
Abstract
Black people comprise 4.3% of Ontario’s population but 19% of HIV-positive people in the province. The “Keep it alive!” social marketing campaign was developed to promote HIV prevention and raise awareness about HIV among Ontario’s Black communities. This article evaluates the campaign’s reception. A convenience sample of 243 Black people completed a cross-sectional self-administered survey in three cities. We assessed the campaign’s reception based on survey responses about campaign exposure, appeal, and importance, and whether the campaign raised awareness. Our results show that reception was more favorable among participants who tested for HIV previously, discussed the campaign with others, demonstrated a superior knowledge of HIV, visited the campaign website, were of Caribbean or African background, and were male. In addition, reception varied by city and according to participants’ language (English or French). These results may inform future campaigns, although how campaigns are received may reflect issues related to their implementation.
Introduction
Black people constitute only 4.3% of Ontario’s total population (Statistics Canada, 2013), but in 2009, Black people infected with HIV through heterosexual contact accounted for 18.8% of the estimated number of people living with HIV in the province (Remis, Swantee, & Liu, 2012). Although unprotected sex is the main factor directly responsible for transmission of HIV among Black people in Ontario, previous research has drawn attention to the role of community practices and systemic factors that reinforce vulnerability to HIV among this group (Gardezi et al., 2008; George et al., 2012; Gray, Calzavara, & Tharao, 2008; Husbands et al., 2010; Tharao, Massaquoi, & Teclom, 2006).
The African and Caribbean Council on HIV/AIDS in Ontario (ACCHO) has coordinated or spearheaded a number of programs, policies, and research initiatives to promote community awareness, strengthen HIV prevention, and improve access to care, treatment, and support. In 2006-2009, ACCHO developed and implemented the “Keep it alive!” (KIA) social marketing campaign (SMC) to promote greater awareness about HIV among Black communities in Ontario, particularly in relation to HIV prevention (safer sex and HIV testing), stigma reduction, and creating a supportive environment for people living with HIV.
In this article, we present results from the KIA evaluation study to determine how the campaign was received among Black communities in three of Ontario’s largest cities—Toronto, Ottawa, and London. Our primary objectives are to (a) evaluate the impact of the KIA campaign on people’s self-reported awareness about HIV and (b) assess the campaign’s attractiveness to Black people in the aforementioned cities. Our secondary objectives address two principal issues. First, we assess how the campaign resonated with Black communities in the three cities (i.e., which groups of people were reached by the campaign or were more likely to attribute increased awareness of HIV to the campaign). Second, we explore the associations between demographic, geographical, and other factors (e.g., HIV-related stigma, history of HIV testing, level of exposure to the campaign) and people’s assessment of the campaign (i.e., self-reported awareness about HIV, appeal and importance of the campaign). These objectives may inform the development of future social marketing campaigns for African diasporic communities in Canada and abroad with disproportionately high numbers of HIV infections. For example, in Canada, Black people accounted for 17.9% of positive HIV test results from 2009-2012 (Public Health Agency of Canada, 2013). Similarly, in the United Kingdom, for example, Africans accounted 24% of new HIV diagnoses in 2012 (National AIDS Trust, 2014).
The “Keep It Alive!” Campaign
ACCHO developed the KIA campaign with funding from the AIDS Bureau, Ontario Ministry of Health and Long-Term Care. The campaign was implemented in seven locales—Toronto, Ottawa, London, Windsor, Peel Region, Hamilton, and Thunder Bay—in which the overwhelming majority of Black people in Ontario and Black Ontarians living with HIV reside. The campaign conveyed messages about stigma, safer sex, and HIV testing by appealing to community values of self-respect, love, family, potential, pride, and friendship, and by portraying Black people as capable of leading change. KIA was inspired by two theoretical traditions: theories of health and behavior change (e.g., Health Belief Model), which assert that people may adopt life-enhancing practices if they become more knowledgeable about the benefits of change (Rosenstock, 1988), and inspiring people to change attitudes, beliefs, and practices, which entails engaging individuals and communities as capable agents of change (Campbell, 2003).
Phase 1 of the KIA campaign was launched in the spring of 2006. This phase began with a range of preliminary activities that included the formation of a coordinating committee, hiring of a communications company (Top Drawer Creative), and conducting focus groups in Toronto and Ottawa to help shape the campaign. This was followed by the development of the campaign’s theme, content, branding, and media strategy. Last in Phase 1, the campaign was delivered through advertisements on billboards, in public transit, and in community newspapers; posters, postcards, and pamphlets distributed through community organizations and community events that attracted primarily Black audiences; and on radio through a rap music advertisement. The print materials publicized a website that gave more in-depth information about HIV and ACCHO. Phase 2 was launched in 2007 with seven TV advertisements that were strategically aired in February and March during a popular sitcom that appealed to Black people, and the advertisements were repeated throughout the summer. The TV advertisements showcased individuals speaking to their significant others or Black communities, using scripts they prepared with assistance from the campaign committee and communications company. The TV advertisements emphasized HIV prevention, stigma reduction, and the well-being of people living with HIV.
Health and HIV-Related Social Marketing Campaigns in Perspective
KIA was similar to other health- and HIV-related SMCs that use mass media or mass communication techniques to influence how people think about or manage their health. Through SMCs, health agencies promote the benefits of certain attitudes, norms, or behaviors by appropriately framing the health-related issue for the target audience, disseminating credible information about the issue, and recommending how the targeted individuals or communities can address or resolve the issue (Coffman, 2002; Randolph & Viswanath, 2004; Wakefield, Loken, & Hornik, 2010).
SMCs are widely used to address a variety of health issues, such as to promote healthy behaviors and choices (Elder et al., 2004), discourage smoking (Alekseeva, Alekseev, & Chukhrova, 2007; Dietz, Delva, Woolley, & Russello, 2008; Gagné, 2007; Klein, Havens, & Carlson, 2005; Secker-Walker, Worden, Holland, Flynn, & Detsky, 1997), and promote safer sex practices (Zimmerman et al., 2007). Mass media campaigns may also challenge misguided views on sensitive health and social issues, such as HIV (Wolffers, 1997). Canadian AIDS service organizations and public health authorities have used SMCs extensively in response to HIV, particularly among gay and other men who have sex with men (MSM) (Ross & Rynard, 2007; Trussler & Marchand, 2005). On the whole, SMCs may be cost-effective vehicles or platforms for health promotion (Geary, Burke, Castelnau, Neupane, Sall, & Wong, 2007; Myhre & Flora, 2000; Wakefield et al., 2010), due to their wide reach and relatively low cost. In this vein, Snyder and colleagues (2004) have suggested that campaigns have “small but tangible effects” (pp. 89-90) and may be more cost-effective than clinical interventions that are developed for individuals or small groups.
Noar, Palmgreen, Chabot, Dobransky, and Zimmerman (2009) have suggested that showing causal evidence for behavior change should be the gold standard of campaign evaluations. However, it is questionable whether SMCs should stand or fall on this basis (Adam et al., 2011; Airhihenbuwa & Obregon, 2000; Coffman, 2002), because (a) the target audiences may be exposed to multiple sources of information in the “real world,” (b) the pervasive stigma associated with HIV may hamper adherence to the campaign messages, (c) some of the putative outcomes of HIV-focused SMCs may not be amenable to a linear causal effect (e.g., promoting community awareness, prioritizing HIV on community agendas, building trust in community organizations, etc.), (d) some campaigns have multiple objectives depending on the level of awareness or understanding of HIV among the target community, and (e) discernible behavior change in a community may emerge over an extended time horizon. In short, it may be logically or methodologically impossible to attribute changes in individual or community attitudes or behaviors to a specific SMC.
Studies to evaluate the effect or impact of HIV-related SMCs among target audiences are mostly post-campaign population surveys, or pre- and post-campaign surveys of a single group or cohort. Most evaluation surveys assess correlates of awareness or exposure to campaigns among the respective target populations (Adam et al., 2011; Agha, 2003; Fraze et al., 2009; Geary, Burke, Castelnau, Neupane, Sall, & Wong, 2007; Geary, Burke, Castelnau, Neupane, Sall, Wong, et al., 2007; Plant et al., 2010; Ross & Rynard, 2007; Trussler & Marchand, 2005). Evaluation studies also assess the adoption of protective behaviors among target populations consequent to the introduction of an SMC, and supplement surveys with relevant data on health system utilization (Davis, Uhrig, Rupert, et al., 2011; Gibson et al., 2010; Guy et al., 2009; Martínez-Donate et al., 2009; Olshefsky, Zive, Scolari, & Zuñiga, 2007; Pedrana et al., 2012; Pettifor, MacPhail, Bertozzi, & Rees, 2007; Snyder et al., 2004; Vidanapathirana, Abramson, Forbes, & Fairley, 2006). Changes in health knowledge after exposure to an SMC (Plant et al., 2010), or how campaign messages were received or understood (Ross & Rynard, 2007; Trussler & Marchand, 2005), can be assessed in evaluation studies as well.
The effectiveness of SMCs in HIV prevention is well documented (Bertrand & Anhang, 2006; Bhatia, Swami, & Kaur, 2004; Farr, Witte, Jarato, & Menard, 2005; Geary, Burke, Castelnau, Neupane, Sall, & Wong, 2007; Geary, Burke, Castelnau, Neupane, Sall, Wong, et al., 2007; Sood & Nambiar, 2006). Many studies have reported that people exposed to mass media campaigns are more likely than the unexposed to know that using condoms reduces the risk of HIV infection (Keating, Meekers, & Adewuyi, 2006), to discuss HIV/AIDS with a partner (Keating et al., 2006; Sood & Nambiar, 2006; Walls, Lauby, Lavelle, Derby, & Bond, 1998), and to be tested for HIV (Olshefsky et al., 2007). Messaging is a critical element of any SMC, and it has been demonstrated that people who rate the message as being effective early in the campaign have stronger intentions to adopt the behavior promoted by the message (Davis, Uhrig, Bann, Rupert, & Fraze, 2011). Of course, HIV-related campaigns are not uniformly received or interpreted among target populations because target populations are neither uniformly constituted nor uniformly exposed to the subject matter.
Methods
The “Keep It Alive!” Evaluation Survey
The KIA survey was implemented in Black communities in Toronto, Ottawa, and London. The goal and objectives of the KIA evaluation study have been outlined in the “Background” section of this article. The study received ethics clearance from the Research Ethics Board at the University of Ontario Institute of Technology.
Between September 2009 and March 2010, we recruited a convenience sample of 243 survey participants. Participants were recruited from a variety of sites and events frequented by Black communities, including barbershops/hair salons, universities, cafés, community events, community organizations, churches, and restaurants. Participants had to be at least 18 years old and identify as African, Caribbean, or Black.
Measures
The survey instrument was a self-administered questionnaire available in English and French. The questionnaire collected information on the following outcomes: participants’ exposure to the campaign’s images, participants’ exposure to the TV advertisements, participants’ self-rated evaluation of the appeal of the images, whether the campaign raised awareness of HIV among Black communities, and the importance of the campaign. The questionnaire also solicited other information, including participants’ socio-demographic background and whether participants discussed the campaign with others. In addition, we assessed HIV-related stigma among participants using the scale developed by Visser, Kershaw, Makin, and Forsyth (2008). Participants’ HIV knowledge was assessed using the scale adopted from the U.S. Centers for Disease Control and Prevention’s National Health Interview Survey and modified by Leake, Nyamathi, and Gelberg (1997; Centers for Disease Control and Prevention, 1989; ). We also included an item to assess participants’ willingness to disclose a positive HIV test: “If you found out that you were HIV positive, who would you tell?” followed by a list of different types of people with whom participants may have relationships (e.g., father, mother, spouse/partner, doctor, religious leader, etc.) and whether they would tell (definitely, maybe) each type of person, or not.
The campaign lasted 3 years (2006-2009), and the evaluation started in September 2009, a few months after the campaign ended. We anticipated that some participants may have had difficulty recalling the campaign. Therefore, we inserted images and screenshots from the respective print materials and TV advertisements to accompany questionnaire items about exposure to the KIA campaign.
Statistical Analysis
We analyzed the survey data using SAS software, Version 9.3 (SAS Institute Inc, 2011). Bivariate analysis was performed using Pearson chi-square test to examine associations between variables. All independent variables were included into the multivariable logistic regression model and were reduced using backward elimination with a critical point of 0.15. The logistic regression model for the importance of the campaign was built using the Firth penalized likelihood method, because there was quasi-complete separation of the data when the maximum likelihood method was used (Heinze, 2006; Heinze & Schemper, 2002). The logistic regression models were used to calculate prevalence odds ratios (PORs) and corresponding 95% Wald confidence limits.
Results
Description of Sample
Most survey respondents were from Toronto, and about equal proportions were from London and Ottawa (Table 1). In terms of its basic demographic composition, the sample included more women than men, was relatively young (only one quarter of the participants were 40 years or older), and was fairly well-educated (one third had completed their education at the tertiary level, and an additional 25% had commenced their tertiary education). In addition, most participants were African-born or of African ethnicity, and English-speaking (although people who spoke predominantly English or French—Canada’s two official languages—accounted for three quarters of the sample).
Demographic Characteristics of the “Keep It Alive!” Evaluation Sample.

M (SD).
Exposure to the Print Images and TV Advertisements
The city of residence was associated with seeing the campaign’s images (p = .0014). For instance, compared with people in Toronto, people in Ottawa were less likely (POR = 0.40; 95% confidence interval [CI] = [0.20, 0.81]) to have seen the images from the campaign (Table 2). Age, gender, education, time spent in Canada, place of birth, having a past HIV test, and general health rating were not associated with being exposed to the print images in the bivariate or multivariable analyses.
Determinants of Exposure to “Keep It Alive!” Campaign’s Images and TV Ads.

Note. POR = prevalence odds ratios; CI = confidence interval; adj = adjusted; PORadj = adjusted prevalence odds ratio.
Multivariable model controlled for city and ethnicity. Ethnicity and language ability were coded as dummy variables because the categories were not mutually exclusive.
Multivariable model controlled for African ethnicity and having an HIV test in the past. Ethnicity was coded as a dummy variable because its categories were not mutually exclusive.
Statistically significant.
As Table 2 also shows, participants who had previously tested for HIV were more likely to report that they saw the KIA television advertisements when compared with those who had never been tested (p = .0425). In the adjusted model, being of Caribbean ethnicity (POR = 2.33; 95% CI [1.13, 4.81[) and having had a past HIV test (POR = 1.99; 95% CI = [1.02, 3.88]) were associated with seeing the advertisements. There was no evidence that age, gender, education, time spent in Canada, place of birth, language, or general health rating was related to seeing the TV advertisements in the crude or multivariable analyses.
Appeal of the Images
Participants who lived in London or Ottawa were more likely than those from Toronto to rate the KIA images as appealing (p = .0006; Table 3). The images were also more appealing to people who had conversations about them (p = .0208), those who had visited the website (.0092), and those with lower stigma scores (.0076). In the adjusted model, finding the images appealing was associated with living outside of Toronto (p = .0001), having a conversation about the images (POR = 3.23; 95% CI [1.01, 10.35]), visiting the KIA website (POR = 11.49; 95% CI = [1.01, 130.28]), and having higher HIV-related knowledge (POR = 1.18; 95% CI [1.01, 1.37]; Table 3). The results from the crude and adjusted analyses suggest that the appeal of the images was not related to gender, education, ethnicity, time spent in Canada, place of birth, language, having a past HIV test, or general health rating.
Determinants of Finding the “Keep It Alive!” Campaign’s Images Appealing.

Note. Multivariable model controlled for city, age, time spent in Canada, the frequency with which images were seen, having a conversation about the images, visiting the Keep It Alive website, HIV stigma score, and HIV knowledge score. POR = prevalence odds ratios; CI = confidence interval.
Statistically significant.
Images and Awareness of HIV
Table 4 shows that participants of Caribbean ethnicity were more likely to say the images raised their awareness of HIV when compared with people who did not identify as having a Caribbean ethnicity (p = .0461), and people of Canadian ethnicity were less likely to believe the images raised their awareness compared with people without Canadian ethnicity (p = .0219). In the adjusted model, living in London was associated with believing that the images raised awareness when compared with living in Toronto (POR = 2.71; 95% CI = [1.15, 6.37]), and visiting the KIA website was associated with saying that the images raised awareness (POR = 4.10; 95% CI [1.10, 15.30]). Being of African ethnicity was associated with saying the images did not raise awareness (POR = 0.41; 95% CI = [0.18, 0.94]). Based on this study, gender, education, time spent in Canada, language, general health rating, and HIV knowledge score did not affect whether or not a participant believed the KIA images raised his or her awareness about HIV.
Determinants of Reporting that the “Keep It Alive!” Campaign’s Images Raised Awareness.
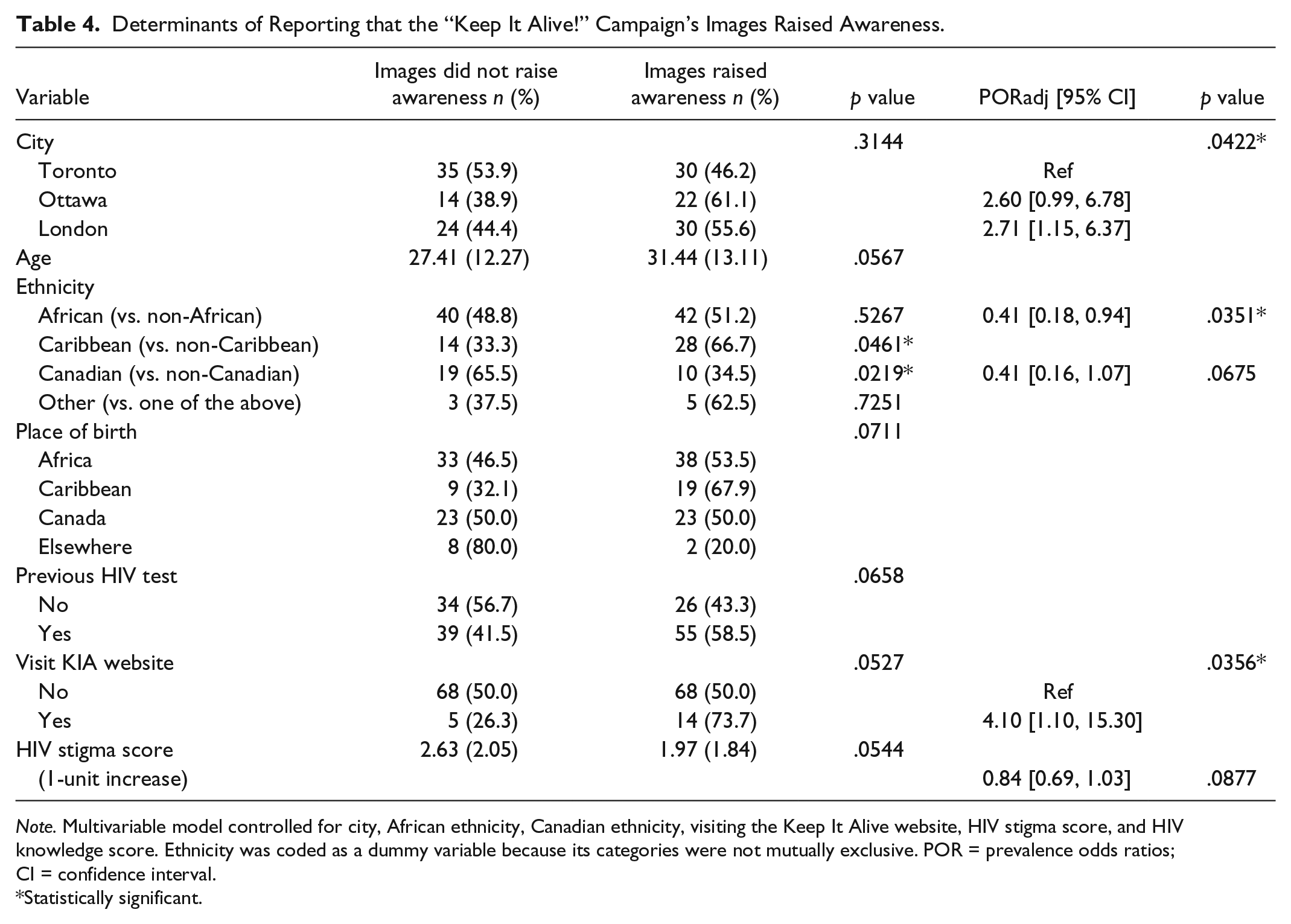
Note. Multivariable model controlled for city, African ethnicity, Canadian ethnicity, visiting the Keep It Alive website, HIV stigma score, and HIV knowledge score. Ethnicity was coded as a dummy variable because its categories were not mutually exclusive. POR = prevalence odds ratios; CI = confidence interval.
Statistically significant.
Importance of the Campaign
As seen in Table 5, men were more likely than women to say the campaign was important (p = .0041). During the evaluation, all survey participants saw the images from the KIA campaign, and regardless of whether or not they had seen the campaign directly, all were asked to provide their opinions on the campaign’s importance. Those who were exposed to KIA directly were more likely to think the campaign was important than those who had only seen the images in the evaluation survey (p = .0003). In the adjusted model, being male (POR = 8.89; 95% CI = [1.91, 41.36]), speaking French (POR = 6.77; 95% CI [1.25, 36.69]), and being exposed to the campaign (POR = 5.89; 95% CI = [1.58, 21.95]) were associated with believing the campaign was important. The results of the analyses did not provide evidence of education, amount of time spent in Canada, place of birth, having a past HIV test, general health rating, visiting the KIA website, HIV stigma score, and HIV knowledge score affecting participants’ ratings of the campaign’s importance.
Determinants of Reporting that the “Keep It alive!” Campaign Was Important.
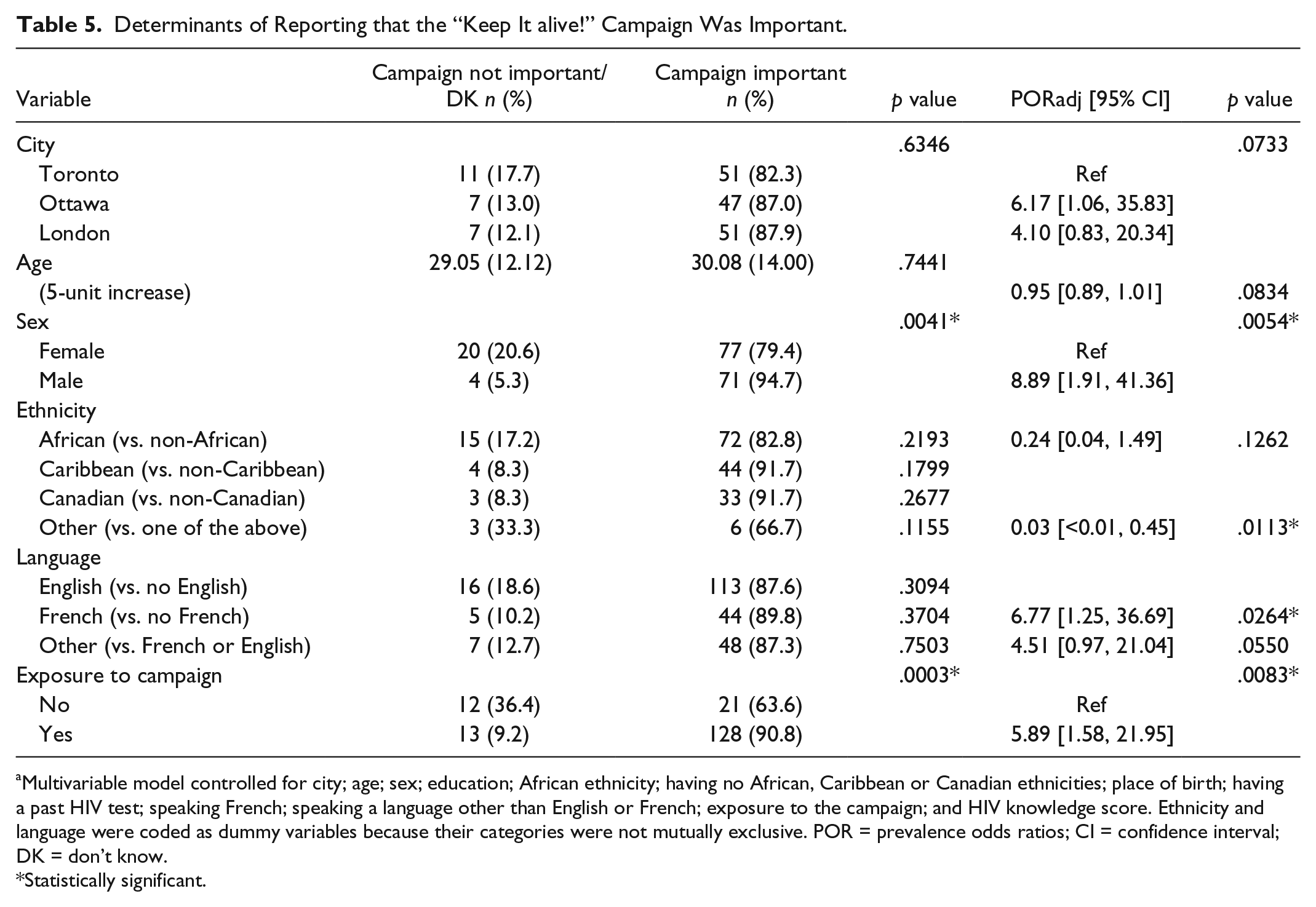
Multivariable model controlled for city; age; sex; education; African ethnicity; having no African, Caribbean or Canadian ethnicities; place of birth; having a past HIV test; speaking French; speaking a language other than English or French; exposure to the campaign; and HIV knowledge score. Ethnicity and language were coded as dummy variables because their categories were not mutually exclusive. POR = prevalence odds ratios; CI = confidence interval; DK = don’t know.
Statistically significant.
Interpretation
We examined how outcomes of an HIV SMC—exposure, appeal, awareness, and importance—emerged among Black people in Ontario. Our findings suggest that exposure to the campaign, the rated appeal and importance of the campaign, and participants’ assessment of whether the campaign raised their awareness of HIV among Black communities varied across Ottawa, Toronto, and London. Reception of the campaign was more favorable among participants who tested for HIV previously, discussed the campaign with others, demonstrated a greater knowledge of HIV, visited the campaign website, were of Caribbean or African ethnicity, and were male. In addition, the campaign’s reception varied by city and participants’ first language (English or French). More generally, our results suggest that people who were already sensitive to or substantively aware of the issues were more inclined to pay attention to the campaign and assess it favorably. The results also suggest that implementation issues (i.e., management of a SMC) may have influenced how the campaign was received among the target audience, as discussed below.
Residents of Toronto and London reported seeing the KIA images at higher rates than those located in Ottawa. Toronto participants’ reportedly greater exposure to the KIA images may have been influenced by their exposure to multiple sources of information—the initial launch of the campaign coincided with the XVI International AIDS Conference in Toronto in 2006, which brought a substantial amount of media attention to HIV/AIDS. In addition, a campaign targeting MSM was running concurrently with the KIA campaign and the International AIDS Conference. The social climate at that particular time with regard to raising HIV as an issue in Toronto may have heightened people’s awareness and may also have had an impact on participants in Toronto being able to recall the KIA campaign images at the time of the evaluation.
Fewer survey participants in Ottawa saw the campaign images, compared with London and Toronto. Ottawa has a substantial French-speaking Black community. The French translation and dissemination of the KIA images in Ottawa proved to be challenging throughout this component of the campaign, which may have limited Ottawa participants’ accessibility to the campaign in a city with a relatively large French-speaking community. Ottawa residents saw the campaign in both English and French, but the French component was rolled out later and was less intense (fewer advertisements) than the English component. The KIA material invited people to go to a website where they could learn more about ACCHO’s Strategy on HIV for Black communities in Ontario (HIV Endemic Task Force, 2003), epidemiological issues related to HIV among Black communities, and what individuals and communities could do to reduce the spread and impact of HIV among Black communities. However, the French website became available after the English version, which may also have contributed to making the campaign less accessible to people in Ottawa.
The analysis showed that participants who recalled seeing the television advertisements were more likely to have been tested for HIV. It is likely that people who have prior involvement in, or connection to, HIV issues (such as getting tested) may be more inclined to notice the campaign, and that people who tested for HIV in the past continue to be informed about or sensitive to HIV issues.
The study results showing that people of Caribbean ethnicity were more likely to see the TV advertisements may also be partially explained by how the advertisements were positioned on TV. In Ontario, some elements of the KIA campaign appeared during a very popular Caribbean-themed sitcom that was based in Toronto. The TV advertisements may have thus been more readily identifiable by people of Caribbean ethnicity but less so among Blacks with other ethnicities. As such, health promoters should be conscious of cultural differences among a target population that may result in some people exempting themselves from health promotion initiatives.
Overall, participants deemed the KIA images to be appealing although there were substantial differences between the three cities. Participants in London and Ottawa were more likely than their Toronto counterparts to find the KIA images appealing. The images were also judged to be more appealing by participants who indicated that they discussed the campaign with others, visited the campaign website, demonstrated lower levels of stigma, and were more knowledgeable about HIV. People with such attributes (high knowledge, low stigma) were not only more likely to rate the appeal of the KIA images highly but also appeared to be more receptive to the campaign as a whole.
Participants in London reported that the KIA images raised their awareness more so than those in Toronto. As discussed previously, the social climate in Toronto due to the International AIDS Conference and other ongoing campaigns may have made people more cognizant of HIV issues and created a general awareness of HIV in the city, which cannot be attributed solely to the KIA campaign.
It should be noted that men were more likely than women to rate the campaign as important. Based on our experience working with Black communities over several years, it appears that Black women are much more publicly involved in community responses to HIV than Black men (heterosexual men in particular). We are hopeful that men’s response to the campaign leads to their increased involvement in community responses to HIV, and increased effort by AIDS service organizations to meaningfully engage men in those responses.
This study addresses an important gap in knowledge about HIV-focused SMCs for Black people in Canada (and the African diaspora). Although the KIA evaluation shares the same purpose or general approach as other studies reported in the literature, it differs from these studies due to their locations, populations, methods, and measures. We identified three studies (reported in four publications) that appear to be closest to the KIA evaluation in some combination of location, population studied, purpose, or approach (Adam et al., 2011; Davis, Uhrig, Bann, et al., 2011; Davis, Uhrig, Rupert, et al., 2011; Keating et al., 2006). The results from the three studies are similar to those of the KIA evaluation and suggest that people who tested for HIV previously or subsequently, and those who discussed the campaign with others, are more likely to report being exposed to a campaign or rate it favorably. In other words, campaigns seem to generate action (getting testing or spreading the word), or attract the attention of previous testers who may use the campaign as an opportunity to have conversations about HIV. The campaigns may allow people who are living with HIV to raise the subject among their social circle without also raising suspicion that they themselves are HIV positive.
Limitations and Conclusion
Our results indicate how certain segments of the Black communities in three of Ontario’s largest cities encountered, understood, and assessed the KIA SMC. The results of this and similar assessments of health-related social marketing campaigns may be prescriptive only to a limited degree. In the current example, should ACCHO, its agency affiliates, and policy makers focus on engaging Black people who were drawn to the campaign? Or should those parties renew their efforts to reach those who were unaware of KIA or for whom it lacked appeal and importance? Some observers may respond affirmatively to both questions. Certainly, quantitative assessments of social marketing campaigns often cannot explain with sufficient depth or detail the reasons behind the differential reception of a campaign among its target audience. Indeed, the reasons why a campaign is assessed in different ways among a target population may reveal more about the activities to develop and implement the campaign than about the target population. Consequently, in addition to the questions noted above, health promoters and communication specialists may need to evaluate the approaches, assumptions, knowledge, and tools that drive campaign development and implementation.
Two specific limitations are worthy of note. First, the study was based on a convenience sample of Black people in three cities in Ontario. Therefore, caution should be exercised in applying the study results to the Black communities in each of the three cities or in Ontario as a whole. Second, we implemented the study a few months after Phase 2 of the campaign had ended, but up to 3 years after ACCHO first launched the campaign. Some participants may have experienced problems recalling various elements of the campaign, although the survey questionnaire included cues to aid recall (e.g., some of the campaign images and screenshots of the TV advertisements).
As noted earlier, HIV social marketing campaigns in Canada are not uniformly received and interpreted among the respective target audiences. This was demonstrated in participants’ differential reports on exposure to the campaign, appeal and importance of the campaign, and their assessment of whether the KIA raised their awareness of HIV among Black communities in Ontario. Of course, Black communities in Ontario and Canada as a whole are heterogeneous, but our results underline the importance of better understanding how and why campaigns are received in varying ways within a targeted population. In addition, the findings raise awareness about the complexity of designing and implementing a positive campaign focused on values and resilience in a community so diverse, even if unitary in many respects. On the whole, our results suggest important lessons for future campaigns and implications for community-based responses to HIV in Black communities in Ontario.
Footnotes
Acknowledgements
Special thanks to all the survey participants. As well, we thank the following people for their contributions: Haile Fenta, Frantz Brent-Harris, Oumar Ongoïba, Rose-Anne Bailey and Felicité Murangira. Additionally, we would like to thank the following organizations and their staff for assistance with various aspects of the campaign and research: the African and Caribbean Council on HIV/AIDS in Ontario (ACCHO), the Ontario HIV Treatment Network, the Regional HIV/AIDS Connection, the AIDS Committee of Ottawa, Africans in Partnership Against AIDS, Women’s Health in Women’s Hands Community Health Centre, and the AIDS Committee of Toronto.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The KIA evaluation was supported by the AIDS Bureau, an entity of the Ministry of Health and Long-Term Care in Ontario, Canada. Winston Husbands was supported by a Community Scholar Award from the Ontario HIV Treatment Network. Neither funder is responsible for the content of this paper.