
Abstract
The persistent power dynamics between men and women in most countries of Africa has continued to deny women necessary access to contraceptive. The study examines the impact of men’s involvement in contraceptive use and wellbeing among married women in Nigeria using DHS data. Two sets of data, NDHS 2008 & 2018 were used in this study. The selection of the samples was based on two-stage sampling techniques and the data for the study were analyzed using three levels of statistical method. The study reveals higher significant effect of men’s involvement on reproductive rights was affirmed while an inverse significant relationship was confirmed between male involvement in contraceptive use and years of schooling of women in the study The study concludes that changing behavioral attitudes of men toward family planning is therefore essential and urgent.
Introduction
In the last six decades, the world has looked for ways of curtailing the growth of population, with specific emphasis on policies and programs that could enhance the use of contraceptives and lower number of births per woman toward an overall improvement in their quality of life. The 1994 International Conference on Population and Development (ICPD) action plan effectively changed earlier strategies of achieving demographic targets specifically through the provision of family planning, to addressing critical essential issues of quality of life and the wellbeing of women (Alyahya et al., 2019; UNFPA, 1995 ). In achieving this, prominence has been given to male involvement in health issues regarding women, focusing on achieving gender equality and promoting the reproductive rights of women. However, the persistent (household and marital) power dynamics between men and women in sub-Saharan Africa has continued to deny women the necessary access to contraceptive use, as decision-making on this is still highly controlled by their male partners. Also, several socio-cultural factors in most African societies restrain women from fulfilling their child-spacing desires and accessing health care services, such as family planning services. Of significance are reports that men are decision-makers in the issue of reproductive health related to the family and spousal consent or disapproval can hold back the use of contraceptives. Increasingly, literature has therefore recognized men as a clog in the wheel of women’s reproductive health progress and believed that involving men in reproductive health decisions of women will transfer decision-making power in this particular area from men to women (Cleland et al., 2011; Kura et al., 2013; National Population Commission, 2009). Similarly, Hartmann et al. (2012), in their study explained that men’s involvement in women’s use of contraceptives could improve spousal relationship and women’s participation regarding reproductive decision making.
Some studies have confirmed that good knowledge and positive attitudes of men toward birth spacing, ideal family size, and contraceptives greatly influence women’s uptake of family planning (Bishwajit et al., 2017; Vouking et al., 2014). In the same vein, spousal supports have been observed as a significant impetus for the use of family planning in strong patriarchal settings,evident in Africa and particularly in Nigeria (Anyanwu et al., 2013). Aryeetey et al. (2010) in their study noted that 20% of respondents admitted that husbands were a barrier to the usage of contraception while most of the women that used contraceptives reported joint decisions and insisted that male partners should be involved in the decision to use family planning. It was also noted that male involvement not only influenced acceptance of contraceptives but was also capable of changing men’s attitude and behavior toward women’s health. Men’s involvement could result in better outcomes in sexual and reproductive health indicators such as safe sexual behavior, contraceptive acceptance, health care utilization and reduction in maternal mortality (Kura et al., 2013).
While it seems intuitive that helping women avoid unwanted pregnancies through the use of family planning methods could improve their well-being, studies also affirmed that women’s contraceptive use could have many other benefits. It could unlock opportunities for economic success, increase the attainment of post-secondary education, increase the uptake of employment opportunities, narrow gender gap in pay, stabilize marriages and improve the chances of success for their children (Bailey et al., 2012; Sonfield et al., 2013). Of special significance is the use of contraceptives which could increase the year of schooling of women and prepare women for jobs with better earnings, thereby alleviating poverty. Availability of contraceptive methods and access to it would enable women to have fewer children and invest more in their families through the accumulation of greater wealth (Gipson et al., 2008; Gribble & Maj-lis, 2009; Miller, 2009; World Health Organization, 2013). It is also good to note that ability to successfully determine the number of children and when to have the next birth plays a part in partner violence, depression, mental health, and happiness. Women and men with unplanned births appear particularly likely to experience depression, anxiety, and lower reported levels of happiness (Mirowsky & Ross, 2002; National Campaign to Prevent Teenage Pregnancy, 2008; Sonfield et al., 2013). Close births is also tied to the well-being of the children in the family in different ways. It could decrease the parental investment on children (Frenette, 2011), lessen money saved for the education of each child and significantly reduce the chance of a child attending private school (quality of nutrition and ability to fight infectious diseases).
In spite of the considerable body of literature on male involvement in sexual and reproductive health (Bishwajit et al., 2017; Cleland et al., 2011; Mullany et al., 2006; Singh & Ram, 2009), substantial gaps still remain in the understanding of males’ involvement in contraceptive use and women’s quality of life in Nigeria. This is a neglected but growing population problem needing deep introspection and action, to avoid a demographic disaster in the nearest future. In a setting where social norms are still largely in favor of men, their involvement should be considered a dominant factor for a successful outcome of reproductive health programs, especially family planning. It is largely through this that one can predict the success of achieving an additional 120 million women and adolescent girls using modern contraceptives by the year 2020 and beyond. At the same time, wellbeing has appeared recently as “something everyone apparently aims for, and arguably has a right to” (McCallum & Price, 2016). It has been viewed by different scholars as the combination of feeling good and functioning well; the experience of positive emotions such as happiness and contentment (Carter, 2016; Huppert, 2009; Ruggeri et al., 2020). People’s perceptions, their thought, their feelings, and their actions, have a direct impact on their own and others’ living conditions (Michalos, 2007). It was also debated that wellbeing is more than just positive affect (happiness, feeling satisfied). Wellbeing extended to subjective wellbeing more specifically as consisting of three essential interrelated components: life satisfaction, pleasant affect, and unpleasant affect. However, looking essentially at overall well-being of women, it is therefore expedient to examine the relationship between men’s involvement in contraceptive use and wellbeing of women in Nigeria, with implications for Family Planning (FP) 2020.
Theoretical Framework and Study Hypotheses
The study is premised on two theories; theory of gender and power (Connell, 1987) and Seligman’s PERMA model (Seligman, 2011). The three grounds on which the theory of gender and power rests are the sexual division of labor, the sexual division of power, and the structure of cathexis. The main thrust of this theory is on sexual negotiations with unequal power-sharing which exist at the societal and institutional levels and are maintained by social mechanisms. The sexual division of labor creates unequal rewards between men and women concerning the value attached to each responsibility. Women are engaged mostly in recognized but “unpaid work” such as child care, housework and caring for the sick family and the elderly which ensures dependence on men for financial support. Little or no participation in income-earning activities will debar women from making certain decisions in the family including their health (Adeyem et al., 2016). Economic dependence on male partners constrains women to sacrifice adoption of health-protective behaviors and compromise on safety in sexual practices and condom usage, contraceptives use, decision-making on the next birth, and number of children.
Ogunjuyigbe and Adeyemi (2005) found that among married women in Yorubaland, it was believed that women should be submissive to their husbands in fertility-related matters and that they were expected to secure permission of their husbands before taking major decisions such as limiting fertility through contraceptives or other means. Overall, discrepancies in the sexual division of power-sharing are one of the core elements of gender and power theory. Apart from the fact that men largely control the economic and financial resources, they also exert authority within heterosexual relationships. The gender gap in power-sharing is the main cause of intimate partner violence. Sex is most frequent in violent relationships because husbands or partner assert the right to demand sex any time and weaken the power of negotiation of women for safe sex and unwanted pregnancies (Adhena et al., 2020; World Health Organization, 2013). Such power imbalance has been documented as an inhibiting factor against the use of condoms among women (Feyisetan & Oyediran, 2020; Woolfork et al., 2020). Likewise, where wives’ decision making power and knowledge about family planning are limited, the use of contraceptives will not be all-embracing between partners (Do & Kurimoto, 2012).
The theory also noted that the structure of cathexis determines the social norms for sharing power between men and women. The structure readouts appropriate sexual behavior for women and are characterized by the emotional and sexual attachments that women have with men. This type of power inequity is upheld by patriarchal social belief systems that support power differentials between men and women. There are biases in the patriarchal societies regarding sexuality, with women believing that sex is limited for procreation while multiple sexual partnerships and sexual domination within heterosexuality belong to men. Looking at the power inequality within the theory and the impact of men’s involvement in issues of sexuality, theoretical framework therefore informed the analysis of the factors that affect men’s involvement in contraceptive use and women’s quality of life in this study. In the same vein, Seligman’s PERMA model suggests that wellbeing has several measurable elements, each contributing to wellbeing (Seligman’s, 2011). The PERMA model identifies five essential elements to wellbeing: (i). Positive emotions include a wide range of feelings, not just happiness and joy {P}. (ii). Engagement refers to involvement in activities that draws and builds upon one’s interests {E}. (iii). Positive Relationships are all important in promoting positive emotions, whether they are work-related, school related, familial, romantic, or platonic {R}. (iv) Meaning also known as purpose, and prompts the question of “why” {M}. (v). Achievement/accomplishment are the pursuit of success and mastery {A}.
Studies have shown that one of the reasons why women don’t use family planning is the societal pressure on women to prove their fertility immediately after marriage despite the fact that they may not want to have the child. This may have negative effects on their emotion as related to child spacing (Bhugra et al., 2013; Carter, 2016). It was also noted that positive relationship between two partners will promote positive emotion as indicated by .PERMA model, When there is good communication between sexual partners it will promote the use of family planning method among partners and improve their wellbeing. Whereas violence will devoid the use of appropriate child spacing methods. Studies have shown that the levels of involvement of partners, as well as their opposition to family planning methods, are crucial factors in using, switching, and discontinuation of contraceptives (Clabaugh et al., 2021; Kupoluyi, 2020; Karra & Zhang, 2020). This may also have negative consequences on the health of the mother.
To this end based on the above theories, the study hypothesized (i) that there is a significant association between male’s involvement in contraceptive use and women’s quality of life. (ii) Male involvement in contraceptive use, and women status may likely influence women’s wellbeing.
Methodology
Study Settings and Sample Selection
Nigeria Demographic and Health Survey (NDHS) data were used for the study after necessary approval had been sought from Measures DHS. Two sets of data, NDHS 2008 & 2018 were used in this study. The selection of the samples was based on two-stage sampling techniques. Stratification was achieved by separating each of the 36 State including the Federal Capital Territory (FCT) into urban and rural. In total 74 sampling strata were identified. The DHS data were collected through stratified cluster probability sampling design with cluster providing the primary sampling unit (PSU). The primary sampling unit (PSU), referred to as a cluster for the 2008 & 2018 NDHS, is defined on the basis of EAs from the 2006 EA census frame From each of the selected cluster households were randomly selected for the interview. A representative sample of 36,800 households was selected for the 2008 NDHS survey, while 42,000 households were selected for the 2018 NDHS survey. The data was nationally representative of the country selected. The detailed information for sampling procedure was published by the appropriate authority in each of the countries (National Population Commission/The DHS Program & ICF, 2008, 2018). The individual women recoded data were downloaded and weighted for proper representation after the approval from DHS Program, ICF USA. From each of these data, women who are currently using modern contraceptive methods aged 15 to 49 were included in the analysis. Since the study is about male involvement in the contraceptive use. While A total number of 3,501 women form 2008 NDHS and 4,397 women form 2018 NDHS were eligible for this study based on the above inclusion criteria (Figure 1).

Trends and patterns of contraceptive use among married women in Nigeria.
Variable Measurement
The outcome variable is wellbeing. Researchers with various backgrounds, from economists to psychologists, suggested two main approaches to measuring the overall well-being; objective well-being and subjective well-being (Bhugra et al., 2013; Carter, 2016).
One component each was selected from the methods of measuring wellbeing for this study, these are education (years of schooling) and health (reproductive rights) In this study reproductive right was used in this study for health based on the available data and the nature of the study. Since women’s health include their right to have control over and decide freely and responsibly on matters related to their sexuality, including sexual and reproductive health, the right to be free from torture, the right to health, the right to privacy, the right to education, free of coercion, discrimination, and violence (Corrêa, 1997, p. 4). The justification for the use of these two variables was based on the availability of data since the DHS data did not contain other variables The reproductive right was generated from two composite variables which are participations in the family decision-making and sexual rights. The questions related to decision making asked in DHS are (person who usually decides on the respondent’s health care; a person who usually decides on large household purchases; and a person who usually decides on visits to family or relatives). For each item, each respondent reported whether the decision was made by the respondent alone, respondent with husband/partner, husband/partner alone, someone else, or other. A dichotomous variable was constructed for each item by re-coding the responses as “1” for those who reported “respondent alone” or “respondent and husband/partner” and “0” for others. An index with value 0 to 3 was generated from this dichotomous variable with ‘0 ‘ indicating none participation and “1” for participation. For sexual rights, questions related to this variable are “Could you say no to your [husband/partner] if you do not want to have sexual intercourse?”; “Could you ask your [husband/partner] to use a condom if you wanted him to?” Each of this questions has two values (0 = no; 1 = yes). This was merged to generate a composite variable sexual right with a value 0 to 2 and dichotomized into “0” no right with others having sexual right “1.” Participation in decision making and sexual rights were merged as an index representing “Reproductive right” with a score range of 0 to 2. This was dichotomized into “0” for those who did not have any rights and “1 or more” for having rights “1.” The second indicator of the wellbeing used in this study was education (years of schooling) which is a count data.
Control variables are knowledge about contraceptives/family planning, intimate partner violence, and working status. This was based on the existing literature on contraceptive use and male involvement in sexual and reproductive health issues (Bishwajit et al., 2017; Kura et al., 2013). Knowledge about contraceptives was generated from three questions; (1) whether heard about family planning on radio, (2) whether heard about family planning on television, and (3) read about family planning from newspaper or magazine. An index 0 to 3 was generated and re-categorized into low = 1 (0 or 1) and high = 2 (2 or 3). Intimate partner violence was generated from three variables; ever experienced physical violence, experienced sexual violence, and experienced emotional violence. Each item was coded 0 for “no” and 1 for “yes.” An index signifying women’s experience intimate partner violence was computed with scores ranging from 0 to 3, 0 indicating no violence and 1 to 3 indicating experienced violence. The employment status of the woman was coded into two values (0 = not working; 1 = working). The independent variable was male involvement in contraceptives use. This was measured by husband participation in decision making concerning contraception. The variable used to measure this was a question on “decision-maker about contraception.” This was re-categorized into two: respondent alone, “0” while husband/partner alone and joint decision were merged as “1.”
Data Analysis
The data for the study were analyzed using STATA 14.0 and three levels of statistical methods was used for the study. First, univariate analysis to show the frequency distribution of the background characteristics of the respondents, outcome variables, and explanatory variables. The bivariate analysis was used to show the differentials among women whose partners were involved in contraceptive use and background characteristics with explanatory variables. For multivariate analysis, three models were constructed to test the formulated hypotheses. The first model shows the relative risks of male involvement and indicators of quality of life. In model 2 the explanatory variables were added (working status, knowledge about a contraceptive, and experienced intimate partner violence). In model 3, respondents’ background characteristics were added to model 2 (age, age at first sex, age at first marriage, wealth status, religion, place of residence, and partner’s educational level). In binary logistic regression was used to show the relationship of male involvement and. reproductive rights since it is a dichotomous variable. Poisson regression was used to test the effect of male involvement on the level of education of women since the year of schooling is a count variable. Stata 14 software was used for the analysis of the data.
Results
Socio-demographic characteristics, shown in Table 1 reveals that more than half of the women who are currently using contraceptives are living in urban centers with an increase in the proportion from 55.32% in NDHS 2008 to 60.97% in NDHS 2018. More than two-thirds (70.66%) have at least secondary education when the data was pooled together. The use of modern contraceptives increased with age at first marriage among the respondents with a slight increase among those who were at least 20 years in NDHS 2008 from 48.39% to 49.04% in NDHS 2018. Majority of the respondents have good knowledge of family planning when the data were pooled together with a sharp decrease from (58.12%) in NDHS 2008 to (29.68%) in NDHS 2018. Concerning the wealth index, the majority of the respondents are in rich wealth status but a sharp decrease was noticed from 72.31% in NDHS 2008 to 65.26% in NDHS 2018. It was observed that majority of the respondents who were using modern contraceptives were those with 1 to 4 children with a proportional increase from 43.18% in NDHS 2008 to 54.13% in 2018 might be unconnected with the respondents’ exposure to media- related to family planning. It was observed that husband/partner involvement in contraceptive use increased from 47.84% in NDHS 2008 to 60.29% in NDHS 2018. One in every five respondents using contraceptives was working while 1 in every 10 respondents experienced intimate partner violence when the data were pooled together in the study area.
Percentage Distribution of Individual Characteristics of Women Using Modern Contraceptives.

Individual characteristics and male involvement in contraceptives varies significantly with respondents’ age-group (p < .01). While male involvement increases with age at first marriage of women, respondents wealth status and partner’s level of education in the study. A significant relationship was established between male involvement and children-ever-born in all the data including when the data were pooled together (p < .01). It was noted that respondents who were other Christians apart from Catholic had the highest male involvement in contraceptive use in the study. From Table 2, the majority of respondents whose partners were involved in contraceptives use were currently working (NDHS 2008, 82.26%; NDHS 2018, 82.48%).
Individual Characteristics and Male Involvement in Contraceptive Use.
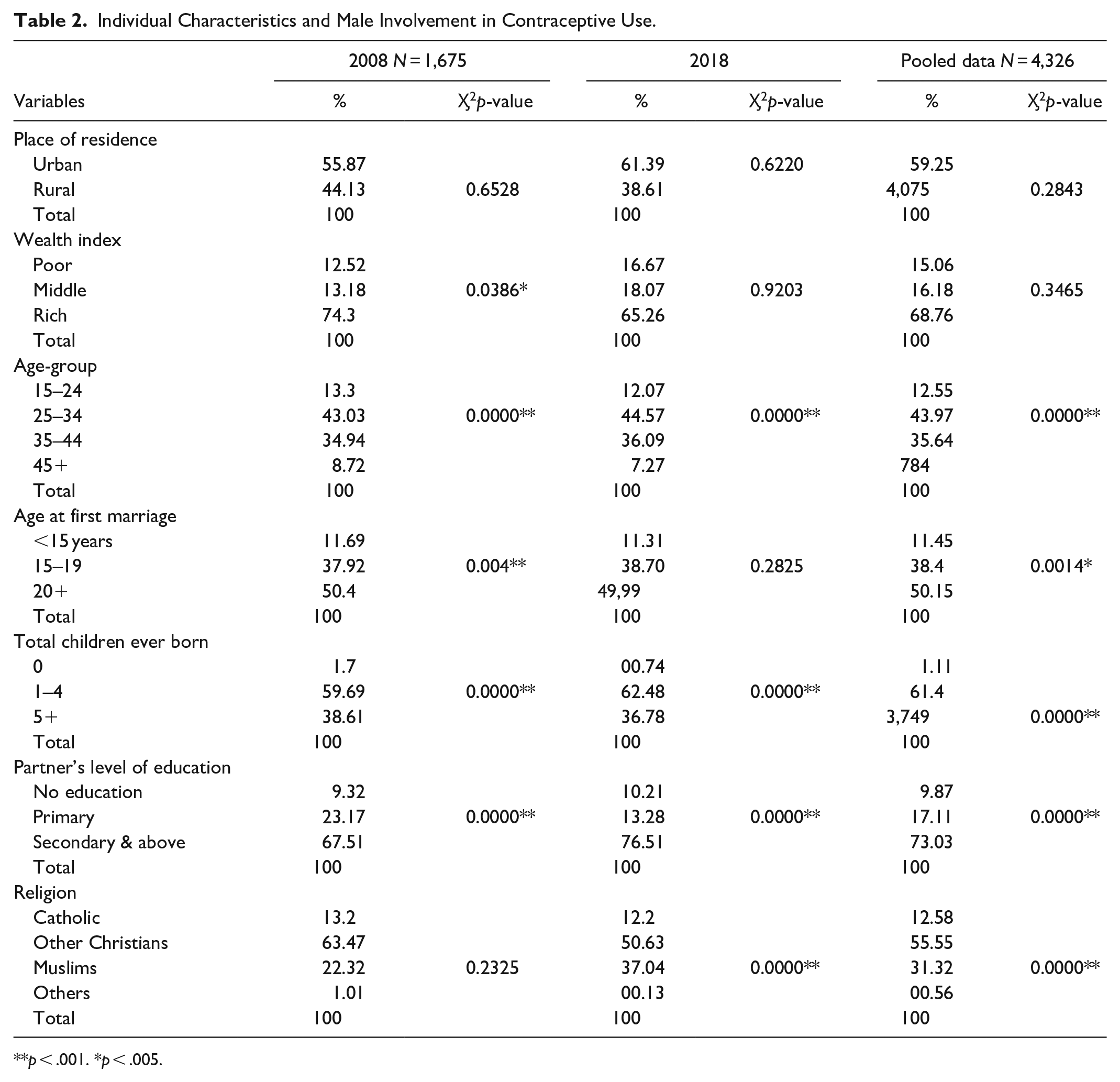
p < .001. *p < .005.
At the same time, male involvement in contraceptive use and women who experienced intimate violence was significantly reduced by half (see Table 3) from NDHS 2008 (24.99%) to NDHS 2018 (12.94%). With regards to knowledge of family planning, less than half of the respondents with good knowledge of FP indicated that their partner was involved in the contraceptive use decision-making when the data were pooled together (42.31%). The significant association was affirmed in the study between employment status, experienced intimate partner violence, and male involvement in contraceptive use except with the knowledge of family planning in NDHS 2008 (p < .01).
Bivariate Relationship Between Male’s Involvement in Contraceptives use and Control Variables.

p < .001. *p < .005.
The multivariate analyses of the data are shown in Tables 4 to 6. In model 1 consisting of male involvement and indicators of quality of life, a higher significant effect of male involvement in contraceptive use was affirmed with reproductive rights in all the data including, the pool data (p < 01). When control variables (working status, ever experienced violence, and Knowledge about FP) were included in model, the significant effect of male involvement and reproductive right was maintained. Working status and knowledge of family planning were significantly associated with reproductive rights in all the data (p < 01). When the background characteristics were added in model 3, a higher significant effect of male involvement in contraceptive use with reproductive right was observed, except in NDHS 2018 (NDHS 2008, odds ratio 1.58 p < .05; pooled data, odds ratio 1.44 p < .05). The relationship between employment status, knowledge of family planning, and reproductive right in model 3 followed the same pattern with significant association in all the data except in NDHS 2018. Surprisingly, experience of intimate partner violence remains insignificant with reproductive right in all the models.
Logistic Regression of Male Involvement in Contraceptive use and Reproductive Rights.

Note. CI = confidence interval @ 95%.
p < .001. *p < .005.
Poisson Regression of Male Involvement in Contraceptive Use and Education (Years of Schooling).
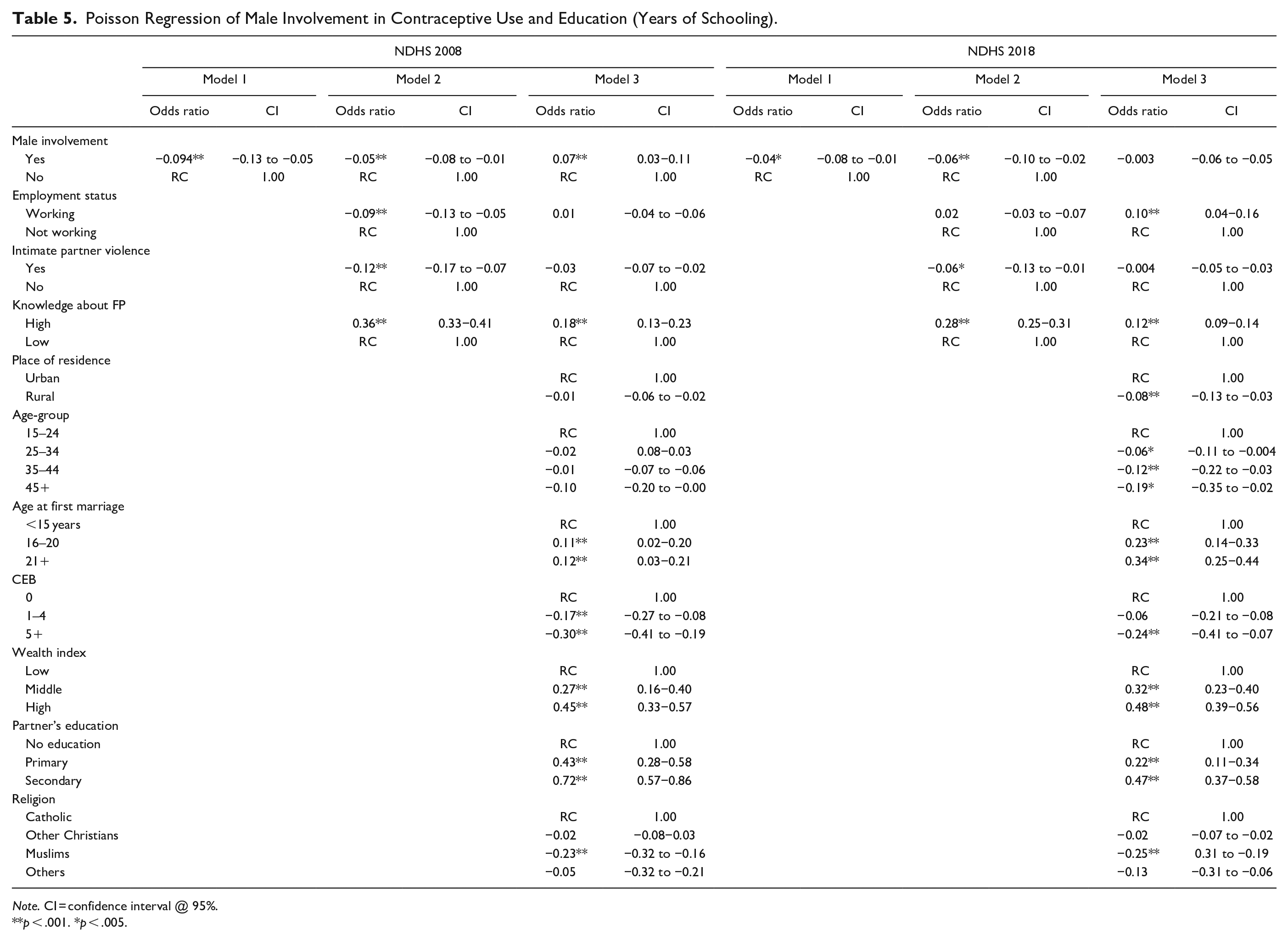
Note. CI = confidence interval @ 95%.
p < .001. *p < .005.
Pooled Data.

In the same vein, an inverse significant relationship was confirmed between male involvement in contraceptive use and years of schooling of women in model 1 for all the data (p < 01). With the addition of control variables in model 2, the relationship between male involvement and contraceptive use remains the same. Employment status was only significant in NDHS 2008 (odds ratio −0.09 p < .01) whereas ever-experienced intimate violence was inversely significant with years of schooling in all the data (p < 01). Similarly, high knowledge of family planning was significantly related to years of schooling in all the data (p < .01). With the inclusion of background characteristics of the respondents in model 3, significant relationship between male involvement and years of schooling of women was only noted in NDHS 2008 (odds ratio 0.07 p < .01). However, significant relationship was demonstrated between knowledge of family planning and years of schooling in all the data (NDHS 2008 odds ratio 0.18 p < .01 NDHS 2–18 odds ratio 0.12 p < .01 pooled data odds ratio 0.11 p < .01). In all, the multilevel analysis above has confirmed the two formulated hypotheses in this study; that male involvement in contraceptive use is significantly associated with women’s quality of life. Also the study affirmed that male involvement in contraceptive use, women status and intimate partner violence may likely influence women’s quality of life.
Discussion
The results of the analyses of this study have provided evidences of the association between male involvement in contraceptive use and women’s quality of life. The study established that majority of those women who were currently using modern contraceptives reported higher wealth status. This is in tandem with the remarks of Gwatkin et al. (2005) that the use of modern contraceptives among the richest women is double of the proportion among the poorest. A similar study in Malawi reaffirmed that women in richest wealth quintiles were more likely to use modern contraceptives than those in poorest quintiles (Adebowale et al., 2014). A similar study confirmed that women’s education, place of residence, occupation religion and partners’ education were independently associated with both decision-making on sexual intercourse and condom use (Darteh et al., 2019).
It was noted in the study that 1 out of every 10 respondents experienced intimate partner violence which agrees with National Population Commission/The DHS Program & ICF (2008) that in Nigeria, women’s lifetime exposure to IPV from their current husband or partner was 19% for emotional IPV, 14% for physical IPV, and 5% for sexual IPV. In the same vein, the significant relationship between IPV and male involvement as observed in the study did not deviate from the earlier studies (Tandrayen-Ragoobur, 2020). Research has shown that men with fewer resources are most likely to use violence to compensate for the shortage of resources and likely to institutionalize power inequality within the family (Conroy, 2013). Apart from men’s role as decision makers in the family, their actions in terms of abuse or neglect have a direct effect on the health of their wives and the well-being of their children. Also, the significant increases in age-at-first marriage with male involvement in contraceptive use in the study reaffirmed the effect of early marriage on contraceptive use reported in Nigeria over the last few decades (Adedokun Olaide, 2000; Adedokun et al., 2017). The age at first marriage not only affects fertility, childbearing, and unwanted pregnancy among married women but also influences women’s prospect for higher education than primary-level education and ability to support the family, especially their children’s well-being. On the other hand, early marriage inclines young women to high fertility and risk of maternal mortality (Ogu et al., 2016). Similarly, the significant relationship between employment status, intimate partner violence and male involvement in contraceptive use verified earlier findings (Rahman et al., 2011; Tenkorang, 2018). Women’s employment will likely lead to sustained decline in fertility when they have control over income, resources and have a greater say in family decision-making, including fertility choices (Lim, 2002). The significant effect of the partner’s level of education and male involvement in the contraceptive use in the study confirmed the earlier studies (Kura et al., 2013; Murarkar et al., 2011) that education enables access to health information by women of reproductive age. Study has found out that men’s educational level was strongly associated with their knowledge of sexual and reproductive issues, discussion of FP with their wives and utilization of maternal services (Hossain et al., 2007). On the other hand, contraceptive access may also have positive effects on the educational attainment of women’s male partners (Hock, 2008). Educational benefit of women’s contraceptives use to men occurred through a reduction in unintended pregnancies and unplanned births among their young female partners. This should give men more freedom to complete their own education without facing the financial and time commitments of being a father (Sonfield et al., 2013). On the other hand a study conducted in the Northern Nigeria on the side efects of of the Husbands’s school intervention on gender dynamics to improve reproductive health revealed gender role shifting and power sharing. The study further explained that men now understand the importance of the reproductive health services use which led to the increase in the accepatability of family planning in the study area (Institute for Reproductive Health, 2019)
Similarly, that good knowledge about family planning has a positive impact on contraceptive use and reproductive health awareness has been approved by this study (Bishwajit et al., 2017). Study has attested that understanding, participations and support of men about safe motherhood are crucial factor for women to access basic reproductive health services (Kura et al., 2013). In the same vein men who reported being influenced by their partner for FP decision-making, by turning to them for FP information, advice and guidance, are even more likely to use contraception (Clabaugh et al., 2021).
Furthermore, higher significant effect of male involvement in contraceptive use on reproductive rights meaningfully identified in this study reenacted the earlier hypothesis about the significant influence of husband/males on women’s reproductive health. Men’s decision and action before, during pregnancy, and after delivery often make a difference between illness and health of women. Recognition of women’s reproductive right by men is essential in setting them free from their seemingly traditional roles and allowing them full involvement in productive activities (Adeyemi, 2017). A study in TanZania affirmed that women who consulted with a family planning worker together with their husbands (rather than alone) experienced a larger reduction in pregnancies and a larger increase in reported contraceptive use (McCarthy, 2019). In a setting where power and sexual rights are characterized by an unequal balance of power as emphasized in gender and power theory (Connell, 1987), men may exercise more influence over their partners’ reproductive rights and the use of contraceptives may be hampered, thus putting women at reproductive health risks. Smith et al. (2003) in their study confirmed that in a community where women decision-making status is low, reproductive health services for women such as fertility regulation (through the use of family planning) gynecological care, and prenatal and postnatal care may not be available or they may be denied the access to utilize these services.
Conversely, Oyediran and Feyisetan (2017) remarked in their study that moderately high percentages of women reported having the ability to negotiate protective sex by refusing sex or asking for condom use during sex. This deviated from the traditional norms where women have no ability to negotiate sex as earlier reported (Gyimah et al., 2010; Ogunjuyigbe & Adeyemi, 2005). The positive influence of employment status on reproductive rights of women as observed in this study collaborate the earlier studies (Mengo et al., 2016; Oyediran & Feyisetan, 2017). The nature of women’s autonomy depends on their income from employment away from home, especially in non-familiar organizations and remunerative jobs in the formal rather than in the informal economy. This will allow them to make decisions concerning the number of children, when to have next births, and the use of contraceptives. Unfortunately, most women are estranged from participating significantly in economic activities as a result of deep-rooted traditional beliefs, customs, and unequal power relations within the households (Worldwatch Institute, 2013).
Furthermore, the inverse significant relationship between male involvement in contraceptive use and education (years of schooling) observed in this study has established significant impact of the gender system on reproductive decision-making (Malhotra, 2012; Upadhyay & Karasek, 2012). Gubhaju (2006) observed that educational level influences the contraceptive choices between couples with the resultant effect on the well-being of the family. For decades it has been confirmed that years of schooling influences the postponement of marriage. On the average, women with seven or more years of schooling marry 4 years later and have fewer numbers of children than those with no education ( Adedokun Olaide, 2000; UNICEF, 2001). In the same vein, women who delay having the first child till late 20s or 30s will have the opportunity to lessen financial pressure and contribute to the family economic stability. Also, the increase in women’s participation in labor force and higher levels of educational completion have shown to produce improvement in family well-being, increase use of contraception, reduce unwanted pregnancy, reduce infant and maternal mortality with economic advantage to the community. Also noteworthy is the inverse significant effect of ever-experienced violence on years of schooling as related to other studies (Abramsky et al., 2011; Karra & Zhang, 2021; Kundapur et al., 2017). A study in India found an inverse relationship between lifetime or recent intimate partner violence and a woman’s educational accomplishment (Ackerson et al., 2008). Study also documented that women without formal education were 4.5 times more likely to report lifetime IPV in comparison with women who completed more than 12 years of education (Naved & Persson, 2005). Over all, it appears that the greater involvement of men in reproductive health issues will improve the well-being of not only their wives/partners but the entire family. Since men are gate keepers regarding the household decision making, they can positively influence child and maternal health by making informed decisions about antenatal care, ensuring good nutrition, reducing work load during pregnancy, and jointly making decisions regarding crucial issues like family planning.
Study Limitations
It is important to mention, first, the study used DHS data which are cross-sectional and the causal relationship could not be measured. Secondly, there is no variable for income in the data sets and wealth index may not be able to capture women’s real income. Lastly, the study was unable to capture the level of involvement of men in the decision making within the household.
Conclusion and Contribution to Knowledge
In-spite of the limitations of the study, this research has reaffirmed the significance of male involvement in contraceptive use decision-making of women in Nigeria. Since one of the commitments of the London Summit is to increase the demand and support for family planning by removing barriers to its access and use by 2020, it is very imperative to revisit the strategies that involve men in family programs in Nigeria because men constitute a significant barrier to women’s contraceptive use. This is expected to enable the achievement of ‘the right of an additional 120 million married women with unmet needs and girls in the world’s poorest countries to use contraceptives without coercion and discrimination”. For example, in Nigeria, only 15.1% of married women of reproductive age were currently using any contraceptive with a significant unmet need in this study. Achieving Contraceptive Prevalence Rate (CPR) of 36% by 2020 requires comprehensive knowledge and information on the relevance of family planning to families with respect to quality of life of women, apart from the reduction in maternal and infant mortality. Changing behavioral attitudes of men toward family planning is therefore essential and urgent, looking at the uncovered benefits in this study such as sexual and reproductive rights, reduction in poverty, improved work conditions and wellbeing of the family.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.