
Abstract
Women’s autonomy is a potentially noteworthy but less studied indicator of women’s control to exercise reproductive rights in a patriarchal country such as Bangladesh. The study is a sociological investigation that examined whether women’s autonomy matters or not in determining their control to exercise reproductive rights in rural Bangladesh. A survey was conducted on 200 randomly selected married women from Hogladanga village in the Bagerhat district of Bangladesh. We administered an interview questionnaire containing 27 Likert-type questions under three mutually interlinked domains for autonomy measures and 12 Likert-type questions under two mutually interlinked domains for reproductive rights status measures. The findings revealed that women’s autonomy status is strongly associated with their control to exercise reproductive rights status (β = .862, p < .001) along with both of the proxy variables, that is, sexual behavior index (β = .915, p < .001) and reproductive behavior index (β = .62, p < .001). The study findings suggest that women’s autonomy must be considered an important sociocultural determinant of higher control to exercise reproductive rights for young mothers in Bangladesh.
Keywords
Introduction
Because of their relationship to an individual’s reproductive functions, reproductive rights are considered legal rights (Amnesty International [AI] USA, 2007; World Health Organization [WHO], 2014), which ensure women’s freedom to decide when to have children as well as the spacing and timing of their children’s births (WHO, 2006). To a great extent, a woman’s participation in fertility behavior is dominated by males, especially her husband and his family, due to the male supremacy in a patriarchal society (Jesmin & Salway, 2000; M. E. Khan, Townsend, & D’Costa, 2002; Sebstad & Cohen, 2000). In rural Bangladesh, the reproductive situation takes its worst form (Ahmed, 2005; Hussain & Khan, 2008; Rashid, 2006) with the common phenomena of physical and mental sexual harassment by husbands (Johnston & Naved, 2008; Wahed & Bhuiya, 2007). Women deserve the right to participate in fertility decision making without facing any type of discrimination or violence (AI USA, 2007; WHO, 2014); however, a husband’s dominance in fertility decisions often results in induced abortion, miscarriage, and fetal death, and also leads to pregnancy-related complications (J. C. Campbell, 2002; Dunkle et al., 2004; Rahman, Mostofa, & Hoque, 2014; Stephenson, Koenig, & Ahmed, 2006).
The norms and values of a patriarchal structure often create a barrier that prevents women from visiting health care centers and withholds maternal health care without the consent of their husbands (O. M. R. Campbell & Graham, 2006; Chowdhury, Islam, Gulshan, & Chakraborty, 2007; Mullany, 2010; Rahman, Haque, & Sarwar Zahan, 2011). Accordingly, 85% of deliveries in rural Bangladesh still take place in homes, whereas less than a quarter of births are attended by skilled health care professionals (Bangladesh Bureau of Statistics [BBS], 2010). Moreover, only a small proportion (25.5%) of women receive antenatal care (ANC), and only 27.1% of women seek postnatal care from qualified health professionals within the first 2 days after delivery (National Institute of Population Research and Training [NIPORT], 2011). Thus, the maternal mortality ratio (MMR) in Bangladesh is 570 per 100,000 live births, one of the highest in the South Asian region (United Nations Children’s Fund [UNICEF], 2009); at the same time, approximately 12,000 women die every year due to various pregnancy-related complications (Planning Commission, Ministry of Planning, Bangladesh, 2008).
The concept of “personal autonomy” plays an important role in understanding the power dynamics between males and females in a male-dominated society such as Bangladesh (Haque, Rahman, Mostofa, & Zahan, 2012; Rahman et al., 2014). In this regard, various literature suggests that the concept of “personal autonomy” denotes an individual’s control over his or her own body and the resources he or she possesses (Haque et al., 2012; Kishor & Subaiya, 2008; Rahman, 2012; Sen & Batliwala, 2000). According to this concept, women’s autonomy generally emphasizes women’s ability to control their lives, easily access resources and information, and participate equally with their male counterparts in every aspect of their lives (E. K. Brunson, Shell-Duncan, & Steele, 2009; Kishor & Subaiya, 2008; Rahman, 2012; Sen & Batliwala, 2000). Along these lines, Rahman et al. (2014) argued that women’s autonomy is closely associated with personal capacity rather than prestige or position within a social context (Haque et al., 2012; Rahman et al., 2014). Thus, women’s autonomy is explained through three different areas: household decision-making power, control over financial resources, and the extent of freedom of movement (Bloom, Wypij, & Gupta, 2001; Nigatu, Gebremariam, Abera, Setegn, & Deribe, 2014; Tiwari & Kumar, 2006; Woldemicael, 2007).
Numerous studies have been conducted in South Asia and diverse international settings to examine the impact of women’s autonomy on various women’s health issues, including fertility (Balk, 1994; Basu, 1992; Dyson & Moore, 1983; Hindin, 2000; Jejeebhoy, 1991; Morgan & Niraula, 1995; Singh, Singh, Singh, & Pathak, 2002; Vlassoff, 1991), birth control (Dharmalingam & Morgan, 1996; Feldman, Zaslavsky, Ezzati, Peterson, & Mitchell, 2009; A. H. T. Khan, 1997; Schuler & Hashemi, 1994), reproductive behavior (Jejeebhoy, 1995), maternal and child health care (Nigatu et al., 2014; Woldemicael & Tenkorang, 2010), unintended pregnancies (Rahman, 2012), and health outcomes (Gupta, 1995). Despite the body of relevant knowledge, we currently lack understanding not only how exactly women’s autonomy status determines their control to exercise reproductive rights but also what composes meaningful measures of women’s reproductive rights status in Bangladeshi setting, and as a result, the present study explores women’s autonomy as a potential indicator of their reproductive rights. In this regard, the study proceeded on with the following research questions:
Method
Study Setting
The study was conducted in the Bagerhat district of Bangladesh. Due to our familiarity with the language and cultural practices of the local people, we purposely selected the “Hogladanga village” of Ujalkur union in Bagerhat district for the study. Under Khulna Division, Bagerhat district is placed in Southwestern Bangladesh, formerly founded by Hazrat Khan Jahan Ali as a part of Khilafatabad Pargana. Bagerhat district has a total area of 3,959.11 km2 with the population of 1,476,090 people having a literacy rate of 44.3% (BBS, 2011; Wikipedia, 2015). Among 77 unions of Bagerhat district, Ujalkur union is considered as one of the oldest union with an area of 31.35 km2 because of its hundred year’s legacy. Ujalkur union has 23 villages and Moujas in total. About 6,615 families live in Ujalkur union with a population of 27,409 people (BBS, 2011). Among 23 villages of Ujalkur union, Hogladanga village has its own uniqueness because of its traditional culture, language pattern, and geographical setting. About 427 families live in Hogladanga village with a population of 1,781 people (BBS, 2011).
Research Design
The nature of the study was explanatory, as we investigated cause-and-effect relationships between women’s autonomy and their control to exercise reproductive rights. We perceived women’s autonomy as an independent variable and reproductive rights as a dependent variable. We conducted the study using survey research design to explore the significance of women’s autonomy in determining their control to exercise reproductive rights along with various sociodemographic variables. Particularly, in dealing with the attitude as well as the behavior of a subject, survey research has a greater importance in collecting the greater body of data within a short time as well as its wider applicability in various dimensions (Shaughnessy, Zechmeister, & Jeanne, 2011).
Participant Inclusion Criteria
To achieve the study objective, we defined participant inclusion criteria of the study, that is (a) all the respondents should be women, (b) aged 15 to 49, (c) they all should be married and currently live with their husbands, (d) they should have at least one child, and last, (e) they should have lived in the selected study areas of Bagerhat district for minimum 2 years. Under these characteristics, we carried out a household census in the study area to identify the exact population to draw a representative sample. In “Hogladanga village,” we identified 230 married women as the population of the study.
Sampling
From the census, we selected a total of 200 married women, having at least one child, using simple random sampling for the conformity of greater validity of the present study as well as giving the equal chance and nonzero probability of being selected to every respondent. We calculatedly 1 selected the samples considering a confidence interval of 2.5 at 95% confidence level.
Data Collection
We collected data from both primary and secondary sources. We collected primary data through face-to-face interaction with the interviewees and secondary data from relevant journals, periodicals, reports, and books.
Development of study instruments
The interview questionnaire contained both open-ended questions such as “Do you have any notion about autonomy?”; if yes, “What do you understand from the term women’s autonomy?”; “How did you see your household decision-making sphere in your family?”; and so on, to understand the respondent’s perceptions about the variables, and closed-ended questions along with 27 Likert-type questions with five possible responses. We incorporated these questions in the survey tools to collect the desired three interlinked and mutually reinforcing indices on women’s autonomy, that is, power in household decision making, control over financial resources, and freedom of movement, suggested and performed by Bloom et al. (2001), Nigatu et al. (2014), Tiwari and Kumar (2006), and Woldemicael (2007). Accordingly, to measure two proxy variables of women’s reproductive rights, that is, power regarding sexual and reproductive behavior, we incorporated 12 Likert-type questions in accordance with AI USA (2007) and WHO (2006), under two indices into the survey tool.
Construction of women’s autonomy
Women’s autonomy is based on three interlinked factors, that is, participation in household decision making, control over finances, and freedom of movement. In the present study, we measured household decision-making autonomy by asking nine categorical questions based on the following variables: household purchases (television, refrigerator, clothes/shoes/jewelry for self and children), purchases of real property, daily household expenditures, money spent on income-generating activities, selection of daily food menu, children’s education, children’s marital decisions, and control over finances. We measured financial autonomy by asking six questions focusing on subsequent variables, such as spending money by herself, the household income, her own income, the selection of family expenditures, and control over credit and savings. Conversely, we explored freedom of movement by asking 12 questions that emphasized succeeding variables, such as trips to the market, other shopping expeditions, visits to hospitals/health centers, visits to children’s schools, interactions with friends and family members, taking walks, watching movies, participating in religious ceremonies, visiting community centers or clubs, going out alone to arbitrary distant places, and returning home from outings late at night. The response options for the aforementioned three domains were (5) very high, (4) high, (3) reasonable, (2) low, and (1) very low.
Measures of reproductive rights
We used two mutually interlinked indices, that is, the extent of power regarding sexual behavior and the reproductive index to measure women’s reproductive rights. We assessed the first indices through the respondents’ observations and experiences by asking six specific questions with such issues as the frequency of enjoying sexual intercourse, forced sex with husband, torture by the husband during forced sex and compelled intercourse during menstruation, or illness and health hazard due to forced intercourse. We measured the second indices by assessing answers to six precise inquiries on decisions about sexual union, contraceptive use, the priority of conception, timing and spacing of having children, maternal health care services, and postpartum health care services. The response options for the sexual behavior index were (1) always, (2) sometimes, and (3) never, and the response options for the reproductive behavior index were (1) decision of husband, (2) joint decision of both husband and wife, and (3) decision of wife.
Fieldwork
Before conducting the actual survey, we piloted the interview schedule on 25 women to identify the shortfalls within the tool. After piloting the questionnaire, we modified the interview schedule based on feedback from pretest. Before going to the actual survey, we gave a 3-day intensive training to five female data collectors to clarify about the aim of the study, research procedure, data collection techniques, content, and clarification of the questionnaire (by going through each question of the questionnaire). Afterward, we used the revised interview schedule to administer the final data collection from the respondents with trained female interviewers in face-to-face situation.
Data Processing
After completion of data collection, we processed the raw information by (a) removing illegal codes, (b) reducing logical inconsistencies and errors, and (c) dropping improbabilities and solving ambiguities. We coded data to classify them into meaningful codes in accordance with its quality, quantity, and periodical basis to draw logical inferences. Later, we tabulated data on the basis of similarities, attributes, and intervals.
Data Analysis
For the first index (household decision-making autonomy), we characterized respondents’ responses using a 1 to 5 range, with a maximum of 45 and minimum of 9 as the expected points/counts in the case of the first index for each person. We also followed this procedure sequentially for the second and third indices. According to frequencies of points (highest/lowest) in the statistical range, we used (highest value − lowest value + 1) formula with the number of classes as three to determine the class interval (range / number of classes) and to categorize the decision-making power into higher, medium, and lower types. Finally, taking into account all of the scores on the different indices, we used the sum of the total responses to construct the overall autonomy index (AI; Cronbach’s α = .879) to facilitate and conduct multivariate analyses (Cronbach’s α = .749, first index; Cronbach’s α = .872, second index; and Cronbach’s α = .875, third index). Besides, counting the sexual behavior index, we quantified each response using a 1 to 3 range with a maximum value of 18 and a minimum of 6, and also followed this method for the second index. Accordingly, we used (highest value − lowest value + 1) formula with the number of classes as three to determine the class interval (range / number of classes) and to categorize the decision-making power into higher, medium, and lower types (Cronbach’s α = .862, sexual behavior index; Cronbach’s α = .877, reproductive behavior index; and Cronbach’s α = .892, reproductive rights status index [RRSI]). Finally, after calculating all the scores on the different indices cumulatively, we used that sum of total indices of every individual to construct the RRSI to facilitate and to conduct multivariate analyses. We used bivariate linear regression technique to show the associations between various sociodemographic characteristics and indices of women’s autonomy with reproductive rights status along with two proxy variables, that is, sexual behavior index and reproductive behavior index. We included all the significant predictor variables in multiple linear regression models. We used SPSS (Version 21) to analyze the study data to measure the association between women’s autonomy and their reproductive rights.
Ethical Considerations
Ethical clearance was obtained from the Academic Committee of Sociology Discipline, Khulna University. Furthermore, potential risks were minimized through strict adherence to confidentiality and informed consent procedures. After explaining the purpose of the study, verbal and written consent was taken from all the participants prior to their participation in the study. In addition, the respondents were informed that their participation in the study is voluntary and that they would not be obligated to provide answers to any question(s) with which they are uncomfortable.
Results
Sociodemographic Characteristics of the Study Subjects
The sociodemographic characteristics of the sample revealed that a majority of the respondents belonged to the age group of between 28 and 38 years, and the average age of the respondents was 30.91 years. Most of the women (93%) in rural areas were reportedly married before their legal age of marriage, 2 whereas 88.5% of the respondents conceived before age 18, and the average pregnancy ratio was 3.91. Among the respondents, 66% lived with extended family and more than half (60%) had six or more family members. A majority of the respondents (74%) were housewives who remained economically dependent (75%), and the average monthly income of the respondents was only BDT 3 1,894. Accordingly, approximately half of the husbands’ (49%) monthly incomes ranged from BDT 4,001 to BDT 7,000, with the average income BDT 5,549, and most of the husbands worked as day laborers (49%; Table 1).
Percentage Distribution of Respondents by Background Characteristics (N = 200).

Source. Field Survey, 2016.
Percentage Distribution of Respondents in Various Indices
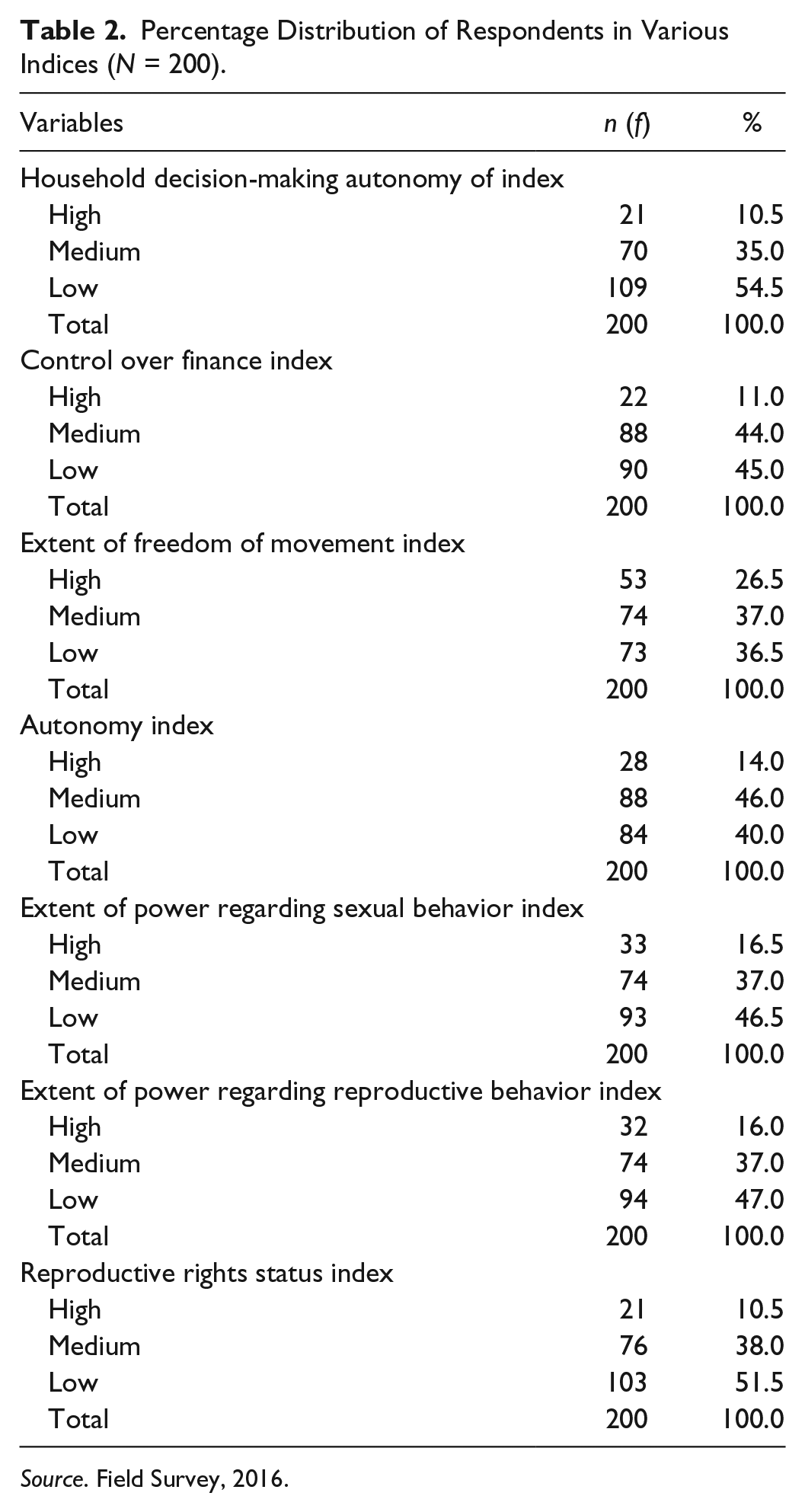
Table 2 displays various indices related to women’s autonomy and control to exercise reproductive rights through percentage distribution. As the table clearly shows, in every aspect of their lives, women’s participation is limited by their male counterparts, especially in household decision making; more than half of the respondents (54.5%) stated that they generally do not play a significant role in household decisions, with a similar situation in financial matters (45%). Regarding freedom of movement, although 37% of the respondents stated that they enjoy that right, this finding does not prove that this freedom makes any crucial improvement to women’s control to exercise their reproductive rights, as they may think. For responses regarding the overall AI, the highest percentage of the sample acknowledged medium (46%) and lower (40%) status, and this picture was diverse in the case of women’s control to exercise reproductive rights as highest percentage of the sample (51.5%) acknowledged low status in RRSI along with its two subindices, extent of power in sexual behavior (46.5%) and reproductive behavior (47%).
Percentage Distribution of Respondents in Various Indices (N = 200).
Source. Field Survey, 2016.
Bivariate and Multivariate Analyses
In the first model, a series of bivariate regression analyses revealed significant correlations between the sociodemographic characteristics and various indices of women’s autonomy with the sexual behavior index of respondents, where significant positive correlations were observed for age of respondent (β = .707, SE = .049, p < .001), educational status (β = .702, SE = .054, p < .001), power in household decision making (β = .782, SE = .048, p < .001), control over financial activities (β = .812, SE = .046, p < .001), and the extent of freedom of movement (β = .683, SE = .048, p < .001). All the significant variables (p < .05) in the bivariate analyses were entered into the multiple linear regression model. All of the variables remained significantly correlated with the respondents’ sexual behavior index, that is, control over financial activities (β = .291, SE = .073, p < .001), followed by power in household decision making (β = .256, SE = .063, p < .001), with the exception of extent of freedom of movement (β = .116, SE = .049, p < .05). In particular, older women and women with more education, more control over finances, household decision-making autonomy, and freedom of movement had more control in reproductive decision making. The adjusted-R2 value showed that approximately 77.7% of variance in the respondents’ sexual behavior index was explained by the predictor variables.
In the second model, bivariate regression analyses showed a similar result, including the respondents’ age (β = .740, SE = .047, p < .001), educational status (β = .744, SE = .051, p < .001), power in household decision making (β = .777, SE = .048, p < .001), control over financial activities (β = .810, SE = .046, p < .001), and the extent of freedom of movement (β = .711, SE = .046, p < .001). These variables were also found to significantly correlate with the respondents’ reproductive behavior index. In determining the respondents’ reproductive behavior index, in the second multiple linear model, all of the variables also remained significantly correlated, such as age (β = .234, SE = .043, p < .001), education (β = .245, SE = .049, p < .001), power in household decision making (β = .221, SE = .057, p < .001), control over financial activities (β = .235, SE = .066, p < .001), and the extent of freedom of movement (β = .143, SE = .044, p < .05). More than 81% of variance in the respondents’ reproductive behavior index was explained by the predictor variables.
Finally, on the subject of the respondents’ control to exercise reproductive rights (RRSI), all of the aforementioned variables in the first two models were found to be significantly correlated in bivariate regression and integrated in the multiple linear model. Except for extent of freedom of movement, all the variables found to correlate: control over financial activities (β = .265, SE = .070, p < .001) followed by power in household decision making (β = .258, SE = .061, p < .001), age (β = .225, SE = .046, p < .001), and educational status (β = .202, SE = .053, p < .001). More specifically, women who were older, had more education, had more control over finances, and had more household decision-making autonomy have higher control to exercise their reproductive rights. The adjusted-R2 value showed that approximately 75.2% of variance in the respondents’ RRSI was explained by the predictor variables (Table 3). No problems were observed because all the variables had a variance inflation factor (VIF) score below 4 (Rogerson, 2001).
Bivariate and Multiple Linear Regression Analyses Examining Correlates of Reproductive Rights Along With Sexual and Reproductive Behavior Indices (N = 200).

Note. CI = confidence interval.
p < .05. **p < .001 (two-tailed).
Bivariate regression analyses revealed significant correlations between women’s autonomy and reproductive rights status (β = .862, SE = .035, p < .001), along with both of the proxy variables, including the sexual behavior index (β = .915, SE = .031, p < .001) and reproductive behavior index (β = .915, SE = .031, p < .001). In particular, women with higher autonomy status had higher control to exercise their reproductive rights and greater control in both sexual and reproductive decision making. The adjusted-R2 values showed that 83.6%, 83.6%, and 74.2% of variance in the respondents’ sexual behavior, reproductive behavior, and RRSI was explained by the women’s autonomy status (Table 4).
Bivariate Association Between Women’s Autonomy and Reproductive Rights Along With Two Proxy Indices (N = 200).
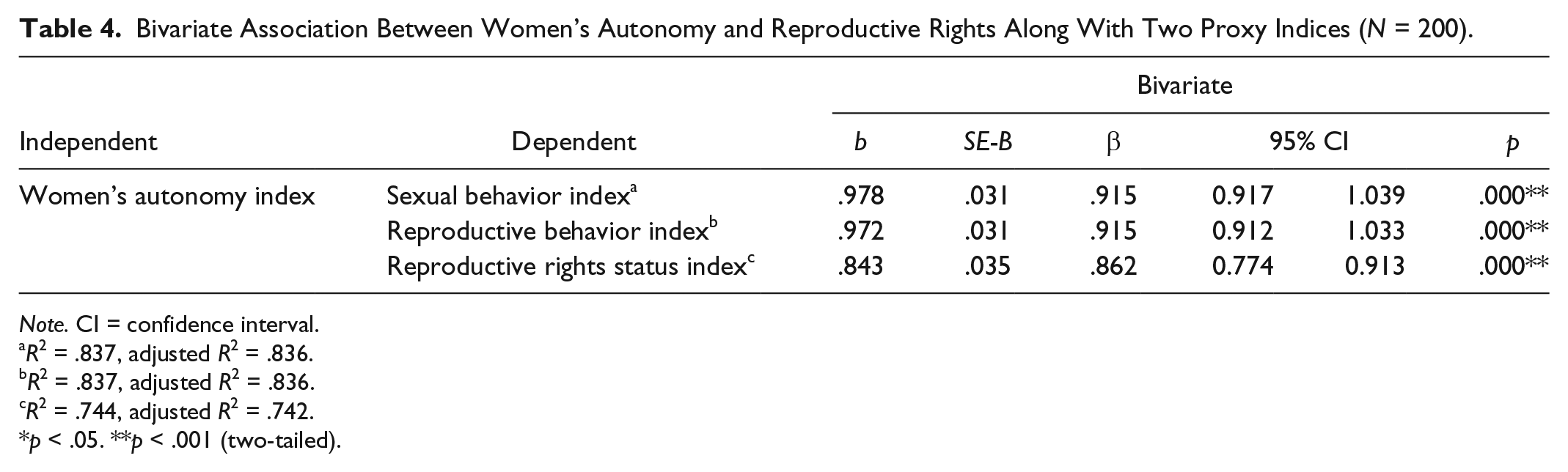
Note. CI = confidence interval.
R2 = .837, adjusted R2 = .836.
R2 = .837, adjusted R2 = .836.
R2 = .744, adjusted R2 = .742.
p < .05. **p < .001 (two-tailed).
Discussion
The study findings suggest that women’s higher autonomy significantly influences their control to exercise their reproductive rights along with both of the proxy variables of reproductive rights (extent of power regarding sexual and reproductive behavior indices). These findings are also consistent with earlier studies such as Dharmalingam and Morgan (1996), Haque et al. (2012), Nigatu et al. (2014), Rahman (2012), and Rahman et al. (2014). From a critical point of view, the aforementioned studies focused only on one or two issues related to reproductive health; for instance, Rahman et al. (2014) indicated that in Bangladesh, married women’s current as well as future intention to use contraception is significantly associated with their household decision-making autonomy. Similarly, Rahman (2012) suggested that greater household decision-making autonomy decreases the likelihood of experiencing an unintended pregnancy. Moreover, Haque et al.’s quantitative study in Bangladesh documented the importance of maternal autonomy in greater utilization of reproductive health care services among young mothers. However, the present study endeavored to focus on all of the indicators of reproductive rights, because in a patriarchal setting such as Bangladesh, all reproductive rights issues, such as access to safe and affordable contraception, the right to safe and healthy pregnancies, and access to reproductive health care utilization, are mutually interlinked and to a great extent influenced by autonomy paradigm of women as well as the power structure of both males and females (Haque et al., 2012; Rahman, 2012; Rahman et al., 2014; Story & Burgard, 2012).
Household decision-making autonomy was considered the first female domain over all autonomy indices, and the research found it was considerably connected with the reproductive and sexual behavior indices of women. These findings are consistent with those in various earlier studies, including Binyam, Mekitie, Tizta, and Eshetu (2011); Haque et al. (2012); A. H. T. Khan (1997); and Rahman et al. (2014).
In accordance with previous studies by Engle, Menon, and Haddad (1999); Haque et al. (2012); and Nigatu et al. (2014), women’s financial autonomy was found to be significantly concomitant with their sexual and reproductive behavior indices. Women who have control over financial resources, such as spending money for different purposes and control over their own income, credit, and savings, had more control regarding their sexual and reproductive behavior.
In addition, the study showed that women’s freedom of movement was also markedly linked with the proxy variables of reproductive rights, that is, the extent of the respondents’ power regarding the sexual and reproductive behavior indices (Bloom et al., 2001; Haque et al., 2012; Rahman et al., 2011; Rahman et al., 2014).
Women’s autonomy status, in particular, was influenced by their sociodemographic characteristics, such as age and educational status (Haque et al., 2012; Rahman et al., 2014), and in the present study, autonomous status was common among women who possessed certain characteristics. The study findings suggested that both women’s age and educational status were associated with their reproductive rights status and influenced women’s sexual and reproductive behavior (Al Riyami, Afifi, & Mabry, 2004; Haile & Enqueselassie, 2006; Haque et al., 2012; Rahman et al., 2014; Schuler & Hashemi, 1994).
From a research standpoint, some limitations should be identified in addition to the present study’s findings. First, the study focused only on rural women, and therefore a comparative study and discussion with urban counterparts would give a more comprehensive background. Second, the current study integrated only three different dimensions in explaining women’s autonomy, that is, the extent of household decision-making power, control over financial resources, and the extent of freedom of movement. In addition, other dimensions, such as the extent of participation in social and political activities and exposure to mass media, would afford the study a stronger basis for generalization because the concept of women’s autonomy is not homogeneous and varies according to cultural setting. Third, the study was conducted on a relatively small sample; a larger sample would enable the study to produce more generalizations.
Despite these drawbacks, this pioneering study sought to examine the association between women’s autonomy and various indicators of reproductive rights together because they are mutually interlinked and strongly connected with the power structure of both males and females in a patriarchal society. Understanding the real situation regarding women’s reproductive health and rights through a single indicator is impractical; for instance, access to safe and affordable contraception influences both fertility status and the likelihood of experiencing unintended pregnancy among Bangladeshi women (Rahman, 2012; Rahman et al., 2014). In addition, women’s access to reproductive health care utilization significantly influences the state of safe and healthy pregnancy in Bangladesh (Haque et al., 2012; Story & Burgard, 2012). However, the present study uncovered significant information that could serve as a starting point to ensure women’s reproductive rights in Bangladesh.
Conclusion
Because women’s autonomy is closely linked with their control to exercise reproductive rights, to improve women’s reproductive rights in a patriarchal setting, female autonomy must be considered a sociocultural determinant for ensuring their reproductive rights. In Bangladesh and the rest of the developing world, research on the women’s autonomy paradigm in connection with various reproductive issues is needed to develop effective strategies and policies to ensure women’s reproductive rights because they are considered legal rights.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.