
Abstract
Loss to follow-up contributes to the low coverage of HIV care interventions among HIV-exposed infants in Beira, Mozambique. This qualitative study explores the perceptions of HIV-infected women and their health care providers regarding the main obstacles preventing women from attending follow-up visits for HIV care, and factors influencing women’s decisions about newborn care. Fifty-two in-depth interviews and two focus group discussions were conducted; transcripts were coded and analyzed using ATLAS.ti. Interviewees perceived three major barriers to follow-up: food insecurity, difficulties navigating the health system, and women’s familial roles and responsibilities. Our findings unveil the complex context in which HIV-infected women and their children live, and suggest that the structure and function of the HIV care system should be reviewed. Economic empowerment of women is crucial to achieving better compliance with medical care. Integration of mother and child services and more efficient and culturally sensitive medical services may improve follow-up.
Introduction
Mozambique is among the countries most affected by the HIV/AIDS epidemic. By 2011, nearly 1.5 million of its population (all ages) and approximately 130,000 children below the age of 15 years were living with HIV or AIDS (United Nations Children’s Fund [UNICEF], 2012). Mother-to-child HIV transmission is a devastating consequence of the spread of HIV. To respond to this problem, the Mozambique Ministry of Health rapidly expanded HIV-related care services to prevent mother-to-child transmission (PMTCT) of HIV and care for infants born to HIV-infected mothers, including the provision of cotrimoxazole prophylaxis, HIV early diagnosis by Deoxyribonucleic Acid Polymerase Chain Reaction (DNA PCR), and antiretroviral treatment (ART). Despite this commitment, the health system has had limited success in providing care to HIV-exposed children. Although national data suggest treatment is increasing, the 2009 figures account for only 19% of eligible children receiving ART (UNICEF, 2009).
One reason for low coverage of HIV care interventions among HIV-exposed infants is the high rate of loss to follow-up (LTFU) of these children in postnatal HIV care. Based on routine program data from HIV treatment clinics in Beira, the capital of Sofala Province in Mozambique, approximately 60% of HIV-positive pregnant women and 50% of HIV-exposed children miss >3 successive clinic visits. Other studies in sub-Saharan Africa found similarly low follow-up rates among HIV-positive women and their infants in postpartum care (Jones, Sherman, & Varga, 2005; Manzi et al., 2005; Wiktor et al., 1999).
Several issues may contribute to LTFU among HIV-exposed infants, including health system factors (e.g., long waiting times, disrespectful treatment by health staff, and uncoordinated referrals between different HIV services; Braun et al., 2011; Orner et al., 2008) and patient factors (e.g., chronic illness, family responsibilities, forgetfulness, lack of understanding, and distrust of health staff; Robiner & Keel, 1997; Robiner, Yozwiak, Bearman, Strand, & Strasburg, 2009). Transportation costs, inadequate spousal or family support, and fear of HIV/AIDS-related stigma and discrimination may discourage women from seeking care (Jones et al., 2005; Maman, 2007; Manzi et al., 2005; Painter et al., 2005). Finally, structural factors, including the physical, social, cultural, organizational, community, economic, or policy aspects of the environment, can act as barriers or facilitators to individually oriented HIV prevention and care services (Blankenship, Bray, & Merson, 2000; Farmer, 2004; Farmer, Leandre, et al., 2001; Gupta, Parkhurst, Ogden, Aggleton, & Mahal, 2008; Jones et al., 2005; Parker, Easton, & Klein, 2000; Sumartojo, Doll, Holtgrave, Gayle, & Merson, 2000).
However, few data have been systematically collected in Mozambique on the conditions that affect the lives of HIV-positive women and their children on a daily basis, and how these conditions affect their acceptance and utilization of HIV care services. We therefore conducted a qualitative study to determine the factors affecting women’s decision to seek HIV care and adhere to follow-up visits for themselves and their newborn babies.
Method
We conducted a cross-sectional qualitative study of a subset of women participating in an observational cohort study of nevirapine (NVP) resistance following prophylaxis with single-dose nevirapine, which started in June 2005 and ended in December 2008 (Micek et al., 2010). Briefly, the study enrolled mothers and newborn infants participating in PMTCT programs at three clinics in Beira, Mozambique. Infants were supposed to make five study visits through 8 weeks of age, at which time questionnaires were administered and blood samples taken for analysis of HIV infection and NVP resistance (Blankenship et al., 2000). Similar to the PMTCT program from which participants were recruited, study-related follow-up of infants was poor, with 57% (499/875) of enrolled infants missing >2 successive scheduled study visits. We investigated the reasons for LTFU in this already assembled cohort of mothers and infants, to provide insights into the reasons for LTFU within PMTCT programs.
Two techniques were used to systematically collect data: individual in-depth interviews (IDIs) with patients and clinic staff, and focus group discussions (FGDs) with patients. A purposive sampling strategy was used to select participants, stratified primarily by the quality of their study follow-up:
mother/infant pairs who participated in the NVP-resistance study and had good follow-up (missing less than two sequentially scheduled visits),
mother/infant pairs who participated in the NVP-resistance study and had poor follow-up (missing more than 2 successive scheduled visits),
mother/infant pairs who only attended the first study visit (early losses),
mother/infant pairs who refused participation in the NVP-resistance study but were registered at the HIV clinic,
mother/infant pairs whose infants were determined HIV-positive, and
clinic workers and study staff involved in the attendance/care of women and children
Interviews focused on exploring the main obstacles preventing women from attending study visits, as well as follow-up with HIV care. Interviews also sought to elicit factors that influence women’s decisions about newborn care, and identify barriers and facilitators of care and of initiating ART for eligible infants.
Preliminary analysis of the information obtained in the IDIs was followed by two FGDs: one including mother/infant pairs with good follow-up and the other including mother/infant pairs with poor follow-up. The goal of these FGDs was to generate debate on recurrent themes that emerged from IDIs.
Interview and FGD data were tape-recorded, and transcripts were coded and analyzed using ATLAS.ti. Independent informed consent was obtained from all study respondents. The study was approved by the institutional review boards from the Mozambique National Institute of Health (Maputo, Mozambique) and Seattle Children’s Hospital (Seattle, Washington, USA).
Results
Fifty-two IDIs were conducted, including 42 with mother/infant pairs, 6 with clinic staff, and 4 with study staff (Table 1). Two FGDs were performed: One included seven individuals with good follow-up and the other six individuals with poor follow-up. All infants of the mother/infant pairs participating in the FGDs were registered at an HIV clinic that provided care for HIV-exposed or infected infants.
Classification of Individuals Who Underwent In-Depth Interviews.
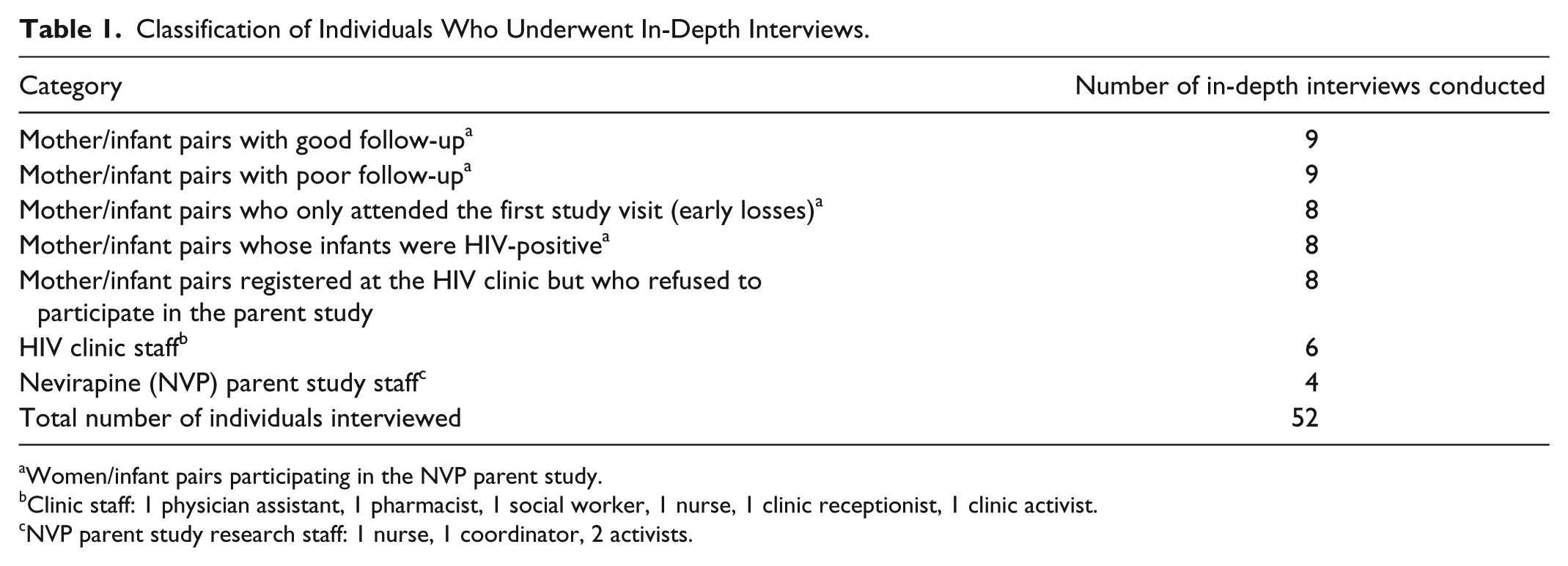
Women/infant pairs participating in the NVP parent study.
Clinic staff: 1 physician assistant, 1 pharmacist, 1 social worker, 1 nurse, 1 clinic receptionist, 1 clinic activist.
NVP parent study research staff: 1 nurse, 1 coordinator, 2 activists.
An array of factors identified by women and health staff were perceived as important barriers to follow-up study and clinic visits, and to the acceptability of services. Figure 1 lists all these factors and attempts to represent schematically the iterative and synergistic interactions among them.

Schematic diagram of iterative and synergistic barriers affecting compliance of women/infant pair follow-up in HIV care.
Among the factors identified by respondents, three major themes pertaining to women accessing health care repeatedly emerged, independent of the degree of follow-up: food insecurity, difficulties navigating a health system perceived as dysfunctional, and women’s familial roles and responsibilities. Further analysis of these three interrelated themes, including specific issues around each, is highlighted below.
Theme 1: Food Insecurity and the Trade-Offs in Women’s Daily Life
The struggle for daily survival
Issues related to food insecurity were common among all participants, and appeared to be inextricably linked to women’s choices for continuing HIV care and complying with follow-up visits. In particular, this issue represented the strongest and most prevailing barrier for all respondents who had poor adherence to follow-up visits. The struggle to get food is a daily constraint among the women interviewed, who often referred to feeling so weak and desperate for not having stable means of feeding themselves and their children—many of whom were also ill. The first excerpt in Figure 2 from the IDI of a woman taking ART illustrates this situation.
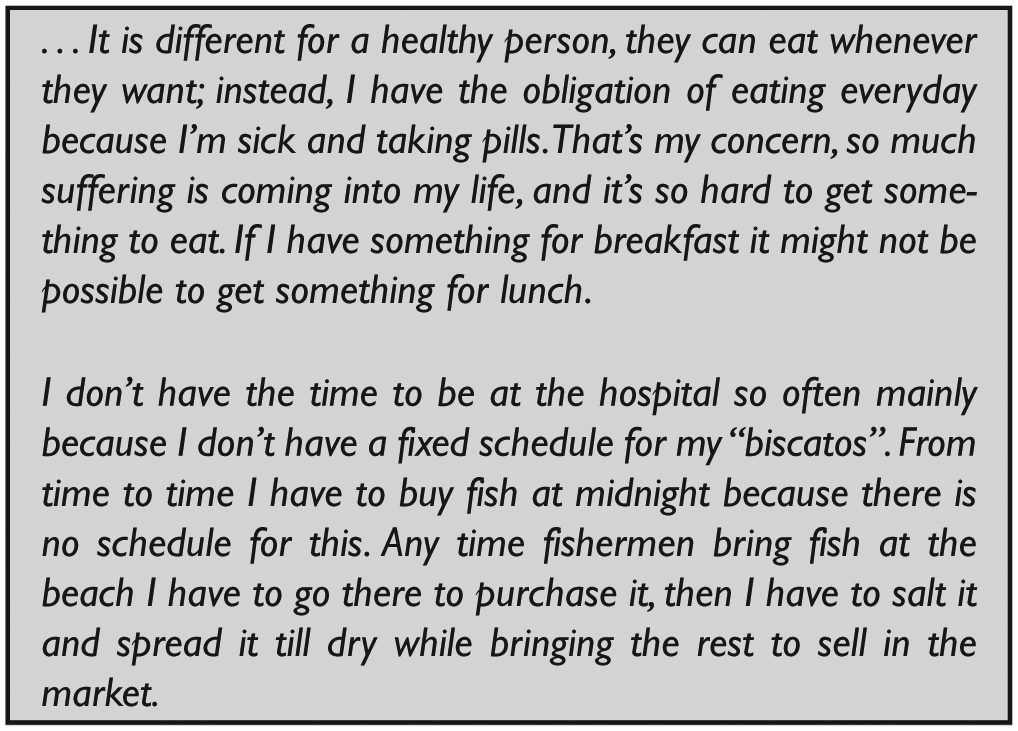
Women narrative related to food insecurity and the trade-off in women’s daily life.
Time spent going to the clinic versus time getting money to buy food
A common dilemma mentioned by women was whether to devote time to get food versus spend time going to the clinic. Women frequently have to help generate income for their families through informal businesses that are based on an unstable economy of subsistence. Common small businesses (biscatos) mentioned by women as a daily means of subsistence included the sale of charcoal processed by them from purchased firewood, the sale of sand gathered on the beach to be used to make concrete for construction (an activity punishable by city officials), the sale of purchased fish, the sale of nipa (a home-brewed alcoholic beverage), and the sale of produce from their farms (machambas) (Figure 2).
Seasonal work and other household responsibilities
Of the 42 interviewed women, 36 were engaged in some kind of agricultural activity, either for household consumption or for selling. Because Beira’s sandy soil is not fertile, many machambas are located far from the city. Taking care of their machambas is done regularly throughout the year, but the time devoted to this activity usually varies depending on the season and distance to the fields. Thus, because most women do not have money to afford public or other transportation, they are required to walk long journeys to get to their crops. The duration of visits to the machambas may range from 1 to 3 days per week.
Fetching water for their households was another mandatory daily activity requiring their time and resources. Most mothers expressed that their household tasks and subsistence activities did not leave time for any additional tasks. Thus, attending the clinic for care or a study was only possible if they sacrificed other responsibilities.
Food aid: a social conflict at clinics
Food insecurity has also become a social problem at health facilities as health workers need to restrict and prioritize beneficiaries of food aid. A recurrent barrier that emerged in several IDIs and FGDs was corruption in the distribution of food aid. Nearly all respondents, including clinic staff, expressed acknowledgment of episodes where nurses or other health staff manipulated recipients of food aid or received bribes to sell food originally intended for patients with HIV/AIDS. The narratives excerpted in Figure 3 illustrate how this issue permeates the dynamics of health facilities.

Conflicts generated by food aid distribution at health facilities.
Clinic and study staff questioned about corrupt practices acknowledged that graft is frequent and systematic. Marketing of items intended as aid is performed clandestinely but accepted as a common way to procure extra income for health staff households. Most of them felt that it was a consequence of meager salaries given to state employees.
Use of transportation subsidies for other household needs
Transportation subsidies were provided as part of the NVP-resistance study for women to attend follow-up study visits. However, women participating in this study who had poor follow-up frequently mentioned using the transportation money for other household needs, mainly food. As a consequence, the woman could not afford transportation to the subsequent study visit.
Theme 2: Difficulties Navigating a Dysfunctional Health System
Most interviewed women identified the rudeness of health care providers and the incomprehensible flow of care as barriers to attending follow-up visits at the HIV clinic. Women perceived the clinic staff to be overloaded, unmotivated, and poorly trained. Furthermore, staff members were frequently accused of lacking compassion in their interactions with patients. In the interviews, mothers described several examples of disrespectful treatment of patients, including verbal and nonverbal derogatory and discriminatory practices (Figure 4).

Barriers faced at the health system.
An erratic flow of services was described by women during interviews and FGDs. Women complained about having separate appointments for themselves and their babies at the pediatric and adult HIV clinics, with most of the appointments within only a few days of each other. They also told of going back and forth between different clinic rooms or wards (i.e., social worker, pharmacy, nurse who interprets CD4 results, multiple blood draws at labs, etc.). Many women claimed they had not had a consultation with a medical doctor since their registration at the HIV clinic. Many of those who had seen a doctor mentioned having several appointments canceled after waiting entire days for a doctor who never arrived or in other cases waiting for a late doctor who never offered an apology for the delay.
Most public health facilities in Mozambique, including all three clinics where this study took place, are extremely busy early in the morning but nearly empty in the afternoons (Figure 4).
Theme 3: Women’s Familial Roles and Household Responsibilities
Many women reported that illness, either in close relatives or themselves, prevented them from attending the HIV clinic. This issue was raised among all women whose babies were HIV infected, but also frequently by women whose babies were not infected (Figure 5).

Women’s familial roles and household responsibilities.
Despite the fact that women felt they were primarily in charge of their children’s health care, the decision to seek medical care was usually a family decision. Women were socially expected to consult their husbands, mothers-in-law, or other relatives before seeking care for themselves and their children. Nonetheless, when their children were sick, some women said that they had the primary responsibility of procuring money to bring the child to the clinic, bringing food to the child while hospitalized, or even paying for the treatment.
Women with an HIV-infected child who had not disclosed their own HIV infection status to their partners had difficulties justifying frequent visits to the health facility. Fear of domestic violence and stigma from their families and communities prevented them from utilizing HIV care services (Figure 5).
Many mothers reported that they sought care for their children from diverse health providers concurrently. Women believe traditional healing practices are important for their children’s health; however, most of them opted to attend public health facilities first because traditional healers and other informal health providers request higher payments than public health facilities.
Discussion
Our qualitative study explored the perceptions of HIV-infected postpartum women and their health care providers regarding the primary barriers to maternal and infant compliance with medical newborn care in Beira, Mozambique. Non-adherence to infants’ clinic visits appeared primarily due to (a) women’s full-time obligation to help gain food for the family, (b) unpleasant and ineffectual past experiences with the health care system, and (c) stigma related to HIV within family units. Our findings unveil the complex context in which HIV-infected women and their children live and function on a daily basis. Furthermore, our findings suggest that the structure and function of the HIV care system implemented by the state and supported by non-governmental organizations should be reviewed.
Although important programmatic goals related to HIV services have been attained in Sofala Province (80,000 people are registered in HIV care and 18,000 have started ART free of charge in more than 39 public health facilities at the time of this study; HAI, 2009), overall living conditions in central Mozambique remain extremely difficult for people living with HIV/AIDS (Kalofonos, 2008). Indeed, a significant body of literature has identified poverty as a main socioeconomic force behind the HIV epidemic (Farmer, 2004; Farmer, Connors, & Simmons, 1996; Kim & Millen, 2002; Parker et al., 2000; Singer, 1998). These reports highlight that other forms of social inequality, instability, and discrimination synergize with poverty to exacerbate the risk of HIV and vulnerability of those who become infected. Our findings regarding the health care system are in agreement with previous research done around the world, showing that structural factors interfere with effective care of HIV infection (Blankenship et al., 2000; Farmer, 2004; Farmer, Leandre, et al., 2001; Gupta et al., 2008; Parker et al., 2000; Sumartojo et al., 2000). Social analysts have increasingly called for an evaluation of the health care system and have advocated a shift of resources to focus intervention primarily on the economic, social, and environmental factors that are thought to underlie the HIV epidemic (Loforte, 2007; Parker et al., 2000).
In Mozambique, where cash income is increasingly important for survival, the informal economy has become vital for women, particularly in urban areas (Inge, Paulo, & Montserrat, 2008). The Mozambican women in our study were expected to accomplish multiple daily tasks that included procuring cash to cover their subsistence needs, providing child and family care, gathering water for daily consumption, and cooking. These tasks and responsibilities prevented them from attending to medical care for their infants at the frequency currently recommended by the HIV care system. Importantly, women’s responsibilities have been demonstrated to include a heavier workload and lower cash returns compared with men, with significant ramifications on their well-being and decision making regarding their and their child’s health care (Parker et al., 2000). As reported by our study participants, others have found that attending frequent clinical appointments jeopardizes household food security when women’s activities are diverted from food production (Kerr, 2005).
The link between poverty, food insecurity, and HIV risk may also be mediated through the need to travel for work. In our study, all women interviewed were settled in urban Beira. However, the seasonal tending of crops in the countryside and women’s daily journeys in the search for work and food were constraints consistently perceived as barriers to clinic visits. Similarly, in Malawi, mobility was a marker of increased risk and vulnerability for HIV-infected women (Bryceson & Fonseca, 2006).
Our study found that the poor quality of services provided by clinic staff affected women’s follow-up with care and that the ineffectual behaviors of health care workers may be rooted in their perceived poor living conditions. Structural adjustment policies imposed by the International Monetary Fund (IMF) have cut national budgets since the 1980s, which has kept health worker salaries at poverty levels, contributing to low morale and pressing health workers to search for more lucrative work in the private or informal sector (Gloyd et al., 2007).
Others agree that resource scarcity must be addressed, structural adjustment policies must be reversed, and overall expansion of public spending are required (Gloyd et al., 2007) to improve the working and living conditions and thus morale and behaviors of staff at health facilities. The implementation and success of culturally tailored health programs in Mozambique (Loforte, 2007) suggest that health services are weakened by health provider’s misunderstanding of their female clients. Anthropological research might facilitate educational strategies to remediate the attitudes and behaviors of health workers (Loforte, 2003, 2007) and lead to improved service utilization.
This study has several limitations. The nesting of our study within a prospective research cohort may limit the generalizability of our findings. The small sample size and purposeful sampling methodology may also limit our ability to generalize to the HIV population in Mozambique. Nonetheless, the voices and life circumstances of those who participated in our study were consistent with the findings of other studies, and provide valuable insights that allow us to better understand reasons for poor follow-up that may apply to women and children in similar contexts (Chapman, 2003, 2006; Farmer, Leandre, et al., 2001; Jones et al., 2005; Painter et al., 2004; Painter et al., 2005).
In conclusion, our study’s findings suggest that the mere provision of clinical HIV care services will not necessarily engage HIV/AIDS-affected women and children into medical care. Our observed LTFU of more than 50% of infants (Blankenship et al., 2000) appeared to be associated with mothers’ daily struggles related to poverty and food insecurity, which prevented their use of available services. Our study suggests that integration of mother and child medical consultations, and more efficient and culturally sensitive medical services may improve follow-up. And finally, our study indicates that economic empowerment of women is crucial to achieving better compliance with medical care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.