
Abstract
This study investigated the prevalence of and factors that determine parent–child communication about HIV/AIDS and sexual and reproductive health (SRH) issues in Nigeria. The study used data from the National HIV/AIDS and Reproductive Health Survey (NARHS). The data are nationally representative and offers sociodemographic information on women aged 15 to 49 years and men aged 15 to 64 years. Prevalence of parent–child communication about HIV/AIDS, family planning, and contraception was generally low at 37.4%, 32.5%, and 9.5%, respectively. Determinants of discussions with children on HIV/AIDS, family planning, and contraception were respondents’ zone, economic status, and educational attainment. Parents held more discussions with female children than with the males. Parents aged 50 to 64 years, compared with the younger parents, were double likely (odds ratio [OR] = 2.04; 1.52-2.73) to discuss HIV/AIDS with their wards older than 13 years. Male parents, parents living in urban areas, and parents with richer economic status had higher odds of discussing HIV/AIDS and SRH issues with their wards.
Keywords
Background and Rationale
Since the outbreak of HIV/AIDS in the early 1980s (AVERT, 2018), efforts have been consistent to curtail its spread. Unscreened blood transfusions, sharing unsterilized needles and syringes among injecting drug users (IDUs), indiscriminate sexual behaviors, limited knowledge and poor perception of HIV/AIDS, concealment of symptoms for fear of stigmatization, and poverty are key spread factors of the deadly virus (AVERT, 2018; Castro-Arroyave, Mora, Arbeláez, & Mignone, 2018; Fenton, 2004; Ojebuyi, 2009; Wu, Sullivan, Wang, Rotheram-Borus, & Detels, 2007).
The Joint United Nations Programme on HIV/AIDS (UNAIDS) reported that adolescents and young people accounted for 39% of all new infections and 15% of all people living with HIV/AIDS in 2012 (UNAIDS, 2014). Citing Centre for Disease Control (CDC), Guzmán et al. (2003) in their study reported that more than 50% of high school people in the United States had sex. The same study also revealed that 42% of U.S. adolescents confirmed that they did not use a condom during their last sexual intercourse. Wamoyi, Fenwick, Urassa, Zaba, and Stones (2010) reported that as is the case, especially in most developing countries, sexual activities expose young people in Tanzania to increased risks of infection with HIV, other sexually transmitted infections (STIs), and propensity for an unplanned pregnancy. In Africa, the authors further explained, by age 15, 11% of girls and boys have had sex, while in Tanzania, the rates of condom use by young people are generally low. In Ghana, most of the young people aged 10 to 24 years who constitute one third of the population are at risk of negative health behavior as a result of inadequate sexual and reproductive health (SRH) education (Manu, Mba, Asare, Odoi-Agyarko, & Asante, 2015). The likely consequences of these early sexual activities and inconsistent use of contraceptives include a high rate of adolescent pregnancies, STIs (Guzmán et al., 2003), a prevalence of unwanted and abandoned children, and population growth. For instance, in South Africa, latest studies have shown the decline in HIV infection rates especially among young women, but the 15-to-24-year-old cohort remains vulnerable (Mpondo, Ruiter, Schaafsma, van den Borne, & Reddy, 2018).
Given the global prevalence of youth’s exposure to sexual and health risks, it is not surprising, therefore, that one of the contemporary global health concerns is how to improve the SRH of young people. To promote healthy sexual behavior among the youth, stakeholders have identified strategic interventions that delay sexual debut, reduce number of sexual partners, and increase condom use (Bastien, Kajula, & Muhwezi, 2011). Because of the prevalence of HIV in sub-Saharan Africa, where nearly 80% of young people live with the disease, there has been the intensity of youth-focused HIV and sexual-health-risk-prevention strategies in the region (UNAIDS, 2012). One of these strategies is effective parent–child communication of health issues. This is because parents, apart from being the most consistent influence in children’s lives, are naturally in a position to inculcate healthy sexual behaviors in the young people to ensure their personal development and smooth metamorphosis into active sexual life (World Health Organization, 2007).
There have been studies on communication about HIV and SRH issues generally, and especially from sub-Saharan Africa (Barker & Ricardo, 2005; Bastien et al., 2011; Defo & Dimbuene, 2012; Fagbamigbe & Ojebuyi, 2017; Iliyasu, Aliyu, Abubakar, & Galadanci, 2012; Jejeebhoy & Santhya, 2011; Leeds et al., 2014; Manu et al., 2015; Mohammadi, Alikhani, Farahani, & Bahonar, 2007; Nundwe, 2012; Ojebuyi, 2009; Pilgrim et al., 2014; Rivers & Aggleton, 1999; Wamoyi et al., 2010). For example, a sub-Saharan African study by Bastien et al. reveals a wide variation in parent–child communication in terms of frequency of discussions, with a range of sociodemographic and other factors associated with sexuality discussions (Bastien et al., 2011). Also, a study from India focusing on parent–child communication on SRH matters has established a regional divide in parent–child communication with more parents in the northern states than in the southern states and, to a lesser extent, the western state of Maharashtra, describing communication with their children as nonliberal (Jejeebhoy & Santhya, 2011). A Tanzanian study showed that parent–child communication about SRH was prevalent in most families, and was mainly on a same-sex basis (i.e., mother–daughter and rarely father–son or father–daughter) taking the form of warnings, threats, and physical discipline (Wamoyi et al., 2010). Manu et al. conducted a study on parent–child communication about SRH in Ghana and established influence of parents’ gender on the frequency of discussing SRH matters with their children (Manu et al., 2015): Whereas 78.8% of mothers had discussed sexual communication with their children, only 53.5% of fathers had done so. In Nigeria, a study by Obono indicated that despite general opinion about the taboo nature of sexual and reproductive communication in traditional African settings, it is prevalent among mothers and daughters in Ugep, a double unilineal descent and patriarchal society in Cross River State, Nigeria (Obono, 2012).
Nevertheless, none of these studies has established the factors that influence parent–child communication of HIV/AIDS and SRH matters, especially in Nigeria, which is a unique, socioculturally diverse nation (Iliyasu et al., 2012; Isika, 2016; Omotola, 2009). Besides, most of the studies on HIV and SRH issues carried out in Nigeria (e.g., Iliyasu et al., 2012; Iyaniwura, 2006; Izugbara, 2008; Mariga, Kullima, Bako, & Kolo, 2012; Obono, 2012; Ojebuyi, 2009) focused on regions—a phenomenon that could suggest geographic and ethnic bias. Given this gap, a nationwide study on HIV/AIDS and SRH matters that presents an inclusive body of evidence as to the prevalence of, and the factors that determine parent–child communication of HIV and SRH issues in Nigeria, is imperative. Specifically, this study aims to contribute to knowledge regarding how demographic variables such as age, gender, religion, social status, and location shape the frequency, direction, patterns, and intensity of parent–child communication of HIV/AIDS and SRH matters in Nigeria. This study answers the following questions: How frequently do Nigerian parents communicate with their children about HIV/AIDS, and sexual and reproduction issues? How do demographic variables such as age, gender, location, religion, and social status influence patterns and intensity of parent–child discussions of HIV/AIDS and SRH matters in Nigeria?
Nigeria, with over 167 million people, is Africa’s most populous country (National Population Commission, 2013; Population Reference Bureau, 2014). It is a multicultural developing society with a sizable percentage of its population uneducated and living in rural settings. Nigeria also has one of the world’s highest total fertility rate of 5.7 (National Population Commission [Nigeria] and ICF International, 2014; Population Reference Bureau, 2014). According to Nigeria’s 2012 NARHS Plus, the nation’s HIV/AIDS prevalence rate stood at 3.4%: 3.2% in the urban areas and 3.6% in the rural areas (Federal Ministry of Health [FMoH], 2013). The prevalence was 2.9% among young people aged between 15 and 19 years. At present, Nigeria has the second largest HIV epidemic in the world; and it is one of the highest rates of new infection in whole of sub-Saharan Africa (AVERT, 2018). The 2009 records by Population Reference Bureau show that one out of five of the world’s population are adolescents, and 85% of them are found in the developing world, including Nigeria (Iliyasu et al., 2012). The foregoing statistics further justify the need for this study.
The Roles of Parents in the Communication of HIV/AIDS and SRH Issues in the Family
The family plays significant roles in guiding and nurturing the children (Zolten & Long, 2006), and effective communication with the children is one of the fundamental responsibilities of the family. Nundwe (2012) supports this reality as the author explains that communication within the family system affects the sexual behavior of the child given the fact that communication about sexual behavior and general reproductive health issues within the family is crucial during the adolescent years (Nundwe, 2012). Research has shown that open communication between parents and children has a strong correlation with a reduction in negative sex behaviors by the children when they become sexually active (Leeds et al., 2014; Rosenstock, Strecher, & Becker, 1994; Viner et al., 2012). These studies confirm that the family is very critical to the sexual socialization of children and adolescents. The vital information and messages between parents and children could affect risky sexual behavior among adolescents (Dilorio, Pluhar, & Belcher, 2003). Parent–child communication about sexuality, and the understanding of how parents influence their children’s feelings, concerns, and decision making have a long history dating back to at least 1965 (Dubbe, 1965). However, during the past decades, parent–child communication studies have expanded beyond sexuality to include content, predictors, and outcomes associated with these discussions (Bastien et al., 2011; Jejeebhoy & Santhya, 2011; Mpondo et al., 2018; Obono, 2012; Soon et al., 2013; Yadeta, Bedane, & Tura, 2014). One reason for this increased interest is the HIV epidemic, which continues to affect millions of adolescents among its victims (Dilorio et al., 2003).
A meta-analysis of 95 studies on parent–child communication about sexuality by Dilorio et al. show that most parents reported discussing “sex” in general with their children; the most frequently discussed topics include menstruation, reproduction, pregnancy, birth, HIV/AIDS, and sexual values (Dilorio et al., 2003). Many parents, however, confessed to having faced difficulties when communicating sex and sexuality with their children. Some of these problems include embarrassment, difficulty in acknowledging and accepting adolescent sexuality, and the use of communication styles with which adolescents were less likely to feel comfortable. This phenomenon notwithstanding, the study notes an apparent correlation between parent–child communication about sexuality and adolescent sexual behavior (Dilorio et al., 2003). Similarly, the perception of adolescents about parent–child communication on sexuality are that such communication is affected by low parental care, difficulty in talking to their parents about problems, and valuing their friends’ opinions in making serious decisions. These were significantly associated with compromised behavioral and emotional health (Ackard, Neumark-Sztainer, Story, & Perry, 2006). Given this fact, parent–child communication of HIV/AIDS and SRH issues in the family is an important factor that deserves the attention of all stakeholders in public health. The extent to which the parents openly share information about health issues with their children determines the children’s health behavioral patterns. Adolescent sexual behaviors are partly influenced by family members and peers with whom they interact (Christopher, Johnson, & Roosa, 1993; Pistella & Bonati, 1998). Besides, parents play a critical role in the socialization of their children, of which sexuality is critical. Mpondo et al. (2018) buttress this reality when they say that “sexual health communication that is provided by the parents is considered very important,” This fact is further corroborated by Soon et al., when they explained that parents play important roles in influencing adolescent sexual decision-making and access to information about HIV and general SRH issues (Soon et al., 2013).
Theoretical Framework
The Health Belief Model (HBM) was adopted as the theoretical framework for this study. The model, being one of the earliest theories of health behavioral change communication, operates on the tenets that people’s decisions and communication about issues concerning their health are always influenced by some key variables: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cue to action, self-efficacy, and demographic variables (Abraham & Sheeran, 2015; Taylor et al., 2007). For instance, if people believe that they are susceptible to a certain health condition, they are likely to discuss the health matter and adopt new health behavior. Also, if people believe that the health condition has severe consequences, they are likely to take actions that prevent such negative consequences. People would take action if they believe that adopting the new health behavior would mitigate their susceptibility to the negative health condition, and if they perceive higher benefits of adopting the new health behavior in relation to the costs to be incurred, they are likely to discuss or adopt the new health behavior. Furthermore, individuals are likely to discuss and adopt the health behavior if they are exposed to factors (e.g., communication campaigns, television adverts, a reminder from their doctors, and encouragement from partners or peers) that prompt or trigger discussion and action. Finally, people are likely to act if they believe that they are capable of performing the prescribed action successfully (Champion & Skinner, 2008; Rosenstock, Strecher, & Becker, 1988)
However, since the HBM is conceptualized on the principle of a value–expectancy relationship (Brewer & Rimer, 2008), whether or not the foregoing would happen is also influenced by demographic variables such as age, gender, location, and social status. Information that adolescents share among their peers, who may or may not be well informed, often form the major source of the scanty knowledge that most adolescents have on reproductive health issues (Yadeta et al., 2014). In this present study, we investigated how demographic variables, as one of the key constructs of HBM, influence patterns and frequency of parent–child communication of HIV/AIDS and SRH issues in Nigeria. We predicted that how Nigerian parents communicated health issues with their children would be shaped by several demographic factors.
Method and Materials
The data for this study are from the 2012 NARHS Plus II (FMoH, 2013). It is a nationally representative cross-sectional data that contained information on knowledge, attitude, practices, and perceptions on HIV/AIDS, reproductive history, sexual characteristics of women aged 15 to 49 years and men aged 15 to 64 years selected using multistage cluster sampling technique. The respondents were drawn from households in the rural and urban areas in all the 36 states and the Federal Capital Territory (FCT) Abuja, Nigeria.
Urban and rural Local Government Areas (LGAs) were selected in each state after stratifying the LGAs into rural and urban localities at Stage 1. Thirty clusters each were then randomly selected from each of the selected LGAs at Stage 2. Selection of households from the clusters and 32 individuals from the selected households was carried out at Stages 3 and 4, respectively. The surveys used pre-tested structured questionnaires by interviewers trained in questionnaire administration. The analysis in this study was based on data from 10,639 respondents who had children older than 10 years.
From the constructs of the HBM (Abraham & Sheeran, 2015; Taylor et al., 2007), we selected the demographic variables to guide our construction of the dependent and independent variables. We examined how demographic characteristics influenced communication about HIV/AIDS and SRH issues between parents and their children. These variables and the relationship between them are explained as follows:
Dependent Variable
The outcome variable in this study is whether a parent having a child older than 10 years discussed (a) sexual relationship, (b) HIV/AIDS, and (c) Family Planning and Contraception with the child within 12 months preceding the survey.
Independent Variables
The independent variables used in this study include “sex of the respondents,” “age of respondents,” “educational attainment,” “religion,” “marital status,” “wealth status,” “location of residence,” and “geo-political zones.”
Statistical Analyses
First, we used descriptive statistics to show the distribution of the respondents who had children older than 10 years and the prevalence of discussions with their wards on (a) sexual relationship, (b) HIV/AIDS, and (c) family planning and contraception with the child within 12 months preceding the survey. We computed and showed a pattern of the prevalence of discussions on either or both HIV/AIDS and family planning and contraception (Table 2). Bivariate analyses were performed to determine the significance of the association between dichotomous dependent and independent variables using the Pearson Chi-square (χ2) test of association (Table 1). We used logistic regression to model the relationship between the dependent and independent variables at the bivariate level (Table 3). The significant independent variables in the bivariate analysis were adjusted for multiple logistic regression models. Logistic regression models are suitable where the variable of interest has binary outcomes. They determine the association between a dichotomous dependent variable and independent variables by converting the dependent variable to probability scores taking on values between zero and one as shown here:

where yi refers to different levels of the dependent variable for the ith observation and xij is the jth independent variable (j = 1,2,…k) for that observation. The parameter β j is the jth coefficient of covariate xij, and it indicates the effect of the covariate xij in the fitted model.
Results
Most of the respondents (54%) were between 35 and 49 years of age, and the proportion of male respondents was 48%. Table 1 shows the distribution of discussion of various types of reproductive health issues considered in this study, which respondents have had with their male and female wards. Discussion of sexual unions with male and female wards was higher among older parents than among younger parents. Fathers appeared to discuss sexual unions with their female child (38%) more than a male child (34%) while the levels of discussion on HIV/AIDS with female and male children were close at 35% versus 34%. Similarly, mothers discussed sexual unions more with their female child (40%) than with the male child (30%) and had more discussions on family planning and contraception with the female child (10%) than with the male child (7%). Generally, parents held more discussions with the female child than with the male child, for instance, 39% versus 32% on sexual unions, 33% versus 31% on HIV/AIDS, and 10% versus 7% on family planning and contraception. There were significant differences in parent–child communication on all topical issues considered both by sex of the children and zone of residence of the parents (Table 1 and Figure 1).
Distribution of Parents With Children Aged 11 Years Plus and Health Discussions Held With Wards by Gender.

Note. Discussions were with children aged 13+ years within 12 months preceding the survey. FPC = family planning and contraception.
Significant at 5% χ2 test.
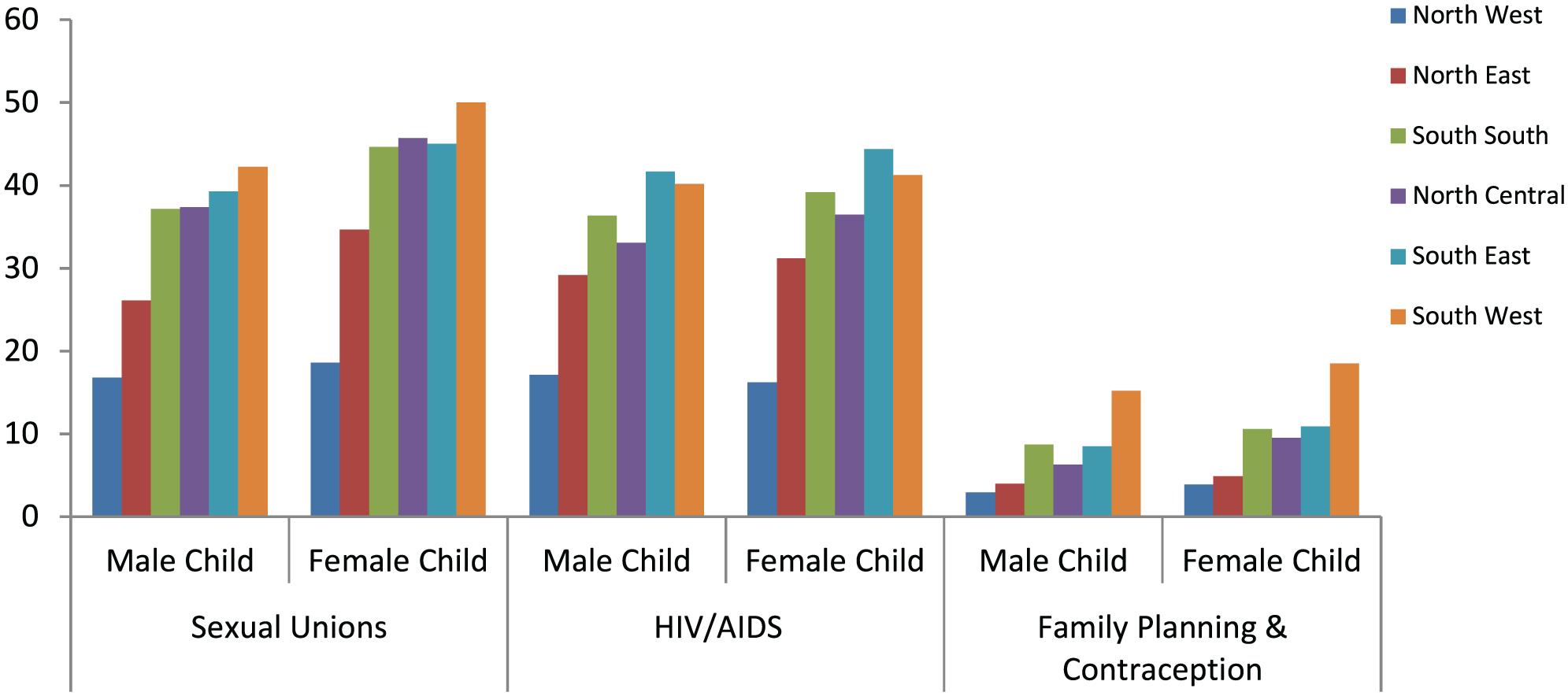
Distribution of parent–child communication on sexual unions, HIV/AIDS, and family planning and contraception by respondents’ zone of residence and sex of the child.
In Table 2, we showed levels of discussion with children irrespective of the sex of the children. Generally, only 37% of parents discussed sexual union with their children, compared with 33% discussing HIV/AIDS and less than 10% who discussed family planning and contraception with their wards within 12 months preceding the survey. Only one third (33%) of the parents discussed either HIV/AIDS or family planning with their wards while only 9% discussed both with their children. Discussions on the reproductive health issues with wards appeared higher among better-educated parents than less educated, higher among parents from households with higher economic status than those from poorer economic status. Discussion of family planning and contraception was higher among other Christians (12%) and Catholics (11%) than among the Islam believers (6%).
Distribution of Parents With Children Aged 13 Years Plus and Health Discussions Held With Wards.

Note. Discussions were with children aged 11+ years within 12 weeks preceding the survey. FPC = family planning and contraception.
Significant at 5% χ2 test.
At the bivariate level, the odds of discussing HIV/AIDS with wards increased with age of parents. Parents aged 50 to 64 years were double (OR = 2.04; 1.52-2.73) likely to discuss HIV/AIDS with their wards older than 13 years than the parents aged 20 to 24 years. Male parents and parents living in urban areas had higher odds of discussing HIV/AIDS with their wards. Parents living in the South West were more than three times (OR = 3.26; 2.82-3.77)likely to discuss HIV/AIDS and SRH issues with their wards. Parents with richer economic status were almost four times (OR = 3.56; 2.95-4.06) more likely to discuss family planning and contraception with their wards than were those with poorer economic status. While adjusting for other independent variables, respondents’ age, zone, economic status, educational attainment, and religious affiliation significantly determined whether a parent discussed HIV/AIDS with their wards. Determinants of discussions with children on family planning and contraception were respondents’ zone, economic status, educational attainment, and religious affiliation at the multivariate level. The odds of parents with higher education discussing family planning and contraception with wards tripled (adjusted OR [aOR] = 3.08; 2.40-3.96) the odds among parents with no formal education (Table 3).
Determinants of Parent–Child Discussions on HIV/AIDS and Family Planning Contraception.

Note. OR = odds ratio; CI = confidence interval.
Reference
Significant at 5%.
Discussion
We found a significant relationship between the sociodemographic characteristics and parent–child communication of HIV/AIDS and SRH in Nigeria. Prevalences of parent–child communication on sexual unions, HIV/AIDS, and SRH were generally at 37.4%, 32.5%, and 9.5%, respectively. On all health-related issues that parents discussed with their children, female children got their parents’ attention more than the male children at 39% versus 32%. Specifically, fathers discussed sexual unions with their female children (38%) more than they did with their male children (34%). Similarly, mothers discussed sexual unions more with their female children (40%) than they did with their male children (30%), and also had more discussions on family planning and contraception with female children (10%) than they did with their male children (7%). However, with regard to HIV/AIDS, both female and male children received almost equal levels of their parents’ attention (35% vs. 34%).
The inference from the foregoing findings is that Nigerian parents seemed to believe that female child deserve more attention than their male counterparts, in terms of sexuality and health communication, perhaps because of the perception that, compared with the male adolescents, the female adolescents are more vulnerable to health risks. This issue is a cultural stereotype in most African countries. As established in literature, African parents tend to give more attention to female children than their male counterparts especially in issues that have to do with risks associated with HIV, sex, and reproductive health (Bastien et al., 2011; Manu et al., 2015; Obono, 2012; Yadeta et al., 2014). For example, as Rivers and Aggleton (1999) explained, in most developing African countries, female adolescents are considered to be at heightened risks of HIV infection more than their male counterparts. Also, the cultural values placed on virginity in most African communities compels parents to give more attention to their female children in matters relating to SRH.
We also found that irrespective of the sex of their children, more parents (37%) discussed with their children issues about sexual union compared with 33% and less than 10% of the parents discussing HIV/AIDS and reproductive health issues, respectively, with their wards. This pattern suggests that parents preferred to discuss sexuality issues more while they gave the least attention to reproductive health matters in their communication with their children. Findings also show that the level of education and religious affiliations influenced the intensity and patterns of HIV/AIDS, and SRH communication in the family. Parents with higher education appeared to discuss reproductive health issues more with their wards than the less educated parents.
At the bivariate level, the probability of parents with higher education discussing family reproductive health (RH) issues with their wards tripled the odds among parents with no higher education. Also, parents with richer economic status were almost four times more likely to discuss family planning and contraception with their wards than those with poorer economic status. It could be inferred from the foregoing findings that the more educated and economically strong the parents are, the higher the likelihood that they would discuss HIV/AIDS and SRH issues with their wards. Our findings here share some level of similarity with a study by Yadeta et al. (2014), which reports that the probability of parent–adolescent discussion on RH issues in Harar, Eastern Ethiopia was found to be significantly higher among parents who had acquired some form of formal education compared with parents with no formal education.
Only 6% of Muslim parents, compared with 12% of Christians and 11% of Catholics, communicated health issues with their wards. Generally, as the findings confirm, economic status, level of education, and religion shape the patterns of discussion of SRH issues in Nigerian households, but religion appears to reduce the intensity of parent–child discussion of HIV/AIDS and SRH in Nigeria more than other factors. This is not surprising given the fact that apart from ethnicity, religion is another strong sociocultural index in Nigeria. A previous study by Mariga et al. (2012) also confirmed that religion, among other factors, was found to prevent effective discussion of HIV/AIDS and SRH issues among sexually active adolescents, especially those from the rural parts of Nigeria. Similarly, in a recent study by Ahmed et al. (2018), low social support, gender norms, and HIV stigma were among other factors why people from low- and middle-income countries would not discuss or initiate treatment of HIV/AIDS. Mpondo et al. (2018), in a study they conducted in South Africa, found that parent–child communication on sexual health matters in rural communities was limited to messages that warned against pregnancy, while the messages were also fraught with cultural idioms that could be difficult to comprehend because of their ambiguous meanings. These findings also confirm the findings of our study that sociocultural and demographic factors influenced discussion of HIV/AIDS and SRH issues between Nigerian parents and their children.
Findings of this study have implications for the HBM, which we adopted as the theoretical framework. The core tenet of the theory is anchored on the philosophy that some factors always serve as stimuli that shape people’s overall health behaviors. These factors include perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cue to action, self-efficacy, and demographic variables (Abraham & Sheeran, 2015; Taylor et al., 2007). It is interesting to note, as established in this study, that parents across Nigeria discussed HIV/AIDS and SRH issues with their children. However, what is more interesting is that these discussions were influenced by various sociodemographic determinants such as respondents’ zone, economic status, educational attainment, and religious affiliation at the multivariate level. We, therefore, consider it relevant to explain how our findings here are relevant to the tenets of the HBM. The model operates on the principle that people’s decisions and communication about issues relating to their health are always influenced by some key variables as already identified earlier. In order words, how people modify their behavior and how they discuss a given health issue depend largely on the values they place on some variables that have implications for their total well-being. This principle is what is described as value-expectancy (Brewer & Rimer, 2008). As the HBM provides, whether an individual would discuss some health issues or change his or her behavior in response to the health issues is often influenced by a number of factors (Abraham & Sheeran, 2015; Taylor et al., 2006), one of which is the nature of demographic variables, which our study examined.
Our present study has established that demographic characteristics influenced communication about HIV/AIDS and SRH issues between parents and their children across Nigeria. As the findings showed, patterns and intensity of communication about HIV/AIDS and SRH in Nigerian households vary according to the identified demographic variables. This suggests that, for instance, male parents’ perception of, and subsequent discussion about, HIV/AIDS and SRH issues are different from that of female parents. The same phenomenon applies to younger parents versus older parents, rich parents versus poor parents, parents with formal education versus parents without formal education, parents who reside in urban places versus parents from less-urban places, and religious affiliations. Also, Nigerian parents communicate about HIV/AIDS, sexuality, and reproductive issues with their female wards more often than they do with their male children.
Conclusion
The primary objective of this study was to establish the factors that influenced the patterns and frequency of parent–child discussion about HIV/AIDS and SRH in Nigerian households. This study is different from most of the previous similar studies from Nigeria, which focused on some regions or ethnic constituents of the country. The present study relied on a body of nationally representative cross-sectional data from a NARHS. The implication is that findings of this study have a high generalizability value.
We found that parent–child communication of HIV/AIDS and SRH issues is generally low in Nigerian households, and the patterns of this prevalence are not even. Different sociodemographic variables such as respondents’ zone, economic status, educational attainment, and religious affiliation of respondents influenced this prevalence. For instance, parent–child communication of HIV/AIDS and SRH issues was higher in richer households than in poorer households, higher in families with highly educated parents than with parents with lesser or no formal education, and most prevalent in the Southwestern part of Nigeria but least prevalent in the Northern region of the country. On the same subjects, female adolescents received their parents’ attention than their male counterparts did. The fact that Nigeria is a heterogeneous nation with high variations in terms of ethnicity, religion, cultural values, and other demographic variables suggests that patterns and intensity of discussing HIV/AIDS and SRH among the citizens are not expected to be even across the country. Given these variations, health communication scholars and stakeholders should be sensitive to sociodemographic variables that always influence prevalence and patterns of parent communication of HIV/AIDS and SRH issues especially in a setting such as Nigeria with manifest sociocultural heterogeneity. Although the importance of HIV/AIDS communication on controlling the transmission of HIV/AIDS is replete in literature, the findings of our study showed that HIV/AIDS communication among parents and their wards is generally poor in Nigeria, especially among parents with lower educational and poorer economic status. Educational attainment of parents and wealth status of their households are main predictors of the likelihood of parents to engage their wards in HIV/AIDS communication. This would have negative consequences on the awareness of HIV/AIDS, and knowledge about transmission and prevention of HIV/AIDS and the possibility of adopting good control measures. Given the fact that greater exposure to HIV/AIDS communication could enhance HIV knowledge, encourage condom use, encourage HIV counselling and testing, discourage risky sexual behaviors, and reduce discrimination and stigmatization of people living with HIV/AIDS, there is the need to give urgent and sincere attention to issues that could improve parent–child communication to curtail the incidence and prevalence of HIV/AIDS.
Health communication on HIV/AIDS and SRH could be improved by first targeting the parents and guardians in a massive campaign against HIV/AIDS. Such massive campaigns will increase the knowledge base of parents on HIV/AIDS, which they can in turn pass on to their children. The capacity of parents and guardians to discuss this important health topic should be developed. Similarly, the misconception of some parents that sexual issues should not be discussed with children should be corrected as the knowledge gap created by absence of this communication could be detrimental in the long run. Parents should be made to understand that communication on HIV/AIDS and SRH between them and their wards is crucial. They should not allow their children to be misinformed by peers and other people outside the family.
Study Limitation and Strength
Secondary data from a survey that requires event recall was used for this study. It is not unlikely, therefore, that recall bias might have been introduced. However, the large size of the data might have eroded a likely effect of such bias on our findings. Besides, studies on the effect and influence of parent–child communication as a strategy to prevent the spread of HIV/AIDS in Africa is relatively scanty, especially in recent times. The present study, therefore, addressed one of the multisectoral approaches to reduction of the scourge of a contemporary public and clinical health problem ravaging developing countries.
Footnotes
Acknowledgements
We acknowledge the Nigeria Federal Ministry of Health for allowing the use of these data. The authors acknowledged the technical support received from North-West University (Mafikeng Campus), South Africa, and the Consortium for Advanced Research Training in Africa (CARTA).
Authors Contributions
B.R.O. and A.F.F. conceived the study and developed the research questions. A.F.F. designed the study, analyzed data, and wrote the methodology and the results and contributed to writing the introduction. B.R.O. contributed to the introduction and literature, and wrote the theoretical framework and discussion. O.O.A. partook in writing the introduction. All authors proofread the final version of the manuscript.
Data Sharing Statement
This study used data from a national survey conducted in 2012. The data used and some data, which are not reported in this study, are readily available on request from the Nigeria Federal Ministry of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.