
Abstract
The purpose of this study was to assess the health, lifestyles, and goals of homeless male shelter users. The mixed-methods descriptive non-experimental study was conducted at a homeless shelter cot program. The Dykeman biopsychosocial interventional model was used as a framework for this study. Thirty men utilizing the program were interviewed using the Chapin Lifestyle Assessment Survey. In addition, the men were asked about their social support system and goals. The results demonstrated that the group had a strong sense of responsibility for their own actions, a desire to learn, and were motivated to make a meaningful contribution. Goals focused on obtaining employment and securing housing. Shelter staff was reported as a source of social support.
Although the U.S. homeless population has slightly decreased in recent years, far too many individuals remain homeless. It is evident that the appropriateness of the current structure of services and modes of delivery require evaluation and modification to meet existing needs. There has been limited literature that examines the health, lifestyles, and goals of the homeless and potential interventions, which will move individuals from homelessness to self-sufficiency and social reintegration. Community health nurses are in a key position to participate in interdisciplinary care models for the homeless through awareness of health, lifestyles, and identification of personal and vocational goals.
Literature Review
Despite the interventions provided by various social services programs and religious and governmental organizations, homelessness continues to be a significant issue in the United States. While it is impossible to measure with exact certainty the number of individuals experiencing homelessness in a given day or year, an estimated 633,782 individuals were reported as homeless in January, 2012 (National Alliance to End Homelessness, 2013). From 2011 to 2012, there was a modest decrease in homelessness of 0.4%, which is representative of approximately 2,235 people (National Alliance to End Homelessness, 2013). The rate of homelessness was 20 homeless persons per 10,000 persons in the general population (National Alliance to End Homelessness, 2013). The problem has been perpetuated over the past two decades by the lack of affordable housing and a concurrent increase in poverty. The poverty rate increased by approximately 5% between 2010 and 2011 with 48 million persons living in poverty in 2011 (National Alliance to End Homelessness, 2013). The circumstances leading to homelessness are numerous and can be classified as personal, financial, and structural (Christiani, Hudson, Nyamathi, Mutere, & Sweat, 2008). Personal causes of homelessness include mental health issues, addiction, physical health issues, and domestic violence. Structural and financial causes include lack of employment, decreased access to health care, minimum wage jobs incapable of providing self-sufficiency, lack of affordable housing, foreclosure, recession, medical bankruptcy, and decrease in public assistance programs.
The majority of homeless are single adults with a variety of complex medical, mental health and addiction issues. The morbidity and mortality rates are higher for the homeless population as compared with the general population with cardiovascular diseases comprising the leading cause of death (Randers et al., 2012).
In many instances, the homeless population exists from day to day lacking a plan or sense of direction for the future. Many of the services currently in existence to serve the homeless aggregate support a day to day existence by providing meals and shelter but lack educational, vocational, and case management components that facilitate reintegration into society and move individuals to self-sufficiency. Providing for basic necessities and safety is of paramount importance but is only the first step in the process of providing holistic care to the homeless population. Most of the homeless seeking assistance focus on meeting immediate needs for food and shelter and do not address the issues that have led to homelessness (O’Toole et al., 2007). To provide holistic care to the homeless, it is imperative that surrounding social and personal issues be addressed (Tsai, Mares, & Rosenheck, 2012; Williams & Stickley, 2011). Homeless individuals often experience social isolation and stigmatization. Possessing an affiliation with a group or organization provides the individuals a sense of societal belonging, thereby facilitating social reintegration (Tsai et al., 2012). Homeless adults may better benefit from a model of long-term management rather than crisis management of food and shelter (Kim, Ford, Howard, & Bradford, 2010). Supportive housing alone does not affect societal reintegration of homeless adults. Providing choice and a sense of control over one’s living environment may slightly affect psychological well-being and satisfaction with housing in this population (Tsai & Rosenheck, 2012b).
To move individuals from poverty, addiction, chronic disease, and homelessness to self-sufficiency and reintegration into society, the provision of structured, goal-oriented programming is essential. One such biopsychosocial interventional model is multidimensional and is designed to meet the complex and holistic needs of the homeless population (Dykeman, 2011). The model includes four components. The first component is initial interface with the homeless client where basic physical and safety needs are assessed and addressed. The second phase focuses on mental health status and cognitive capabilities as well as the as the ability to access community resources. This adaptive functional assessment describes the client’s skill set for coping with various social and environmental demands such as relationships, school, and work. The need for referrals and associated case management is often identified. The third intervention phase focuses on psychological counseling to address lifestyle issues surrounding work and social demands as well as self-concept and spirituality. The fourth phase of the intervention addresses client advocacy. This is accomplished when working on a one on one basis with clients and also when assisting them as they negotiate local, regional, and federal resources. This type of supportive housing and comprehensive case management provides the much-needed resources beyond the basics of meals and shelter to assure that the personal, social, and environmental issues leading to homelessness are addressed.
While there is an abundance of literature describing the challenges and experiences of the homeless in terms of physical, mental, and social challenges, few studies examine the perspectives of the homeless population in terms of health, lifestyle, and goals. To effectively care for the homeless population, it is imperative that health care professionals possess insight into and awareness in these areas. Ideally, the function of shelters should be to provide temporary crisis or transitional residence in conjunction with active and ongoing collaboration with the homeless population on goal-directed educational and vocational training, which facilitates self-sufficiency instead of merely providing for basic necessities. Supporting housing models need to focus on social reintegration and improvement of clients’ life satisfaction (Tsai et al., 2012; Tsai & Rosenheck, 2012a). Community health nurses are in a key position to participate in interdisciplinary teams and provide expertise in case management, wellness, health promotion, and maintenance.
Method
To further expand the body of knowledge related to the health, lifestyles, and goals of homeless men, a study was conducted at a homeless shelter with an overnight cot program for homeless men in a Midwestern city. The study was a mixed-methods design of descriptive statistical analysis and naturalistic inquiry using qualitative data (Patton, 1990). Homelessness was theoretically defined as “an individual or family living in a supervised publically or privately operated shelter designated to provide temporary living arrangements” (U.S. Department of Housing and Urban Development [HUD] Homeless Emergency and Rapid Transition to Housing Act, 2011, p. 75995). Operationally, homeless was defined as residents sleeping in the local shelter cot program. The Lifestyle Assessment Survey (Chapin & Ivey, 2004) was used to measure health and lifestyles. Open-ended interview questions inquired into events leading to homelessness, long- and short-term personal goals, and social support. Interviews were conducted by a male registered nurse research assistant. This nurse was chosen due to his prior relationship with the men and their comfort with the nurse.
Sample and Procedure
There was an average of 40 to 50 men sleeping at the shelter nightly. A convenience sample of 30 homeless men was interviewed. All men sleeping at the shelter were above the age of 18 years. Participants were solicited during the morning breakfast. Those choosing to participate received two bus passes and a bottle of water as an incentive for participation. After an individual introduction to the study by the interviewer, informed consent was understood if the individual verbally chose to proceed with the interview. The study was approved by the agency and the university institutional review board.
Instrumentation
Participants were interviewed using the Lifestyle Assessment Survey (Chapin & Ivey, 2004). The survey consisted of 60 questions on a 5-point Likert-type scale. There were six subscales dividing lifestyle into Physical Health, Emotional Well-Being, Intellectual Enrichment, Life–Work Satisfaction, Social Effectiveness, and Spiritual Awareness. Each subscale consisted of 10 statements reflective of a positive lifestyle. Participants were asked to rate their lifestyle behaviors with a maximum score of 50 in each subscale. Possible total scores range from 60 to 300 with higher scores indicating more positive lifestyle behaviors and lower scores indicating less positive lifestyle behaviors and a need for improvement.
In addition, participants were interviewed regarding their social support system, events leading to homelessness, and their personal goals for the week, month, and year. Demographic variables included age, number of years homeless, and level of education. The interview format was chosen due to a potential lack of reading ability and to assure comprehension of the survey items, and to allow for open-ended questions that encourage free responses. Participants were able to seek clarification regarding statements. Each interview took place in a private setting located in the shelter and lasted approximately 30 min.
Results
The results of the study found the average age of homeless men to be 45 years with ranges of 24 to 69 years. Eighty-six percent completed high school or additional education. The majority of men were found to be on the street 1 to 5 years with outliers ranging from 10 to 44 years.
The mean score for the participants on the Lifestyles Assessment Survey (Chapin & Ivey, 2004) was 188 with scores ranging from 133 to 244 of a possible 300. Overall, this score indicated the group as “having the right idea but more work is needed” according to the Lifestyle Assessment Survey. Internal consistency of items on survey was demonstrated with a Cronbach’s alpha of .917. Survey item means indicate areas that lend opportunity for programming and lifestyle improvement. Individual questions were reviewed, and 7 mean scores were at or above 4.0/5.0. Three individual questions had mean scores of 2.0/5.0 or less. See Table 1.
Lifestyle Assessment Survey Results.
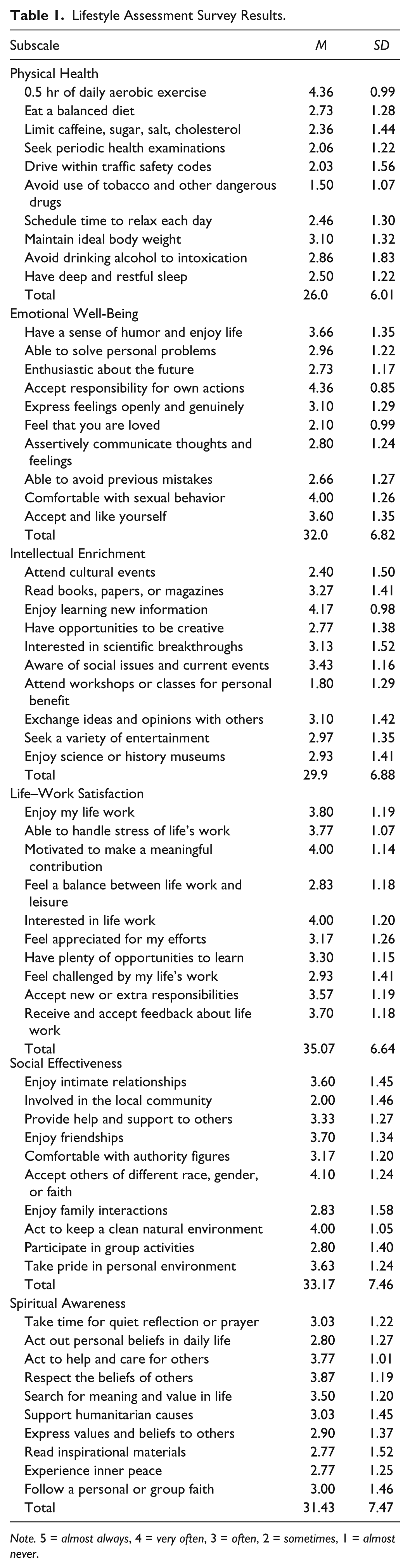
Note. 5 = almost always, 4 = very often, 3 = often, 2 = sometimes, 1 = almost never.
The mean total score of the Lifestyle Assessment Survey was compared for the men who reported being homeless for less than 2 years with the total score of those reporting being homeless for 2 years or more. It was hypothesized that those being homeless for a longer time would report a less healthy lifestyle. There was no significant difference between the mean total scores of the two groups, t(28) = 1.008, p> .05.
For the analysis of the open-ended questions, a cross-case analysis was done individually by three researchers to describe the data. Each question was reviewed, and items were grouped by topic and color coded. Subsequently, researchers gathered to compare grouped items and discuss the interpretation of the data.
There were a variety of responses to the question associated with events leading to homelessness. The responses were grouped into four categories: relationships, economic, substance abuse, and health. Relationship responses were related to loss; many had divorced or lost a parent who had been providing a home. Economic responses were related to job loss, money mismanagement, and child support. The loss of a driver’s license also affected ability to find employment. Many study participants were forthright with responses related to substance abuse. Alcoholism, drug abuse, and multiple DUIs (driving under the influence) were reported as events leading to homelessness. In addition, substance-abuse-related health issues including depression, multiple surgeries, and a bleeding disorder were reported as factors leading to homelessness.
All of the study participants had personal goals. Short-term goals focused on employment, whereas long-term goals were related to housing. The immediate or weekly goals were related to getting sober, being healthy, and finding a job. Monthly goals included finding a home, while goals for the year were staying sober, getting a job, finding a home, and finding transportation.
Friendship and emotional support were reported from many men. Most participants reported having family and friends. Some singled out parents and siblings. In addition, the shelter staff was reported to be a source of social support.
Limitations
A significant limitation of the study was the lack of a comparison group for the assessment tool. Specific metrics were not available from the author. In addition, the tool may have not been the most appropriate to utilize with this population. It is possible the tool did not capture data specific to this population, particularly information regarding physical health and health promotion behaviors. Finally, the sample size was small, and interviews were conducted by one interviewer at one homeless shelter with an exclusive male population. Therefore, results may not be generalizable.
Discussion
The purpose of this study was to assess the health, lifestyles, and goals of homeless male shelter users. The literature describing these concepts in the homeless population is limited. The findings of this study suggest that this sample of homeless men have a broad range of lifestyle behaviors and personal goals. Many of the study participants, like many homeless, have made poor lifestyle choices related to substance abuse, which in turn, resulted in their homelessness. The mean of the total score on the Lifestyle Assessment Survey demonstrates this population is in need of assistance to increase healthy lifestyle choices, health promotion, and health maintenance behaviors. To best address the broad range of needs of this population, an interdisciplinary approach utilizing a biopsychosocial model (Dykeman, 2011) is essential. Services for the homeless population must provide interdisciplinary interventions including supportive housing, which facilitates social reintegration, assistance with obtaining employment or vocational training, and the provision of comprehensive health care services.
In the Dykeman (2011) model, physical and safety needs are initially assessed. Although basic safety needs are being addressed in the shelter cot program, physical and health promotion parameters were demonstrated as lacking. Mean scores on the Physical Health subscale were the lowest of all subscales (26.0/50.0). Although participants reported daily aerobic exercise, it can be assumed this is related to walking around town as they have no permanent housing or shelter at this emergency facility. More structured exercise programs could benefit these men. To address the issue of physical fitness, community health nurses must be innovative in their approach and encourage aerobic activities in ways the homeless population can easily access and participate. Street soccer is one such activity that has demonstrated success (Randers et al., 2012). Incentivizing organized exercise or walking programs may increase daily aerobic activity. Other item means in the Physical Health subscale were very low. This group of homeless men did not report avoidance of tobacco or other dangerous drugs. The community health nurse might refer or design programs in smoking cessation and/or partner with Alcoholics Anonymous (AA) or Narcotics Anonymous (NA). Additional health measures of diet, health exams, substance abuse, rest, and relaxation are not typically under the control of the homeless. Therefore, the Physical Health subscale may not have been ideal to accurately assess physical health parameters in the homeless population.
The Lifestyle Assessment Survey subscale on Emotional Well-Being mean was 32.0/50.0. This score reflects a sense of responsibility for one’s actions, an acceptance of self and life circumstances, possessing a sense of humor, and deriving enjoyment from life. It is both troubling and noteworthy that the lowest subscale item mean ascertaining whether the individual felt loved was 2.1/5.0. Overall, despite being homeless, the resiliency of the human spirit prevailed, and individuals reported a relatively high degree of emotional well-being and acceptance of their life station.
The Lifestyle Assessment Survey subscale on Intellectual Enrichment was the second lowest mean (30.0/50.0) of the six subscales. Although participants reported they enjoyed learning new information, the opportunities to express creativity, enjoy a variety of entertainment, and acquire and share new information are limited in a shelter setting. Nurses in collaboration with community agencies can provide programing on a variety of health topics, entertainment, creative art and music classes, and speakers with discussion on current world events.
The Lifestyle Assessment subscale on Life–Work Satisfaction mean (35.1/50.0) was the highest of the six subscales. Participants reported being motivated to make a meaningful contribution, were willing to accept new or extra responsibilities, and were receptive to feedback regarding their life work. The mean for an item in the subscale related to the balance between life work and leisure was particularly low (2.8/5.0). This is most likely reflective of the survival mode reality in which homeless individuals exist. Shelter program directors are in a position to facilitate partnerships with agencies and community colleges for skills training and job placement.
The Lifestyle Assessment Survey subscale mean on Social Effectiveness was 33.2/50.0. The low mean on the subscale item related to involvement in the local community (2.0/5.0) is likely reflective of the social isolation a marginalized group experiences. The highest mean for an item on the subscale was related to acceptance of others of a different race, gender, or faith (4.1/5.0). Although shelter residents may not feel part of the local community, a sense of belonging and a culture of friendship exist. The men enjoy camaraderie with fellow residents. Shelter staff were frequently reported to be a source of social support and identified as family.
The Lifestyle Assessment Survey subscale mean for Spiritual Awareness was 31.4/50.0. Item means for respecting the beliefs of others (3.8/5.0) and acting to help and care for others (3.7/5.0) were the highest. This is also supported by the reported sense of community in the interviews related to social support. Similarly, Tsai and Rosenheck (2011) concluded that assessing and promoting spirituality may benefit homeless populations in both clinical and psychological outcomes.
A hallmark finding in this study was the lack of feelings of esteem from others, as participants had to contemplate whether or not they felt loved. Dykeman’s (2011) third intervention phase recommends a focus on counseling surrounding work, social demands, and spirituality. Health professionals at this shelter need to be aware that shelter personnel may be identified as “family” and, therefore, are an important source of social support. Therapeutic relationships and professional boundaries must be negotiated by nurses and social services personnel while being viewed by homeless clients as supportive and caring. Finally, persons who were previously homeless identified that a critical component of moving off of the streets was someone reaching out to them (MacKnee & Mervyn, 2002). It is important that community health nurses and other health professionals interfacing with this population validate and promote these attributes, as this will facilitate the process of goal setting and attainment necessary to move from homelessness to self-sufficiency.
In the Dykeman (2011) model, the second intervention phase addresses cognitive capabilities and mental health status. It is noteworthy that 86% of the sample reported graduating from high school. This level of educational attainment suggests a strong potential for success with vocational training. Future services directed toward this population should focus on educational and vocational programs that challenge and encourage these men to succeed. Goals should be directed toward attaining and maintaining sobriety, obtaining appropriate housing, and securing employment. Community health nurses must partner with addiction recovery specialists and social services personnel to facilitate optimal outcomes for this population. Transitioning from homelessness into a community residence is a tremendous undertaking because of the complex psychosocial issues inherent in the homeless population. Homeless persons will require more assistance and support while navigating the social service system after obtaining housing, as obtaining housing alone is not sufficient. On obtaining housing, continued and long-term additional assistance in the form of supportive housing and active case management is necessary to improve outcomes. Ongoing social support can facilitate improvement in physical and mental health outcomes (Stein, Nyamathi, & Zane, 2009). Continued monitoring and support will facilitate a successful transition (Drury, 2008).
Community health nurses possess the knowledge, attitude, and skills to lead and take the initiative in the development of a tool to more accurately assess the health and lifestyles of the homeless. Traditional tools may not accurately assess physical health and health promotion behaviors. Further study, which includes a modified assessment of those parameters, is warranted. Interventions must be tailored to meet the unique and individual needs of this population. Finally, community health nurses must assume a leadership role and advocate for changes in public policy and streamlining of services, which facilitate the process of social reintegration (Daiski, 2007; Dykeman, 2011).
Footnotes
Authors’ Note
This manuscript has not been published elsewhere, nor has it been submitted simultaneously for publication elsewhere.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article