
Abstract
This preliminary multiple case study examined the behavioral outcomes of neurocognitive training on children with attention-deficit/hyperactivity disorder (AD/HD) in China, as well as parent acceptance of the treatment. The training approach targeted working memory, impulse control, and attention/relaxation (via brain electrical activity). Outcome measures included overt behavior as rated by parents and teachers, AD/HD symptom frequency, and parent opinion/feedback. Training was completed by five individuals and delivered via a themed computer game with electroencephalogram (EEG) input via a wireless, single-channel, dry-sensor, portable measurement device. The objective (i.e., training outcomes and EEG) and subjective (i.e., parent ratings/feedback and teacher ratings) data suggested that use of the neurocognitive training resulted in reduced AD/HD behaviors and improvement in socially meaningful outcomes. The parents expressed satisfaction with the training procedure and outcomes. It is concluded that the innovative neurocognitive training approach is effective for improving behavior and reducing symptoms of AD/HD for children in China.
Introduction
The core characteristics of children with attention-deficit/hyperactivity disorder (AD/HD) are age-inappropriate levels of inattentive, impulsive, and hyperactive behaviors. These behaviors may result in repeated school failures, poor social functioning and relationships, and low self-concept and self-esteem (Bussing et al., 2012; DuPaul, McGoey, Eckert, & Vanbrakle, 2001; DuPaul & Stoner, 2003; Wiener et al., 2012).
Children with AD/HD form a large group in China, with prevalence estimates ranging from 4% to 12% (Chen, Zeng, & Dang, 2004; Sun et al., 2003; W. Zhang, Liu, Liao, & Gu, 2007; Zhang & Yu, 2000) and with boys 4 times more likely to be diagnosed than girls. The prevalence is in line with the data from other countries or cultures (e.g., Barkley, 2006).
Children with AD/HD in China face difficulties at school and home (Jin, Du, Zhong, & Rui, 2010; Wei, Su, & Jin, 2004; Zhang et al., 2007). In particular, they have low acceptance from their teachers (Jin et al., 2010), and behaviors such as inattention, talking out of the turn, and disrupting others are seen to have negative influences on classroom discipline (Ding, Li, Li, & Kulm, 2008; Shen et al., 2009). These perspectives are associated with a cultural belief that Chinese students are expected to be disciplined autonomously and work hard in school (Xie & Wang, 2010). Furthermore, Chinese society endorses that effort makes up for low ability. As indicated by the cross-cultural study by Norvilitis and Fang (2005), Chinese teachers are more likely to attribute the problem to poor parenting and the children’s low effort compared with teachers in the United States. In this sense, children with AD/HD, in comparison with children without AD/HD, have experienced more anxiety and depression, and had significantly lower satisfaction on peer relationships, school life, family life, and self-cognition (Xie et al., 2011; Xin et al., 2009).
Poor academic performance and low acceptance from teachers and peers can result in increased pressure (Wei et al., 2004) and reduced quality of life (Xie & Wang, 2010) for parents of children with AD/HD. Furthermore, Chinese parents face a dilemma about the use of medication that is currently the main treatment for AD/HD (Gai, Lan, & Liu, 2008). On one hand, as most families in China are under the one child policy, there is an expectation of rearing the “perfect only child” (Milwertz, 1997), and parents are eager to address the problem. On the other hand, Chinese parents are concerned about this method of treatment and express low acceptance. Huang and colleagues (2012) reported that 33.7% of parents were against medication and 27.3% would only consider it when there was no alternative. Chen, Jing, and Yang (2008) reported that less than one third of parents of children with AD/HD had chosen medication. Both studies indicate that Chinese parents are particularly concerned about the side effects that medication might have on their child’s cognitive and physical development.
Given negative attitudes toward medication, beliefs that they and the child are at least partially responsible for the problem, and Chinese parents’ strong need for technical and professional support for their children (Gu et al., 2010), it is not surprising that they look for alternative, positive, and safe treatments for AD/HD.
Neurocognitive Training for Children With AD/HD
Two alternative technology-based approaches to addressing symptoms of AD/HD are cognitive training and neurofeedback training. Cognitive training involves the use of purpose-designed computer software to exercise particular psychological abilities (e.g., memory) with the aim of improving them with practice. These tasks typically include performance feedback, with task difficulty varied according to performance to promote challenge, engagement, and learning. Neurofeedback training involves non-invasive measurement of ongoing brain electrical activity (electroencephalogram [EEG]) via electrodes on the scalp, with the user provided continuous simplified feedback about that activity (e.g., current level of attention shown as a number, a bar graph, or an engaging visual display). The aim of neurofeedback training is to promote awareness and control of psychological “state” factors that are reliably reflected in the EEG, such as high versus low attention or being relaxed versus tense. Several meta-analyses indicate research support for neurofeedback training as a method to reduce symptoms of AD/HD and improve behavior (Arns, De Ridder, Strehl, Breteler, & Coenen, 2009; Klingberg et al., 2005; Lofthouse, Arnold, Hersch, Hurt, & DeBeus, 2012). Evidence also supports the efficacy of working memory (Klingberg et al., 2005; Klingberg, Forssberg, & Westerberg, 2002) and combined working memory and inhibitory control training for children with AD/HD (Johnstone et al., 2012; Johnstone, Roodenrys, Phillips, Watt, & Mantz, 2010).
Our neurocognitive training approach targets fundamental cognitive processes such as working memory and inhibitory control, as well as the psychological state factors of attention and relaxation via neurofeedback (Johnstone, 2013). Together, these processes provide a foundation for an individual’s effective engagement with information in their external world. In the current study, these two treatment approaches are brought together for the first time in an attempt to enhance the behavioral benefits. This combined approach to training cognitive and state-control factors is supported by the cognitive energetic model (CEM) of AD/HD (Sergeant, 2005a, 2005b), which proposes that AD/HD stems from a state-regulation dysfunction that affects efficient engagement of computational/cognitive processes and executive functions. In the current study, EEG-based neurofeedback training is included to facilitate awareness and, with practice, control of the psychological states of attention and relaxation. In addition, working memory and inhibitory control training are included and conducted independently by different games. As suggested by the CEM, improved control over psychological/arousal states should provide a solid foundation for the effective engagement and use of cognitive processes, and concurrent training of these processes takes advantage of the dynamic interplay between them.
Foundation research in this area examined the cognitive elements of the neurocognitive approach, building on working memory training research (Klingberg et al., 2005) to include another fundamental and closely related psychological factor, inhibitory control (Johnstone et al., 2010). Note that short-term training of inhibitory control processes has been shown to improve behavioral control toward sweet foods and alcohol (e.g., Houben, Nederkoorn, Wiers, & Jansen, 2011). In the Johnstone et al. (2010) study, children with AD/HD carried out 25 training sessions using purpose-built software over a 5-week period. After training, children had improved at the training tasks, and their parents and another (potentially less-biased) adult observer reported significant behavioral improvements, with larger improvements for those who trained with a variable, as compared with fixed, difficulty level.
A subsequent study added attention-monitoring to the cognitive training via a portable, wireless, dry-sensor EEG recording device (Johnstone et al., 2012). The training promoted an awareness of attention (as measured by EEG) during cognitive training, with reward for good performance and focused attention. After training, task and behavioral improvements were reported, with these improvements being larger for those with than without AD/HD and slightly larger for children who used combined cognitive training and attention monitoring (compared with cognitive training alone).
In summary, the issues faced by children with AD/HD and their parents in China, as well as the findings of previous studies on neurocognitive training, warrant evaluative research undertaken in a cross-cultural context. The present study is a preliminary study that aims to evaluate feasability and outcomes of combined cognitive and neurofeedback training on the behavior of children with AD/HD in China. The study also examines parent acceptance of the training, as social validity is critical for determining the effectiveness of an intervention (Gresham & Lopez, 1996; Wolf, 1978).
Method
The present study involved five single cases. The procedures of training, data collection, and analysis were the same for all cases. Each case was conducted in a naturalistic way in that the training was undertaken at the child’s home, and children and parents decided the training time and could quit each session at any time. Technical support and training advice were available from the researcher if required. Such a design allowed the training to be evaluated as part of the everyday life of the children and their families. Due to the minimized control on the participants, outcomes measured in the study reflect children’s use of the training in their daily life (Lincoln & Guba, 1985). The research protocol was approved by the joint University of Wollongong and Illawarra and Shoalhaven Local Health District Human Research Ethics Committee prior to commencement of data collection.
Participants
Under recommendation of the local education department, two elementary schools in an urban area of China volunteered to participate in this study. Research advertisements were posted on the school’s notice board. Detailed information packages were provided at the school reception desk. Parents interested in the study contacted the researcher for further information. The first five children who had been clinically diagnosed with AD/HD and did not suffer from clinically significant comorbidities were recruited. The parents were requested to complete an information sheet that contained questions of diagnostic information of AD/HD (e.g., What subtype of AD/HD was your child diagnosed with? Please specify if your child is currently on any other form of medication.) and possible co-morbid diagnoses, including learning disabilities, intellectual disabilities, anxiety, and behavioral disorders. All the child participants had been diagnosed with AD/HD without other co-morbid diagnosis. In addition, the parents needed to provide supportive documents (e.g., certificate of diagnosis, approval of special service from local educational department) for the child participants’ qualification. The families were required to have a computer and Internet access at home. The background information for each child is listed in Table 1. Information about each child’s academic performance was collected through initial contact with the parents and homeroom teachers.
Background Information of Participating Children.
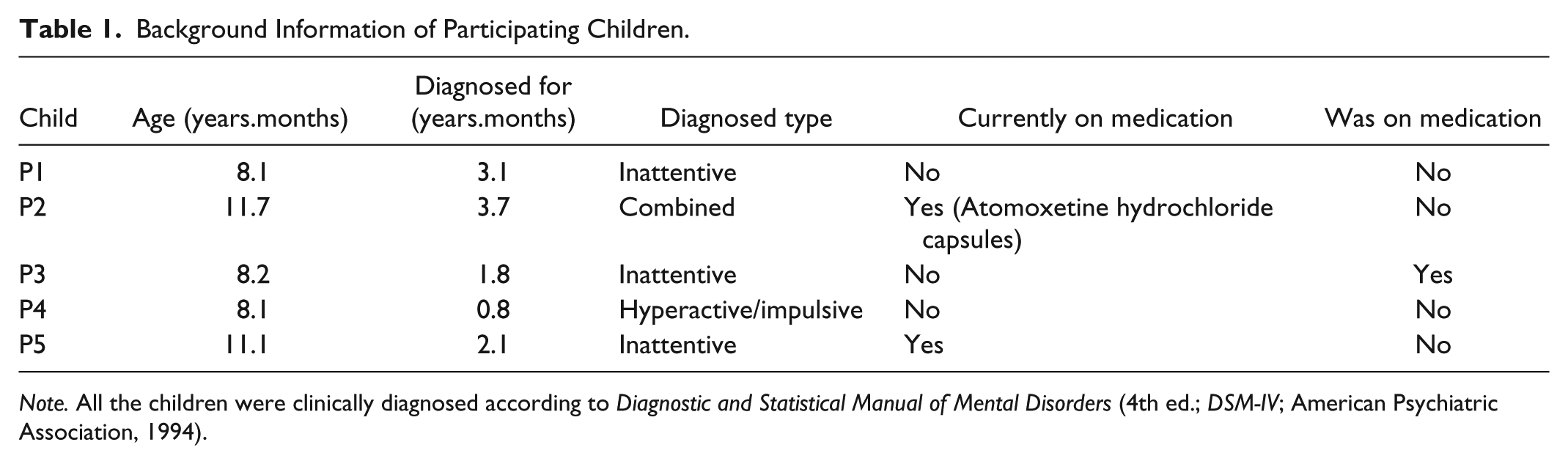
Note. All the children were clinically diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994).
P1’s academic performance was acceptable in the first semester of Grade 1, but became worse from the second semester. Sometimes, he did not know how to complete classroom activities and refused to take class quizzes or tests. Although he was placed in a general classroom, he was seated individually whereas other students were seated in pairs. After class, his mother supervised his completion of homework and checked the accuracy for 2 to 4 hours. He did not have any friends in his class but had a few in his neighborhood.
P2 refused to participate in most academic activities, quizzes, or tests, but showed some interest in mathematics. His academic achievements had been below minimum requirements since Grade 3. He began displaying serious problem behavior (e.g., excessive climbing, running away from class) in Grade 3. He was seated in isolation from other students in a general classroom and received extra tutorials in an after-school educational center. The school was worried about his safety and tried to persuade his parents to transfer him to a special school. However, the parents rejected the suggestion because they did not want P2 to be isolated from general education and a normal social life. He did not have any friends in school or his neighborhood.
P3 had fair academic achievements. He could participate in classroom activities and complete homework under adult supervision. Although he was seated with another student, he received more supervision from his teachers than other students. He had a few friends in school and his neighborhood.
P4 had difficulty adhering to classroom rules since Grade 1, including keeping in his seat and following teacher direction. He could only complete half of the classroom activities, assignments, or quizzes even under the teacher’s full supervision. He also displayed serious problem behavior (e.g., fighting, eating food and other items that were on the ground). Due to the nature of these issues, P4’s mother had accompanied his studying at school full-time for the last academic year. He did not have any friends both in school and his neighborhood.
P5 could complete most classroom activities and assignments but needed frequent teacher direction and feedback. He also could pass most quizzes and tests and showed above average performance in English. Although he was seated with another student, he received more supervision from his teachers than other students. He had a few friends in school and his neighborhood.
All the parents reported that it was the unmanageable problems displayed by their child and pressure from the schools that resulted in them seeking assessment that led to the diagnosis. Only two children were on medication at the start of training. P2’s mother stopped the medication during training because she perceived behavioral improvement. Although P5 was on medication, his parents sought non-medication treatments. The other parents reported a reluctance to have their child on medication because of known side effects. P3 had previously used medication for a short period, but stopped for this reason. P1’s and P4’s parents were against using medication. These negative attitudes about medication are consistent with the previous studies investigating Chinese parents’ attitudes (Chen et al., 2008; Huang et al., 2012).
Measures
Data collection involved four sources: questionnaire, parent interview, record of assignment completion, and data from the training. These consisted of quantitative and qualitative data, and responses from different stakeholders (i.e., parents and teachers). Data drawn from the training and record of assignment completion were unobtrusive, as they existed independent of the present study design. The use of multiple sources provides corroborating evidence, allows for convergent logic in the inquiry, and is key for ensuring validity in case study methodology (e.g., Creswell, 2007; Johnson & Turner, 2003; Merriam, 1988; Patton, 1990).
The Child Behavior Checklist (CBCL)
This standardized questionnaire is rated by parents to measure a child’s behavioral and emotional problems (Achenbach, 1991a). The CBCL is one of the most commonly used behavioral checklists and has been used widely in China (Achenbach et al., 2008; Tepper et al., 2008). It consists of 118 items rated on a 3-point Likert-type scale from not true (0) to very true (2). In the present study, the Chinese version of the CBCL was used, and ratings of 11 items of the syndrome Attention Problems were summed. The CBCL has good to excellent test–retest reliability (intraclass correlation coefficient [ICC] = .83) and validity (area under the curve [AUC] = .85) for Total Problems, and test–retest reliability (ICC = .79) and validity (AUC = .90) for the Attention Problems (Leung et al., 2006).
The Teacher Report Form (TRF)
This is the teacher version of the CBCL (Achenbach, 1991b). The Chinese version of TRF was used, and has good to excellent test–retest reliability (ICC = .85) and validity (AUC = .91) for Total Problems, and test–retest reliability (ICC = .87) and validity (AUC = .91) for the Attention Problems (Leung et al., 2006).
Behavior Rating Scale (BRS)
This is a purpose-designed 18-item questionnaire assessing the frequency of AD/HD characteristic behaviors based on the diagnostic criteria listed in DSM-IV (American Psychiatric Association, 2000). Ratings of the frequency of display of behaviors (e.g., “Has difficulty sustaining attention in tasks or play activities”) are made using a scale ranging from never (1) to always (5). The questionnaire was translated to Chinese, with independent back translation performed.
Parent interview
Semi-structured interviews were conducted before and after the training. The interview protocol was adapted from the subjective evaluation of social validation developed by Gresham and Lopez (1996). It consisted of 14 questions that addressed three aspects of social validation, namely, social significance of goals (e.g., Which behaviors are the most problematic for your child in learning?), social acceptability of procedures (e.g., How do you feel about the training program?), and social importance of effects (e.g., What are the outcomes that you have perceived from use of the training program?).
At the pre-training phase, parents were asked to provide responses to four questions in regard to the social significance of goals. The responses reflect the child’s problem that was the most troublesome to the parents. At the post-training phase, parents were asked to provide responses to five questions in regard to social acceptability of procedures and social importance of effects, respectively. Parents’ feedback at the pre- and post-training phases was compared and interpreted.
Record of assignment completion
The record was taken by the homeroom teachers to determine whether the child participants had completed their assignments in time. The homeroom teachers agreed to take the record constantly from 2 weeks before the training to 3 or 4 weeks after the training. To calculate the percentage of assignment completion for individual children, the number of completions in a week was divided by the total number of assignments in the same week and multiplied by 100.
EEG data
The dry-sensor EEG recording device constantly monitored and recorded EEG activity during training and was used to (a) control game-play during the state-control games and (b) quantify attention level during the working memory and impulse-control games. The device consists of microchips, embedded firmware, a 10 mm active electrode, and ear-clip reference ground electrode (ThinkGear, Neurosky, San Jose, California, USA) contained within a headset (MindWave, Neurosky, San Jose, California, USA). The EEG was recorded continuously from site Fp1 at 256 Hz and has been shown to be reliable and valid when compared with research-grade equipment (Johnstone et al., 2012). The device converted the raw signal from the time- to the frequency-domain via a fast Fourier transform to calculate EEG power in the delta, theta, alpha, and beta frequency bands (see Johnstone et al., 2012 for more information). Proprietary algorithms then calculate values representing two independent psychological state dimensions of “attention” (low to high; highly correlated with power in the beta EEG band) and “relaxation” (tense to calm; highly correlated with power in the alpha EEG band). These measures are presented as a value between 0 and 100, enabling the provision of generalized feedback about ongoing brain activity in a form understood by children. This method provides a robust and universal index of ongoing EEG activity that does not require individual calibration. An additional index, termed Zen, was calculated in the software by averaging the attention and relaxation indices. The state indices were sent to the PC wirelessly via a radio-frequency USB dongle connection. The single-channel frontal EEG data have been reported to be sensitive to psychological state variations that are relevant to the neurofeedback training goals contained within the state-control component of this training approach, that is, high versus low attention and high versus low relaxation (Johnstone et al., 2012). Note that the EEG is used actively in the state-control training (see “Training Session” section) but passively during the impulse control and working memory training, where it simply monitors background attention level and categorizes attention into low/medium/high/very-high as a multiplier for game points achieved (x1/x2/x3/x4, respectively). The device constantly monitors electrode impedance and provides an ongoing numerical representation of its quality. The neurocognitive training software monitors this value and if sub-standard impedance occurs at any point (e.g., device is removed, or as a result of substantial head movement), the training game is paused until acceptable impedance is once again achieved.
Game difficulty
The within-training game difficulty level data provided another way to look at changes in psychological abilities as a function of training. Difficulty level increases were based on perfect performance at the lower difficulty level. As difficulty level increased, the child was required to put in more effort and ability to maintain the cognitive processes and/or psychological state factors to complete the task at a high level.
Procedure
Pre-/post-training assessment
Data collection for pre-training assessment started when approval had been obtained from the parents and teachers. Parents were then asked to complete the child information form, the CBCL, and BRS, and were interviewed by the researcher. Teachers were required to complete the TRF and BRS. On completion of the training program, the same parent completed the CBCL and BRS and was interviewed by the researcher. Teachers were asked to complete the TRF and BRS.
Pre-training preparation
An information session about the software was provided to each child and a parent at their home. The software was installed on the home computer, and an instructional manual in Chinese was provided. The EEG device and software (see Figure 1) were provided at no cost. The researcher demonstrated each game first (for an example, see Figure 1) and then observed the participants to ensure understanding and answer any questions.
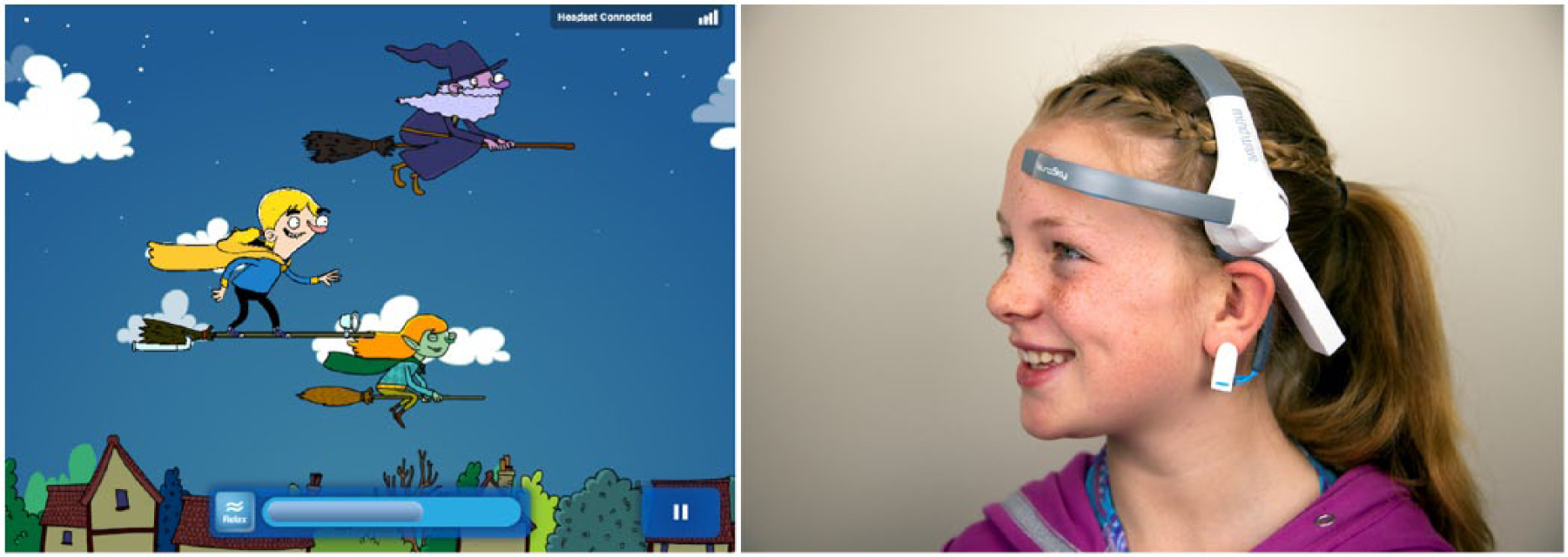
The dry-sensor EEG recording device (right) with active electrode on forehead and reference electrode on earlobe, and a screenshot of one state-control game (left).
Training sessions
The neurocognitive training consisted of 25 sessions, with each session lasting 15 to 20 min. Each session consisted of 14 games: 4 working memory, 4 impulse control, and 6 state control. The 6 state control games included 2 that were controlled by attention level, 2 controlled by relaxation level, and 2 controlled by combined attention and relaxation index (termed Zen; see below). The working memory games involved holding information in memory with subsequent recall to complete an action. The impulse-control games entailed a response to frequently presented “Go” stimuli and withholding of responses to infrequent “Nogo” stimuli. The state-control games required children to be attentive, relaxed, or in a “Zen” state (i.e., both attentive and relaxed), with game-play linked to levels of these EEG-derived factors. For example, the player’s speed in broomstick race was dependent on the level of attention above that particular player/games current threshold level. The threshold level increased with successful completion of the previous level and decreased if the previous level was not successfully completed. All games started at the lowest level of threshold/difficulty. Parents were asked to provide a quiet and consistent environment for each training session, so that the child would not be distracted during training.
Results
EEG Data During Training
The EEG summary score values, comparing the average of the first five training sessions with the last five training sessions (see Table 2), indicated that each participant was able to produce a higher level of the desired psychological state late in training for at least one of the three states.
EEG Summary Scores of Attention, Relaxation, and Zen at T1 (the First Five Training Sessions) and T2 (the Last Five Training Sessions).

Note. EEG scores range from 1 to 100. EEG = electroencephalogram.
Game Difficulty Level
Comparing game difficulty levels during the first five training sessions with last five training sessions (see Table 3) indicated that all participants were able to engage in the impulse control and working memory games with higher difficulty levels. Increases for impulse-control games were large for P3 and P5, and for working memory games were large for P2. Four participants were able to play higher levels in the attention-driven games. Fewer participants progressed to higher levels in the relaxation- and Zen-controlled games.
Average Game Difficulty Levels at T1 (the First Five Training Sessions) and T2 (the Last Five Training Sessions).
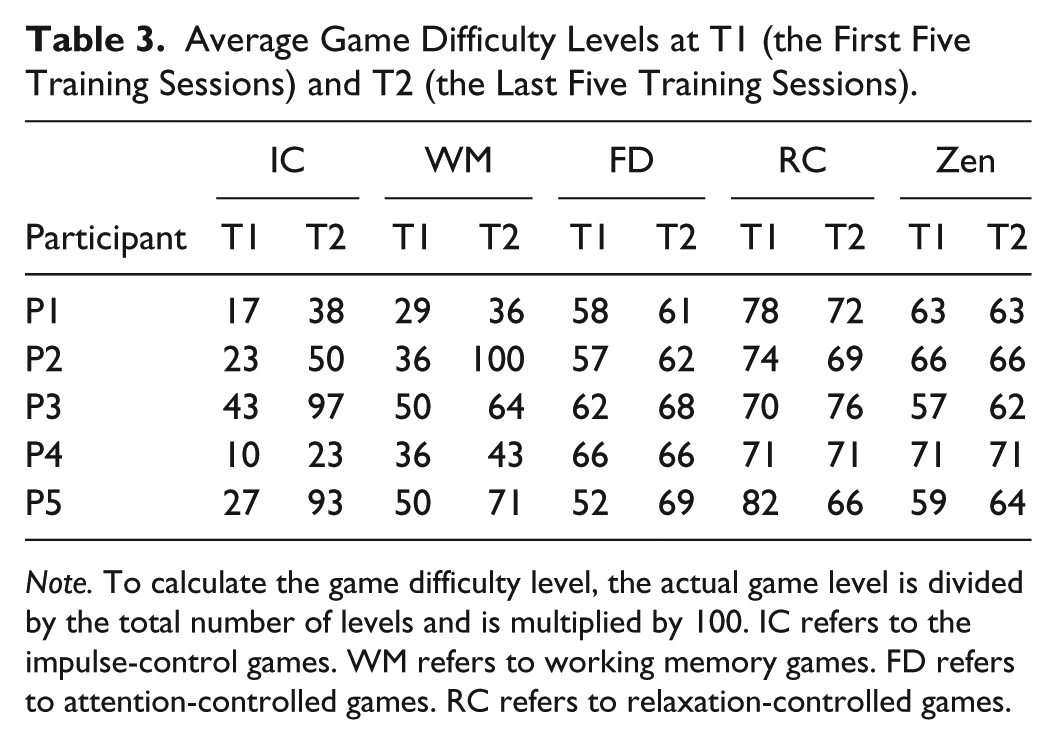
Note. To calculate the game difficulty level, the actual game level is divided by the total number of levels and is multiplied by 100. IC refers to the impulse-control games. WM refers to working memory games. FD refers to attention-controlled games. RC refers to relaxation-controlled games.
Behavioral Ratings
T-scores of Attention Problems on the CBCL and TRF for pre- and post-training stages are presented in Table 4. The scores were lower at post-training on both ratings for all participants. According to CBCL T-scores, all participants were in the normal range after training, whereas P2, P3, P4, and P5 were either in the clinical or borderline clinical ranges before training. Large training effect sizes were found for P2 and P3. According to TRF T-scores, P2 and P3 downgraded to the normal range from the clinical or borderline clinical ranges, and P5 downgraded to the borderline clinical range from the clinical range. A large effect size and medium-large effect size were found for P2 and P1, respectively.
Scores on the CBCL, TRF, and BRS Rated by Parents and Teachers at Pre- and Post-Training, and Effect Size Values for the Training.

Note. CBCL = Child Behavior Checklist; TRF = Teacher Report Form; BRS = Behavior Rating Scale.
A broad range of reductions on the other categories of the CBCL and/or TRF also has been found (see Table 5). Most (80% for the CBCL and 74% for the TRF) of the T-scores were lower at post-training for all participants. In particular, the T-scores were lower (except for the situation that the minimal T-scores were found at the both stages) for Somatic Complaints, Delinquent Behavior, Aggressive Behavior, Internalizing, and Externalizing on the CBCL for all participants. As for the TRF, T-scores were lower for at Social Problems for all participants, and lower for Somatic Complaints, Delinquent Behavior, Aggressive Behavior, Internalizing, and Externalizing for P1, P2, P4, and P5.
T-Scores on Other Categories of the CBCL and TRF at Pre- and Post-Training, and Effect Size Values for the Training.
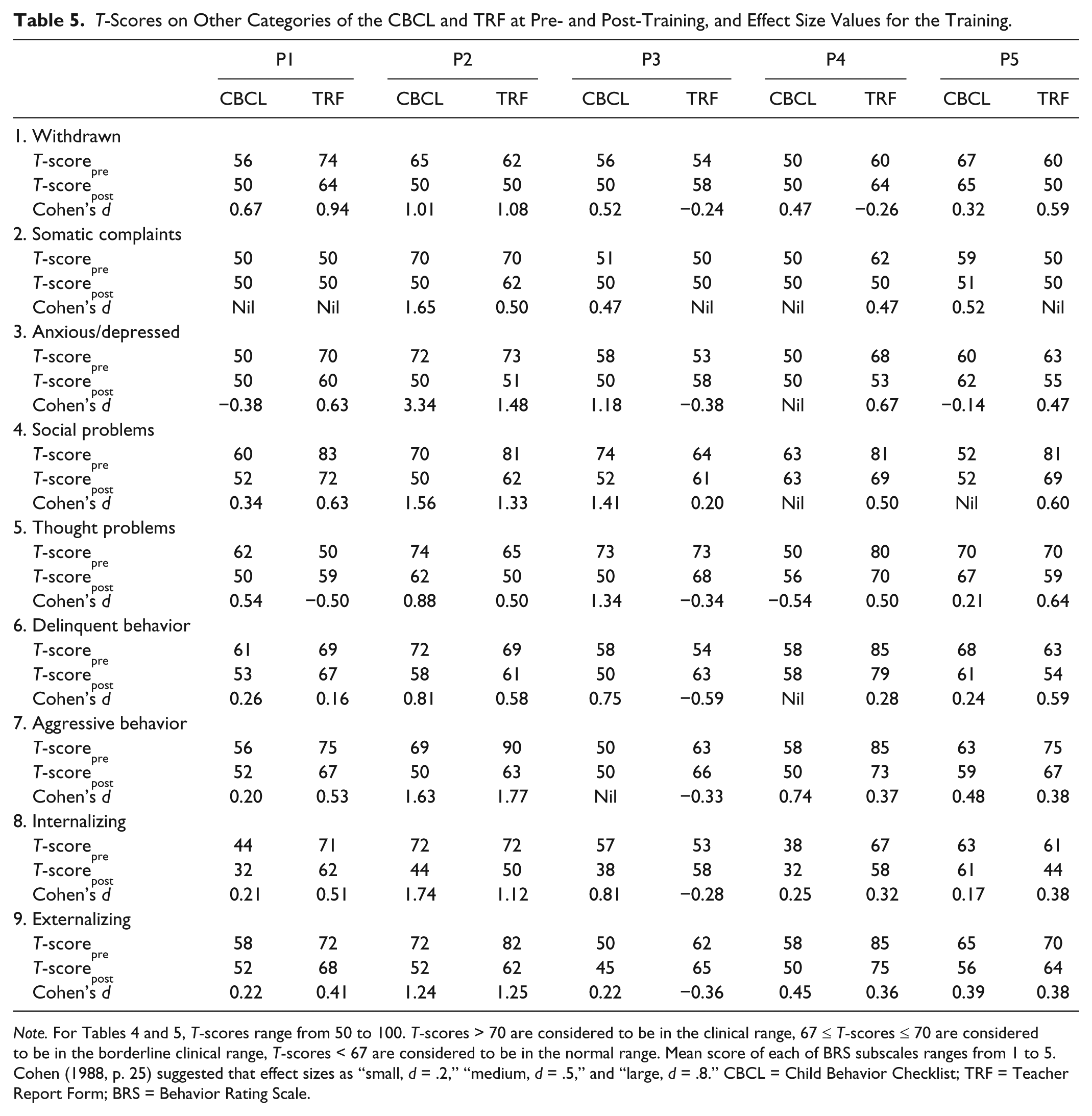
Note. For Tables 4 and 5, T-scores range from 50 to 100. T-scores > 70 are considered to be in the clinical range, 67 ≤ T-scores ≤ 70 are considered to be in the borderline clinical range, T-scores < 67 are considered to be in the normal range. Mean score of each of BRS subscales ranges from 1 to 5. Cohen (1988, p. 25) suggested that effect sizes as “small, d = .2,” “medium, d = .5,” and “large, d = .8.” CBCL = Child Behavior Checklist; TRF = Teacher Report Form; BRS = Behavior Rating Scale.
The largest improvement was for P2. A lower T-score and large effect size were found on each category of the CBCL. A lower T-score on each category and large effect size were found on the TRF. Considerable improvements were evident for P3 and P5. A lower T-score on each category of the CBCL (except that the scores of the Social Problems were the same at the two stages) and on each category of the TRF (except that the minimal T-scores on the Somatic Problems were found at the two stages) was found for P5. A lower T-score on each category of the CBCL (except that the minimal T-scores on the Aggressive Behavior were found at the two stages) was found for P3.
Inattention, Hyperactivity, and Impulsivity scores from the BRS rated by parents and teachers are also presented in Table 4. Inattention was lower at post-training for all participants based on parent ratings. Large effect sizes were found for P2, P3, and P4, and a medium effect size was found for P5, for the Inattention category. Hyperactivity was lower at post-training for four participants, and large effect sizes were found for P1 and P2. Impulsivity was lower at post-training for four participants, and large effect sizes were found for P1, P2, and P4.
Examining teacher’s BRS scores showed that Inattention was lower for three participants at post-training, and large effect sizes were found for P2 and P5. Hyperactivity was lower for four participants at post-training, and large effect sizes were found for P2 and P5. Impulsivity was lower for three participants at post-training, all of which yielded large effect sizes.
Assignment Completion
The percentages of assignment completion are shown in Figure 2. All participants (except P5) showed improvements during the training sessions. P4 showed the largest improvement. P1, P2, and P3 showed moderate improvements, relative to higher pre-training values. Although P5 did not show remarkable improvement during the training, his performance increased largely after the training. After the termination of the training, all participants maintained or increased their performance. Although a slight decrease of the percentages was found on P2, his average performance (M = 70%) was still better at this stage than at pre-training (M = 64%).

Percentage of assignment completion for each child across the phases.
Parent Acceptance
Significance of goals
Before the training, parents were asked to describe their child’s problem behaviors that affected learning. All parents mentioned that inattentive behavior, including distraction and daydreaming, had the biggest negative influence on their child’s learning. Parents thought that being inattentive in class lead to insufficient class participation and less chance to acquire and practice new skills/knowledge. In turn, the child’s ability to work efficiently was reduced and academic performance deteriorated. P1’s and P2’s parents believed that inattention was a major cause for repeated academic failures. The problem also interfered with the teacher’s instruction process and classroom management, and all parents reported that their child had low acceptance from teachers and peers.
Avoidance of doing assignments was another issue. Based on parent reflections, the problem generated from inattention. Inattention in class caused insufficient acquisition of knowledge and skills, and therefore, the children did not know how to complete assignments. Second, as the children were easily distracted while doing assignments, they took much longer to complete. Some parents reported that a piece of 1-hr work might take more than 3 hr to complete, even under adult supervision. This increased time limited the children’s time to participate in activities that they were interested in, such as playing with peers. This further reduced the children’s motivation in doing assignments or homework and reinforced the avoidance.
Acceptance of training procedure
After the training, all parents expressed acceptance of the training procedure. Parents expressed that they liked the training content. They reflected that their children were interested in the themed games and were satisfied in taking the training. Parents of P3, P4, and P5 observed that their children were motivated because the game difficulty levels adjusted appropriately. Four parents expressed acceptance of the training design. P2’s mother explained that the day-to-day training schedule was beneficial for sustained improvement. In addition, a session of 20 min was easy to schedule and did not create extra burdens for their normal lives. When asked which aspects of the training they found the most difficult to implement, all parents reported that the training was easy to implement and supervise. Similarly, none of the parents observed a negative effect or expressed concerns about potential negative effects.
Perception of effects
All parents perceived improved attention levels displayed by their children. It was reported that children initially exerted a high level of attention during the training. As the training progressed, all parents observed more on-task behavior during academic tasks. For example, P2’s mother observed that P2 displayed longer periods of sustained attention in requested tasks after five training sessions. Having consulted with their doctor, she stopped P2’s medication from the 10th training session. P2 still maintained attentive behavior after the termination of medication.
Another major change was that the children could complete classroom assignments at school, though they still required more time than peers. As the children’s working efficiency improved, they could complete more homework assignments. Parents of P2 and P4 also reported that their children started being less aggressive in doing tasks. The children exerted more patience and worked longer than before. When the children encountered failure, they would control negative emotions and try again rather than give up or throw tantrums as before.
As a positive side effect of the training, four parents reported that their children were more accepted by teachers at school. For example, P5 was nominated by the homeroom teacher to deliver a speech in the flag-raising ceremony due to his improved academic performance. P1 was nominated by his English teacher to be the group leader in class. Increased teacher acceptance also enhanced peer acceptance. Four parents reported that the children had received praise and nomination for class activities from peers. P2 and P4, in particular, made a few friends in class. Before the training, these children had low peer acceptance (see Table 1).
When asked whether they were satisfied with the outcomes of the training, all parents expressed positive satisfaction. Parents of P2, P3, and P4 thought the training was especially useful. Expressions such as “interesting” and “motivating” were frequently used in their general evaluations. When asked whether the training would work with similar problems in the future, four parents believed that it would work, while P5’s parent was not sure. When asked whether they would recommend the training to other parents, all parents expressed agreement. P3’s parent, in particular, suggested that the school adopt the training as a special support for children with attentive problems.
Discussion
The neurocognitive training approach was developed to assist children through exercising particular psychological abilities that are theorized to underpin AD/HD symptoms, as outlined in the CEM of the disorder (Sergeant, 2005a, 2005b). As a preliminary investigation, this multiple case study examined the outcomes of training on children with AD/HD and parent acceptance of the training in China. Five children with diagnosed AD/HD and their parents and homeroom teachers were involved in the study. The primary finding was that all participants benefited from the training, in terms of psychological abilities and AD/HD behaviors.
In general, the comparison of EEG summary score and game difficulty data at two training phases implied that the training improved psychological abilities commonly associated with AD/HD. When the children have an opportunity to practice these underlying psychological abilities, with an appropriate level of challenge and feedback, they can manifest much better performance. As the game level increased, children exerted more ability and effort to complete the tasks. Although the comparison of EEG data also showed reductions of ability values for some children, it may be that these children had already exerted high level of state control early in the training (an assertion supported by parent feedback), which made improvement harder to achieve. The limited increment on the relaxation-controlled game was likely due to such a reason.
The training resulted in reduced AD/HD behaviors and symptoms; this finding is supported by various forms of evidence. First, as illustrated by the CBCL and TRF, all participants yielded better results after training. Moreover, all children were rated by their parents as being at the normal level after training. Second, scores on the BRS completed by parents and teachers showed reductions in AD/HD symptom frequency. In particular, P2 and P5 showed reductions in all categories as rated by their parents or teachers. Third, responses from the parent interview indicated that more attentive behaviors were perceived during and after training sessions. As a secondary effect, children started showing more socially meaningful behaviors; that is, improvement in assignment completion and exertion of more patience during tasks. It is acknowledged that the outcome measures were largely subjective, and so open to expectation bias, with teacher ratings included as they are likely to be less affected by this than parent ratings.
The training also reduced other types of problem behaviors that commonly occur along with AD/HD. Wang, Zhang, Chen, and Liu (2009) found that children with AD/HD in China often demonstrated more broad behavioral problems than just AD/HD associated behaviors. In particular, boys with AD/HD are likely to display social, aggressive, and delinquent problems. As illustrated by change scores on the Chinese version of Child Behavior Checklist (CBCL-CV) and the Chinese version of Teacher Report Form (TRF-CV), all children showed reductions in associated behaviors. Some children (e.g., P1 and P2) showed reduction on more than six associated behaviors as rated by their parents or teachers. These findings indicate that parents and teachers have perceived a broad range of behavioral improvements as a result of the neurocognitive training. The records of assignment completion also support the conclusion. As the training progressed, the children had completed more schoolwork, and the improvements remained after the training.
The present study indicates that the neurocognitive training can result in broader and more socially meaningful outcomes than just improvement of AD/HD symptoms. Two reasons possibly explain the side effect. First, it may be the case that the increased attentive behavior in class and improved quality of schoolwork improved these children’s social status. As suggested by previous studies, Chinese children’s social acceptance is profoundly influenced by their in-class behavior and academic performance (Wei, et al., 2004; Xie & Wang, 2010). In the present study, all the children had better social status after the training, as rated by their homeroom teachers. Second, game-driven and task-directed features of the training increased the children’s confidence in doing tasks. The training conveys a message that the children themselves can improve AD/HD symptoms or related outcomes if they put in effort. When the children feel they are partially in control of the problem, their motivation for doing daily tasks may improve and their expectation for success may increase (for details about Weiner’s attributional theory of achievement motivation and emotion, see Weiner, 1985). These further reflect the fact that children with AD/HD had encountered difficulties in varied life domains due to the manifested symptoms. This is consistent with other studies that found that children with AD/HD in China had poor quality of life (e.g., Wei & Su, 2004; Xie et al., 2011).
The findings of the present study indicate improvement of the cognitive and state-control problems that are commonly associated with AD/HD, with positive implications for AD/HD symptoms and related problems as reported by parent and teachers. The findings are in line with previous studies on children with AD/HD in Western countries (Johnstone et al., 2012; Johnstone et al., 2010) that examined only the cognitive training element. These findings speak to the relationship between underdeveloped psychological abilities, negative behavior patterns, and inadequate academic and social participation at school, and indicate that once the children have received positive support and technical aids, they can achieve dramatic improvements.
Previous work targeted only cognitive factors and reported a more limited range of benefits (Johnstone et al., 2012; Johnstone et al., 2010), as is the case in previous cognitive (e.g., Klingberg et al., 2005) and neurofeedback training studies (Arns et al., 2009, Lofthouse et al., 2012). Here, the concurrent practice and improvement at working memory and impulse-control processes, and awareness and regulation of psychological states (i.e., attention and relaxation levels), appear to have had broad implications for AD/HD symptoms and related effects on day-to-day functioning including areas such as behavioral control and social contact. The CEM of AD/HD (Sergeant, 2005b) would predict this broad influence from a training approach that addresses the state-regulation, cognitive, and executive function problems that underpin the disorder.
As for parent acceptance, all reported the training to be useful and acceptable for their children. Before the training, parents identified that two problem behaviors, namely, inattention and avoidance of doing assignments, had the biggest impact for children’s learning. According to parent interviews after the training, both problem behaviors were reduced and children showed more desirable behavior when doing academic and non-academic tasks. Moreover, they found more socially desired outcomes (e.g., teacher praise, peer acceptance) as the training progressed. In addition to the perceived effect of training, all the parents accepted the training procedure and did not report any inconvenience. Without the minimal social acceptance, it is insufficient to conclude that an intervention will be widely applied, even though the intervention may have promising outcomes in empirical research (Wolf, 1978).
Previous studies (Chen et al., 2008; Huang et al., 2012) on parent acceptance of medication for children with AD/HD suggest that Chinese parents are concerned about potential negative side effects. Parents in the current study held similar attitudes. In contrast, they considered the neurocognitive training to be a positive treatment and accepted the procedure. Furthermore, it is important that the training procedure is easy to understand and implement, and does not require professional assistance. As computers and access to the Internet become more widely available in Chinese families, this type of training could be easily implemented.
Limitations and Conclusion
These findings should be interpreted in light of the following limitations. First, the cases did not include participants under 8 year of age because this study was interested in school-aged children in China. Thus, the findings have limited implications for neurocognitive training for younger children. Second, two of the participants were on medication during the training, which might cause an interaction effect between training and medication. Third, there was no follow-up phase (except for assignment completion), so it is uncertain how the effects might maintain over time. Although it should be noted that Johnstone et al. (2012) reported that effects remained present at a 6-week follow-up, this was following the cognitive training element of the approach reported here, so it will be necessary to assess the longer-term effects of the combined approach in future studies. Fourth, while the EEG summary score data allowed comparisons of pre- and post-training state control, benchmarks for the EEG summary score data were not available, so it is difficult to judge whether the improvements measured in the study reflect a move toward a typical pattern. Fifth, given that this study was a naturalistic study (Lincoln & Guba, 1985), parents and teachers were not blinded from the training purpose and procedure. Such a study design has some advantages; for example, parents gradually formed their understanding and subjective acceptance of the training throughout the procedure and eventually gave a comprehensive opinion after the training. Nonetheless, behavioral ratings provided by these participants might not have been free from bias, given their relationships with the participating children. Although the use of multiple sources of evidence may reduce this potential bias (Yin, 2009), future studies should adopt a more rigorous design (e.g., blinded treatment-control design; Lofthouse et al., 2012). Finally, while the case study design provides more detailed descriptions of the results for specific participants, it also involves a small sample size making statistical comparison difficult and does not contain a control group. Future research should include a randomized control design, follow-up sessions to determine the longevity of effects, a larger sample size, and attempt to examine the impact of the training on academic performance as well as its social validity. It would also be interesting to examine the unique contribution of each element of the training approach to outcomes, and to subsequently examine tailoring the training to suit the specific needs of each child based on an assessment of areas of need.
In summary, the findings from the present preliminary study support the use of neurocognitive training for children with AD/HD in China. The objective (i.e., training and EEG) and subjective data (i.e., parent ratings/feedback and teachers’ ratings) suggest that neurocognitive training has the potential to improve psychological abilities and behaviors that are associated with AD/HD. The training was considered by parents to be an effective and positive intervention to be conducted in the home context. This reflection warrants the need for investigation on a larger sample size and in other contexts that are important to children in China, and indeed other locations around the world.
Footnotes
Acknowledgements
The authors thank the participating schools, children, and families for their generous time and effort.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.J. is a co-inventor on several pending patent applications in relation to the cognitive training methodology, which is used within the training software product and which is licensed by University of Wollongong (UOW) to Neuro Cognitive Software. He is entitled to a portion of royalties received by UOW in relation to sale of the product.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Neuro Cognitive Solutions provided hardware/software for the current study.