
Abstract
The utilization of contraceptives depends on women’s autonomy in making decisions. Limited and inconclusive information is available on women’s decision-making autonomy to use contraceptives in East Africa. Therefore, the main objective of this study was to assess married women’s decision-making autonomy on contraceptive use and associated factors in East African countries. The most recent Demographic and Health Surveys were used for this study. The study included a total weighted sample of 41,893 married reproductive-age women. A multilevel mixed-effect binary logistic regression model was fitted. The prevalence of married women’s decision-making autonomy on contraceptive use was 18.91% (95% CI: 18.54, 19.29). Respondents who are employed (AOR = 1.24; 95% CI: 1.03, 1.44), having more than two alive children (AOR = 1.38; 95% CI: 1.13, 1.67), and visited a health facility in the last 12 months (AOR = 1.22; 95% CI: 1.05, 1.45), urban residency (AOR = 1.39; 95% CI: 1.27, 1.50), lower middle-income level 1.37 (AOR = 1.37; 95% CI: 1.17, 1.60), and community media exposure to family planning message (AOR = 1.25; 95% CI: 1.04, 1.45) were significantly associated with women’s decision making autonomy on contraceptive use. Despite the fact that every woman has the right to participate in her own healthcare decisions, less than one-fifth of married women in East Africa have contraceptive decision-making autonomy. Hence, Women’s decision-making autonomy on contraceptives should be promoted through mass media as an essential part of sexual and reproductive rights, with particular attention paid to rural women, women with no children, and women living in low-income households.
Background
Maternal mortality decreased by 2.9% every year between 2000 and 2017 globally, but there were still 295,000 maternal deaths and 2.6 million neonatal deaths (UNICEF, 2019). Most of the deaths can be prevented with basic maternal and child health care. Contraceptive use and decision-making autonomy on contraceptives are improved by improving maternal health care service utilization, like antenatal care (ANC), institutional delivery, and postnatal care (PNC) (Zimmerman et al., 2019). Previous scholars revealed that women’s decision-making autonomy is also associated with promoting maternal healthcare utilization, such as ANC, institutional delivery, and PNC (Ameyaw et al., 2016; Awoleye et al., 2018; Tiruneh et al., 2017). Women’s decision-making autonomy on contraceptives is one of the key strategies for reducing maternal morbidity and mortality, particularly in developing countries (Yaya et al., 2018). Additionally, scholars revealed women’s decision-making autonomy is also linked with controlling high fertility (Alemayehu & Meskele, 2017), unintended pregnancy (Kassahun et al., 2019; M. Rahman, 2012), and unmet need for family planning (Sougou et al., 2020).
Factors influencing women’s decisions about accessing and using maternal health care include socioeconomic status, the perception of modern healthcare, family size, the perceived severity of illness, and previous experiences with illness and death (Abegaz et al., 2019; Ajibade et al., 2013). As a result of power imbalances within marriage, couples may not have clear communication regarding reproductive health care decisions, which in turn can have an impact on contraceptive use (Mane et al., 2001). Furthermore, culture, marital status, education, and male dominance are other factors that can affect women’s decision making autonomy to use contraceptives (Kulczycki, 2008; Santelli et al., 2009). Because of these constraints, women often do not have the autonomy to make healthcare decisions under certain circumstances.
Globally and regionally, different strategies such as the International Conference for Population Development (ICPD), Millenium Development Goals (MDGs), and Sustainable Development Goals (SDGs), have been implemented to improve the health of mothers (UNFPA, 2010). From these strategies, Sustainable Development Goal 5 aims to eliminate gender inequality and empower all women and girls (Osborn et al., 2015). Different studies indicated that women who had higher decision-making autonomy had a higher rate of contraceptive use (Loll et al., 2019; Viswan et al., 2017). Additionally, decision-making autonomy in the household influences the use of contraceptives (Story & Burgard, 2012; Tiruneh et al., 2017).
Most of the previous studies in the East African region on women’s decision-making autonomy on contraceptives were institutionally based, restricted to specific regions or zones, and had a small sample size. But this study seeks to use nationally representative data to determine the magnitude and factors associated with decision-making autonomy on contraceptives. As to our search of the literature, no study has been conducted to investigate the magnitude and related factors of married women’s decision-making autonomy on contraceptives based on the pooled Demographic and Health Surveys (DHSs) data in East Africa. The findings of this study is crucial to assess cross-national disparities in women’s autonomy. Additionally, the study had adequate statistical power for detecting the true effects of variables; thus, it is based on pooled DHS data in East Africa. The results of this study will be beneficial to program planners, who will use the results in allocating resources to improve maternal and child health. Therefore, the aim of this study is to determine married women’s decision-making autonomy on contraceptives and associated factors in East African countries.
Methods
According to the UN Statistics Division, the African continent can be divided into five regions. Among these countries, East Africa is the largest region that includes 19 countries (Burundi, Comoros, Djibouti, Ethiopia, Eritrea, Kenya, Madagascar, Malawi, Mauritius, Mozambique, Reunion, Rwanda, Seychelles, Somalia, Somaliland, Tanzania, Uganda, Zambia, and Zimbabwe). Based on Demographic and Health Surveys (DHS), this study analyzed secondary data. In these 19 East African countries, 13 have DHS data, while 6 (Djibouti, Somalia, Somaliland, Seychelles, Mauritius, and Reunion) don’t. Two of these 13 countries have DHS data that were collected before 2010 (Eritrea, 2002, and Madagascar, 2008). Our study included DHS data from 11 countries conducted after 2010 (Corsi et al., 2012). The dependent and independent variables were extracted from the women’s recode (IR file) data set. You can download the dataset for free at https://www.dhsprogram.com/Data.
A two-stage stratified sampling technique is used by the DHS. As a result, the data is representative of the entire country. A total weighted sample of 41,893 married reproductive-age women was included in the study. Those women who were not using contraceptives, unmarried or not in a union, and pregnant at the time of the survey were excluded. Women with missing values were included in the no category. Details about the selected countries, the survey year, and the sample are shown in Table 1 below.
Sample Size for Women’s Decision-Making Autonomy on Contraceptive Use in Each East Africa Countries (N = 41,893).

Variables of the Study
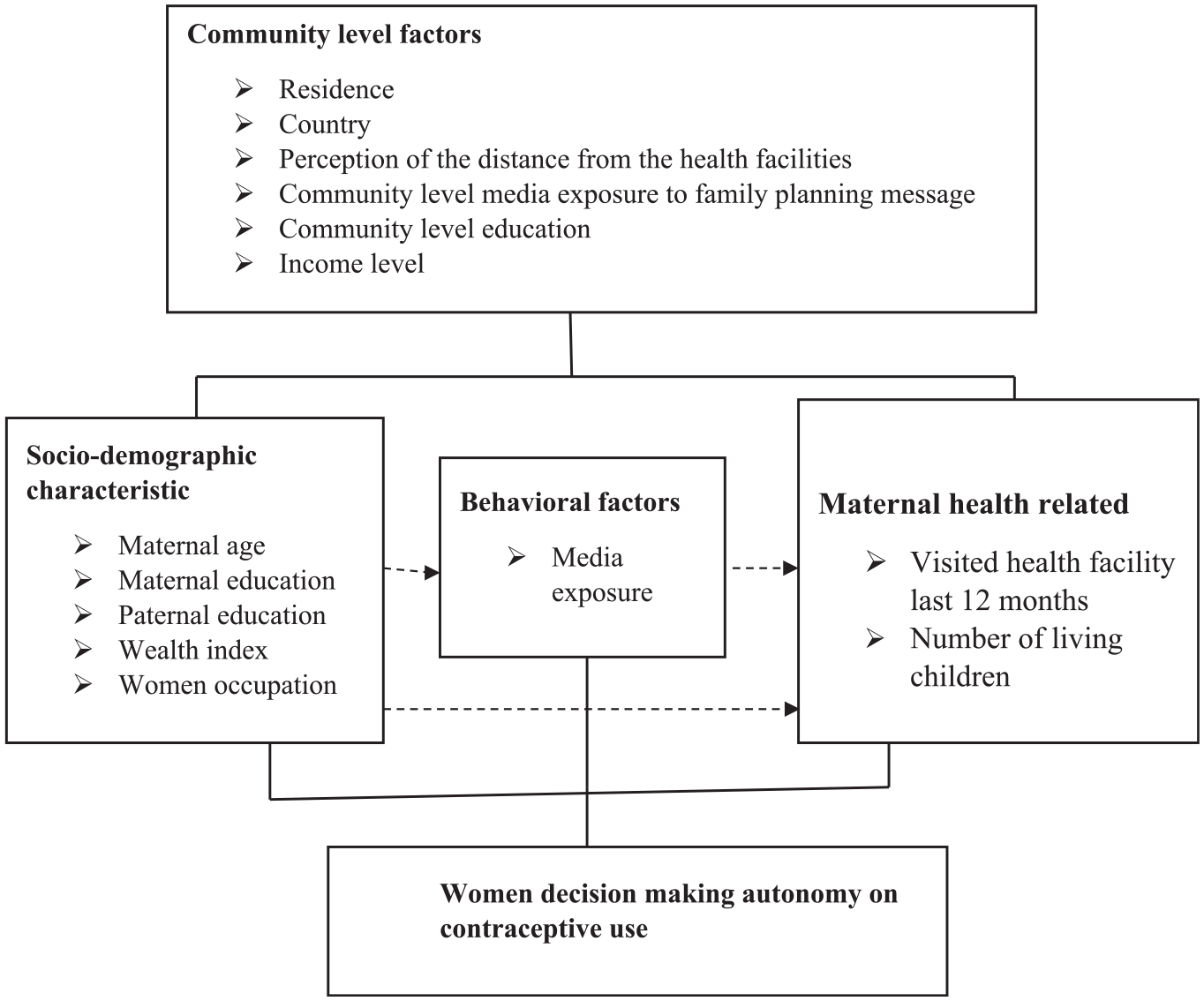
Conceptual framework of factors associated with women’s decision-making autonomy on contraceptives developed from searching of literature (N = 41,893).
List of Individual and Community Variables for the Assessment of Women Decision-Making Autonomy on Contraceptive Use Among Reproductive Age Women in East Africa (N = 41,893).

Data Analysis
Data analysis was performed using Stata version 14. The DHS surveys use four types of sampling weights: household weights, household weights for the men’s subsample, individual weights for women, and individual weights for men, of which we used individual weights for women. Prior to data analysis, all frequency distributions were weighted (v005/1,000,000) to ensure that the DHS sample was representative and to obtain reliable estimates and standard errors.
The first step was a graphical representation of women’s decision-making autonomy on contraceptive use in East African countries. The second step was a bivariable analysis that calculated the proportion of women’s decision-making autonomy on contraceptive use across the independent variables. Those variables with a P-value less than or equal to .2 in the bivariable analysis for both the individual and community-level variables were fitted in the multivariable model. All variables entered in the bivariable analysis were less than or equal to 0.2. In the final step of the analysis, a multilevel logistic regression analysis comprising fixed effects and random effects was done. Variables with an adjusted odds ratio (AOR) with a 95% Confidence Interval (CI) and a P-value <.05 in the multivariable model were reported to be significantly associated factors for women’s decision-making autonomy on contraceptive use. A traditional logistic regression model violates the independent observations and equal variance assumptions due to the hierarchical structure of the DHS data. As a result, women were nested within households, and households were nested within clusters. They may share similar characteristics within the cluster. Therefore, multilevel binary logistic regression analysis must take into account the variability between clusters.
Four models were fitted, including the null model (model 0), which shows the variations in the women’s autonomy on contraceptives in the absence of any independent variables. Model I accounts for individual-level variables, Model II accounts for community-level variables, and Model III accounts for both individual and community-level variables. Deviance (−2LLR) was used to assess the model’s fitness, and the model with the lower deviance (model III) was the best-fitted model. The correlation coefficient (ICC), Median Odds Ratio (MOR), and Proportional Change in Variance (PCV) were computed to measure the variation between clusters.
Results
Individual and Community Level Factors
A total weighted sample of 41,893 women has participated in the final analysis of this study. Majority (44.23%) of the women were under the age group of 25to 34 years and the median age of the women was 31 (IQR: 19, 43) years. More than half (53.59%) of the women had primary education and most (51.12%) of the women had media exposure to family planning messages. Majority (71.00%) of the women were rural dwellers. Of the respondents, 47.00% were from a community with high educational exposure, and distance to the health facility was not a big problem for 62.2% of the women (Table 3).
Individual and Community Level Factors of the Women in east Africa (n = 41,893).

Women’s Decision-Making Autonomy on Contraceptive Use in East Africa
The prevalence of married women’s decision-making autonomy in East Africa was 18.91% (95% CI: 18.54, 19.29), with Rwanda and Comoros having the lowest and highest prevalence of 8.72% and 33.46%, respectively (Figure 2).

Women decision-making autonomy on contraceptive use in East Africa countries (N = 41,893).
Factors Associated With Women Decision-Making Autonomy on Contraceptive Use
Multilevel logistic regression analysis was used to assess the presence of an association between the outcome and independent variables. On the bivariable analysis, age of the women, educational status of the women, husband’s educational status, resident, women’s occupation, wealth index, number of living children, visited health facilities in the last 12 months, media exposure to family planning messages, income level, community level education, and community media exposure to family planning messages, Perceived distance to the health facilities was found to be associated with the women’s decision-making autonomy on contraceptives, with a P value of <.2. After adjusting for the individual and community-level variables, residence, number of living children, visited health facilities in the last 12 months, occupation, income level, and community media exposure to family planning messages were significantly associated with women’s decision-making autonomy on contraceptive use. Accordingly, women who were employed had 24% (AOR = 1.24; 95% CI: 1.03, 1.44) times higher odds of decision-making autonomy on contraceptive use as compared with non-employed women. The odds of decision-making autonomy on contraceptive use were 38% higher among women who had more than two alive children (AOR = 1.38; 95% CI: 1.13, 1.67) as compared with their counterparts. Urban resident women had 39% higher odds of decision-making autonomy on contraceptive use than rural resident women (AOR = 1.39; 95% CI: 1.27, 1.50).
The odds of decision-making autonomy on contraceptive use among those women who had community-level media exposure to family planning messages were 25% (AOR = 1.25; 95% CI: 1.04, 1.45) times higher than their counterparts. The odds of decision-making autonomy on contraceptive use among women who visited a health facility in the last 12 months were 22% (AOR = 1.22; 95% CI: 1.05, 1.45) times higher than those women who had not visited the health facilities in the last 12 months. The odds of decision-making autonomy on contraceptive use among women who lived in the lower middle class were 1.37 (AOR = 1.37; 95% CI: 1.17, 1.60) times higher than those women who lived in the low-income level.
The odds of decision-making autonomy on contraceptive use among women who lived in Burundi, Comoros, Ethiopia, Kenya, Malawi, Mozambique, Uganda, Zambia, and Zimbabwe 1.34 (AOR = 1.34; 95% CI: 1.13, 1.58), 5.29 (AOR = 5.29; 95% CI: 4.26, 6.58), 2.94 (AOR = 2.94; 95% CI: 2.52, 3.44), 6.40 (AOR = 6.40; 95% CI: 5.51, 7.44), 1.80 (AOR = 1.80; 95% CI: 1.56, 2.08), 5.61 (AOR = 5.61; 95% CI: 4.68, 6.74), 5.41 (AOR = 5.41; 95% CI: 4.70, 6.21), 2.00 (AOR = 2.00; 95% CI: 1.71, 2.33), and 2.54 (AOR = 2.54; 95% CI: 2.18, 2.97) times higher than those who lived in Rwanda, respectively (Table 4).
Multilevel Analysis of Factors Associated with Women’s Autonomy to Use Contraceptive in East Africa (n = 41,893).

Note. ICC = Intra class correlation coefficient; MOR = median odds ratio; PCV = proportional change in variance; AOR = adjusted odds ratio; CI = confidence interval.
P-value <.05
Measures of Variation
The ICC from the null model revealed that 47.42% of the variation in decision-making autonomy on contraceptive use was due to cluster differences, while the rest (52.58%) was due to individual factors. A PCV of 0.3287 in the final model indicates that individual as well as community-level factors contributed to about 32.87% of the variation in decision-making autonomy on contraception use. We used deviance to compare models’ fitness. The third model had the lowest deviance (5835.23), making it the best-fitting model (Table 4).
Discussion
This study aimed to determine women’s decision-making autonomy on contraceptive use and associated factors among married women in East Africa countries. The current study revealed that less than one-fifth of married women in East Africa had contraceptive decision-making autonomy. This finding is lower than studies done in Ethiopia 21.60 (Mare et al., 2022), South Africa 22% (Osuafor et al., 2018), and Nigeria 24% (Alabi et al., 2019). This disparity could be attributed to differences in sample size, socioeconomic, sociocultural aspects of society, and the study population. In addition, possibly due to internal conflicts in the area, scholars indicated that women decision making autonomy was lower in conflict areas than in non-conflict affected areas (Ekhator-Mobayode et al., 2021).
Women’s decision-making autonomy on contraceptive use who reside in urban areas was higher than that of rural residents. This is supported by studies done in Ethiopia (Edossa et al., 2020; Mare et al., 2022). This might be because urban women are more likely to use contraceptives and discuss them with their husbands. Moreover, urban women have greater exposure to media and, therefore, they have good knowledge about modern contraceptives (M. M. Rahman et al., 2014). The current study found that women who have more living children are more likely to have contraceptive decision-making autonomy than their counterparts. The reason for this is that women’s status in society is socially constructed, and the number of children they have, as well as their role within society, affects their status (Sougou et al., 2020). Furthermore, as women have more children, male-centered decisions have decreased, and achieving fertility desires might also affect these findings (Bogale et al., 2011).
In comparison to women with low community media exposure to family planning messages, women with high exposure to family planning messages were more likely to have autonomy in making contraceptive decisions. This finding is in lined with the findings of a study conducted in Ethiopia (Mare et al., 2022). This finding may be explained by the fact that women exposed to family planning messages in the community media have a deeper understanding of reproductive health rights and the advantages of utilizing health care services, which encourages them to participate in reproductive health decisions (Mare et al., 2022).
Women occupation was also found to be a significant factor in women’s decision-making autonomy in the current study. This study found that women who are employed have a higher chance of decision-making autonomy on contraceptive use than women who are not employed. This is in line with a study in Southern Ethiopia (Alemayehu & Meskele, 2017). Which found that employed women are more likely to have decision-making autonomy than women who are not employed. This could be because women who are employed have access to education and contact with different individuals. This might enhance women’s decision-making confidence and access to information and challenge men’s dominance in making decisions (Kabeer, 2005; Tesema et al., 2021).
Furthermore, the current study revealed that women who visited a health facility for maternal health service utilizations in the last 12 months were more likely to have had decision-making autonomy on contraceptive use as compared to their counterparts. This is in line with a study done in Ethiopia (Mare et al., 2022). The possible justification could be that women who visit health facilities have better access to health information and a good understanding of sexual and reproductive health rights and health issues, which enables them to make an independent decision on contraceptive use.
Women who lived in countries with lower-middle income levels were associated with higher decision-making autonomy on contraceptives than those who lived in countries with low-income levels. This could be due to the fact that women in lower middle-income households engage in income-generating activities that increase their economic independence, challenging the traditional belief of male dominance in decision-making, which in turn improves spousal communication and household autonomy (Gebeyehu et al., 2022). The decision-making autonomy of married women who live in Comoros, Burundi, Ethiopia, Kenya, Malawi, Mozambique, Uganda, Zambia, and Zimbabwe is more likely to be higher than that of women who live in Rwanda, respectively. The possible justification might be due to the difference in sociodemographic characteristics and cultural variations. In Rwanda, for example, only 13.4% and 12.9% of married women and their husbands had a secondary education or higher, whereas 15% to 71.5% and 16.5% to 78.6% of married women and their husbands in other countries had a secondary education or higher. The other reason could be that the contributions and commitments of each country to empowering women may vary from one county to another (Onditi & Odera, 2017).
The study’s main strength was that it used nationally representative survey data with a large sample size. In order to accommodate the hierarchical nature of the data, we used multilevel analysis. However, Due to the cross-sectional nature of the study, cause-and-effect relationships between the dependent variable and the independent variables cannot be determined. DHSs are based on self-reported information, which is likely to be prone to social desirability bias due to its socio-cultural nature. In addition, the current study lacks triangulation of data using diverse data collection methods since it used data collected from the DHS.
Conclusion
Despite the fact that every woman has the right to participate in her own health-care decisions, less than one-fifth of married women in East Africa have contraceptive decision-making autonomy. This can result in high rates of unmet need for family planning, unintended pregnancy, and unsafe abortion. This raises the risk of maternal and child morbidity and mortality. Residence, occupation, number of living children, visited to a health facility in the last 12 months, community media exposure to family planning messages, and country were identified as associated factors of women’s contraceptive decision-making autonomy. Based on these findings, Women’s decision-making autonomy on contraceptives should be promoted through mass media as an essential part of sexual and reproductive rights, with particular attention paid to rural women, women with no children, and women living in low-income households. The concerned body should also engage women in out-of-house employment. Healthcare providers should be supported in the dissemination of family planning messages in areas with limited access to mass media to reach rural women. This, in turn, would be helpful to increase women decision-making autonomy.
Footnotes
Acknowledgements
We are grateful to the DHS programs, for the permission to use all the relevant DHS data for this study.
List of Abbreviations
AOR: Adjusted Odds Ratio; CI: Confidence interval; DHS: Demographic and Health Survey; ICC: Intra-class Correlation Coefficient; MOR: Median Odds Ratio; PCV: Proportional Change in Variance; SD: Standard Deviation; SSA: Sub-Saharan Africa; WHO: World Health Organization.
Authors’ Contributions
DBA and WDN conceived the idea for this study, involved in the data extraction, analysis, interpretation of the finding and writing the original draft. FMA, DGB, EAF, SMF and WDN assisted in the analysis of the study. ESS, RET, TGA, HBE and FMA writing the review and editing the manuscript. All the authors read and approved the final manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The study does not involve the collection of information from subjects. Consent to participant is not applicable since the data is secondary and is available in the public domain. All the methods were conducted according to the Helsinki declarations. More details regarding DHS data and ethical standards are available online at (![]() ).
).
Consent for Publication
Not applicable