020). Varying degrees of fear, uncertainty, and stress defined the COVID-19 pandemic, particularly in the first phases when daily activities and social opportunities changed drastically (Paluszek et al., 2020). As easement of restrictions and threat level associated with COVID-19 fluctuated, further uncertainty and concerns of another wave of COVID-19 impacted the public (Paluszek et al., 2020).
In Canada, citizens experienced COVID-19 public health measures, including masking, testing, and contact tracing (Detsky & Bogoch, 2021). The government also implemented business-closures, stay-at-home orders, border, and travel restrictions (Detsky & Bogoch, 2020, 2021). COVID-19 restrictions impacted Canadian labor force participation, where the first 2 months of the pandemic were accompanied by a 32% decrease in employee weekly work hours and a 15% decline in employment, frequently affecting public-facing jobs (Lemieux et al., 2020).
Meanwhile, the perhaps underrecognized lifeline of citizens, public safety personnel (PSP; e.g., police, firefighters, paramedics, correctional workers), including public safety communicators (PSCs; e.g., telecommunicators, 9-1-1, call-takers, and dispatchers), continued their employment. PSC serve as a first point of contact (Ricciardelli et al., 2019), connecting citizens in distress with necessary medical or public safety responses. As such, we surveyed PSCs about their COVID-19 experiences, particularly asking about workplace stresses, occupational activities, and personal changes resultant from the pandemic’s onset, with the intention of better understanding PSC occupational health and learning how to better support PSCs in future pandemic events.
Operational and Organizational Stress
Sources of stress in employment settings can be best categorized as arising from either operational or organizational factors (Duxbury et al., 2015). Organizational stressors are contextual to the job such as interactions with management, workplace communication, and workplace support while operational stressors arise from the strain caused by the job content (Duxbury et al., 2015). In PSP populations, specific organizational cultures contribute to stress, as issues such as low support and high workload contribute to an overload in work demanded (Duxbury et al., 2015). Organizationally, leadership within PSC workplaces can affect PSC wellbeing (Leduc et al., 2023). Operational stressors are clear within PSP employment, as such work is accompanied by exposure to potentially psychologically traumatic events (PPTEs), which is associated with negative mental health outcomes for PSP (Carleton et al., 2019). Operational strains may also increase turnover rates within communications organizations (Sprigg et al., 2007) with rates found to be as high as 30% in some jurisdictions (Association of Public-Safety Communications Officials International [APCO International], 2018) causing staffing issues. To exemplify, a 2016 survey of Public Safety Answering Points (PSAP) in the United States found only 28% of PSAPs reported meeting authorized staffing levels for the entirety of the year, with a more common experience of 41% of PSAP being below authorized levels for a part of the year and 29% being below levels for the entirety of the year (APCO International, 2018).
There exists a paucity in investigations into occupational health impacts of the COVID-19 pandemic, with much scholarship focusing on physical aspects of workers health rather than mental or emotional factors (Hamouche, 2020). Lack of focus on workplace stressors from organizational and operational levels is a detriment to essential populations who continued to attend their workplace through the COVID-19 pandemic (Papazoglou et al., 2020), such as the PSP who played a critical role in supporting public safety.
The Role of Public Safety Personnel in Epidemic Response
PSCs play a critical role in disaster response including epidemic events where the physical and mental health of the public is threatened as occurred with H1N1 influenza (Tsubokura et al., 2010) and global severe acute respiratory syndrome (SARS) outbreaks (O’Sullivan & Phillips, 2019). During previous epidemics, researchers investigated impacts on frontline healthcare workers (HCW), finding increased exposure to illness and death from epidemics elevated the risk of experiencing symptoms of psychologically traumatic stress (Naushad et al., 2019; Wu et al., 2009), harming HCW’s well-being (Naushad et al., 2019). Similar studies on PSP are limited in comparison (Hamouche, 2020), creating a lacunae in knowledge given the differences in the roles of HCW and PSCs, the former maintaining public health while PSP maintain necessary social systems—most under the purview of PSCs— which society relies upon during epidemics (O’Sullivan et al., 2007).
Prior to COVID-19, PSCs faced elevated occupational and posttraumatic stress injuries due to their role, including exposure to PPTE (Carleton et al., 2019), and organizational stresses (e.g., staffing shortages, burnout and fatigue, and insufficient resources). COVID-19 introduced additional strain on PSCs (Heber et al., 2020) as, unlike many, PSCs were required to attend their workplace in-person (Papazoglou et al., 2020). Consequential fears of contagion to family members due to work attendance were intensified for some PSP by their requirement to interact with the public, further contributing to potential stress (Heber et al., 2020). PSCs, although not interacting frequently with the public in-person, did attend their workplace, interacting with peers while many in the world stayed home, becoming the lifeline between intervention and illness, risking infection while supporting the public.
Public Safety Communicators and the COVID-19 Pandemic
PSCs perform a foundational role in public safety ecosystems, being the first point of contact in emergency situations, wherein they support the public and other PSP by allocating resources to support positive public safety outcomes (Ricciardelli et al., 2019). PSCs are the lifeline for members of the public, bridging them to other supports while facing critical incidents in succession (often without knowledge of the outcomes), playing a critical role in public safety and health responses (Adams et al., 2015). PSCs are consistently exposed to PPTE, with such frequent and repeated exposure associated with increased risk of adverse mental health outcomes and mental health disorders (Carleton et al., 2019). A Canadian sample of PSP found that 44.5% of PSPs screen positive for a mental health disorder (Carleton et al., 2019), a prevalence much higher than diagnostic rates found in the general population (Government of Canada, 2019).
Anticipated exacerbation of stress in PSCs is likely with the onset of COVID-19, despite PSCs not having in-person interactions with the public, lowering risk of occupational exposure to COVID-19 (Wagner et al., 2022) compared to other front-line PSP. Rather, PSCs serve ahead of the front lines (Ricciardelli et al., 2019), where vicarious trauma becomes omnipresent. Moreover in 2020 as the first peaks of COVID-19 infections occurred internationally, increases in calls to PSAPs occurred (Al Amiry & Maguire, 2021; Marrazzo et al., 2020). For example, calls increased 1,900% in Israel in the first 3 months of the pandemic and 440% in the first 5 weeks of the pandemic to Northern Italy PSAPs (Al Amiry & Maguire, 2021). As workloads increased due to the pandemic, the potential for exposure to PPTEs and accompanying strain also increased. Lowered requests for dispatches for medical issues such as stroke or cardiac events prevailed, while out of hospital morbidity for such conditions increased, suggesting patient fears toward COVID-19 prevented them from calling 9-1-1 (Al Amiry & Maguire, 2021; Ong et al., 2021; Scquizzato et al., 2020) – potentially attributing increased calls to communications centers to COVID-19 related calls.
Researchers have analyzed PSAP calls to demonstrate the evolution of the pandemic drawing from jurisdictional mappings of PSC workload to create predictive models for monitoring pandemic progression and demand on frontline healthcare services, such as intensive care units (COVID-19 APHP-Universities-INRIA-INSERM Group, 2020; Gaubert et al., 2020). Despite the invaluable information and service provided by PSCs, limited research examines the personal occupational experiences of PSCs during COVID-19.
Current Study
We surveyed PSCs about their occupational wellness during COVID-19, striving to interpret the nuance in PSCs experiences and to interrogate how PSCs can better be supported in future crises. In keeping with previous occupational health work, theoretically we aim to analyze such occupational experiences of PSC, as they currently remain a rarely researched population. We aim to reveal empirically their occupational experiences specific to the challenges that accompanied the COVID-19 pandemic, to analyze how such challenges affected them, and changes that could be made to better support communicators.
Methods
We administered a 179-item online survey through the Qualtrics survey platform, intended to characterize the self-reported mental health of PSCs, and shed light on PSC occupational wellness. In the current paper, we unpack a section of three open-ended items focusing on the impact of COVID-19 on the PSC role. Here, we asked: “What does it look like since COVID-19 in your place of work?,”“How has COVID-19 changed your occupational responsibilities?,” and “What has changed, and what has stayed the same, because of COVID-19?.”
Recruitment occurred through the Association of Public-Safety Officials (APCO) Canada, through an email informing their membership of the study and sharing a link to the study entry page. Written informed consent was obtained from all participants at the beginning of the survey, and only those who gave additional consent for direct quotation in publication were quoted in the presentation of our results. Given not all PSCs are members of APCO Canada we also sent study information to interested PSC and their organizations. This could be considered a variant of snowball sampling (i.e., potential participants forwarding study information to other PSCs who are not members of APCO Canada), and our intention was to create a national sample. We also contacted provincial or territorial organizations responsible for PSCs to increase awareness of the study and invite participation.
Inclusion criteria requested participants be actively or previously employed as a PSC for police, fire, or ambulance services in Canada, including for OnStar or VoIP. The survey was available in English and French; thus participants could engage in either official Canadian language. The survey was open for participation from November 4, 2020, until April 30, 2021, which was during the COVID-19 pandemic. The Newfoundland and Labrador Human Research Ethics Board provided ethical clearances for our study (#20210168).
Participants
A total of 333 participants responded to at least one of the three items we analyze in the current study. Of our participants, 78.1% identified as women, 21.6% as men. Most self-identified as white (78.08%). Participants ranged from 22 years of age to 67, with a majority falling within the ranges of 30 to 39 (33%) and 40 to 49 (32.9%) years of age. Over half the participants graduated from a college or university (53.45%). Regarding occupational tenure, some were new to their current PSC role (i.e., with less than 1 year experience) with participants most frequently having been in their role for over 10 years (34.4%). PSC roles held by our participants included call-taker, dispatcher, supervisor, manager/commander, director/chief, trainer, and quality assurance/quality improvement (QA/QI). Some reported holding multiple roles, often both call-taking and dispatching. The age, gender, occupational role, and participant number (represented as “P#”) are included as identifiers to accompany participant quotes in our results section. For more information, we provide a summary of participant demographics in Table 1.
Summary of Participant Demographics (n = 333), With Response Categories Including Fewer Than Five Participants Omitted to Protect Participant Anonymity.

Analyses
We sought to identify emergent themes by taking a semi-grounded constructionist approach (Charmaz, 2006; Glaser & Strauss, 1967). We coded survey data using QSR NVivo, after first creating an inclusive and exhaustive codebook for each of the three items (i.e., responses were coded by item and each item had a somewhat unique codebook). Two independent coders created each codebook by refining categorizations of the data (i.e., codes). As more responses were reviewed, each coder was able to refine the codebook by adding, amalgamating, or disaggregating codes. The two coding schemes were aggregated into one, with any disagreements being resolved through discussion and consensus. The exhaustive list of codes was then analyzed into themes, with sub-themes through axial coding (Saldaña, 2013). To constitute a theme, the idea, interpretation, perception, experience, etc. had to be articulated across a group of unique participants.
Results
Participants frequently noted occupational changes resulting from COVID-19, (see Figure 1 for a graphical summary) reporting that “everything about how we do our job is different” (58, woman, supervisor, P217). Differences were operational (e.g., calls, response protocol, and workload) and organizational (e.g., work policies, staffing, management, hiring and training)—with the job transforming in how it was done but with performance requirements staying consistent. To explain, despite most participants reporting vast changes in how they do their job, what they did as their job—connecting citizens to public safety resources—did not undergo “much of a change” (51, man, dispatcher, P96). PSCs felt their baseline “operational functions have not changed” (36, woman, dispatcher, P19) as PSCs were “still required to perform all the same duties I had before” (31, woman, dispatcher, P62). Thus, the essence of the communicator role remained as the public “are still having medical emergencies that need to be addressed” (49, woman, dispatcher, P185).
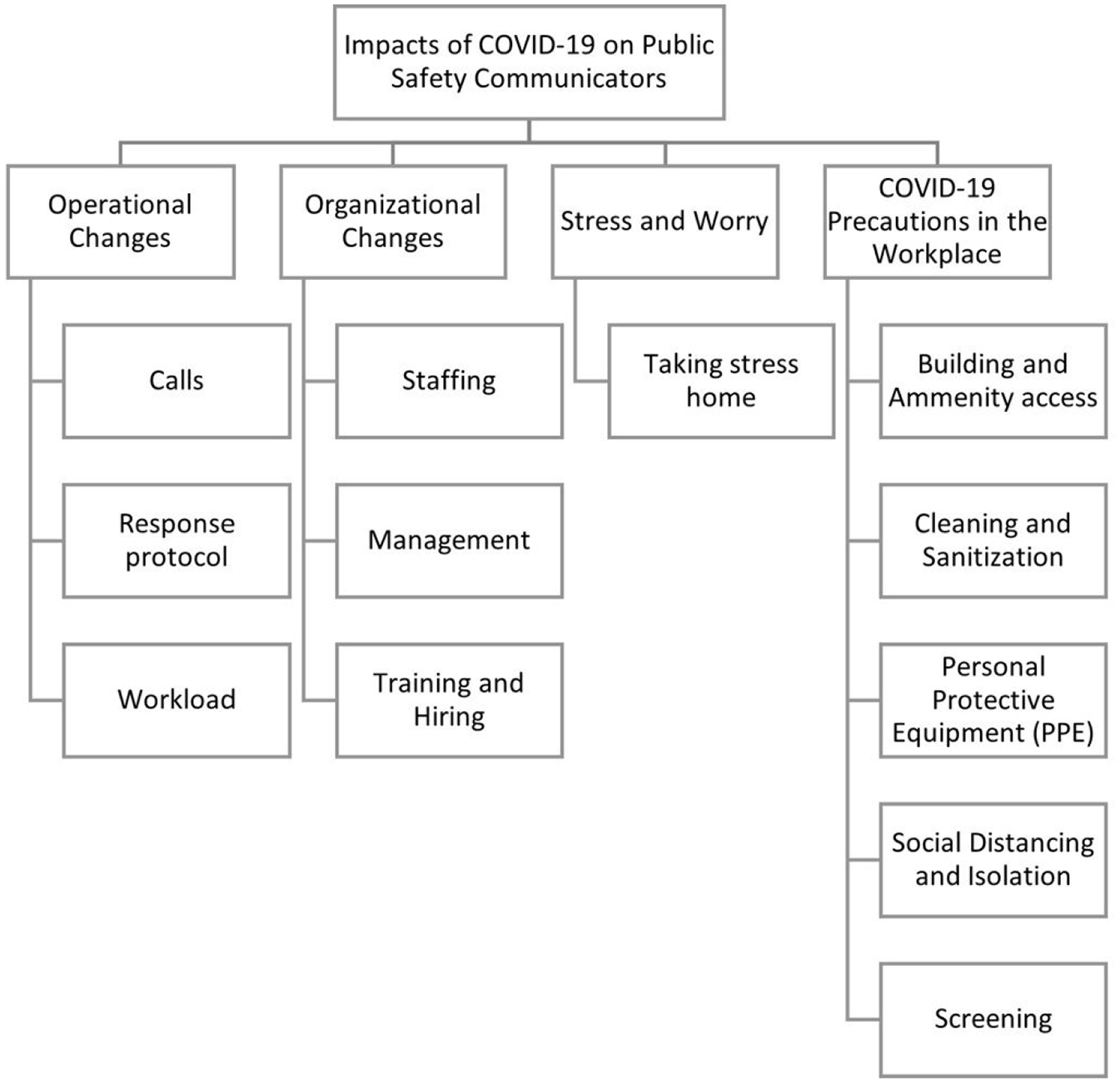
Major themes and sub-themes emerging from our analysis.
Outside of baseline operational responsibilities, some reported minimal change as the “same understaffing” (48, woman, dispatcher, P126) prevailed, along with noting that while “the job is still the same… (it is) the physical environment that has changed” (45, man, dispatcher, P81) due to COVID-19 precautions. However, a lack of impact was not the norm, as most participants felt shifts in their working life. In the current results, we first speak to the self-reported increase in stress experienced by PSCs, which was laced with worry for many. Next, we examine the operational and organizational stressors experiences by PSCs during COVID-19 and how such work stresses also informed their personal lives, particularly in light of public health measures and chronic exposure to the detriment of infection.
Operational Changes
Calls
Changes in experiences with callers, the foundation of a communicator’s work, were often mentioned. Respondents reported “many callers are uncooperative and some are downright verbally abusive” (48, woman, dispatcher/call-taker, P121), being “more angry and irrational than normal” (53, woman, supervisor, P166), “rude regarding the (COVID-19) questioning” (27, woman, supervisor, P222), and “more scared or hesitant” (44, woman, dispatcher, P406). Changes in caller behavior were attributed to callers being “more stressed and cooped together in bad circumstances when they call us” (35, woman, dispatcher, P95). Moreover, the attitudes of the PSP they worked with had changed, detailing that “responders are tired and short tempered” (44, woman, dispatcher, P406), which indirectly stressed communicators who recognized how PSP became entrenched in systemic concerns, such as “hospitals are dismissive of impacts of holding paramedics in (emergency departments)” (P406).
Participants reported that “call volumes have increased because some detachments/offices are closed” (52, man, director/chief, P143) along with detachments having “closed their front counters causing additional calls to the centre” (43, woman, supervisor, P15). The increased call volume may also be due to the rise of “new call types” (51, woman, supervisor, P112) such as COVID-19 related calls, including callers asking questions to communicators “that they should be asking (provincial) health services” (26, woman, call-taker/dispatcher, P184). Such calls involved “inquiries about government restrictions regarding COVID” (37, man, call-taker, P264), and calls “for advice, to discuss COVID (and) call for COVID complaints” (35, woman, dispatcher, P95). This created instances of “re-directing callers with questions to the correct phone number” (33, woman, call-taker/dispatcher, P403) leading to feelings that “public health seems to have shifted a lot of responsibilities onto us” (28, woman, call-taker/dispatcher, P374).
Another new hurdle faced by communicators involved enforcement of COVID-19 restrictions. This included “send(ing) officers to do curfew checks” (50, woman, dispatcher, P66), “resources being deployed to shut down parties” (51, woman, supervisor, P112), and “people wanting to report non-compliance” (26, woman, call-taker/dispatcher, P184). This was coupled with an “increased severity of calls” (53, woman, supervisor, P166), suggesting circumstances were increasingly dire with the emergence of a “higher ratio of complex calls” such as “mental health, addiction, and domestic abuse” (45, man, call-taker/dispatcher, P198). COVID-19 affected calls as the public was “stressed spending more time at home in domestic situations and using drugs and alcohol more” (35, woman, dispatcher, P95).
Response Protocol
The pandemic caused shifts in typical response protocols to address COVID-19 related challenges. Many communicators commented on “additional call taking screening questions” (34, woman, dispatcher, P32) where communicators “screen all callers with a list of COVID questions for calls in which (other PSP) need to attend” (34, woman, call-taker/dispatcher, P40). They “have to screen for covid symptoms even when callers are panicked or in an emergency and people get frustrated and scared” (39, woman, call-taker/dispatcher, P91). The new protocol caused callers to “get very frustrated” (P91) along with taking “more time to get through a call because of screening each caller” (35, woman, dispatcher, P47), leaving little time to “breath in between emergency calls” (40, woman, call-taker/dispatcher, P79).
The “many changes in protocols during calls for service from the public and dispatching (PSP)” (40, woman, supervisor, P303) led to changes in judgments made by communicators when responding to calls for service and dispatching PSP. For one respondent, COVID-19 protocols made it necessary to “base treatment decisions with covid in mind instead of what is best for the patient” (24, woman, dispatcher, P199). Concerns for their PSP counterparts dispatched to the physical scene of a call for service developed, as communicators are responsible for “ensuring the safety of all first responders on scene” (36, man, call-taker/dispatcher, P17), sometimes creating “stress around sending officers/paramedics into situations with confirmed or potential COVID” (44, woman, dispatcher, P116) as “no one wants to be responsible for spread that can be prevented by proper questioning” (49, woman, dispatcher, P185). However, at times PSCs found it challenging screening client with urgent crises at hand: “it’s extremely difficult to do a phone Covid screening for a screaming domestic or a stabbing etc.” (23, woman, dispatcher, P98). Thus, the protocol did not appear sensical and at times may have reduced PSC help provision capabilities.
Workload
COVID-19 increased occupational duties, with “many added responsibilities” (32, woman, trainer, P13) and a common experience of a “higher workload overall” (31, woman, call-taker/dispatcher/supervisor, P401). PSCs reported reduced breaks and downtime as “time on task has increased significantly” (45, man, call-taker/dispatcher, P198), resulting in work being “very chaotic for much of the shifts” as “there is no ‘down time’ anymore” (58, woman, dispatcher, P219). Workload increase, beyond call volume and screening protocols, included “more paperwork” (46, woman, call-taker/dispatcher, P226), “exorbitant amounts of emails” (32, woman, call-taker/dispatcher, P271), and “additional responsibilities to monitor the pandemic and spread amongst employees” (28, woman, call-taker/dispatcher, P420).
Organizational Changes
COVID-19, participants report, impacted the organization of PSAPs, informing staffing, hiring, training, and management. Respondents detailed frustrations, even hardship, due to changing organizational structures and the introduction of new processes and policies. Due to COVID-19, participants reported that “policies change frequently, sometimes more than once a day. Very stressful while still in a live environment” (45, man, supervisor, P140). Examples of changing policies included: “everyone staying at one desk instead of moving around” (32, woman, trainer, P31) meaning instead of how communicators “used to change stations every few hours, now (communicators) keep our station for the 12 hour shift” (36, woman, dispatcher, P19), changes to “how we come into the building” (33, woman, call-taker, P196), and inability to “have any non-essential personnel in the center” (52, man, director/chief, P1).
The roles of supervisors expanded to include “monitoring compliance for PPE [Personal Protective Equipment] and social distancing for my staff” (45, man, supervisor, P140) as well as staff monitoring to ensure adhere to public health measures, as detailed by P143, a 52-year-old man working as a director/chief: “I feel like I’m constantly ‘nagging’ about not becoming complacent. Further, I feel like I’ve had to worry more about employee’s & their personal lives, due to the potential negative impact it could have to work.” Such increased supervision over employees, bridging into concern for employees’ actions outside the workplace, created a novel challenge in organizational responsibilities for those in management positions.
Staffing
Impacts on staffing levels were felt by communicators during COVID-19 with many being “constantly short staffed” (32, woman, trainer, P13), given “people being sick and not being able to come to work due to mental health stresses or getting COVID tested due to themselves or people in household being sick” (26, woman, call-taker, P42). PSCs with children felt exacerbated hardship, due to competing demands impairing work life balance, as detailed by P153, a 35-year-old woman working as a call-taker: The staffing levels have fallen off the charts. When someone is symptomatic or has a symptomatic child at home to care for, instead of being off work for a day or two, that person is off for 10-14 days. That has a serious effect on staffing and morale.
Being ill prevented PSCs from attending work (e.g., “as soon as they have even 1 cold or flu symptom” (37, woman, trainer, P193)), which was a change from a culture of “toughing it out” (37, woman, trainer, P193) where PSCS came into work despite illness. With “more staff (being) respectful about not coming to work sick” (37, woman, call-taker/dispatcher, P88), there was a “massive increase in sick time being used” (33, woman, dispatcher, P252), affecting staffing levels, leaving a “skeleton crew…creating more work for remaining workers” (40, woman, call-taker, P256). Compounding reduced staff was how “morale has gone down,” which was attributed to “dwindling staff levels” (32, woman, call-taker/dispatcher, P271).
Measures to combat staffing shortages placed additional strain on communicators, with shift structure changing to, “split shifts” (34, woman, call-taker/dispatcher, P28) for some (i.e., working two shifts per day) including “split shifts between two work centers” (P28). This impacted PSCs abilities to meet personal obligations (e.g., “We cannot do anything everything is closed, need to adapt to one schedule that government is implementing (store hours) very hard to make errands as a shift worker now” (25, woman, call-taker, P9)). Others reported “overtime needs have increased” (42, man, dispatcher, P277) and “vacation approved was diminished” (36, man, call-taker/dispatcher, P17), creating additional sources of stress and fatigue. A phenomenon of taking “vacation time away for indeterminant amounts of time…in the name of unprecedented times” (29, woman, call-taker, P10) left staff unsure if “they have their days off or not” (40, woman, call-taker, P256), particularly straining parents facing “pressure to be there and get a sitter even when kids are forced to isolate” (46, woman, call-taker/dispatcher, P157).
Management
Novel “management issues” (36, woman, call-taker/dispatcher, P271) resultant from COVID-19 included “less management contact” (59, woman, supervisor, P149) between employees and management, and “less support on site with management working from home” (38, woman, supervisor, P210). The introduction of “admin/management working from home” left a PSC to write “haven’t worked with a supervisor in the room for over 6 months which is challenging” (26, woman, call-taker, P42). Thus, in the midst of an epidemiology crisis, PSCs perceived a lack of leadership.
Training and Hiring
During COVID-19, “training and hiring is very difficult” (43, woman, supervisor, P15). PSCs reported “challenges in training new people” (32, woman, call-taker/dispatcher, P271) while practicing “physical distancing” (50, man, dispatcher, P280) and training being “cancelled” (37, woman, trainer, P193). “Face-to-face” training was “limited,” such that “new changes implemented need to be self-taught” (27, woman, call-taker/dispatcher/trainer, P169). As an alternative to in-person training some courses were “online and self-directed” (53, women, dispatcher, P52).
Stress and Worry
COVID-19 created “anxiety in the workplace” (26, woman, call-taker, P42) and at home (e.g., “I am more careful when going grocery shopping/errands and stay home as much as I can to ensure I do not get sick” (29, woman, dispatcher, P139)). PSCs self-described being “more anxious” (54, woman, call-taker/dispatcher, P51), however this anxiety varied in intensity (e.g., “certain co-workers are more sensitive to the covid outbreak, so you have to be careful not to offend” (48, woman, dispatcher, P142)). Stress resulted largely from the threat of COVID-19 for dispatched public-facing PSP (e.g., “more danger placed on my officers means more stress for me” (44, woman, call-taker/dispatcher/supervisor, P275)) and the newly introduced caller screening measures (e.g., “increased stress due to screening questions agitating callers” (40, woman, supervisor, P303)).
Some participants such as P151, a 54-year-old man working as a supervisor, worried about contracting COVID-19: I think about COVID constantly. It’s the first thing I think about when I wake up and the last thing I think about when I fall asleep. I wish others took it as seriously as I do. And I wish politicians would listen to the doctors who know what’s coming. I watched my mother die from pneumonia as her lungs filled with fluid so I know exactly what all those poor COVID patients are in for. My god respiratory failure is an awful way to die. I wish it caused your brain to catch fire or lizards to jump from your chest because I’d deal with that way better than I’m dealing with this.
The worry, as evidenced in P151’s words, left some co-workers to feel “suspicious and judgemental of how others conduct themselves outside of work” (32, woman, dispatcher, P426). Working in-person left others concerned about bringing the virus home. The stresses and worries intensified with the ever-changing public health measures and, consequently, the job.
Taking Stress Home
Communicators reported alterations in their out of work behavior, influenced by their PSP role as described by one communicator: “As an emergency employee/essential employee, I am more careful when going grocery shopping/errands and stay home as much as I can to ensure I do not get sick” (29, woman, dispatcher, P139). This sentiment was echoed by another respondent who detailed the importance of “making sure we don’t do anything to come in contact with a covid positive case to make sure we are fit for duty” (25, woman, call-taker/dispatcher, P174). Alterations in behavior outside the workplace meant missing out on events or activities due to the COVD-19 pandemic, as described by P368 “I cannot see my parents, kids, or grandchild in person. My Dad died alone in a nursing home because I was unable to visit. I do not go into stores, restaurants or any other commercial establishments” (54, woman, supervisor). These changes caused communicators to lack “opportunities to relax/destress” (27, man, dispatcher, P411) and “decreased self-care activities” (25, woman, call-taker, P9), with P426, a 32-year-old woman working as a dispatcher, detailing harms on their ability to manage workplace stress: Nothing is the same. The biggest loss is not being able to cope in the healthy ways I used to (i.e. yoga class, gym, social gatherings, spending time with family). It is far more difficult to manage workplace stress without this foundation.
COVID-19 Precautions in the Workplace
To limit COVID-19′s spread, communicators reported “added protocols to protect workers at work” (29, man, dispatcher, P205), with public health measures equating to “more restrictions” (56, woman, manager/commander, P189). Adherence was widespread (e.g., “stricter guidelines for us all personally, which is fine. We need to protect each other” (58, woman, dispatcher, P219)) pushing PSCs to put “more thought into how to safely modify the fun things (communicators) usually do” (33, woman, dispatcher, P268). Restrictions were tied to PSAP access, sanitation measures, PPE, physical distancing, and screening.
Building and Amenity Access
PSCs reported changes in building access and workplace amenities encountering “cordoned off areas” (34, woman, dispatcher, P32) with “certain parts of the building closed down” (47, woman, call-taker, P381). One participant noted that “access to gyms have changed” (39, woman, call-taker/dispatcher, P131) distressing some communicators (e.g., “inconsistent or discontinued use of the gym facilities at work. This is my number one stress release and it’s been taken out of my control” (42, man, dispatcher, P359)). When arriving to work, some communicators had “to use a different entrance” (50, woman, dispatcher, P66) and adhere to new protocols for building access (e.g., “you can only access the building through one door. They take temperature and ask screening questions” (49, woman, dispatcher, P185)). Access restrictions reduced interactions with non-essential staff, with “signage indication to all nonessential staff (that they) are barred from the communications center” (37, man, call-taker, P264).
Cleaning and Sanitization
Participants explained “increased cleanliness” (43, woman, dispatcher, P2) at work, where maintenance of cleanliness included “hand sanitizer and cleaning wipes at all workstations” (46, man, manager/commander, P5), “disinfect(ing) stations before and after shift” (36, woman, dispatcher, P19), and “extra hand hygiene” (28, woman, call-taker/dispatcher, P30). Some PSAPs used “a hospital grade UV air scrubber machine” (33, man, dispatcher, P90) to combat viral spread. New measures meant some PSCs had “to come in a little earlier than our scheduled shift now to screen in and disinfect the console” (36, woman, dispatcher, P19), which was “exhausting constantly sanitizing” (31, woman, dispatcher, P62). Some benefited from being issued their own “personal keyboard and mouse” (49, man, supervisor, P320).
Personal Protective Equipment (PPE)
Mandated PPE created discomfort and difficulties, including “wearing masks” (44, woman, call-taker/dispatcher, P359), which were required except “when seated at our desk or sitting down while eating (for trainers this means masks all the time essentially)” (32, woman, trainer, P13) or, even, “100% of the time” (47, woman, trainer, P4). In consequence, PSCs were at times dehydrated (e.g., “not drinking enough water through the day” (41, woman, call-taker/dispatcher, P64)) and expressed masks were “somewhat stressful” and “annoying” (56, woman, supervisor, P80). Other PPE measures involved “visors during coaching/direct supervision” (35, woman, call-taker, P153) and “gloves” (45, woman, call-taker, P298), making their occupational responsibilities more difficult to complete.
Physical Distancing and Isolation
Similar to precautions implemented for the general public, mandated “staff social distancing” (43, woman, supervisor, P35) occurred. Many described “barrier devices on the workstations” (46, man, manager/commander, P5) which caused communication issues between co-workers (e.g., “have to be louder to hear and be heard by coworkers through the boundaries” (53, woman, dispatcher, P52)). Staff were also moved – they were “separated – police dispatch is being done at the main office. Fire dispatch is being done at our back up site” (50, woman, dispatcher, P66). Virtual meetings increased and “many people (were) working from home” (40, woman, call-taker, P256). Some described availing of a remote position as a positive (e.g., “I was able to work from home and it was so great. Less stress on my family because I’m a solo parent and my kids were home” (46, woman, 911 systems analyst, P106)), while others found remote work isolating. This was intensified by reduced interactions with colleagues (e.g., “socializing at work is limited due to physical distancing requirements and attempting to ensure ‘contacts’ are kept to a minimum” (52, man, director/chief, P143); “no celebrations or treats allowed in the centre” (40, woman, call-taker, P256)). As P303, a 40-year-old woman working as a supervisor said: “COVID-19 has taken away the well needed trips and social lives of employees, the time that we take to get away from the job and reset.” As a result, morale dissipated (e.g., “team building non-existence” (59, woman, dispatcher, P312).
Screening
Self-screening required for attending work occurred with PSCs’ recounting having to “pre-screen COVID-19 questions when starting (their) shift” (36, man, call-taker/dispatcher, P17), attend “a station at the entry door where we must have our temperature taken” (63, woman, supervisor, P103) and for some “supervised handwashing upon entering the building” (44, man, dispatcher, P362). In consequence, for PSCs, “it takes slightly longer to get set up at start of shift due to screening myself prior to start” (46, woman, dispatcher, P311).
Discussion
While the general population’s experience of job loss and reduced work hours (Lemieux et al., 2020) may not be reflective of PSC experiences, PSCs did experience COVID-19 informed change in their working lives. Their occupational experiences showed transformation in efforts to counterbalance the risks of COVID-19. Theoretically, we posit that strain resultant from operational and organizational factors associated with COVID-19 within the occupational environment had negative effects for PSCs. Reflecting on previous occupational health knowledge, we found PSCs experienced additional stress while not having the resources available to meet the demands of a challenging situation (see: Meurs & Perrewé, 2011). We show PSCs’ strain and stress from the imbalances (Meurs & Perrewé, 2011) in control and demands (see: Karasek, 1979), between effort and rewards (see: Siegrist, 1996), and between resources and demands (see: Lazarus, 1991 and Hobfoll, 1989; see also Chen et al., 2015) were brought forward during the pandemic. Specifically, operational and organizational shifts due to COVID-19 contributed to less control and higher demands on PSCs, all while being attenuated by the already low resources and low rewards afforded.
Empirically, we drew from open-ended survey data to show that PSCs faced hardships during the COVID-19 pandemic due to factors including additional operational strain, rapidly changing organizational policies, and COVID-19-specific workplace demands due to remaining in-person with little reprieve. In terms of employment impacts in our sample, division was found between operational and organizational changes. Operationally, the performance of a PSC’s role was impacted, which required an evolution of their role and responsibilities as the pandemic progressed. This potentially created a loss of control for PSCs within their working life as the foundation of their work changed, beginning with the calls for service answered and callers themselves. Instances of caller’s attitudes and emotions changing and subsequent negative experiences with abusive callers raised possibilities of PSCs facing increased stress, a factor found to impact PSC in pre-COVID-19 samples (Adams et al., 2015; Sprigg et al., 2007). Exposure to abusive callers may result in emotional exhaustion, anxiety, and depersonalization for PSCs, alongside increased staff turnover intent (Sprigg et al., 2007). Added strains which potentially contribute to already present occupational issues creates concern for occupational health of such workplaces, especially as public health disasters are being navigated.
The type of calls PSCs fielded also diversified, with PSCs experiencing a higher call volume from citizens with questions about COVID-19, including queries about the virus, public safety measures, and reporting other citizens who were not following regional COVID-19 restrictions, which added to their responsibilities for upholding public health measures, increasing their already demanding workload. Such experiences of fielding more calls than usual can contribute to post-shift worry and irritability (Hoang et al., 2022), creating risk for the negative emotions of the job following PSCs home. Another shift in call type identified was a reported increase in severe calls, namely mental health and domestic abuse calls, further placing demands upon PSCs coupled with loss of control in their working experiences. These increases are in alignment with reports of deteriorations in societal mental health during COVID-19 and increased domestic violence occurrences as a result of isolation (Béland et al., 2020). With severe calls causing risk of vicarious trauma (Adams et al., 2015) and increases in PPTE exposure (Carleton et al., 2019) negative impacts to well-being and mental health outcomes are an exacerbated concern for occupational health conditions in this population.
In reaction to novel challenges created by COVID-19, respondents reported a shift in response protocols, which further changed their operational role. PSCs who received calls from members of the public had to screen patients for COVID-19 symptoms (an added measure to protect PSP who may encounter the civilian as dispatched by a PSCs). Screening was required regardless of the call’s circumstance, causing PSCs to face further frustration from callers who were not calling about COVID-19 and led to difficulties when responding to panicked callers, further provoking abusive callers who disapproved of the screening protocols.
The culmination of increased calls to PSAPs and additional screening steps contributed to increased demands placed upon PSCs. Time to decompress dissipated as new response protocols increased time-on-task and an upturn in calls lowered down-time between call-taking. As work-tasks of PSCs are correlated with elevated levels of the stress associated hormone cortisol (Weibel et al., 2003), the lack of downtime between tasks, and prolonged attention to such tasks raises concern of allostatic load, or wear and tear on the body, given the prolonged stress exposure (McEwen, 1998), threatening occupational health. The frequent and repeated exposure to PPTE, such as severe calls for service, is further associated with negative mental health outcomes such as mental health disorder development (Carleton et al., 2019).
Similar to operational demands, organizational changes were numerous, creating a lack of control as changes affected management, training and hiring practices, and staffing. At times, policies were interpreted as rapidly changing, thus creating an unstable working environment. Even elements of the job that should be benign or that emerged as a method of coping with the role, such as where PSCs sat for the duration of their shift, were made stressful (i.e., new restrictions on movement with workplaces or regarding visitor protocols), contributing to further discomfort in the workplace.
PSAP supervisors found ensuring organizational standards were achieved difficult. Some were required to take on an enforcement role to uphold COVID-19 protections, opening the door for conflict with staff. This also extended outside of the workplace, with supervisors experiencing worry about what employees were doing while off-shift, fearing their out-of-work actions could cause workplace spread of the infection. New sources of stress, induced by COVID-19, within organizational management level are likely to have trickle-down consequence to the employee: unpopular regulations and management level strains created uncertainty, compromising occupational wellness (Adams et al., 2015).
Reported training and hiring challenges exacerbated the highly unstable occupational environment of PSAPs, which already face high turnover (APCO International, 2018). COVID-19 outcomes reported by our participants (i.e., increases in abusive callers) had the potential to exacerbate turnover (Sprigg et al., 2007), and when compounded by reported deficits in hiring and training capabilities, may have further strained staffing levels. As society relies upon PSCs as the foundation for public safety response, especially in a public health emergency (O’Sullivan et al., 2007), staffing strains and training impediments can negatively affect communities served, and harm PSCs who are left to cover an understaffed workplace.
Stress and worry surrounding the COVID-19 pandemic and the potential of contracting the virus were frequently reported by our sample, similar to effects found in the general population (Paluszek et al., 2020). Much of the stress was experienced in the workplace for PSCs, along with reports of stress following them home from the workplace, as considerations of the interaction between COVID-19 and their employment encroached into their daily lives. The need to remain fit for duty by undertaking increased responsibility to remain healthy and free from COVID-19 contact was strong, potentially from both a sense of social responsibility to uphold public safety in their community and in their workplace which may have faced staffing challenges and increased call loads. The decreased ability to engage in coping practices due to COVID-19 restrictions (i.e., participating in social or physical activities) impacted PSCs’ opportunities to de-stress while off the clock. Such activities are critical for PSC well-being (Coxon et al., 2016) as PSP are more likely to avail of non-professional supports, such as personal coping methods, only turning to professional resources as a last resort (Carleton et al., 2019).
PSCs’ workplaces underwent many operational and organizational structure changes in response to the COVID-19 pandemic. Our respondents reported a myriad of precautions implemented to mitigate workplace spread of COVID-19. Though such precautions were valuable in restricting viral effects on workplaces, the potentially cumulative impacts from the many additional demands upon employees negatively impacted PSCs’ occupational well-being. Restrictions placed upon rewarding aspects of the job such as closed fitness centers and reduced social interactions with colleagues, contributed to social isolation, and potentially poor occupational health due efforts made in the workplace not being met with adequate rewards for workers (Siegrist, 1996). Physical distancing between PSC and their co-workers by changing the layout of communications centers or adding physical barriers further contributed to reduced social opportunities, likely impacting PSCs well-being as social isolation relates to negative impacts upon mental health and overall wellness (see Pancani et al., 2021; Pietrabissa & Simpson, 2020).
Some workplace COVID-19 precautions introduced meant additional responsibilities placed upon PSCs to prevent the spread of COVID-19. While of similar importance to screening patients for COVID-19 to maintain public health, such precautions added steps to a PSC’s day, increasing their workload and responsibilities, while available resources remained scarce including staffing issues and available supports, a further detriment to occupational health conditions Hobfoll, 1989; Lazarus, 1991). Mitigation steps such as frequent cleaning and pre-work screening for COVID-19 imposed PSCs with more required tasks, beyond an already busy role (e.g., needing to attend their shift earlier or stay later to ensure pre-shift screening was completed, on-shift cleaning of their stations occurred).
Overall, the COVID-19 pandemic caused change within operational and organizational facets, along with personal impacts to communicators as stress and worry accompanied the pandemic, all exacerbated by their burdensome role of supporting the public in a time of high uncertainty and stress. Though respondents reported many changes, including some aiming to protect from COVID-19 viral spread, discussions of occupational supports or programing to help PSCs navigate their role during COVID-19 were not present. This lack of positive and supportive experiences for PSCs is of importance as we recognize that wellbeing is more than simply the absence of negative states but should also include the presence of positive states of being (Meurs & Perrewé, 2011). The lack of support, and recognition, for PSC well-being at a time when their definition of essential was never so applicable highlights how PSCs are too often overlooked. As such, the often-forgotten PSC population deserves acknowledgment for their contributions to public safety—especially during times of crisis—along with improved supports to suppress the manifestation of burnout, deterioration of wellness, and turnover intention in already unstable workplaces. By taking lessons learned from COVID-19, changes can be made to PSC workplaces to ensure that in future public safety disasters, including pandemics, the occupational health of essential PSP workers is supported, thus protecting public safety systems, and supporting communities served by such systems when they are needed most.
We do caveat, a survey was used, thus participant responses are limited by how individual participants interpreted questions—a current study limitation. We did not complete interviews, therefore we could not probe for additional information. Future work, we recommend, should employ qualitative methods such as interviews to allow for achievement of depth in responses to gain richer data.
Conclusions
The COVID-19 pandemic provides a major opportunity for creation of foundational knowledge for the next potential public health disaster that impacts our communities. Our findings show that impactors of the COVID-19 pandemic were diverse, with some mirroring stain felt by the general population, such as the stress and worry that accompanied navigating the COVID-19 pandemic. Many other factors were more specific to the unique role held by those deemed essential workers within public safety systems, such as PSCs. These included the operational and organizational changes occurring in response to COVID-19, leading to increased workloads, changes in protocols, changes in caller emotions and attitudes, staffing and training challenges, and challenges with communication between staff and management. A multitude of COVID-19 precautions also changed the workplace experience of PSCs (cleaning protocols, PPE, social distancing, screening, and building access). Lessons learned can be harnessed to create better protocols for supporting the occupational health of essential workers facing such disasters including PSCs. By supporting PSCs, communities they serve will also be better supported, contributing to overall health and well-being for all. PSC also deserve to be supported as their work directly impacts all facets of public safety responses due to the foundational nature of their role (Ricciardelli et al., 2019).
Footnotes
Acknowledgements
We would like to thank the Association of Public Safety Communications Officials Canada for their support of this project, and all the Canadian public safety communicators who voluntarily participated in our study.