
Abstract
We investigated the psychometric properties of the Japanese version of the Posttraumatic Stress Disorder Checklist–Stressor Specific Version (PCL-S) using baseline data from the Fukushima Health Management Survey. A total of 26,332 men and 33,516 women aged 16 and above participated in this study. Participants lived in the Fukushima evacuation zone in Japan and experienced the Great East Japan Earthquake and nuclear power plant (NPP) incident. The PCL-S was used to assess participants’ posttraumatic stress disorder (PTSD) symptoms. In addition, we described participants and tested the validity of the PCL-S by administering the Kessler Six-item Screening Scale for Psychological Distress (K6) and assessing education; employment; self-rated health; sleep satisfaction; experiencing the earthquake, tsunami, and NPP incident; and bereavement as a result of the disaster. PCL-S scores exhibited a positively skewed, slightly leptokurtic distribution. Confirmatory factor analysis revealed that the five-factor model was a better fit than were the three- or four-factor models. The PCL-S and its subscales had high Cronbach’s alpha coefficients. The PCL-S scores had weak-to-moderate correlations with history of mental illness, bereavement, experiencing the tsunami, experiencing the NPP incident, self-rated health, and sleep satisfaction, as well as a strong correlation with psychological distress. There were significant gender and age differences in PCL-S scores. Overall, this study confirmed the psychometric properties of the PCL-S, including the score distribution, factor structure, reliability, validity, and gender and age differences. Thus, the Japanese version of the PCL-S would be a useful instrument for assessing the PTSD symptoms of community dwellers who have experienced traumatic events.
Keywords
Introduction
Some disaster sufferers experience posttraumatic stress disorder (PTSD) symptoms, including flashbacks, nightmares, and excessive anxiety. PTSD is a mental disorder that develops after exposure to traumatic events. The Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnostic criteria for PTSD include 17 symptoms classified into the following three clusters: re-experiencing, avoidance/numbing, and hyperarousal. To date, PTSD has been noted to occur in response to a wide variety of traumatic events, including natural disasters (e.g., earthquakes, tsunami, hurricanes; Arnberg, Michel, & Johannesson, 2014; Pietrzak, Van Ness, Fried, Galea, & Norris, 2012; Zhang, Shi, Wang, & Liu, 2011), man-made disasters (e.g., factory explosions, motor vehicle accidents, nuclear power plant [NPP] incident, terrorism; Bromet & Havenaar, 2007; Lang et al., 2007; Stellman et al., 2008; Taylor, Kuch, Koch, Crockett, & Passey, 1998), assault (e.g., domestic and sexual violence, sexual harassment; Blanchard, Jones-Alexander, Buckley, & Forneris, 1996; Krause, Kaltman, Goodman, & Dutton, 2007; Palmieri & Fitzgerald, 2005), severe diseases (e.g., cancer; Cordova, Studts, Hann, Jacobsen, & Andrykowski, 2000; DuHamel et al., 2004), and military actions (e.g., peacekeeping and settling disputes; Asmundson, Wright, McCreary, & Pedlar, 2003; Simms, Watson, & Doebbeling, 2002). PTSD symptoms can continue for years after the traumatic event and can have severe negative impacts on psychological and physical health. Therefore, it is critical to develop strategies for identifying and supporting people with PTSD symptoms.
On March 11, 2011, a massive earthquake and tsunami struck Japan, which led to the Fukushima Daiichi NPP incident (Yabe et al., 2014; Yasumura et al., 2012). Since then, there has been an urgent need to assess actual PTSD symptoms among evacuees both within and outside of Fukushima prefecture to provide them with the relevant support and to accumulate scientific evidence for assisting future disaster survivors in Japan.
The Posttraumatic Stress Disorder Checklist (PCL) is a self-report scale developed in the United States (Weathers, Litz, Herman, Huska, & Keane, 1993) comprising 17 items that correspond to the 17 symptoms of the DSM-IV diagnostic criteria for PTSD. It is a useful means of quickly identifying individuals requiring support in an emergency. Three versions of this scale have been developed: the PCL–Military Version (PCL-M; Weathers et al., 1994a), PCL–Civilian Version (PCL-C; Weathers et al., 1994b), and the PCL–Stressor Specific Version (PCL-S; Weathers et al., 1994c). So far, the psychometric properties of the Japanese version of the PCL-S have not been reported. As such, the present study aims to evaluate these properties, with a specific focus on score distribution, factor structure, reliability (i.e., internal consistency), and validity (i.e., construct validity).
We used a confirmatory factor analysis (CFA) to examine the factor structure of the PCL-S among community dwellers in Japan (Byrne, 2009). Determining the factor structure of the PCL-S is useful because “Proper identification of symptom structure can improve our understanding of PTSD and, in so doing, inform its assessment, diagnosis, and treatment” (Palmieri & Fitzgerald, 2005, p. 657). Because the PCL-S is based on the three PTSD symptom clusters of the DSM-IV (American Psychiatric Association, 1994), it was initially reported as having a three-factor structure (re-experiencing [five items; Items 1-5], avoidance/numbing [seven items; Items 6-12], and hyperarousal [five items; Items 13-17]). However, little empirical support has been obtained for the three-factor model (Elhai & Palmieri, 2011). Indeed, the majority of reports utilizing CFA to clarify the factor structure have found support for 2 four-factor models and, more recently, a five-factor model. The four-factor models include the “numbing model” (re-experiencing [five items; Items 1-5], avoidance [two items; Items 6-7], numbing [five items; Items 8-12], and hyperarousal [five items; Items 13-17]; Asmundson et al., 2000; DuHamel et al., 2004; Elhai, Gray, Docherty, Kashdan, & Kose, 2007; King, Leskin, King, & Weathers, 1998; Palmieri & Fitzgerald, 2005; Schinka, Brown, Borenstein, & Mortimer, 2007) and the “dysphoria model” (re-experiencing [five items; Items 1-5], avoidance [two items; Items 6-7], dysphoria [eight items; Items 8-15], and hyperarousal [two items; Items 16-17]; Baschnagel, O’Connor, Colder, & Hawk, 2005; Krause et al.,2007; Simms et al., 2002). The five-factor model has gained some empirical support in recent years; it comprises factors of re-experiencing (five items; Items 1-5), avoidance (two items; Items 6-7), numbing (five items; Items 8-12), dysphoric arousal (three items; Items 13-15), and anxious arousal (two items; Items 16-17; Armour et al., 2012; Arnberg et al., 2014; Elhai et al., 2011; Pietrzak et al., 2012). Given these discrepancies, we sought to clarify the factor structure of the PCL-S by comparing the goodness of fit of the original three-factor model with that of the four-factor models (i.e., the numbing and dysphoria models) and the five-factor model (i.e., the dysphoria-arousal model).
To examine the scale’s validity, we performed correlation analyses between the PCL-S scores and various external criterion variables, as follows. First, because PTSD symptoms show high lifetime comorbidity with other psychiatric disorders such as major depression and anxiety (Breslau, 2001a; Wilkins, Lang, & Norman, 2011), we assumed that individuals with a history of mental illness would have higher PCL-S scores. In the same vein, PCL-S scores would likely relate to psychological distress, which has a confirmed link with PTSD symptoms (Paxson, Fussell, Rhodes, & Waters, 2012). Thus, we administered the Kessler Six-item Screening Scale for Psychological Distress (K6), which has been widely used in community surveys as an indicator of psychological distress (Furukawa, Kessler, Slade, & Andrews, 2003; Sakurai, Nishi, Kondo, Yanagida, & Kawakami, 2011).
Second, we expected PTSD symptoms to influence both physical and mental health status; indeed, PTSD is associated with an increased risk of chronic physical complaints (e.g., gastrointestinal symptoms, pain; Breslau, 2001b) and poor self-rated health (Breslau, 2001b). Thus, we investigated the relation of the PCL-S with self-rated health, which we used as an indicator of physical health status.
Third, PTSD symptoms are well-known to correlate with sleep problems (e.g., Germain, Hall, Krakow, Katherine Shear, & Buysse, 2005)—in fact, the DSM-IV criteria for PTSD include symptoms of insomnia (American Psychiatric Association, 1994), and the PCL-S itself contains items on disturbed sleep (Item 13; Weathers et al., 1994). As such, we expected that the PCL-S would relate to subjective sleep satisfaction (using a single item), which we used as an indicator of sleep problems.
Finally, there is little doubt that the events caused by the Great East Japan Earthquake—the tsunami, NPP incident, and bereavement as a result of these disasters—were extreme traumatic stressors and thus enough to satisfy the DSM-IV’s diagnostic criteria for PTSD (Criteria A). Given that previous studies have reported significant relationships between PTSD symptoms and experience of bereavement (Tural et al., 2004; Zhang et al., 2011), tsunami (Heir et al., 2011), and NPP incidents (Bromet & Havenaar, 2007), we expected that individuals who had experienced these events in addition to the earthquake were at a greater risk of PTSD symptoms than were those who had not. As such, significant correlations were expected between PCL-S scores and experience of each event.
We also sought to identify gender and age differences in PCL-S scores as part of assessments of its psychometric properties. There is robust evidence that women are more likely to develop PTSD (Breslau, 2001a, 2001b) and experience PTSD symptoms as assessed by the PCL (Freedy et al., 2010; Kline et al., 2013) than are men. Therefore, we expected that women would tend to score higher on the PCL-S than would men. Meanwhile, there has been no consistent finding regarding age differences in PCL-S scores. Thus, we sought to explore any age-related differences in the PCL-S among community dwellers in Japan.
In summary, we determined the psychometric properties of the Japanese version of the PCL-S using baseline data from the Fukushima Health Management Survey conducted in 2012. Specifically, we determined (a) the frequencies of responses to the PCL-S items, (b) the distribution of PCL-S scores, and the (c) factor structure, (d) reliability, and (e) validity of the PCL-S, as well as (f) whether there are gender and age differences in PCL-S scores.
Method
The data for the present study were drawn from a longitudinal study monitoring the mental health status of evacuees of the Fukushima Daiichi NPP incident (i.e., the Fukushima Health Management Survey). A detailed description of this survey is provided elsewhere (Yabe et al., 2014; Yasumura et al., 2012). In this article, we analyzed cross-sectional data from the 2012 survey.
Participants
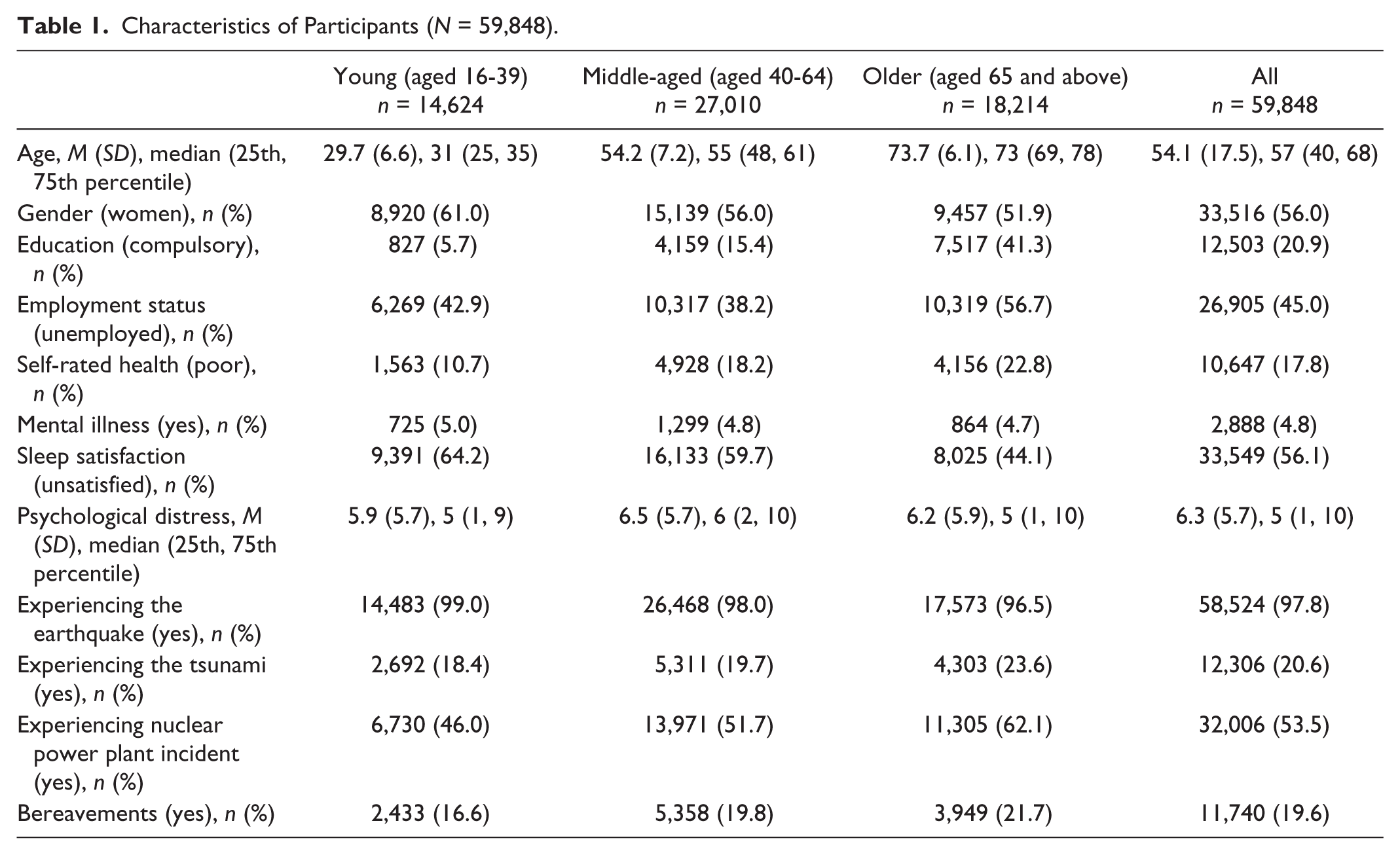
The study participants were the entire population of community dwellers who lived in the evacuation zone designated by the government (N = 210,189) and who were 16 years old or older as of March 11, 2011. The participants’ residential information was obtained from the municipal resident registration files. These 180,604 residents were invited to take part in a mail survey, and 73,569 residents responded (response rate: 40.7%; Yabe et al., 2014). Among them, 13,721 were excluded from the analyses for the following reasons: 136 questionnaires were virtually blank; 9,245 were completed by a proxy; 1,422 had not experienced the disasters; and 2,918 had two or more missing values on the PCL-S. In total, data from 59,848 individuals were used in the present analyses. Participants were divided into three groups according to their age at the time of the survey: young (i.e., adolescents and young adults): 16 to 39 years old (n = 14,624); middle-aged: 40 to 64 years old (n = 27,010); and older: 65 years and above (n = 18,214). This age classification was determined based on a developmental psychology framework on the developmental processes of the human life span (Azuma, Shigeta, & Tajima, 1992). Furthermore, our classification of the middle-aged and older groups accords with the division of “Class 2 Insured” individuals (40-64 years old) and “Class 1 Insured” individuals (65 years and above), respectively, in the long-term care insurance system in Japan (Long-term Care Insurance Division, Social Welfare Department, Shinjuku City, 2011). Table 1 shows the baseline characteristics of the participants.
Characteristics of Participants (N = 59,848).
Measurements
PTSD symptoms were measured using the PCL-S. The English-to-Japanese translation procedure used for the PCL-S is described below. After the translation was authorized by the scale’s original author (Weathers et al., 1994c), a Japanese psychiatrist translated the original English version into Japanese. This Japanese version was then back-translated by two native English-speaking bilingual scientists. One was a mental health professional with a background in social work, and the other was a mental health professional with a background in ethnography. These two scientists were blind to the original version of the scale. The back-translated version was then compared with the original, and adjustments were made to the Japanese version with consideration of the linguistic and semantic equivalents.
Using the PCL-S (Weathers et al., 1994c), we asked participants about their experiences with the Great East Japan Earthquake, including the earthquake itself and the tsunami and NPP incident. The PCL-S comprises 17 items rated on a 5-point Likert-type scale (1 = not at all, 2 = a little bit, 3 = moderately, 4 = quite a bit, and 5 = extremely) to assess the extent to which participants have been bothered in the past month by the 17 symptoms of PTSD based on the DSM-IV.
Item scores were summed to provide total PTSD symptom scores (range = 17-85), with higher scores reflecting a higher level of PTSD symptoms. With regard to handling missing values, those who had only one missing value were included in the present analysis; the missing value was replaced by the mean of the remaining 16 items (Gries et al., 2010).
Additional measurements were also used: Psychological distress was measured using the K6 (Furukawa et al., 2003; Sakurai et al., 2011), which comprises six items rated on a 5-point Likert-type scale. Item scores are summed to provide a score for total psychological distress (range = 0-24), with higher scores reflecting higher distress. The Cronbach’s alpha coefficient for all six items of the K6 was .91. We also assessed educational attainment, employment status (employed/unemployed), history of mental illness (yes/no), self-rated health (1 = very good, 2 = good, 3 = normal, 4 = poor, and 5 = very poor), sleep satisfaction (1 = satisfied, 2 = slightly dissatisfied, 3 = quite dissatisfied, and 4 = very dissatisfied or haven’t slept at all), experiencing the earthquake (yes/no), experiencing the tsunami (yes/no), experiencing the NPP incident (yes/no), and bereavement as a result of the Great East Japan Earthquake (yes/no). Participants who had experienced the NPP incident included those who had heard the explosive sounds from the Fukushima Daiichi NPP that occurred between March 12 and 15, 2011.
Data Analysis
CFA was conducted to examine the factor structure of the PCL-S. As noted above, we assessed four models: the three-factor DSM-IV model, the four-factor numbing model, the four-factor dysphoria model, and the five-factor dysphoria-arousal model (see Table 2 for the item mapping of the PCL-S). Four indices of model fit were used: the standardized root mean square residual (SRMR), the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the Akaike information criterion (AIC; Byrne, 2009). According to previous studies, model fit is deemed “adequate” when the CFI, RMSEA, and SRMR are ≥0.90, ≤0.08, and ≤0.10, respectively, while it is deemed “excellent” when they are ≥0.95, ≤0.06, and ≤0.08, respectively (Byrne, 2009; Hu & Bentler, 1999; Simms et al., 2002). The AIC is used when comparing two or more models, with smaller values being indicative of a better fit (Byrne, 2009).
Item Mapping and Model Fit Indexes for Confirmatory Factor Analysis in the PCL-S (N = 59,848).

Note. PCL-S = Posttraumatic Stress Disorder Checklist–Stressor Specific Version; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.); R = Re-experiencing; AV = Avoidance; N = Numbing; D = Dysphoria; H = Hyperarousal; DA = Dysphoric Arousal; AA = Anxious Arousal; SRMR = standardized root mean square residuals; CFI = comparable fit index; RMSEA = root mean square error of approximation; AIC = Akaike information criterion.
The Cronbach’s alpha coefficients for the 17-item total score and each of the subscales of the PCL-S were calculated as indices of scale score reliability.
Because of non-normal distributions, Spearman’s rank correlation coefficients were calculated to examine the validity of the PCL-S total score and its subscales. Seven external criteria were used: history of mental illness, bereavement, experiencing the tsunami, experiencing the NPP incident, psychological distress (K6), self-rated health, and sleep satisfaction.
Descriptive statistics were calculated and distributions plotted. Again, due to non-normal distributions, the Mann–Whitney U test was conducted to examine gender differences in PCL-S scores. The Kruskal–Wallis test was conducted to examine age differences, followed by Mann–Whitney U tests for multiple comparisons within each age group, applying the Bonferroni correction (alpha level modified to .0167).
All probability values were two-tailed. We used IBM SPSS Statistics Version 22 and IBM SPSS AMOS 22 (IBM Corp., Armonk, NY ) for the analyses.
Ethical Considerations
The study was approved by the Ethics Committee of Fukushima Medical University. The study was described to all participants, who were advised that their participation would be entirely voluntary, that they could withdraw from the study at any time, and they would not be disadvantaged in any way if they chose to withdraw or to not participate.
Results
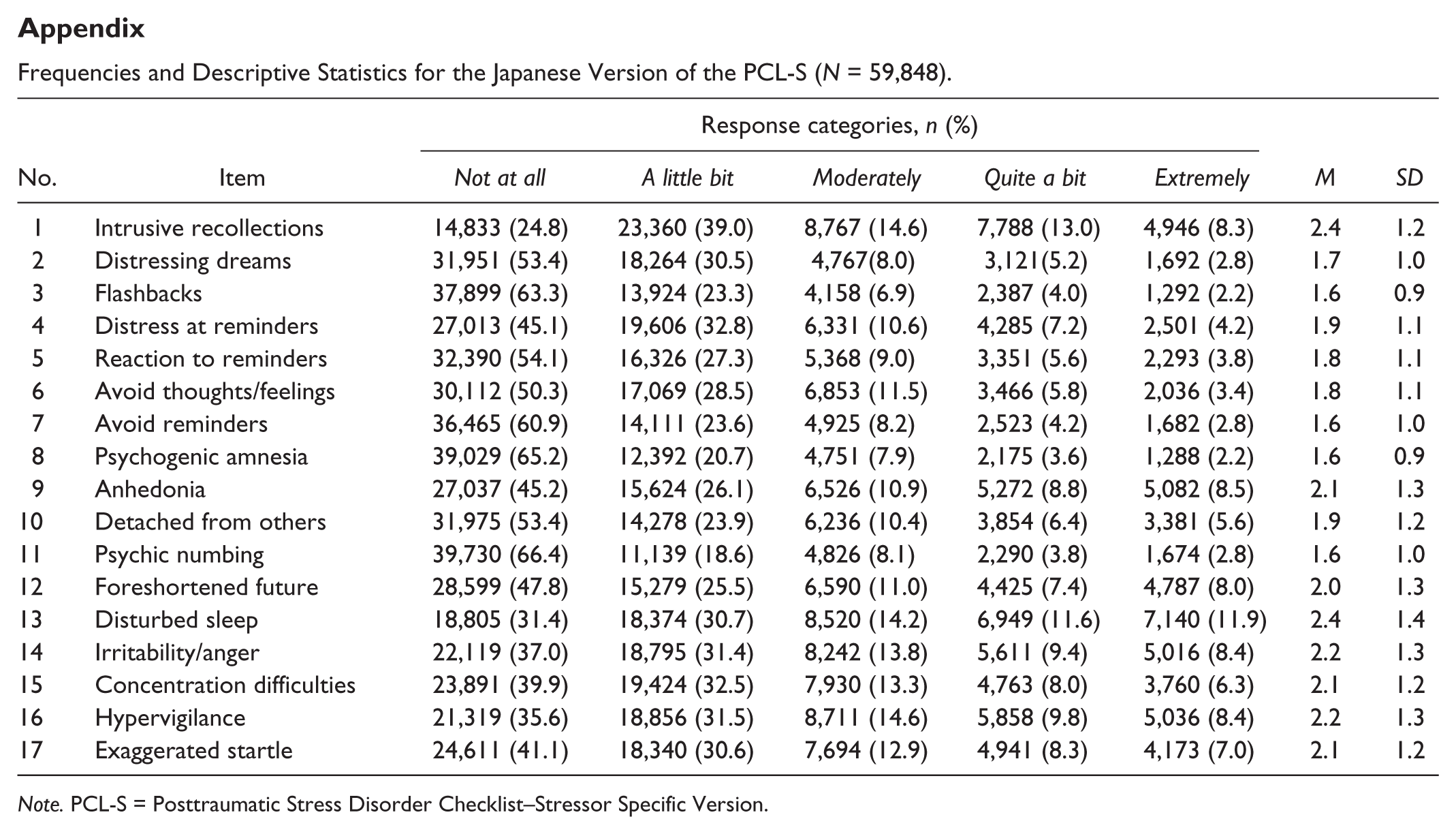
The response frequencies, as well as the mean scores and standard deviations for each item on the PCL-S, are shown in the appendix.
Figure 1 shows the distribution of PCL-S scores. Note that the distribution of PCL-S scores was positively skewed (skewness = 1.13) and slightly leptokurtic (kurtosis = 0.73).

Distribution of the Japanese version of the PCL-S.
The CFA showed the following results: The three-factor DSM-IV model had few acceptable model fit values (χ2 = 67,135.8; df = 116; p < .01; SRMR = 0.04; CFI = 0.91; RMSEA = 0.10; AIC = 67,209.8). In contrast, the four-factor numbing (χ2 = 46,605.4; df = 113; p < .01; SRMR = 0.04; CFI = 0.94; RMSEA = 0.08; AIC = 46,685.4) and dysphoria models (χ2 = 42,901.1; df = 113; p < .01; SRMR = 0.04; CFI = 0.95; RMSEA = 0.08; AIC = 42,981.1) had adequate fit values. However, the five-factor dysphoria-arousal model showed several excellent fit values (χ2 = 33,414.1; df = 109; p < .01; SRMR = 0.04; CFI = 0.96; RMSEA = 0.07; AIC = 33,502.1); thus, we retained the five-factor model.
Figure 2 shows the standardized factor loadings and inter-factor correlations in the CFA using the five-factor model. The smallest loading was that of Item 8 (0.64), and the largest one was that of Item 17 (0.91). Inter-factor correlations were .83 for Factors 1 and 2, .80 for Factors 1 and 3, .76 for Factors 1 and 4, .79 for Factors 1 and 5, .79 for Factors 2 and 3, .70 for Factors 2 and 4, .71 for Factors 2 and 5, .90 for Factors 3 and 4, .81 for Factors 3 and 5, and .86 for Factors 4 and 5.

Factor loadings and inter-factor correlations in a confirmatory factor analysis of the Japanese version of the PCL-S (the five-factor dysphoria-arousal model; N = 59,848).
Regarding the scale score reliability, the Cronbach’s alpha coefficients for all 17 items and for the PCL-S subscales were .95 (all 17 items), .91 (Factor 1), .86 (Factor 2), .86 (Factor 3), .85 (Factor 4), and .89 (Factor 5).
The validity analyses revealed that there were significant relationships between the PCL-S and all criterion variables (Table 3). Specifically, PCL-S scores were relatively weakly associated with history of mental illness (rs = .18, p < .001), bereavement (rs = .18, p < .001), experiencing the tsunami (rs = .14, p < .001), and experiencing the NPP incident (rs = .23, p < .001). Moderate correlations were found between PCL-S scores and self-rated health (rs = .43, p < .001) and sleep satisfaction (rs = .49, p < .001), and a strong correlation was found between PCL-S scores and psychological distress (K6; rs = .76, p < .001). The results for the five subscales of the PCL-S were very similar (see Table 3).
Validity of the Japanese Version of the PCL-S (N = 59,848).

Note. All correlation coefficients were significant (p < .001). Higher scores for the PCL-S, psychological distress, sleep satisfaction, and self-rated health indicate a poorer state in each index. NPP = nuclear power plant; PCL-S = Posttraumatic Stress Disorder Checklist–Stressor Specific Version.
The median (25th, 75th percentiles) values on the PCL-S among young, middle-aged, and older men were 24 (19, 35), 27 (20, 37), and 29 (20, 41), respectively. Median values among young, middle-aged, and older women were 28 (21, 39), 31 (23, 42), and 33 (23, 48), respectively. The Mann–Whitney U test revealed significant inter-gender differences (U = 374,637,025; p < .001), with median PCL-S scores being higher for women than for men.
The Kruskal–Wallis test revealed significant differences in PCL-S scores by age (χ2 = 599.1, df = 2, p < .001). Specifically, median PCL-S score for the older group was higher than were those for the young (U = 112,683,107.5; p < .001) and middle-aged groups (U = 227,445,494.5; p < .001). Furthermore, the median for the middle-aged group was higher than was that of the young group (U = 180,754,861.5; p < .001).
Discussion
The study aim was to determine the psychometric properties of the Japanese version of the PCL-S using baseline data from the Fukushima Health Management Survey. We presented response frequencies and the distribution of scores on the PCL-S, and confirmed its factor structure, reliability, and validity. We also found significant differences in PCL-S scores by gender and age.
The items with the highest mean scores were Item 1 (intrusive recollections, M = 2.4) and Item 13 (disturbed sleep, M = 2.4; see the appendix). The Great East Japan Earthquake led individuals to experience a number of simultaneous, extreme, and unprecedented events (i.e., the earthquake itself as well as the tsunami and NPP incident). In addition, after the disaster, they were forced to evacuate and spend time in an unfamiliar place (i.e., temporary housing; Brumfiel, 2013). Therefore, they may be prone to intrusive recollections of the disasters and disturbed sleep in their everyday lives. A similar finding was noted in a previous study, wherein Item 1 (intrusive recollections) had the highest mean scores among older sufferers of a natural disaster (Pietrzak et al., 2012).
As shown in Figure 1, the distribution of PCL-S scores was positively skewed and slightly leptokurtic, with the most frequent score being 17, which is the lowest possible score. This suggests that a majority of participants were not experiencing PTSD symptoms 1 year after the disaster. However, 176 participants (0.3%) had the maximum score (85 points), which suggests that there might have been individuals who still suffered from high levels of distress caused by trauma exposure during the disasters 1 year after the disasters; immediate aid for those high-risk individuals is likely required.
According to the results of the CFA, the three-factor DSM-IV model had a relatively poor model fit overall. In contrast, the four-factor models and the five-factor model both had adequate model fit indices (Byrne, 2009; Hu & Bentler, 1999; Simms et al., 2002). We decided to retain the five-factor model because its fit indices best approached the “excellent fit” cutoffs described previously (Byrne, 2009; Hu & Bentler, 1999; Simms et al., 2002). Our findings on the factor structure of the PCL-S are consistent with those of several recent studies (Armour et al., 2012; Arnberg et al., 2014; Elhai et al., 2011; Pietrzak et al., 2012). In addition, the correlations between the five factors were all very strong, which also coincides with the results of previous studies (Armour et al., 2012; Elhai et al., 2011).
The Cronbach’s alpha coefficients for the PCL-S and its subscales were very high, suggesting strong scale score reliability. This is consistent with previous studies, which have also reported high reliability for the PCL-S (Blanchard et al., 1996; Blanchard, Rowell, Kuhn, Rogers, & Wittrock, 2005; Wilkins et al., 2011; Zhang et al., 2011).
The validity testing revealed that PCL-S scores were significantly but relatively weakly correlated with a history of mental illness, bereavement, experiencing the tsunami, and experiencing the NPP incident. In addition, correlations were moderate with self-rated health and sleep satisfaction, and strong with psychological distress (Table 3). These results indicate that the PCL-S has good validity in relation to (a) mental illness and psychological distress (Armour et al., 2012; Breslau, 2001a; Wilkins et al., 2011; Zhang et al., 2011), (b) self-rated health (Breslau, 2001b), (c) sleep problems (Germain et al., 2005), and (d) experiencing disaster-related events (i.e., bereavement, tsunami, and the NPP incident; Bromet & Havenaar, 2007; Heir et al., 2011; Tural et al., 2004; Zhang et al., 2011).
We found a significant gender difference in PCL-S scores in this study, with the median for women being higher than that for men. This accords with previous findings among community dwellers (Freedy et al., 2010) and a military sample (Kline et al., 2013), wherein women tended to have more PTSD symptoms as assessed by the PCL than did men. PTSD scores have also been shown to be higher among women when measured using the Impact of Event Scale–Revised, Japanese Version (Asukai et al., 2002), which suggests that women are more vulnerable to developing PTSD symptoms.
There were also significant differences in PCL-S scores based on age, with the older group obtaining the highest scores and the young group obtaining the lowest; this suggests that PTSD symptoms assessed using the PCL-S in older individuals are likely to be more severe than those in younger individuals. Research has shown that older individuals may be more vulnerable to not only traumatic stress but also secondary psychological distress induced by lifestyle changes as a result of the disasters and relocations (Chen et al., 2011). The majority of participants in this study were forced to evacuate, and therefore experienced a drastic lifestyle change due to the NPP incident or massive earthquake. In fact, one previous study reported that there was high excess mortality among institutionalized older people who were relocated after the disaster in this area (Yasumura, Goto, Yamazaki, & Reich, 2013). Other explanations for the higher scores include that, compared with the young and middle-aged groups, the older group had a lower education level (Heir et al., 2011) and poorer self-rated health (Breslau, 2001b), and had experienced much greater frequencies of disaster-related traumatic events (Bromet & Havenaar, 2007; Heir et al., 2011; Tural et al., 2004; Zhang et al., 2011), all of which are risk factors for PTSD.
This study has some limitations. First, as this study was conducted in one region of Japan, the external validity of these findings may be limited. Nevertheless, this study examined the psychometric properties of the Japanese version of the PCL-S using a large sample (N = 59,838) of community dwellers with a broad age range (16 to 100 years). Second, as participants in this study were evacuees of the disaster, some aspects of the findings may not be the same as those of previous studies on PTSD symptoms among sufferers of other traumatic events. However, it should be noted that the factor structure of the PCL-S in this study was consistent with that of previous studies involving primary care medical patients (Armour et al., 2012, Study 2), victims of domestic violence (Elhai et al., 2011), war veterans (Armour et al., 2012, Study 1), and disasters victims (Pietrzak et al., 2012). This suggests that the PCL-S has a relatively stable factor structure regardless of the profiles of the respondents and the type of events to which they were exposed (Wilkins et al., 2011). Third, we did not examine test–retest reliability of the Japanese version of the PCL-S; we examined only the internal consistency reliability using Cronbach’s alpha coefficients. In future studies, the test–retest reliability of the scale should be examined to further confirm the psychometric properties of the scale.
This study also has several strengths and unique qualities. First, this study was conducted among a very large sample of community dwellers who experienced multiple extreme events, including an earthquake, tsunami, and NPP incident. Second, this study collected data quite promptly, only 1 year after the disaster occurred. Finally, the study examined a variety of possible factor structures based on the literature and concluded that the five-factor structure was the best fit.
In conclusion, this study aimed to determine the psychometric properties of the Japanese version of the PCL-S using baseline data from the Fukushima Health Management Survey. Standard psychometric methods showed a positively skewed and slightly leptokurtic score distribution. Furthermore, the PCL-S had a five-factor structure, excellent reliability, and good validity (according to the weak-to-moderate correlations with mental illness, bereavement, experiencing the tsunami, experiencing the NPP incident, self-rated health, and sleep satisfaction, and the strong correlation with psychological distress). We also noted significant differences based on gender and age in the PCL-S scores. In summary, the results indicate that the Japanese version of the PCL-S is a useful instrument for assessing PTSD symptoms among community dwellers who have experienced traumatic events.
Footnotes
Appendix
Frequencies and Descriptive Statistics for the Japanese Version of the PCL-S (N = 59,848).
| No. | Item | Response categories, n (%) |
M | SD | ||||
|---|---|---|---|---|---|---|---|---|
| Not at all | A little bit | Moderately | Quite a bit | Extremely | ||||
| 1 | Intrusive recollections | 14,833 (24.8) | 23,360 (39.0) | 8,767 (14.6) | 7,788 (13.0) | 4,946 (8.3) | 2.4 | 1.2 |
| 2 | Distressing dreams | 31,951 (53.4) | 18,264 (30.5) | 4,767(8.0) | 3,121(5.2) | 1,692 (2.8) | 1.7 | 1.0 |
| 3 | Flashbacks | 37,899 (63.3) | 13,924 (23.3) | 4,158 (6.9) | 2,387 (4.0) | 1,292 (2.2) | 1.6 | 0.9 |
| 4 | Distress at reminders | 27,013 (45.1) | 19,606 (32.8) | 6,331 (10.6) | 4,285 (7.2) | 2,501 (4.2) | 1.9 | 1.1 |
| 5 | Reaction to reminders | 32,390 (54.1) | 16,326 (27.3) | 5,368 (9.0) | 3,351 (5.6) | 2,293 (3.8) | 1.8 | 1.1 |
| 6 | Avoid thoughts/feelings | 30,112 (50.3) | 17,069 (28.5) | 6,853 (11.5) | 3,466 (5.8) | 2,036 (3.4) | 1.8 | 1.1 |
| 7 | Avoid reminders | 36,465 (60.9) | 14,111 (23.6) | 4,925 (8.2) | 2,523 (4.2) | 1,682 (2.8) | 1.6 | 1.0 |
| 8 | Psychogenic amnesia | 39,029 (65.2) | 12,392 (20.7) | 4,751 (7.9) | 2,175 (3.6) | 1,288 (2.2) | 1.6 | 0.9 |
| 9 | Anhedonia | 27,037 (45.2) | 15,624 (26.1) | 6,526 (10.9) | 5,272 (8.8) | 5,082 (8.5) | 2.1 | 1.3 |
| 10 | Detached from others | 31,975 (53.4) | 14,278 (23.9) | 6,236 (10.4) | 3,854 (6.4) | 3,381 (5.6) | 1.9 | 1.2 |
| 11 | Psychic numbing | 39,730 (66.4) | 11,139 (18.6) | 4,826 (8.1) | 2,290 (3.8) | 1,674 (2.8) | 1.6 | 1.0 |
| 12 | Foreshortened future | 28,599 (47.8) | 15,279 (25.5) | 6,590 (11.0) | 4,425 (7.4) | 4,787 (8.0) | 2.0 | 1.3 |
| 13 | Disturbed sleep | 18,805 (31.4) | 18,374 (30.7) | 8,520 (14.2) | 6,949 (11.6) | 7,140 (11.9) | 2.4 | 1.4 |
| 14 | Irritability/anger | 22,119 (37.0) | 18,795 (31.4) | 8,242 (13.8) | 5,611 (9.4) | 5,016 (8.4) | 2.2 | 1.3 |
| 15 | Concentration difficulties | 23,891 (39.9) | 19,424 (32.5) | 7,930 (13.3) | 4,763 (8.0) | 3,760 (6.3) | 2.1 | 1.2 |
| 16 | Hypervigilance | 21,319 (35.6) | 18,856 (31.5) | 8,711 (14.6) | 5,858 (9.8) | 5,036 (8.4) | 2.2 | 1.3 |
| 17 | Exaggerated startle | 24,611 (41.1) | 18,340 (30.6) | 7,694 (12.9) | 4,941 (8.3) | 4,173 (7.0) | 2.1 | 1.2 |
Note. PCL-S = Posttraumatic Stress Disorder Checklist–Stressor Specific Version.
Authors’ Notes
The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the Fukushima Prefecture government.
The Fukushima Health Management Survey Group Chairpersons: Masafumi Abe (Director General, Radiation Medical Center for the Fukushima Health Management Survey), Shunichi Yamashita, Kenji Kamiya (Vice Director, Radiation Medical Center for the Fukushima Health Management Survey), Makoto Akashi (National Institute of Radiological Sciences), Kazunori Kodama, and Kotaro Ozasa (The Radiation Effects Research Foundation).
Participating other expert committee members, advisors, and staff of the Mental Health and Lifestyle Survey of the Fukushima Health Management Survey: Ohtsura Niwa, Shiro Matsui, Tetsuya Ohira, Hirobumi Mashiko, Yasuto Kunii, Shuntaro Itagaki, Itaru Miura, Yoko Nakayama, Misao Ohta, Aya Goto, Mitsuru Hisata, Norito Kawakami, Mitsuaki Hosoya, Mayumi Harigane, Akiko Yagi, Yu-ichi Oikawa, Yuki Ueda, and Naoko Horikoshi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was supported by the national “Health Fund for Children and Adults Affected by the Nuclear Incident”.