
Abstract
Stigma attached to HIV/AIDS remains a global problem, with severe negative consequences for people living with HIV (PLHIV). Family support is fundamental for PLHIV’s psychological and physical well-being. HIV-related stigma is high in Turkey, where HIV/AIDS prevalence is low and the epidemic is not considered a priority. Based on qualitative data generated with HIV-positive women and men, this article explores the process of stigmatization, as experienced and perceived by PLHIV in Turkey, focusing on the institution of the family. Results indicated that enacted stigma from family members is lower than anticipated. While most participants’ narratives showed patterns of support rather than rejection from families, the strong expectations around the cultural value attributed to “the family” are found to be the main facilitators of internalized stigma. The article critically discusses the meaning and implications of family support, addressing the role of patriarchal values attributed to womanhood, manhood, and sexuality in Turkey.
Introduction
Stigma attached to HIV/AIDS is still a global problem, despite the achievements in the global response to the epidemic and the expectations that universal access to antiretroviral therapy (ART) will reduce stigma (Castro & Farmer, 2005; The Joint United Nations Programme on HIV/AIDS [UNAIDS], 2013). For people living with HIV (PLHIV), stigma has important negative consequences, such as physical and social isolation, violence, loss of livelihood and housing, differential treatment in educational and health institutions, limitation of travel opportunities, limitation of the sexual life, disruption of social identity, and loss of agency (Department for International Development [DFID], 2007; Mahajan et al., 2008; Nachega et al., 2012; Ogden & Nyblade, 2005; Reis, Galvao, & Gir, 2013; UNAIDS, 2009). Stigma also provides ground for the spread of the epidemic, by limiting the impact of interventions and deterring people from being tested, seeking help, and adhering to treatment (Adam, 1992; de Bruyn, 2002; Derksen & Muula, 2014; Goudge, Ngoma, Manderson, & Schneider, 2009; Mall, Middelkoop, Mark, Wood, & Bekker, 2013; Misir, 2013; van Brakel, 2006).
Drawing on 12 months’ fieldwork, this article explores the process of stigmatization as experienced and perceived by PLHIV in Turkey, with a specific focus on the institution of the family. The main purpose is to understand the processes in which PLHIV attribute meaning to living with HIV and its stigma in relation with the “family” as an institution. Through the investigation of PLHIV’s encounters with stigma, both in felt and enacted forms, the article addresses the role of patriarchal discourse seen in PLHIV’s experiences in the institution of family.
In Turkey, official figures show low rates of HIV/AIDS incidence and prevalence. However, Turkey belongs to a region (Eastern Europe and Central Asia) where new HIV infections continue rising despite the global decline (UNAIDS, 2013). As of 2014, there are 9,379 people diagnosed with HIV or AIDS in Turkey (Ministry of Health [MoH] of Turkey, 2015). These figures are considered to be underestimates, because of the low level of HIV testing and the inadequacy of surveillance and registration systems (Ay & Karabey, 2006; Tümer, 2009). The main route of transmission is heterosexual intercourse, followed by homosexual intercourse. The majority of PLHIV are diagnosed during pre-surgical and blood donation tests (Bal, 2009; Özlü, 2012). Treatment is free of charge as long as the patient is registered with the social security system. Educational campaigns, activism, advocacy, and research on HIV/AIDS have started rather late, mainly after 2003, with the support of international funds (Çokar, 2008; Kaplan, 2008). HIV/AIDS is not considered as a priority issue within health policies nor among the general public.
The stigma attached to HIV/AIDS is powerful and widespread in Turkey. HIV/AIDS is associated with socially disapproved forms of sexuality and is considered as a consequence of the integration of “foreign” and “immoral” elements into Turkish society. Available studies, mostly surveys, have demonstrated the low levels of knowledge and negative attitudes toward PLHIV among various populations such as health workers (Duyan, Agalar, & Sayek, 2001; Okan & İrgil, 1993; Ünsal, 1999), medical school students (Ekuklu, Tuğrul, Gül, Eskiocak, & Saltık, 2004; Oğuzkaya & Güleser, 2006), and university/college students (Çok, Gray, & Ersever, 2001; Mağden, Şahin, Metin, & Akkaya, 2003).
Very little research has been done with the aim of understanding the experiences and perceptions of PLHIV in Turkey. Few available surveys show that human rights of PLHIV are being violated mostly in health care settings and workplaces (Pozitif Yaşam Derneği, 2007, 2008, 2009). Although PLHIV experience stigmatization most frequently in health care settings, the most significant role in the formation of internalized and felt stigma is played by the institution of the family, as discussed in this article. The article argues that although family support is considerably high in Turkey, family-related social expectations and desires are the main drivers of internalized and felt stigma, because the effects of HIV are expressed in terms of perceived success or failure to fulfill family-related social roles. The article critically discusses the meaning of family support toward PLHIV, referring to the role of patriarchal values attributed to womanhood, manhood, and sexuality in the cultural setting of Turkey.
Conceptual Framework
In his classical work, Goffman (1963) defines stigma as “an attribute that is deeply discrediting” and that “constitutes a special discrepancy between ‘virtual’ and ‘actual’ social identity” (pp. 2-3) of an individual. Although there have been growth and advancement in the conceptualization and methodology of stigma research in the last few decades, the stigma concept has been criticized from many angles, mainly by being too individually focused (Hatzenbuehler & Link, 2014). This study follows Link and Phelan’s (2001) conceptualization, which has been developed to address this criticism. According to them, stigma is a “social process that exists when elements of labelling, stereotyping, separation, status loss, and discrimination occur in a power situation” that allows them. In line with this emphasis on power relations, stigma researchers, especially in the area of health-related stigma, have recently focused on the role of “structural,” that is, broader, macro-social dimensions of stigma (Hatzenbuehler & Link, 2014, p. 1).
The term “structural discrimination” is particularly important for an understanding of stigmatization as a production of social inequalities of class, race, gender, and sexuality and as reproducing and legitimizing the existing power relations (Castro & Farmer, 2005; Parker & Aggleton, 2003). In a similar way, Reidpath and Chan (2005) state that the stigma of HIV is “layered with other stigmas, such as those associated with the routes of transmission (e.g., sex work and injecting drug use) and personal characteristics (e.g., race, religion, ethnicity and gender).”
Scambler and Hopkins (1986) distinguished between “felt” and “enacted” stigma. While the former refers to the “instances of discrimination” on the grounds of the “perceived unacceptability or inferiority” due to a health condition, the latter is the fear of enacted stigma, the fear of being discriminated which “also encompasses a feeling of shame associated with” the illness (Scambler & Hopkins, 1986, p. 33). Even if the stigmatized persons do not experience enacted stigma in the form of direct discrimination, they still can “internalize” negative representations of their stigmatized status (Goffman, 1963). “Internalized stigma” often causes loss of confidence and self-esteem (Campbell & Deacon, 2006). Therefore, not only enacted stigma but also felt and internalized forms of stigma are important for a better understanding of PLHIV’s experiences.
When we look at the interrelated determinants of HIV-related stigma, first, we see that HIV/AIDS is associated with behaviors that are already stigmatized or considered “deviant,” such as homosexuality, injection drug use, and sex work. Second, PLHIV are thought to be “responsible” for being infected with HIV. In addition, HIV/AIDS is considered as a life-threatening disease; thus, people are afraid of acquiring HIV. Finally, religious and/or moral beliefs lead people to conclude that having HIV is the result of a moral fault, such as promiscuous or deviant sex, that deserves punishment (de Bruyn, 1998).
There are also individual and socioeconomic factors affecting stigmatizing attitudes toward PLHIV. For example, lower levels of stigmatizing attitudes are documented in younger individuals, in persons having personal contact with someone living with HIV and having “more favourable attitudes” toward homosexuals (Herek, 1999). The role of socioeconomic factors, mainly education, class, and rural–urban residency, at individual and/or community levels has also been discussed in the literature as determinants of stigmatizing attitudes. Lower educational and income levels are found to be related with higher levels of discrimination against PLHIV, while varying across settings, cultures, and forms of stigma (Aggleton, Yankah, & Crewe, 2011; Amuri, Mitchell, Cockcroft, & Andersson, 2001; de Araujo, 2008; Lim et al., 2013; Nyblade et al., 2003).
Stigmatizing attitudes among the communities and also among health care providers around the globe (see, for example, Abdelrahman et al., 2015; Mukolo, Torres, Bechtel, Sidat, & Vergara, 2013; Persson et al., 2014) indicate that anti-stigma campaigns and initiatives are still not yet effective, partially due to inadequate conceptual and methodological tools (Misir, 2013) and because of certain social, cultural, and economic contexts (Reis et al., 2013) that act as barriers against access to prevention, test, treatment, care, and support services.
With regard to the gendered aspect of stigmatization, it is documented that women, especially adolescent and young women, are disproportionately affected by the epidemic (World Health Organization [WHO], 2003; UNAIDS, 2013). Women are often blamed for bringing disease and shame to the family, and are abandoned, isolated, denied accommodation, and subjected to violence (Ertürk 2005; Reis et al., 2013; Udobong, Udonwa, Charles, Adat, & Udonwa, 2015). Violence against women, patriarchal norms about motherhood, division of labor in the household, patrilineal systems of inheritance, and early and forced marriages are among important factors increasing women’s susceptibility to HIV/AIDS and disproportionately affecting HIV-positive women (Barnes & Murphy, 2009; Ertürk, 2015; Russell & Seeley, 2010). Homosexual and transgender individuals are also disproportionately affected, in terms of both vulnerability to and experiences of living with HIV. As a set of cultural ideologies, including beliefs about gender, morality, and danger, heterosexism perpetuate HIV-related stigma against sexual minorities and creates barriers against their access to health care (Herek, 2004; Seidman, 1988; UNAIDS, 2013).
The concept of patriarchy provides a suitable basis for discussing the above-mentioned gendered aspects of HIV-related stigma, especially in relation with PLHIV’s experiences within the family. As “a form of social organization in which cultural and institutional beliefs and patterns accept, support, and reproduce the domination of women and younger men by older or more powerful men” (Levy, 2007), patriarchy has a distinct form in which the “operations of the patrilocally extended household” gives the senior man authority over everyone else (Kandiyoti, 1988, pp. 275-278). Therefore, family is accepted to be the fundamental institution of patriarchy (Demir, 1997).
The institution of family in relation to HIV/AIDS has been studied in various ways, such as by focusing on the patterns of disclosure of HIV status to family members, sexual behavior among partners, emotional relationships in sero-discordant couples (in which one partner is infected by HIV and the other is not) caregiving to PLHIV by spouses or parents, and courtesy stigma (perceived or experienced stigma due to the person’s association with a stigmatized individual) experienced by family members (see, for example, Bonuck, 1993; Folasire, Akinyemi, & Owoaje, 2014; Liu, Xu, Sun, & Dümenci, 2014; Patel et al., 2013; Persson, 2008; Rispel, Cloete, Metcalf, Moody, & Caswell, 2012; Skurnick, Abrams, Kennedy, Valentine, & Cordell, 1998; Wouters, van Loon, van Rensburg, & Meulemans, 2009). While research on PLHIV and their families from different backgrounds and cultures has resulted in different conclusions about the levels and forms of stigma experienced in the family, the common finding is that the support of family members, particularly spouses and parents, is fundamental in living with HIV, especially in medication adherence and coping strategies (Camargo, Capitao, & Filipe, 2014; Folasire et al., 2014; Harris, 2014; Stumbo, Wrubel, & Johnson, 2011; Udobong et al., 2015; Ushie & Jegede, 2012; Wouters et al., 2009). Family support has also been considered as a relatively unexplored but promising resource for gay and lesbian youth (LaSala, 2015). As Li et al. (2006) state, the importance of family in living with HIV is expected to be higher, but remains relatively under-researched, in family-oriented societies.
Based on the above presented literature and conceptualizations around HIV-related stigma and family support, the conceptual framework that guides this article can be summarized as following: In line with the criticism toward individualistic approaches to stigma and following Link and Phelan’s (2001) conceptualization that emphasizes “power” relations in which stigma occurs, this research is concerned with both micro (intrapersonal and interpersonal, such as internalized stigma and enacted stigma) and macro (“structural” or discursive) forms and levels of stigmatization. Among the many intersecting lines of social inequalities at the structural level (such as race, class, economic status), the main line this research is focused on is gender inequalities. This is discussed with reference to the patriarchal values intrinsic to the institution of the family. Thus, the interaction between family members is approached from a critical point of view, looking at the gendered power relations beyond family acceptance/support patterns. Seeing the institution of the family—including the culturally attributed norms and values to that institution—as both a potential source of support and a source of internalized stigma, micro and macro-social processes are linked.
Method
This article is based on a qualitative and interpretive research, conducted through a year of fieldwork in 2010 and 2011. Biographical narrative interviews were conducted with 24 PLHIV and semi-structured interviews with 32 key informants (KI), including doctors, people working in the MoH, Turkey offices of international bodies, non-governmental organizations (NGO) working on sexual and reproductive health, human rights, and lesbian, gay, bisexual, transgender (LGBT) rights. Informal conversations and daily interactions with other PLHIV, as logged in the field diary, provided additional primary data.
The questions that are addressed in this article are as follows: “In what forms and contexts do PLHIV experience stigma in their parental and formed families?” “What are the factors that differentiate their experiences?” “How are the meanings attributed by PLHIV to HIV/AIDS constructed in the institution of the family?” and “How is internalized stigma formed by and/or affecting experiences in family?”
Participants
The primary participants were women and men living with HIV. The sampling procedure was purposive, based on an intersectional approach, which states that the experience of stigma differs according to the individuals’ multiple social locations. Based on the assumption that the effects of the HIV-positive status on the stigmatization of the already stigmatized identities are different, having “an already stigmatized identity” was considered as one axis of difference in the sample design. Involvement in sex work and sexual minority status have been considered as sources of stigmatized identity prior to HIV. This group of participants was called the “Sample Group A.” The second, “Sample Group B,” consisted of an approximately the same number of individuals who did not belong to any of the categories mentioned above. In total, 24 PLHIV, as demonstrated in Table 1, have been reached.
Purposive Sampling Based on An Intersectional Approach.

Main characteristics of the participants are provided in Table 2, in descending order of frequency.
Characteristics of the Participants.
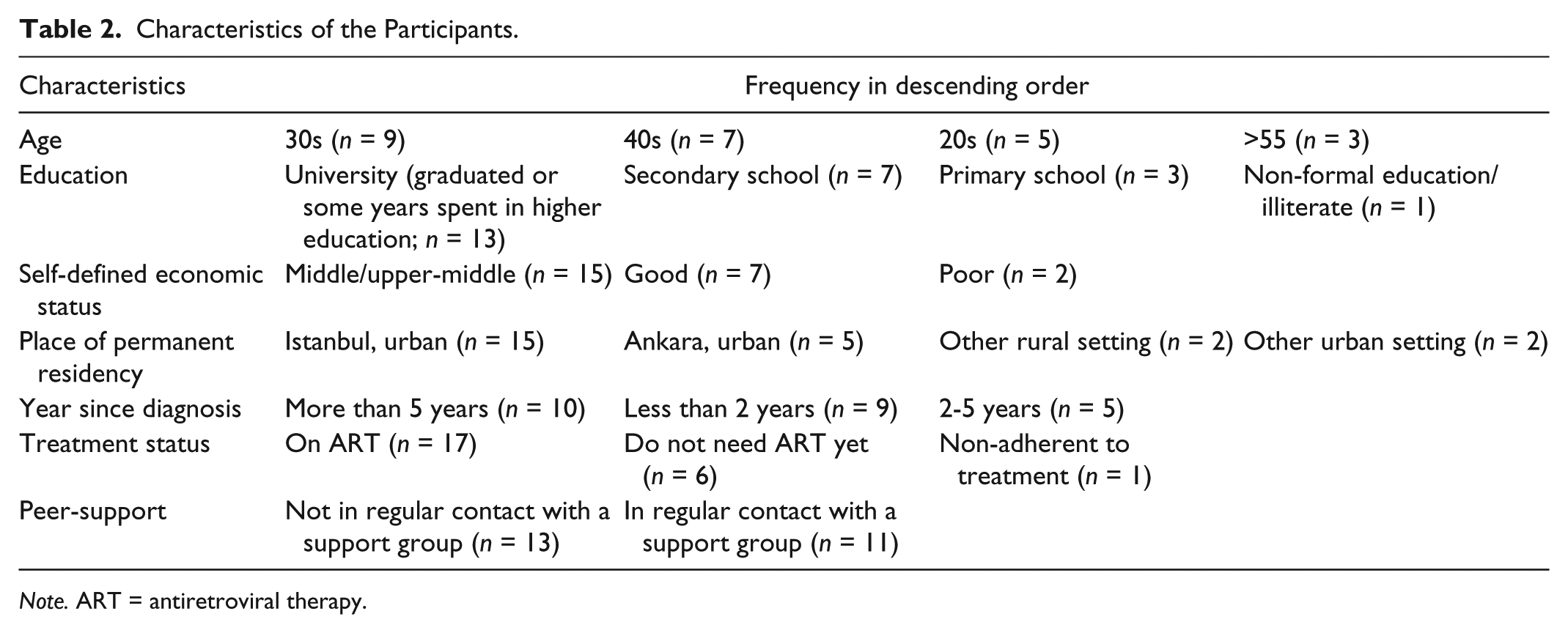
Note. ART = antiretroviral therapy.
Ethical Considerations
Ethical considerations are at paramount importance in this research, considering the high stigma and the limited number of individual and institutional actors related to HIV/AIDS in the research setting. Utmost care for prevention of disclosure risks has been taken. Confidentiality and anonymity of all research participants have been managed through strict adherence to the procedures of safe data storage and anonymity. Participation to the research was voluntary and based on informed consent. Ethical approval has been granted by the University of East Anglia, International Development Ethics Committee on December 24, 2009. 1 Only the sex and age group of the participants are used in this article when quoting from the transcripts, to protect anonymity and confidentiality.
Data Generation
The research was conducted in two urban settings, Ankara and Istanbul, which are the two cities on top of the list of the reported HIV/AIDS cases in Turkey. Most of the participants (n = 17) were reached through an NGO that offers support to PLHIV. Others were reached through the author’s personal contact (n = 5) and through infection clinics (n = 2).
Instead of focusing solely on illness narratives, the interviews were aimed at generating the entire life story of each participant, with a view to gain a deep understanding of the lives and identities of PLHIV. The interview method took insights from the framework of Biographic–Narrative–Interpretive Method (BNIM; Wengraf, 2006), initiated with a single question aimed at generating an “uninterrupted,” “free-form” of narrative (Wengraf, 2009) and, therefore, considered useful to elicit research participants’ self-defined perspectives on their lives and identities.
The first sub-session of the interviews began with asking a “single question aimed at inducing narrative.” After listening to the “whole story” without any interruption until the respondent explicitly expressed that they have finished, the second sub-session started, after a short break. In the second sub-session, questions were asked to the participants, based on the notes taken by the author during the first sub-session, using a particular “formula,” without changing the exact words used by the respondent (Wengraf, 2009). The average time of an interview was 2 hr (minimum 45 min, maximum 4½ hr). Interviews were tape-recorded with the consent of the participants and were transcribed verbatim.
Data Analysis
A combination of thematic and narrative analysis techniques was used for data analysis. The thematic analysis was composed of three steps, namely, data expansion, data reduction, and data display. These steps are summarized below, based on Grbich (1999), Mason (2002), Richards (2006), and Holliday (2007).
First, the transcripts and related notes from the fieldwork were read and a brief summary narrative for each participant was written. Doing this, particular passages that are found interesting in terms of the research questions or in terms of raising a different question were identified. In the second step, data reduction, “topic nodes” and “analytical nodes” were generated using a data management software. The topic nodes were created based on the research questions, the theoretical framework and other themes emerged from the transcripts. The analytical nodes were created to link the emerging themes under each topic to their meanings and relevancies to the conceptual framework. Finally, regularities, similarities, variations, and singularities in passages were coded under a category, and possible correlations between the topic codes and analytical codes were identified.
Despite variations in the method of narrative analysis (Riessman, 2000), a common approach is to identify ordering and sequencing in the narrative, to pay attention to the “telling” of the story (Grbich, 2007; Riessman, 2000). Accordingly, all narratives were analyzed not only by looking at the expressed experiences, events, and feelings but also focusing on the ways in which they were expressed. The main steps taken to understand the telling of the story (Grbich, 2007), in each of the particular topics identified through the above explained procedure, were as follows: (a) identification of the boundaries of the narrative segments in the transcript, (b) identification of the ways of expression (e.g., comparison, argumentation, etc.), (c) identification of the content (what feelings, emotions, and ideas are displayed with this particular way of expression) and context (the background information) of the story, (d) comparison among participants’ ways of telling the stories that are grouped under the same topic.
Results
Most participants’ narratives showed patterns of support rather than rejection from families, as explained below in detail. Although stigmatization in the family appeared to be less than anticipated, family-related social expectations and desires are found to be the main drivers of internalized and felt stigma for PLHIV. The effects of HIV were expressed in terms of perceived success or failure to fulfill family-related social roles. Results suggested that this is related with the fundamental role of family in Turkey in the construction of individuals’ social identities, within the framework of social control. Consequently, the narratives of the participants revealed that while PLHIV experience stigmatization most frequently in health care settings, stigmatization in relation to the family was perceived as most important. In addition, results indicated that support received by family members could be understood and problematized in relation with patriarchal values, as will be exemplified below.
To begin, a brief look at the participants’ family situations is necessary. With the purpose of securing utmost protection of the anonymity of the participants, their family situations are not presented here in a case-based or cross-table format, but instead explained briefly as below.
Participants’ Family Situations
Among women (n = 9), including male-to-female (MTF) transsexual participants, three were married and six were single. Among married women, two had HIV-positive husbands. Among six women who were single, three were never married, one had lost her husband to AIDS, and two were divorced. One of the divorced women was MTF transsexual who was married to a woman and had fathered children before her transition. Among unmarried women, two were in a long-term relationship with HIV-negative partners. One MTF transsexual was also in a long-term relationship. In total, five women had become infected through their husbands during their marriage. Four had children. None of the children were HIV-positive.
Among heterosexual men (n = 7), four were married and three were never married. All four of the former had been diagnosed with HIV since marrying their present wives; only one had an HIV-positive wife. Among homosexual men (n = 8), three were divorced from their wives (two had children), one had been engaged to a woman, and three were in long-term relationships with HIV-positive partners and had been diagnosed with HIV while in this relationship.
None of the single participants who were in a relationship with intimate partners (n = 6, including two women, three homosexual men, and one transsexual participant) were cohabiting, reflecting the general social norm in the country. It is more desirable and acceptable for both men and women to live with their parents than with a partner outside marriage, regardless of age. Accordingly, the concept of “family” in the participants’ narratives did not include intimate partners.
The household structures of the participants are presented in Table 3. Eleven participants, most aged above 30, were living with their own or their spouse’s parents. Participants who lived with their parent(s) and another family member included single people, divorced women, and men with children. Three women who were married or widowed were living with the parents or another family member of the husband. These sample characteristics of relationships with parents point to one of the unique cultural features of Turkey.
Household Structures of the Participants.

Experiences of Stigmatization in the Family
Family support experienced in both parental and formed families are explained below and discussed with regard to its positive outcomes and problematic aspects.
Parental family
Among 24 participants, six had not disclosed their HIV status to their parents; most of these had elderly parents who lived elsewhere. Among people who lived with parents (n = 11), only one concealed his or her status and another had disclosed it to his or her mother only. All but three participants whose HIV status was known to their parents generally described their parents as supportive. Of the others, two had already negative, violent relationships with their parents prior to their diagnosis, due to their nonconformity to expected gender norms, and one did not offer clear examples of and motives behind their parents’ non-supportive attitudes.
Some of the participants’ narratives described isolating themselves from their families because of the strong fear of rejection, but then being surprised by their parents/siblings’ support and realizing that “this wasn’t something to be so frightened of.” Many described their mothers and/or fathers as supportive or even closer and/or more understanding than before the diagnosis. In some cases, their relationships with their parents improved after being diagnosed with HIV because the parents became less authoritative or more indulgent, mostly because of their fear of losing their child. “To look on the bright side,” these participants said, they got closer with their parents: One day, I was sitting alone in my room, locked myself in my room when my father called me, he said “come down here let’s eat some fruits and have some chat.” As soon as I went [to the living room] I threw myself into his arms and for the first time [after being diagnosed] I cried sobbing, for hours. . . My father cried too. My mother started to cry too. Three of us cried. That day, what my father said was so nice. Uhm, “I am X years old but I’m very sound and very healthy and I’m still working and we have money. I will send you anywhere you want and I will absolutely get this thing treated. Nothing will happen to you,” he said and hugged me. That was one of the most beautiful memories of my life. (Man, in his 20s)
However, few participants perceived the closer attention from parents as a problem. This is because, parents’ perception of their child as sick, vulnerable, and in need of help can lead to a protective reaction. For example, a 40-year-old male participant explained that he needed to live far away from his mother and aunts “because they remind me of my disease all the time . . . it makes me live, like, face-to-face with the disease.”
When we look closer to parents’ attitudes toward their HIV-positive male children, sexual orientation of the child is seen as a determinative factor. The fathers’ acceptance of their heterosexual adult child was related to their acceptance (or even affirmation) of pre-marital sex for men as a sign of “healthy manhood.” In this case, being infected by HIV is seen as a consequence of “wrong” behavior in terms of not practicing safe sex. It is not the nature of the sexual relationship but the negligence in taking the risk that is questioned, and this does not become a moral basis for judgment.
However, in the case of homosexual men whose sexual identity is known by their families, the “HIV virus could not get ahead of homosexuality, could not be seen as an illness,” as a 40-year-old homosexual male participant explained, The only thing they [my family members] ever know, “oh! AIDS, oh, it’s a homosexual disease.” [They] are not interested in the illness part, they’re interested in homosexuality. I mean, . . . it is still being discussed in this country about whether or not homosexuality is a disease; whereas, on the other hand, there is HIV, which is an illness, and it’s not discussed at all. (Man, in his 40s)
Formed family
Both married men and married women were “accepted” and/or “supported” by their spouses. No HIV-positive women were blamed by their husbands or their husbands’ families and expelled from their homes. In the narratives of heterosexual men, the most important people mentioned as a source of support was their wives, whereas single heterosexual men only mentioned their parents as a primary source of support. For homosexual men, however, the primary source of support was their partner or friends.
Although spouses’ acceptance of their HIV-positive partners function as a source of support, it is seen that the reasons behind this acceptance are closely related with patriarchal norms attributed to womanhood and manhood in the society. Women’s “forgiveness” or “toleration” of their HIV-positive husbands, despite the fact that their husbands acquired HIV through sexual contact with another women, can be seen as related to the acceptance of patriarchal norms. These women support their husbands for different reasons, such as accepting men’s extramarital relationships as “normal,” holding valued social identity as a caring wife, or sustaining economic status. Yet, in some cases, where the source of the HIV is “unknown” or thought to be “something else,” families’ support and acceptance are based on trust.
Women participants of the research who were infected by their husbands during their marriage were not rejected by their parents or their new partners. Being infected within the institution of marriage “protected” them from being labeled as “immoral.” As will be discussed later in detail, an activist woman participating the study stated that this argument is questionable, as it reproduces the patriarchal norms ascribed to women: . . . if it’s a woman, especially a woman who appears to conform to societal norms, then instead of discrimination, people immediately say “what a pity for her!” . . . If it’s a man . . . this is more certain that we put many labels on him, without knowing anything about him. [But if it’s a woman:] “Oh but it’s such a pity.” . . . And obviously, this is also discriminatory, in a strange way. (KI1)
Lack of knowledge and ignorance about HIV/AIDS was interestingly expressed by some of the women participants as a reason behind families’ acceptance of HIV-positive women without reservation. For example a woman, whose husband and his family were illiterate, from a low socioeconomic background and from an “underdeveloped” region of Turkey, said, I got the diagnosis and my spouse took it as. . . I don’t know maybe out of ignorance but he said “Allah verdi” (it is from/by God) and he didn’t leave [me]. I mean if it was somebody else he would’ve left right away but he didn’t, he said “if God gave this” he said “we’ll put up with it, together,” he said. (Woman, in her 30s)
However, her husband and his family did know that HIV is contagious and that her status had to be kept a secret. Even if her husband’s family only “feared from her disease,” her own family had rejected her, not only for fear of being infected but also because of the moral stigma she brings to the family name.
We have a falling out [with my brother]; he doesn’t want me, because of all these affairs of mine (leaving home, being raped by strangers, married twice). In a way I acknowledge him to be right; but in a way I don’t. At the end of the day, he’s a man. He feels it beneath him [to take me back home or to help]. (Woman, in her 30s)
Attribution of Meaning to HIV and the Construction of Internalized Stigma Within the Family
As mentioned above, although enacted stigma in the family was less than anticipated, the institution of family has found to be the main source of internalized and felt stigma for PLHIV. The reason behind this is addressed in this section.
It is seen that family is the main reference point for self-evaluation to locate oneself in the broader society. Many participants’ freely formed life stories began with a statement about the kind of a family they were born into or had formed. Family-related social expectations and desires were recurrent themes throughout all the narratives, regardless of whether or not the issue under discussion was related to HIV. These expectations were not only evident in the stories told but were also articulated with great emphasis and was expressed as “fact” by all the participants from either an affirmative or a critical point of view. A 30-years-old homosexual man summarized a typical life plan tailored for middle-class men: At the end of the day, you are the only son of a household (bir evin bir oğlu
2
). This is what you have been taught: You will study, get your university degree, do your military service, establish your job, get married, have children, after getting children work forever to provide your children with a high quality of life, put [their] life in order, arrange the marriage for them, have grandchildren and die. I mean this is what has been taught to a person, to us, in Turkey, the plan from the very moment when we were born until the moment we die. . . . If anything apart from that plan or any delays in between [the planned steps] occur . . . then you will have to face oppression from peers and from society. Both you and your family. (Man, in his 30s)
Participants who described their families as educated, literate, or “modern” also stated that in spite of this, traditional values were maintained and preserved by their families. Others stated that however individually minded or strong they thought they were, it was very difficult to resist following the course of events within this life plan. The “turning points”, before being diagnosed with HIV, in the lives of many participants manifested themselves as the changes that occurred as a result of ruptures or delays in this life plan.
Overall, participants’ narratives exemplified situations where the family comes into play in the construction of identity, regardless of HIV status. Considering that the research context is a relatively less individualistic society, it is not surprising that family was a predominant theme in the participants’ narratives. However, the fundamental role of the family in framing perceptions and experiences of HIV-related stigma becomes evident when we consider the link between the stigma and the construction of self. An individual’s self-definition is central to their perception and management of stigma, thus, in the incorporation of the stigmatized identity into self (Link & Phelan, 2001). Stigmatization is about a “discrepancy between the ‘virtual’ and ‘actual’ social identities” of an individual (Goffman, 1963). In the perception of this discrepancy and its outcomes, comparison of the self with in- and out-groups is important (Crocker, Major, & Steele, 1998). Family was the main point of reference in the research participants’ narratives, in their self-evaluation in general and when comparing themselves with others and giving meaning to living with HIV in particular.
In this sense, HIV was perceived as a major obstacle to fulfilling family-related expectations, which were seen as normal and desirable social functions, such as getting married, having children, and earning money to maintain the family. Being diagnosed with HIV breaks the socially expected life trajectory designed around the concept of family.
This is why, while discrimination in the workplace and health institutions is more frequently mentioned in previous research (Öktem, 2014b; Pozitif Yaşam Derneği, 2007, 2008, 2009, 2010; Stigma Index Turkey [SIT], 2011), family rejection or acceptance remains the most important factor affecting PLHIV’s self-management. According to a participant who also worked as a peer counselor, the reactions of family are more important than those of any others and can literally be a matter of life or death: It hurts you much more; it hurts you enormously. I mean, someone whom I know for three days (expression meaning for a relatively short time) can discriminate against me, but so what? It won’t affect me. . . . But if your mother excludes you . . . this is your mother! It’s an indispensable part of yours. So, “my mother doesn’t love me; doesn’t want me; it is already a bad illness; I deserved it; it’s the curse of Allah and my family doesn’t want me.” That’s how you go get sucked in to a whirlpool. And after that. I saw people who expedited their own death. I saw families facilitating death. (Woman, in her 30s)
Comparing their problems caused by HIV and those caused by family-related issues in their lives, some respondents stated that “HIV and so forth” are “trifles” or “just trivial” compared with current familial problems and that they can “laugh away other things” such as discriminatory attitudes in health institutions.
The main ways in which family-related expectations and desires contributed to internalized stigma are discussed below, based on the examples most frequently seen in participants’ narratives.
The feeling of “guilt” and responsibility to family members
Some heterosexual men stated that they saw their HIV-positive status as a punishment that they must accept. Whether the sexual relationship was extramarital or not, their feeling of guilt and responsibility was related to “disappointing” or “betraying” their family. This is either about the perceived possibility of failure to fulfill family-related duties and functions or about putting their loved ones, including their children, at risk. For married men, the fact that their wives were HIV-negative was expressed as a major source of relief amid all the negative feelings that came with HIV. Apart from one person who believed that he had not been infected through sexual contact, they all expressed the feeling of guilt for putting their families in danger. These men did not show patterns of non-acceptance such as self-isolation, high distress, or non-adherence to their treatment, probably because of the support they received from their wives.
Not only men, but also one widowed woman talked about her feeling of self-blame, even though she did not consider herself responsible: . . . Unavoidably, you blame yourself. I mean, if something happens to [your children], it would be because of me. You yourself are living in this situation because of someone else [the husband], but still . . . your thinking is focused only and solely on your child. (Woman, in her 30s)
Another example of the feeling of guilt in relation to family, to abandon one’s family member after diagnosis, is expressed in the below quote: My mother, me and [my child] were living together, my mother is old, she’s got hypertension, she’s a person who takes medicines all the time. . . . Thinking that it might affect the order of my life and that two people at home who deal with illnesses might negatively effect a growing child, her/his education, I sent [my child] to her/his mother’s, on the very same day [I learned my HIV status]. Now I look back and think that I made a very wrong decision. (Man, divorced, homosexual participant, in his 40s)
The felt responsibility to family members also affects disclosure behavior to a great extent. The participants who had not disclosed their HIV status to all their family members explained that the reason they have not done so is not necessarily the fear of stigmatization. Especially people whose parents were elderly stated that they did not want their families to worry about them. For younger participants, the main motive behind the concealment of their status was to protect their families from gossip and rumor. Two women participants with HIV-negative teenage children explained that their most important motivation for hiding their positive status from their children was to avoid being asked, “Who did this to you?” They both stated that they did not want their children to feel hostility toward their fathers.
Single heterosexual HIV-positive men’s attitudes toward marriage
Heterosexual single men who participated in this research (n = 4) were most concerned about not being able to get married and with not being able to complete their military service, which is compulsory for men in Turkey and is generally seen as a condition for marriage. As a form of self-isolation, they had ended their romantic and/or sexual relationships, and given up their plans to get married and to have a family.
The problem of not being able to marry is discussed around questions about whether it is possible to practice safe sex and have a healthy and happy marriage, and whether it is possible to find a non-prejudiced partner. A young heterosexual participant whose long-term girlfriend left him after he disclosed his HIV status a few months after our interview, explained how he and his family had arranged a “required marriage”: There was this girl, who my mother really wanted, okay? . . . At first, she fixed her up with me, by “fixed her up” I mean she wanted her to become ours (to be married into our family). I never spoke to that girl . . . [my mother saw this girl in a women’s gathering and thought:] she’s very white and pure (chaste). And, I was of course very sad that I cannot be able to get married, I was so so sad and my mother didn’t want to miss that girl and she was seeing that I was healthy, so she was thinking that I was normal, I mean . . . “what if . . . what if you’re not [sick]” she kept saying, “while there is life there is hope, with the will of Allah” [she kept saying]. And I said, “so, if you want this girl that badly . . . let my brother marry her.” [She said:] “Are you saying this for real? Do you want to give your turn?” I said “mom, is there anything else to do? No there isn’t. What else have I got, except being a kind person? What can I do?” . . . So they sought my father’s advice, asked my opinion again and then they said “okay then let’s ask for the girl’s hand for [my brother].” . . . They [brother and his wife] are very happy now [and I console myself with it]. (Man, in his 20s)
Even if these participants knew about safe sex practices and about how PLHIV can have children, they stated that they did not want to risk causing physical or emotional harm, explaining this in terms of religious obligations related to not harming others.
“I would like to marry a negative [HIV-negative woman] and I would like to have a descent. But I wouldn’t like to violate kul hakkı. Kul hakkı is not only about not to steal you know.” (Man, in his 30s)
Kul hakkı and vebal were terms used by both married and single, heterosexual and homosexual men to explain their feelings of conscientious responsibility toward others. Some also used these terms when explaining their motivations for using condoms. By vebal they meant that they did not want to “shoulder the unworldly moral responsibility of an evil action,” whereas kul hakkı (“rightful due”) refers to the Islamic rule specifying protection of the rights people have with regard to each other.
The role of family in the construction of the sense of “normality”
Fulfilling family-related expectations has a role in the perception of “normality” and order in life. As mentioned earlier, participants’ familial situations served as a criterion and a reference point for their self-evaluation. Their reflexive accounts of whether or not life is good, normal, ordinary, or in order often included comparisons between their own and others’ familial situations. The unmarried compared their lives with those of married people; those who were married with no children compared themselves with people who have children. A sero-concordant couple (both spouses are HIV-positive) explained that their main aim was to have a child to complete their family and satisfy their relatives: [Our infection doctor] said “you’ll never have a baby.” . . . We were completely devastated. [We thought:] We’ll stand alone, at home, by our selves, like two deadwoods. I mean . . . you know, a child is required for a person, I mean a child is an important factor for a family, in my opinion. I mean this is one of the most important elements that make up a family. Er . . . as you would suppose or you would know, the child is one of the most important elements, that brings joy to home . . . child means the future. (Man, in his 30s)
A very clear example of how family status and roles serve to secure a sense of normality can be seen in a 40-years-old homosexual participant’s accounts. His first sentences after he stated that he identified himself as homosexual at the beginning of his interview were “Er . . . what can I tell you about my life story? Like every human, I too have a family. Like most people, I too was once married, I too have a child.” The last sentences of his uninterrupted life story (First BNIM session) were as follows: In conclusion, er . . . I told that I was a father; that I also have a mother and father, that I am a son, a younger brother and an older brother as well. I told you I have a job, a family life and a social life as every other person. . . Me being gay or being HIV patient er . . . doesn’t mean that I’m living in a different world. (Man, in his 40s)
Considering the differences between younger and older HIV-positive people, this sense of normality was stronger in people diagnosed with HIV at a stage when they have already established “order” in their lives. Also, it is important to note that, for openly gay men and for transsexuals, the “aim” or “hope” of “establishing the order” was not a question that had arisen after the diagnosis.
Discussion
The results showed that enacted stigma in the context of the family, such as being shunned or rejected by family members, was not common. Although this finding from a small sample of PLHIV cannot be generalized to all PLHIV living in Turkey, the observations of KIs, as well as previous research (Kasapoğlu, Kuş Saillard, Kaya, & Turan, 2011; Köse, Mandıracıoğlu, Mermut, Kaptan, & Özbel, 2012), support that acceptance from parents, spouses, and other close family members was common.
The results of Turkey’s PLHIV Stigma Index survey (SIT, 2011) supports the conclusion that PLHIV’s most important fears are the fear of being shunned by family (61%) and being left by spouse/partner (46%), whereas actual stigmatization is considerably less than anticipated. For example, 75% of participants described their spouse/partner as “supportive” or “very supportive.” Yet the highest rates of self-stigma were found to be related to family. Participants reported that they had decided not to get married (20%) and not to have children (28%), and isolated themselves from their families and friends (27%).
As a significant result of the study, the gendered nature of stigmatization in Turkey appeared to have different dimensions to those often found in other settings of gender inequality. In contrast to the findings of other studies set in the contexts of South Asia or Southern and Eastern Africa, in which HIV-positive women are blamed for bringing HIV into the household, thrown out of their homes, and/or subjected to violence (Ertürk, 2005; Ogden & Nyblade, 2005; Reis et al., 2013), the women participated in this research did not experience disproportionate or more violent forms of stigmatization from their spouses or their parents. Previous research (Aşar-Brown, 2007; Kasapoğlu & Kuş, 2008) has shown, and KIs in this research argued, that married women are in an “advantageous” position in terms of being perceived as “victims” who, because of their “purity” or “innocence,” could not have brought the disease and related shame onto themselves or the family. This is particularly remarkable in a cultural context where women are almost always blamed for “dishonouring” the family. It is very well-documented that in Turkey, women who came back to their parental house because of domestic violence are often rejected, are sent back, or face further violence from their parents. Women who are raped, even when the perpetrator is a relative, are blamed for “dishonouring” their family and are killed by their own fathers or brothers (Akkoç, 2004; Ertürk, 2004; Sirman, 2004). The support that HIV-positive women received from their husbands, their parents, and their husbands’ parents is therefore a particularly significant finding in this context.
Public perception of HIV-positive married women as “victims” affirmed that they find the only possible way for married women to be infected with HIV to be through their husbands’ extramarital affair(s). This shows that the general public does not fully agree that the ideal of “monogamy” is always upheld, or that the ideal “Turkish family structure” is always seen to be present, as set out in the statements of government authorities. 3 The responsibility of men in the transmission of HIV is acknowledged by PLHIV and by the people around them. However, the idea that female sex workers are the main drivers of the disease in the country (MoH of Turkey, 2006) provides a “scapegoat”: the sex worker or another “immoral” woman. In case the man did not acquire HIV from a sex worker, he must have acquired it from another woman—a woman to whom he did not choose to get married or a kind of woman who has sex out-of-wedlock, which makes her “unchaste.” Therefore, the acceptance of HIV-positive married women can be explained in terms of the existence of another female who can be blamed and the existence of an “official” discourse that approves it.
Another explanation for why HIV-positive married women are not blamed, as they would be in the case of rape, for example, stems from the fact that there is no “other” man involved in the situation. The perception of HIV-positive women as “victims” when they are married or when they “appear to conform to gender roles” suggests that a woman’s involvement in a relationship with a man, other than her husband, is unthinkable. It is not even regarded as a possibility. This echoes the general perception of women held by both secularists and conservatives in Turkey, as detached from their sexualities (İlkkaracan & Ronge, 2008). They are perceived as being “modest,” located in the private sphere of home, and as responsible for satisfying their husband’s demands. In this sense, even though the perception of women as victims seemingly puts them in a more advantageous position in terms of facing less discrimination, it reflects patriarchal values and as such is a form of social control over women’s behavior and their sexuality.
Previous research shows that HIV might have a particular effect on men in terms of damaging their “masculine reputation” (Siu, Wight, & Seeley, 2012, p. 1). Feeling sick and in need, being unable to work and care for the family, and a diminished “authority” in the household and in “sexual privileges” might contribute to the perception that HIV damages idealized masculinity (Siu et al., 2012; Wyrod, 2011). However, male participants of this research did not articulate any damage in their perceived masculinity due to those factors.
The role of perceived failure in fulfilling family-related roles in internalized stigma and in enacted stigma from family members was demonstrated in the general literature on HIV-related stigmatization. However, one important difference between the cases shown in this research and the ones discussed in previous research is that the male participants of this research did not articulate their perceptions about failure in family-related roles in terms of their identities as “breadwinners” (Wyrod, 2011). This is partially because of the sample bias, as very few participants had to stop working because of their ill health. Even those few married male participants who were unemployed at the time of the study due to their HIV status did not express their failure in terms of a failure to provide. Their narratives about “disappointing their families” were not related to their inability of providing for the family, but were expressed in terms of putting the lives of their family members in danger and making them feel sad.
This research contributes to understanding the relationships between adult HIV-positive individuals and their parents, which has received very little attention in the wider literature. Research in developing countries has tended to focus on the role of parents mainly as caregivers to their sick adult children, or as caregivers to their orphaned grandchildren (Saengtienchai & Knodel, 2001; Ukockis, 2007). As adults living with HIV have more distant relationships with their parents in the cultural settings mostly explored in the general HIV/AIDS literature, disclosure to and support from parents have not been major issues, unless the parents become the primary caregivers to their adult children. However, in the context of Turkey, where the relationship between parents and adult children continues to be very close, and living together with parents is very common even in later stages of life, parental support remains as important as support from the chosen family.
The link between socioeconomic background and level of stigmatizing attitudes, cited in the literature that was mentioned earlier, suggests a potential association between families’ socioeconomic conditions and their attitudes toward the HIV-positive family member. However, results of this research did not indicate such a connection. As mentioned above, there were cases in which families described as “educated and modern” were strongly maintaining traditional values around family, and families from low educational and economic background embracing their HIV-positive family member without reservation. In other words, the acceptance and/or support patterns did not show significant difference in terms of education, income, or urban/rural residency of the participants. This would be caused by the limitations of the sample, which contains relatively low numbers of people from rural areas and low economic status.
Policy Implications
Currently, there is no national policy or intervention in Turkey aimed at reducing HIV-related stigma or enhancing support mechanisms for PLHIV. The following recommendations based on the findings could contribute to the development of such policies.
Both parental and formed family members should be included as potential source of support in any policy/program developed in the future. Informative, educational, and communication materials designed for such programs should target all family members.
Considering the relationship between disclosure to spouses/partners and prevention of further transmission of HIV, beneficial, positive disclosure stories such as the ones exemplified here could be used in guiding safe partner disclosure decisions, which are important for both public health outcomes and PLHIV’s psychological well-being. (For a detailed discussion on disclosure patterns and more policy recommendations on the issue, please see Öktem, 2014a)
Family disclosure strategies and support/discussion groups for family members as developed and used by LGBT communities in Turkey could provide an example to be used in improving HIV-positive youth’s relationships with their parents.
Families being an important source of support means that family members can become primary caregivers. To minimize the social and economic burden of care on families in the future, family members should be provided with accurate information and adequate moral support. All interventions about care and support should be gender-sensitive, to prevent women from bearing a double burden of care.
Results showed that family support is not adequate for reducing anticipated and internalized stigma, in a context where prejudices and human rights violations prevail. Therefore, immediate steps should be taken to eradicate discrimination in health care and workplaces, to provide a protective legal framework for PLHIV, and to eliminate gender inequality.
Limitations
The main limitation of this research is that in the sample consisting of 24 PLHIV, the experiences of persons who did not seek treatment due to fear of stigmatization and of those who rejected to get in touch with anyone related to HIV/AIDS were not represented adequately. Although the numbers of people who are and who are not in regular contact with a support group were relatively balanced, it was not possible to reach people outside health care or people who are non-adherent to treatment. Second, and equally importantly, female sex workers (other than transsexuals) and the women who are perceived as the “source” of HIV, the “foreign sex workers,” could not be included. Inclusion of the above-mentioned populations, who withdraw themselves from social contact and perhaps seeking health care, would have provided the research with more insight about the higher fear of stigma they experience. Finally, while the participants differed in terms of demographic and health-related characteristics, inclusion of higher number of people from lower socioeconomic status would be beneficial in terms of comparing experiences across educational and economic backgrounds. Considering the scarcity of HIV-related social research conducted in Turkey, further qualitative and quantitative research is needed for a better understanding of PLHIV’s experiences.
Conclusion
Patterns of family support were seen in most participants’ narratives, which showed that PLHIV’s encounters with enacted stigma from their family members were less than they have expected. With regard to the experiences in the parental family, it is seen that a strong fear of rejection prior to disclosure caused self-isolation from parents/siblings. Positive disclosure outcomes expressed by the participants included closer and improved relationships with parents. Yet, closer attention from parents can also become a problem for some people, as such behavior might make them feel “sick” or “in need of help.”
The narratives about experiences in the formed family demonstrated acceptance and/or support by spouses for married participants, including women and men. Although their wives were the main source of support for married men, single heterosexual men mentioned their parents as the main source of support. Women participated in this research mostly accepted their HIV-positive spouses/partners and were accepted by their husbands’ families. These results pointed to different aspects of gender inequality which lie behind the acceptance and/or support from family members, as seen in the perception of married women as “victims” and in the silence surrounding the sexual orientation of homosexual HIV-positive family member.
It is also found that although patterns of acceptance and support were common, this did not mean that the institution of the family in Turkey was perceived by PLHIV as a source of comfort. Family support did not prevent people from having to struggle with a “tainted” or “deviant” identity. On the contrary, strong social expectations and personal desires around familial roles, and the cultural value attributed to “the family” in the ideal life trajectory, acted as the primary drivers of internalized and felt stigma. Future plans, turning points, and self-definitions, which are all related with how one attributes meaning to be actually living with HIV, were constructed around cultural values attributed to family, for the majority of the participants, regardless of the socioeconomic status of the families. Getting married, having children, being a “responsible” spouse/mother/father are perceived as the main sources of acquiring respected and valued social identities in the society of Turkey. Consequently, the actual and potential damaging effects of HIV on one’s life were evaluated by PLHIV in terms of the failures in fulfilling family-related social norms. The main ways in which these norms and values contributed to internalized stigma included the feeling of “guilt” and responsibility to family members, hopelessness and concerns about marriage felt by single participants, and the construction (or lost) of the sense of “normality” through the presence or absence of functional familial ties.
Results indicated that family is one of the main areas for detailed investigation if we are to understand the context-specific characteristics of HIV-related stigma in Turkey. Acceptance by both the parental and the formed family is an important factor of the nature of HIV-related stigma in Turkey, which differs from what was generally seen from the wider literature. The general lack of knowledge on HIV/AIDS among the society and the absence of counseling and support services, which are a result of the low priority given to HIV/AIDS in Turkey, could be seen as important factors contributing to the construction of internalized stigma in relation to family. Support from families has many positive effects on PLHIV. However, this great potential empowering effect of support received from family cannot be realized in the absence of comprehensive HIV-related interventions at national level. A safe and empowering environment for PLHIV, where family support could effectively contribute to improved health and life quality, can be reached in Turkey by enhancing support mechanisms, improving the sensitivity of health care workers, and creating a legal framework that protects human rights and gender equality for PLHIV and for most-at-risk populations.
Footnotes
Acknowledgements
The author expresses her deepest gratitude to all the participants of this research, to anonymous gatekeepers who facilitated the fieldwork, and to Dr. Steve Russell and Dr. Catherine Locke for their invaluable guidance.
Author’s Note
Turkish words used in this article are italicized.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The research was self-funded.